
Structural and Functional Validation of a Full-Thickness Self-Assembled Skin Equivalent for Disease Modeling

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture and Treatment
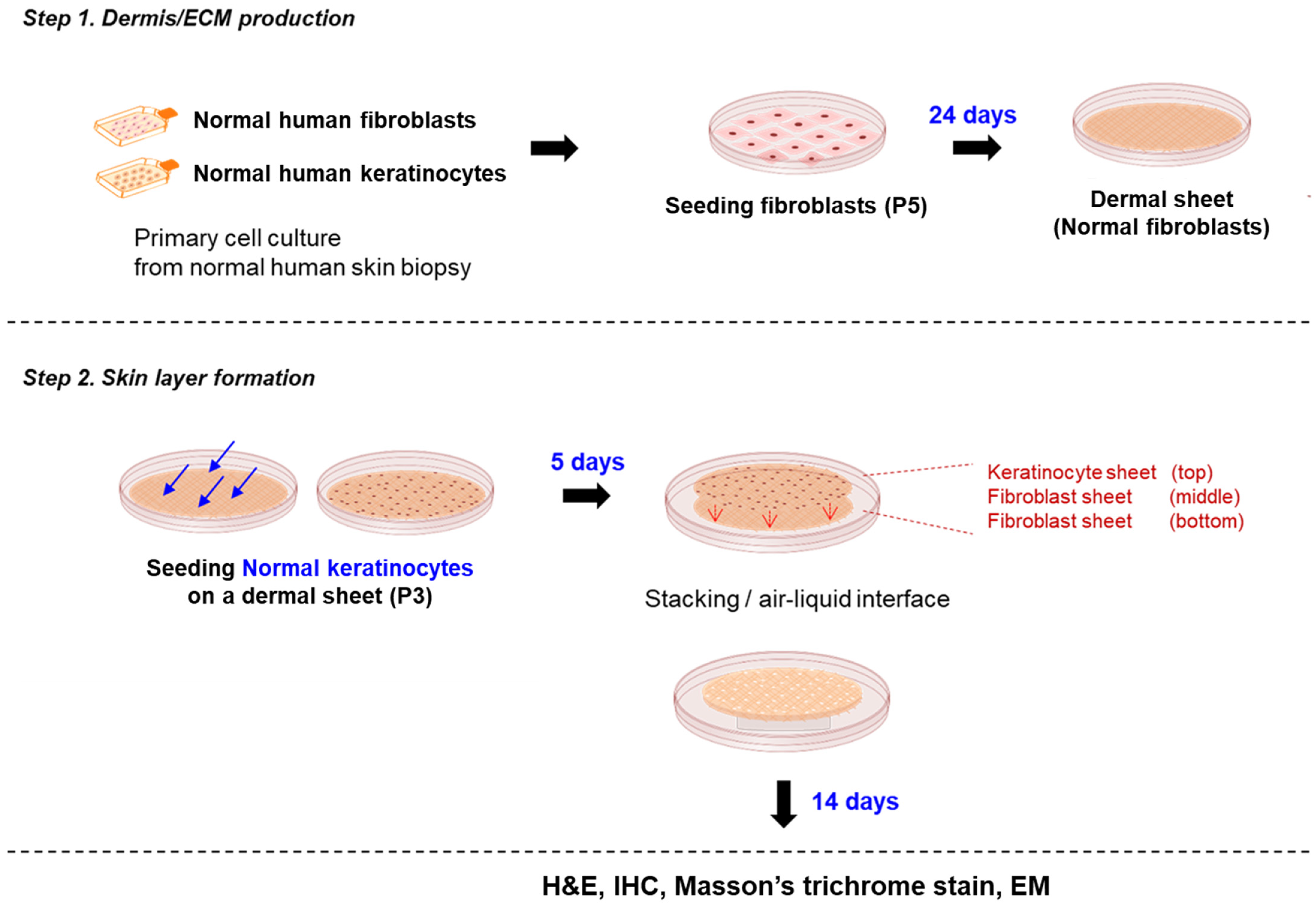
2.2. Generation of the RSE
2.3. Histological Analysis
2.4. Scanning Electron Microscopy (SEM)
2.5. Transmission Electron Microscopy (TEM)
2.6. Tissue Viability
2.7. Immunostaining
2.8. RNA Extraction and Quantitative Real-Time PCR
2.9. Statistics
3. Results
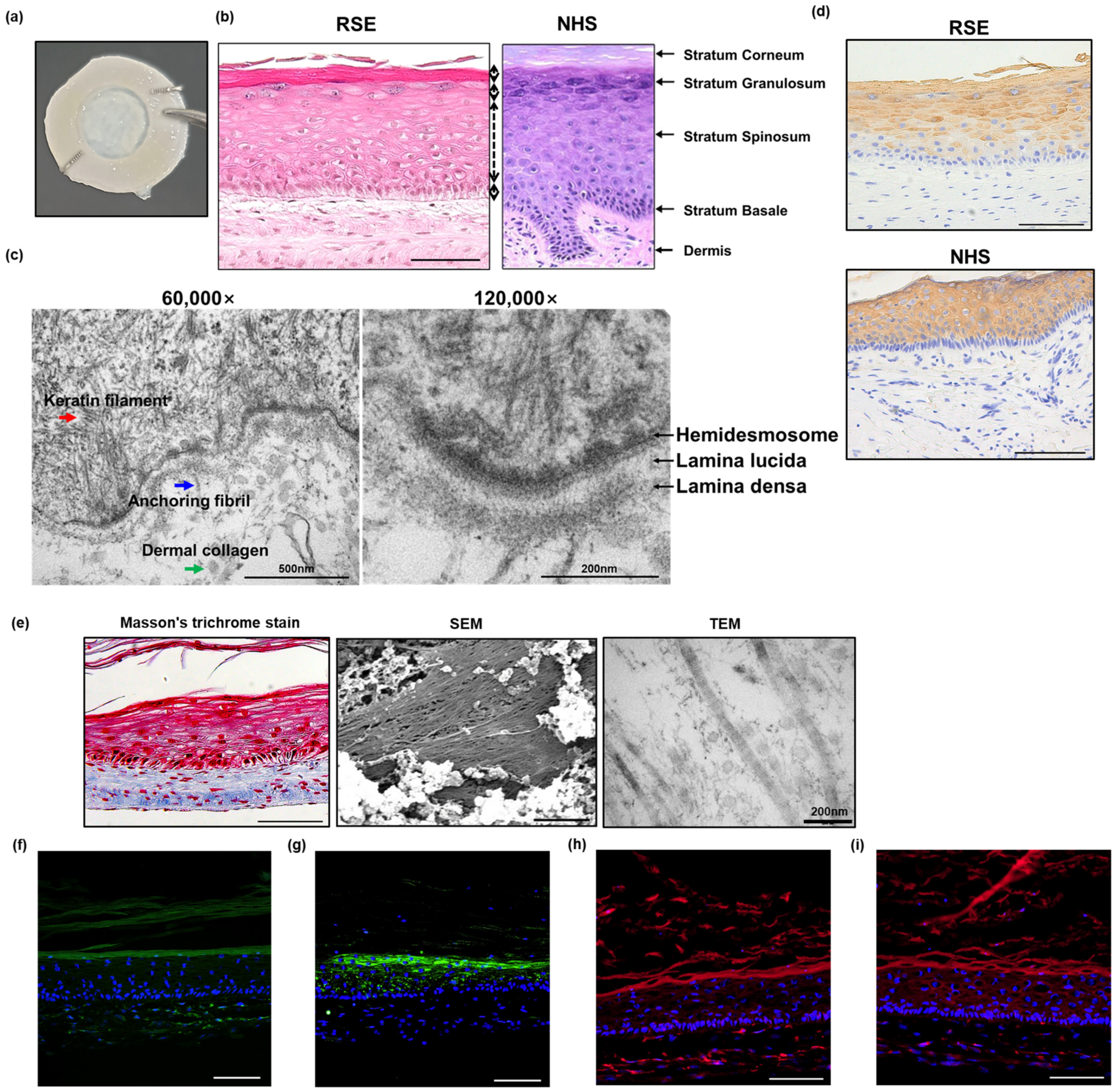
3.1. Histological Morphology of the Self-Assembled RSE Model Was Similar to That of the Normal Human Skin
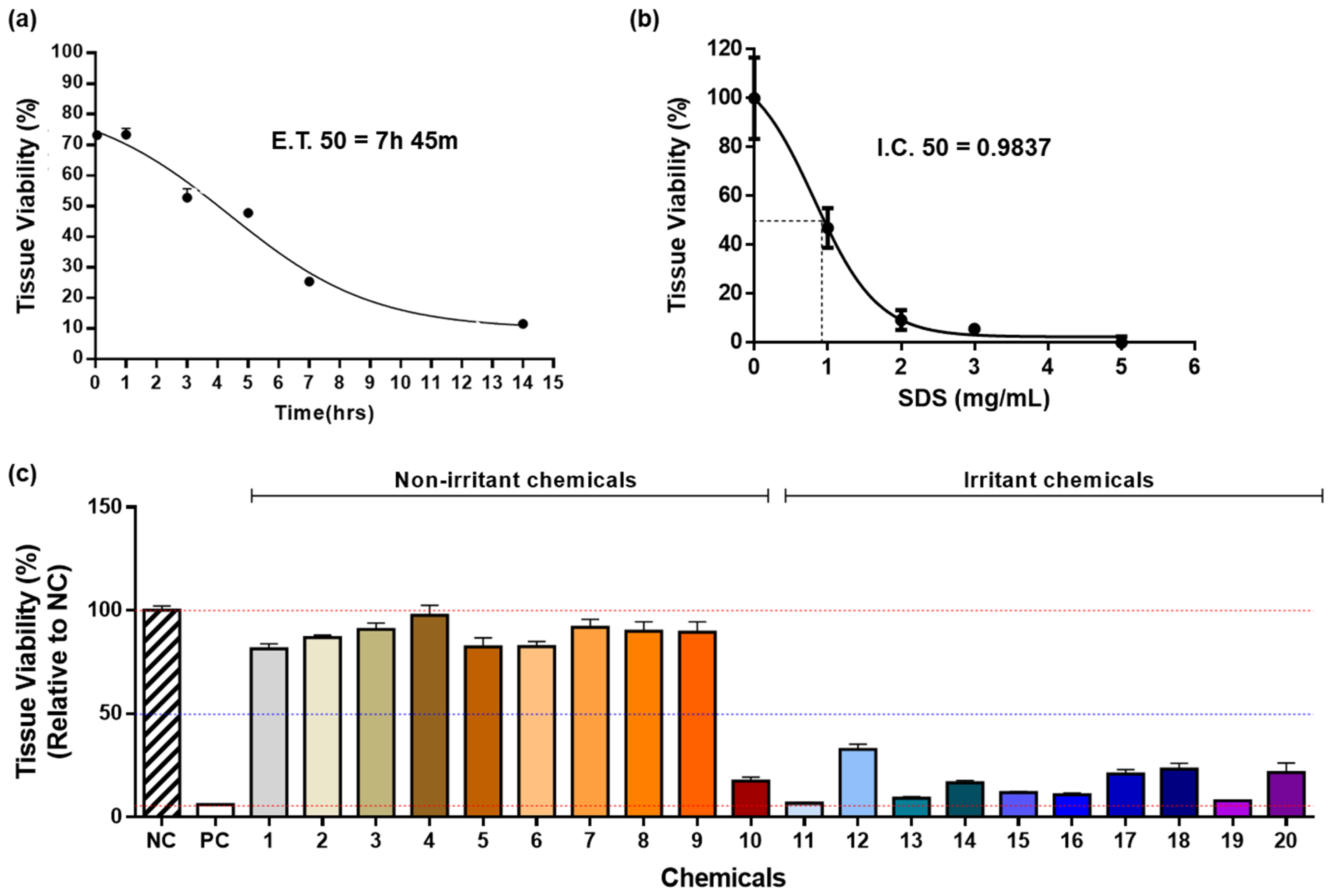
3.2. Biological Reactivity of the Self-Assembled RSE Model
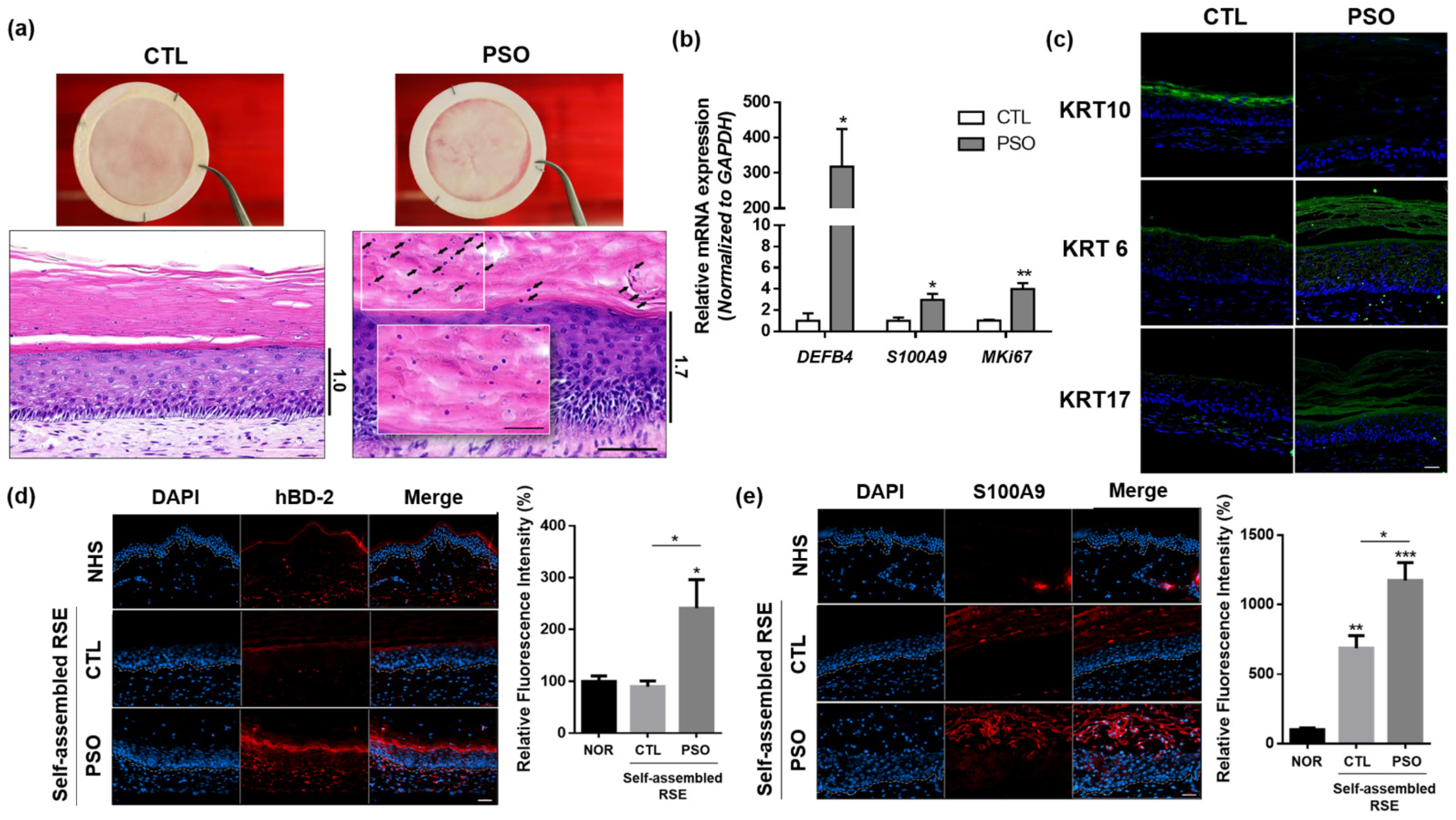
3.3. Development of an In Vitro Psoriasis-Like RSE Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Niehues, H.; Bouwstra, J.A.; Ghalbzouri, E.I.; Brandner, J.M.; Zeeuwen, P.L.J.M.; Bogaard, E.H. 3D skin models for 3R research: The potential of 3D reconstructed skin models to study skin barrier function. Exp. Dermatol. 2018, 27, 501–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathes, S.H.; Ruffner, H.; Graf-Hausner, U. The use of skin models in drug development. Adv. Drug Deliv. Rev. 2014, 69–70, 81–102. [Google Scholar] [CrossRef] [PubMed]
- Sanabria-de la Torre, R.; Fernández-González, A.; Quiñones-Vico, M.I.; Montero-Vilchez, T.; Arias-Santiago, S. Bioengineered Skin Intended as In Vitro Model for Environmental Skin Impact Analysis. Biomedicines 2020, 8, 464. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.M.; Lee, S.H.; Jang, W.H.; Jung, H.S.; Heo, Y.; Park, Y.H.; Bae, S.J.; Lim, K.M.; Seok, S.H. KeraSkinTM-VM: A novel reconstructed human epidermis model for skin irritation tests. Toxicol. Vitr. 2014, 28, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, K.; Lombardi Borgia, S.; Korting, H.C.; Mewes, K.R.; Schäfer-Korting, M. The phenion® full-thickness skin model for percutaneous absorption testing. Skin Pharmacol. Physiol. 2010, 23, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aureélie, F.; Malaisse, J.; Vuyst, E.; Minner, F.; Rouvroit, C.L.; Poumay, Y. Epidermal morphogenesis during progressive in vitro 3D reconstruction at the air-liquid interface. Exp. Dermatol. 2012, 21, 871–875. [Google Scholar]
- Test No. 439: In Vitro Skin Irritation—Reconstructed Human Epidermis Test Method; OECD: Paris, France, 2013. [CrossRef]
- Takami, A.; Nagura, M.; Hiura, A.; Kojima, H.; Akashi, M. Construction of Three-Dimensional Dermo-Epidermal Skin Equivalents Using Cell Coating Technology and Their Utilization as Alternative Skin for Permeation Studies and Skin Irritation Tests. Tissue Eng.-Part A 2017, 23, 481–490. [Google Scholar]
- Liao, C.C.; Cheng, Y.W.; Meng, H.L.; Hsieh, F.K.; Hsu, L.T.; Chang, S.Y.; Chen, K.J. Validation study of a new reconstructed human epidermis model EPiTRI for in vitro skin irritation test according to OECD guidelines. Toxicol. Vitr. 2021, 75, 105197. [Google Scholar] [CrossRef]
- Kandarova, H.; Jamin, A.; Willoughby, W.H.; Jong, D.; Letasiova, S.; Milasova, T.; Bachelor, M.A.; Breyfogle, B.; Handa, Y.; Fonteyne, L.; et al. Pre-validation of an in vitro skin irritation test for medical devices using the reconstructed human tissue model EpiDermTM. Toxicol. Vitr. 2018, 50, 407–417. [Google Scholar] [CrossRef]
- Pedrosa, T.N.; Catarino, C.M.; Pennacchi, P.C.; Assis, S.R.; Gimenes, F.; Consolaro, M.E.L.; Moraes-Barros, S.B.; Maria-Engler, S.S. A new reconstructed human epidermis for in vitro skin irritation testing. Toxicol. Vitr. 2017, 42, 31–37. [Google Scholar] [CrossRef]
- Mok, B.R.; Kim, A.R.; Baek, S.H.; Ahn, J.H.; Seok, S.H.; Shin, J.U.; Kim, D.H. PFN1 Prevents Psoriasis Pathogenesis through IκBζ Regulation. J. Investig. Dermatol. 2022; ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Nestle, F.O. Mechanisms of disease: Psoriasis. N. Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Andrea, C.; Romanelli, P.; Volpe, E.; Borsellino, G.; Romanelli, M. Scanning the immunopathogenesis of psoriasis. Int. J. Mol. Sci. 2018, 19, 179. [Google Scholar]
- Yaxiong, D.; Chang, D.; Lu, Q. The Inflammatory Response in Psoriasis: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2016, 50, 377–389. [Google Scholar]
- Moos, S.; Mohebiany, A.N.; Waisman, A.; Kurschus, F.C. Imiquimod-Induced Psoriasis in Mice Depends on the IL-17 Signaling of Keratinocytes. J. Investig. Dermatol. 2019, 139, 1110–1117. [Google Scholar] [CrossRef] [Green Version]
- Christina, K.; Antoniadou, I.T.; Dimou, A.; Andreou, E.; Kostakis, G.; Sideri, A.; Vitsos, A. Optimization of psoriasis—Like mouse models: A comparative study. bioRxiv, 2020; ahead of print. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.; Kim, D.H.; Shin, J.U. In vitro models mimicking immune response in the skin. Yonsei Med. J. 2021, 62, 969–980. [Google Scholar] [CrossRef]
- Larouche, D.; Cantin-Warren, L.; Desgagné, M.; Guignard, R.; Martel, I.; Ayoub, A.; Lavoie, A. Improved Methods to Produce Tissue-Engineered Skin Substitutes Suitable for the Permanent Closure of Full-Thickness Skin Injuries. Biores. Open Access 2016, 5, 320–329. [Google Scholar] [CrossRef]
- Gu, L.H.; Coulombe, P.A.; Coulombe, P.A. Keratin function in skin epithelia: A broadening palette with surprising shades. Curr. Opin. Cell Biol. 2007, 19, 13–23. [Google Scholar] [CrossRef]
- Mildner, M.; Jin, J.; Eckhart, L.; Kezic, S.; Gruber, F.; Barresi, C.; Stremnitzer, C.; Buchberger, M.; Mlitz, V.; Ballaun, C.; et al. Knockdown of filaggrin impairs diffusion barrier function and increases UV sensitivity in a human skin model. J. Investig. Dermatol. 2010, 130, 2286–2294. [Google Scholar] [CrossRef] [Green Version]
- Furue, M. Regulation of Skin Barrier Function via Competition between AHR Axis versus IL-13/IL-4-JAK-STAT6/STAT3 Axis: Pathogenic and Therapeutic Implications in Atopic Dermatitis. J. Clin Med. 2020, 9, 3741. [Google Scholar] [CrossRef] [PubMed]
- Steinert, P.M.; Cantieri, J.S.; Tellert, D.C.; Lonsdale-Ecclest, J.D.; Dalet, B.A. Characterization of a class of cationic proteins that specifically interact with intermediate filaments. Proc. Natl. Acad. Sci. USA 1981, 78, 4097–4101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewer, M.G.; Anderson, E.A.; Pandya, R.P.; Benedetto, A.; Yoshida, T.; Hilimire, T.A.; Martinez-Sobrido, L.; Beck, L.A.; Miller, B.L. Peptides Derived from the Tight Junction Protein CLDN1 Disrupt the Skin Barrier and Promote Responsiveness to an Epicutaneous Vaccine. J. Investig. Dermatol. 2020, 140, 361–369.e3. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, K.; Asahina, R.; Nishida, H.; Kamishina, H.; Maeda, S. Expression of ZO-1 and claudin-1 in a 3D epidermal equivalent using canine progenitor epidermal keratinocytes. Vet. Dermatol. 2018, 29, 288-e98. [Google Scholar] [CrossRef]
- York, M.; Griffiths, H.A.; Whittle, E.; Basketter, D.A. Evaluation of a human patch test for the identification and classification of skin irritation potential. Contact Dermat. 1996, 34, 204–2012. [Google Scholar] [CrossRef]
- Lavoie, A.; Fugère, C.; Beauparlant, A.; Goyer, B.; Larouche, D.; Paquet, C.; Desgagné, M.; Sauvé, S.; Robitaille, H.; Dunnwald, M.; et al. Human epithelial stem cells persist within tissue-engineered skin produced by the self-assembly approach. Tissue Eng. (Part A) 2013, 19, 1023–1038. [Google Scholar] [CrossRef]
- Climov, M.; Climov, E.; Farkash, E.A.; Quiao, F.J.; Rousseau, C.F.; Dong, S.; Zawadzka, A.; Racki, W.J.; Al-Musa, A.; Sachs, D.H.; et al. Bioengineered self-assembled skin as an alternative to skin grafts. Plast. Reconstr. Surg.-Glob. Open 2016, 4, e731. [Google Scholar] [CrossRef]
- Germain, L.D.; Larouche, B.; Nedelec, I.P.; Duranceau, L.; Bortoluzzi, P.; Cloutier, C.B.; Genest, L.; Caouette-Laberge, L.; Duman, A.; Bussiere, A.; et al. Autologous bilayered self-assembled skin substitutes (Sasss) as permanent grafts: A case series of 14 severely burned patients indicating clinical effectiveness. Eur. Cells Mater. 2018, 36, 128–141. [Google Scholar] [CrossRef]
- Perera, G.K.; Meglio, P.D.; Nestle, F.O. Psoriasis. Annu. Rev. Pathol. Mech. Dis. 2012, 7, 385–422. [Google Scholar] [CrossRef]
- Nestle, F.O.; Meglio, P.D.; Qin, J.Z.; Nickoloff, B.J. Skin immune sentinels in health and disease. Nat. Rev. Immunol. 2009, 9, 679–691. [Google Scholar] [CrossRef] [Green Version]
- Jean, J.; Lapointe, M.; Soucy, J.; Pouliot, R. Development of an in vitro psoriatic skin model by tissue engineering. J. Dermatol. Sci. 2009, 53, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Pouliot, B.C.; Zaniolo, K.; Guérin, S.L.; Pouliot, R. Tissue-engineered human psoriatic skin supplemented with cytokines as an in vitro model to study plaque psoriasis. Regen. Med. 2016, 11, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Roy, B.; Simard, M.; Lorthois, I.; Bélanger, A.; Matheux, M.; Duque-Fernandes, A.; Rioux, G. In vitro models of psoriasis. In Skin Tissue Models; Elsevier Inc.: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Bogaard, E.H.; Tjabringa, G.S.; Joosten, I.; Vonk-Bergers, M.; Rijssen, E.; Tijssen, H.J.; Erkens, M.; Schalkwijk, J.; Koenen, H.J.P.M. Crosstalk between keratinocytes and T cells in a 3D microenvironment: A model to study inflammatory skin diseases. J. Investig. Dermatol. 2014, 134, 719–727. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.U.; Abaci, H.E.; Herron, L.; Guo, Z.; Sallee, B.; Pappalardo, A.; Jackow, J.; Wang, E.H.C.; Doucet, Y.; Christiano, A.M. Recapitulating T cell infiltration in 3D psoriatic skin models for patient-specific drug testing. Sci. Rep. 2020, 10, 4123. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Order | Test Chemicals | Formulation | UN GHS Cat. |
|---|---|---|---|
| 1 | 1-Bromochlorobutane- | L | No |
| 2 | Diethyl phthalate | L | No |
| 3 | 1-Naphthalene acetic acid | S | No |
| 4 | Propylene glycol | L | No |
| 5 | Isopropanol | L | No |
| 6 | 4-Methyl-thio-benzaldehyde | L | No |
| 7 | Methyl stearate | S | No |
| 8 | Mineral oil | L | No |
| 9 | Hexyl salicylate | L | No |
| 10 | trans-Cinnamaladehyde | L | No |
| 11 | 1-decanol | L | R38 |
| 12 | 1-Bromohexane | L | R38 |
| 13 | 5% Potassium hydroxide (5% aq.) | L | R38 |
| 14 | Di-n-propyl disulfide | L | R38 |
| 15 | 2-Benzyloxyethanol | L | R38 |
| 16 | Heptanal | L | R38 |
| 17 | Tetrachloroethylene | L | R38 |
| 18 | Decanoic acid | B | R38 |
| 19 | Alpha-terpineol | B | R38 |
| 20 | Butyl Methacrylate | L | R38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mok, B.R.; Shon, S.-J.; Kim, A.R.; Simard-Bisson, C.; Martel, I.; Germain, L.; Kim, D.H.; Shin, J.U. Structural and Functional Validation of a Full-Thickness Self-Assembled Skin Equivalent for Disease Modeling. Pharmaceutics 2022, 14, 1211. https://doi.org/10.3390/pharmaceutics14061211
Mok BR, Shon S-J, Kim AR, Simard-Bisson C, Martel I, Germain L, Kim DH, Shin JU. Structural and Functional Validation of a Full-Thickness Self-Assembled Skin Equivalent for Disease Modeling. Pharmaceutics. 2022; 14(6):1211. https://doi.org/10.3390/pharmaceutics14061211
Chicago/Turabian StyleMok, Bo Ram, Su-Ji Shon, A Ram Kim, Carolyne Simard-Bisson, Israël Martel, Lucie Germain, Dong Hyun Kim, and Jung U Shin. 2022. "Structural and Functional Validation of a Full-Thickness Self-Assembled Skin Equivalent for Disease Modeling" Pharmaceutics 14, no. 6: 1211. https://doi.org/10.3390/pharmaceutics14061211