Microbial Contamination of Dental Unit Waterlines and Potential Risk of Infection: A Narrative Review


Department of Health Sciences, University of Genova, 16132 Genova, Italy
*
Author to whom correspondence should be addressed.
Pathogens 2020, 9(8), 651; https://doi.org/10.3390/pathogens9080651
Submission received: 17 July 2020
/
Revised: 9 August 2020
/
Accepted: 12 August 2020
/
Published: 13 August 2020
(This article belongs to the Special Issue Healthcare-Associated Infections)
{kind=link}
{kind=link}
{kind=link}
Abstract
:Several studies have revealed that dental unit waterlines (DUWLs) are often contaminated by large numbers of various micro-organisms (bacteria, fungi, protozoa, viruses). Microbial contamination in DUWLs may originate from the mains water piped into the dental unit, the suck-back of patients’ saliva into the line due to the lack of adequate valves, and contamination from bottled water systems. Some of the main determinants of microbial contamination in DUWLs are: a very small lumen size (0.5–2 mm) of the tubing used, high surface-to-volume ratio (6:1), low throughput and the materials of which the tubing is made, water stagnation outside of working hours. The environmental conditions present inside the conduits of the dental unit may facilitate the proliferation of micro-organisms and the consequent formation of biofilm on the interior surface of the pipes of DUWLs. During the use of handpieces, particularly high-speed rotating instruments, a spray is thrown up in the form of aerosols or spatters containing biological material (saliva, blood and dental plaque) and micro-organisms. This means that the health of both dental staff and patients could be at risk of infection. The risk of cross-infections in dental settings can be tackled by implementing combined interventions to prevent the contamination of DUWLs.
1. Introduction
1.1. Background
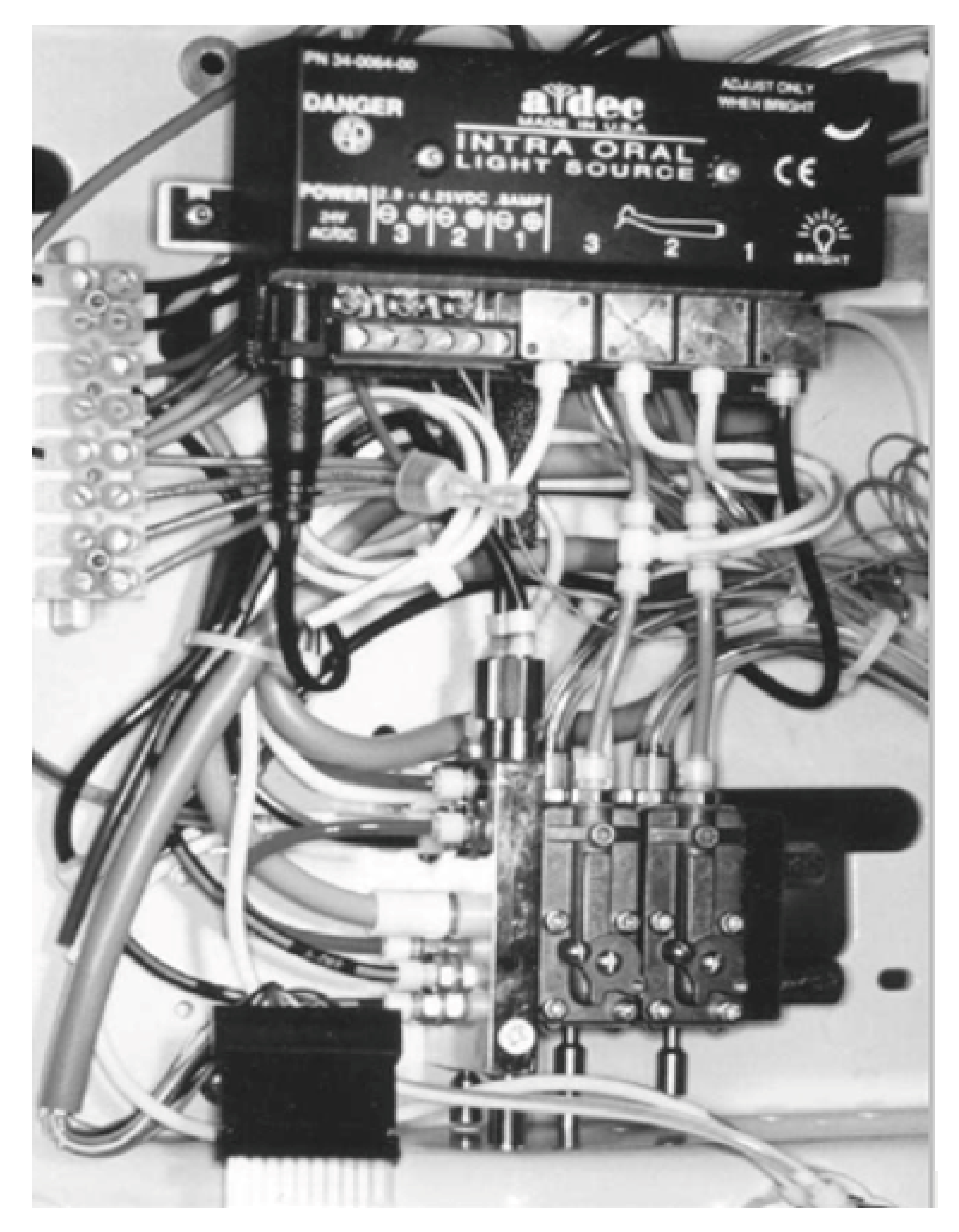
Dental treatment requires various essential services, such as electric power, suction, air and water supply, which are provided by the dental unit. During treatment, high-speed rotating instruments and ultrasonic scalers generate heat, which can damage dental tissues. To avoid overheating, these instruments are cooled by water, which may be supplied by the municipal water-main or by tanks (bottles) directly connected to the dental unit. This water, which is also used to irrigate the operating field, travels to the instruments of the dental unit through a complex network of narrow-bore plastic tubes, valves and connectors: the so-called dental unit waterlines (DUWLs) [1]. This network conveys water to the high-speed handpiece, air/water syringe, and ultrasonic scaler (Figure 1), in order to cleanse, cool and rinse both the site of intervention and the equipment needed for work on soft and hard tissues [2,3].
Several studies have revealed that DUWLs are often contaminated by large numbers of various micro-organisms (bacteria, fungi, protozoa, viruses) [4,5,6,7]. Indeed, copious evidence of dental unit water contamination has accumulated since the 1960s, when water from DUWLs was first found to contain micro-organisms in concentrations ranging from 104 to 106 colony-forming units (CFU)/mL [8].
The Guidelines on infection control in dental healthcare settings issued by the US Centers for Disease Control and Prevention (CDC) recommend that the level of heterotrophic plate counts (HPCs) in dental unit water should not exceed 500 CFU/mL [9]. Moreover, the American Dental Association (ADA) has set a limit of ≤200 CFU/mL on the heterotrophic bacterial load in water from dental unit waterlines [10]. In the EU, however, there is no current guideline regarding DUWLs, though in some countries the drinking water standard is used as a reference [11].
Microbial contamination in DUWLs may originate from the mains water piped into the dental unit, the suck-back of patients’ saliva into the line due to the lack of adequate valves, and contamination from bottled water systems [12,13]. Thus, dental waterlines may be contaminated not only by water-borne environmental microorganisms, but also by germs from the oral cavity of the patient, which is host to microbes that belong to different species, such as Porphyromonas gingivalis, one of the bacteria implicated in the biofilm formation of bacterial plaque [14,15].
Indeed, dental turbines rotate at high speed and, during the slowdown phase, exert an aspirating effect, which causes organic material present on the tip of the instrument to be drawn inside, thereby giving rise to the phenomenon of back-contamination of the water supply [16]. This contaminated water may contain bacterial loads that are thousands of times greater than the limits set on drinking water. Thus, even the most scrupulous sterilization of the handpieces of the dental unit will be in vain if these instruments are connected to a contaminated water supply.
Some of the main determinants of microbial contamination in DUWLs are: a very small lumen size (0.5–2 mm) of the tubing used, high surface-to-volume ratio (6:1), low throughput and the materials of which the tubing is made. Indeed, during working hours, the water flows, albeit for brief periods; outside of working hours, however, the water stagnates. Together, these factors offer the micro-organisms present in the water ample opportunities to build up a strong matrix-encapsulated biofilm that can resist antimicrobial treatments [1,11,12,17,18,19]. This means that the health of both dental staff and patients could be at risk if water is not appropriately treated [20].
1.2. Aim
The aim of this narrative review is to describe microbial contamination of dental unit waterlines and the potential risk of infection. Searches were made in PubMed.gov and Scopus for publications regarding dental unit waterlines, DUWLs, related to microbial contamination, biofilm and infection risk prevention.
2. Microbial Contamination of DUWLs and Biofilms
Many micro-organisms (bacteria, viruses, fungi) have been found in water samples from DUWLs: Streptococcus mitis, Streptococcus salivarius, enterococci, Staphylococcus cohnii, Staphylococcus warneri A, Klebsiella (Enterobacter) aerogenes, Bacillus subtilis, Enterococcus faecalis, Enterobacter cloacae, Pseudomonas aeruginosa, Legionella pneumophila, Serratia marcescens, Aeromonas spp., Acinetobacter spp., Flavobacterium spp., Moraxella spp., Cladosporium spp., Pseudomonas spp., Legionella spp., etc. [4,5,6,7].
Abdouchakou et al. [21] reported the pattern of microbial contamination of waterlines over 6.5 years in a dental healthcare center in which 61 dental unit waterlines (DUWLs) were connected to the same water supply. One clone of P. aeruginosa and 2 clones of Achromobacter sp. gradually colonized all the DUWLs; the last colonization by P. aeruginosa ST309 prompted the closure of the dental care center. Moreover, confirmation of the literature reports was provided by a recent study [22] which found Legionella and P. aeruginosa contamination in 32% (6/19) and 68% (13/19), respectively, of water samples from DUWLs. In addition, the presence of Gram-negative bacteria in DUWLs can lead to the production of endotoxins (LPS) in the water and air of a dental surgery [23].
Fungi have also been found in water from dental units. In a study conducted by Mazari et al. [24], 18 dental waterlines were analyzed for the presence of yeasts on their internal surfaces. Of the 18 DUWLs studied, 10 were contaminated (55.56%). Candida albicans, Candida guilliermondii and Candida glabrata and two species of non-Candida, Rhodotorula spp. and Trichosporon spp., were identified.
In addition to bacteria, fungi and viruses, protozoa such as free-living amoebae have been isolated from DUWLs [25,26]. These can act as a reservoir for micro-organisms (e.g., Legionella spp. Pseudomonas spp. etc.) or as pathogens in their own right [27,28].
In our previous study [29], we assessed the level of contamination by bacteria and amoebae in 30 dental units, all of which were supplied directly by the municipal water network and no additional disinfection systems were used in the facilities. The mean concentration of HPCs at 22 and 36 °C was 1168.53 CFU/mL and 827.90 CFU/mL respectively, while the concentration of P. aeruginosa proved to be of 25.13 CFU/100 mL. Of the 30 units, 26.67% displayed a concentration of ≥103 CFU/L of L. pneumophila; about 23% of cases involved L. pneumophila sg 1. The study revealed that the water in the DUWLs contained considerably higher concentrations of micro-organisms than the input water supply, thereby confirming the role of the water system inside the dental unit in increasing microbial contamination, especially in the absence of proper management of the water and healthcare risk.
Previous studies have found a wide range in the rate of recovery of Legionella contamination of DUWLs, from 0% to 100% of DUWL systems [30,31] including Legionella pneumophila serogroup 1 [32], reaching levels as high as 105 colony-forming units per milliliter [30,33,34]. The presence and concentration of Legionella contamination in DUWLs varies according to the features of the water supply system, the design and model of the dental unit, and the methods of disinfection used [30].
3. Formation of Biofilms in DUWLs
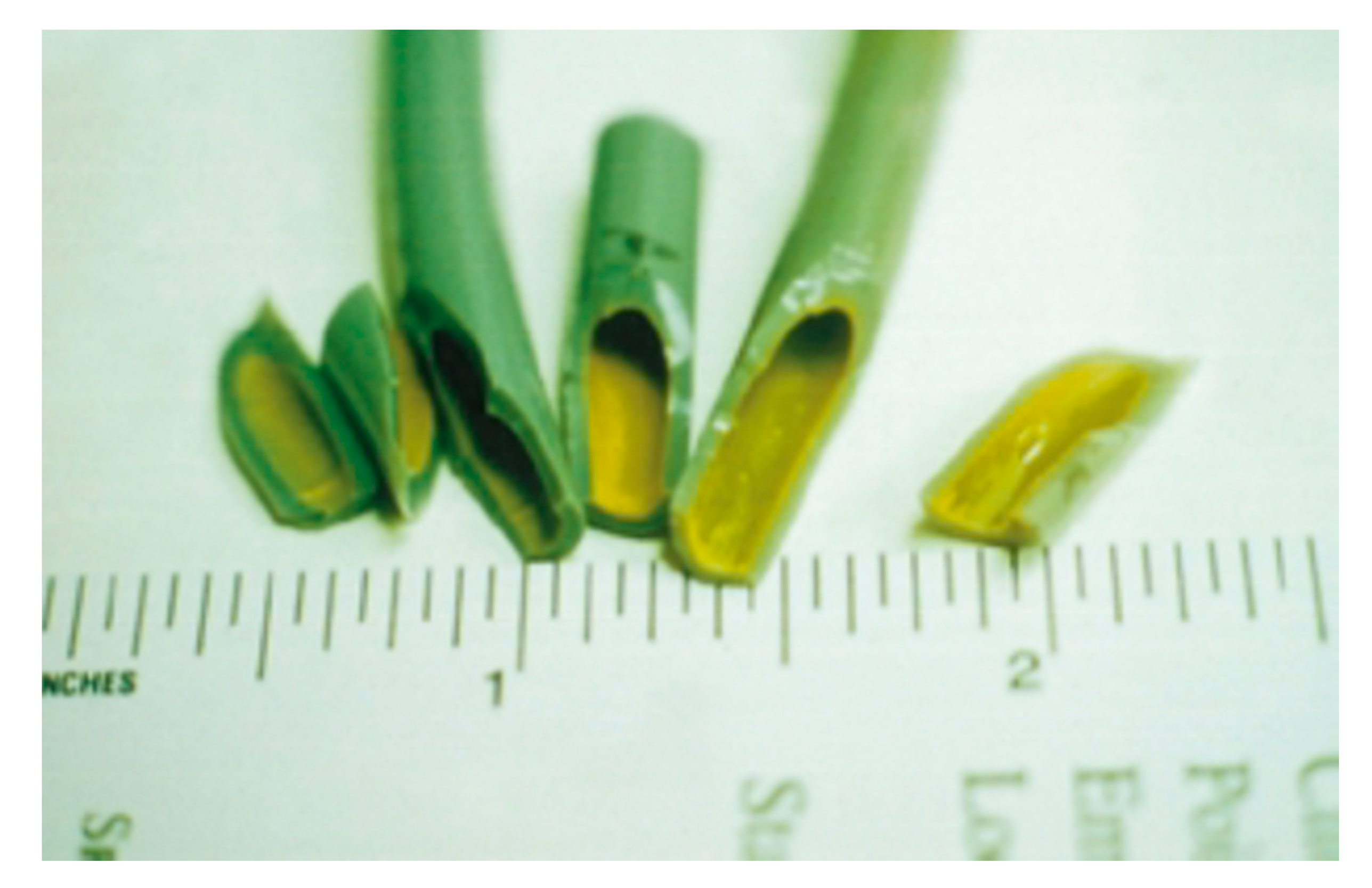
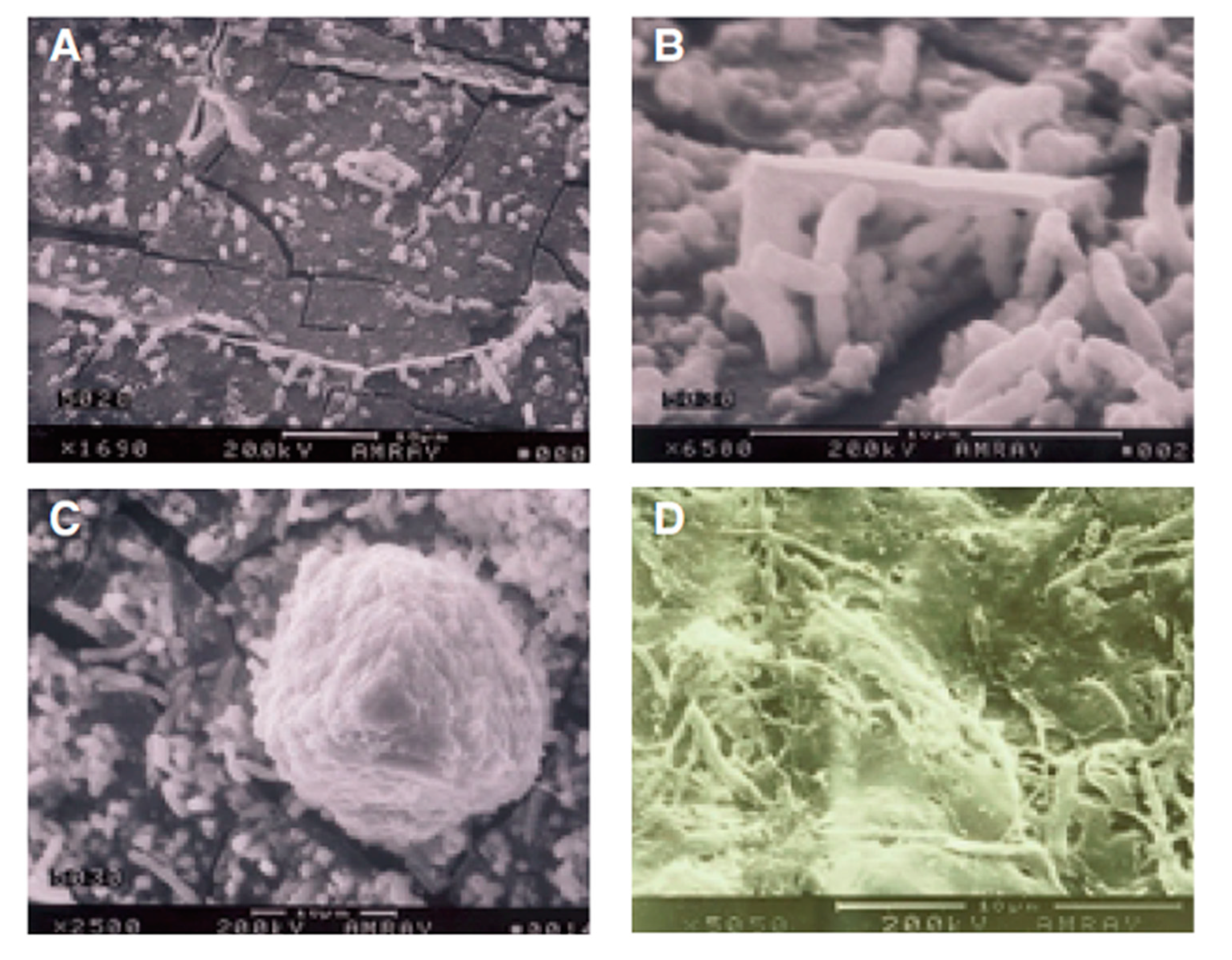
The proliferation of micro-organisms and the consequent formation of biofilm on the interior surface of the pipes of DUWLs (Figure 2 and Figure 3) may be facilitated by the environmental conditions present inside the conduits of the dental unit.
The formation of biofilm in DUWLs is a universal problem, as is indicated by the results of many studies in several countries. Biofilms constitute the main reservoir for continued contamination of water supply systems [35]. They are made up of bacteria that adhere to the surface of a substrate and which are embedded in a matrix of extracellular polymeric substances (EPS) [36]. As EPS may constitute 50–90% of the total carbon present in biofilms, they can therefore be regarded as the primary matrix. Although their chemical and physical properties vary, EPS are chiefly composed of polysaccharides and proteins, which form highly hydrated matrices. The micro-organisms in the biofilm can maintain a stable synergy among different species, thereby orchestrating the degradation of complex substrates. Inside the biofilm, micro-environments are created which are characterized by physical and chemical gradients in which a fundamental role is played by the EPS. As the matrix can sequester nutrients from the environment, it plays a part in the general strategy for survival in oligotrophic conditions. The micro-organisms contained in the biofilm display resistance to biocidal agents that is 2–3-orders of magnitude greater than that of non-adherent microbial cells [37].
Thus, biofilms form as a result of a process of microbial attachment to the substrate, cell proliferation and matrix production, which may be followed by detachment [38,39,40,41] (Figure 3). Indeed, during the normal use of the dental unit, portions of biofilm may detach from the substrate and be conveyed to the external environment through the sprays of handpieces.
Tall et al. [42] conducted a 6-month study of bacterial colonization and biofilm formation in plastic waterlines connected to dental air/water syringes. During the period of observation, changes in biofilm flora were observed by means of both scanning electron microscopy and bacteriological culture. After 6 months, several layers of morphologically different micro-organisms were detected, which completely covered the lumen. The authors presented the succession of species in order of appearance, as cultured. Early colonizers were mainly Pseudomonas spp.; later, Pasteurella, Moraxella, Ochrohactrum, Aeromonas spp., Flavobacterium and Acinetobacter spp. were observed.
4. Risk of Infection from DUWLs
The risk of infection resulting from dental treatment is a public health concern, especially since such treatment is extremely common in the population and increasing numbers of medically compromised or immunocompromised individuals (for various reasons: chronic diseases, AIDS, cystic fibrosis, immunosuppressive therapy for organ transplantation and chemotherapy, etc.) are receiving regular dental treatment.
Fortunately, few published studies concern cases of infection resulting from dental care. Nevertheless, there is a risk that large numbers of pathogenic micro-organisms may be swallowed, inhaled or inoculated into oral wounds during dental treatment, potentially giving rise to colonization or infection [43].
In dental settings, infections may spread directly through contact with blood, oral fluids or other secretions; indirectly, through contact with contaminated instruments, equipment or environmental surfaces; and through inhalation or contact with micro-organisms present in aerosols or spatters of oral and respiratory fluids or in dental unit waterlines [23,44]. Moreover, back-pressure phenomena created by rotating instruments play a major role in the retrograde aspiration of contaminated fluids from the oral cavity into DUWLs. These fluids may then be sprayed onto the mucosae of the next patient treated, even if the handpiece has been correctly replaced with a sterilized one and sterile water is used for irrigation [45]. Thus, during the use of handpieces, particularly high-speed rotating instruments, a spray is thrown up in the form of aerosols or spatters containing biological material (saliva, blood and dental plaque) and micro-organisms [46,47]. This cloud, which comes directly into contact with dental staff and patients, is made up of material that partly originates from the treatment site and partly comes from dental unit waterlines. The aerosol produced can remain airborne for long periods and may be inhaled by dental staff and patients; it then tends to sediment, contaminating surfaces, operating equipment, etc., thereby increasing the risk of infection [44,48].
Anyway, some methods can be used to reduce aerosols contaminating load, such as mouth-rinses with chlorhexidine, cetylpyridinium chloride, hydrogen peroxide and other bactericide and virucide agents, the use of the dental dam and of the high-volume evacuator.
The aerosols thrown up by the rotating instruments used in dentistry were analyzed in a study carried out by Miller; this revealed that particles ranging from 0.06 to 13 µm in diameter, and with a half-life of 35 min to 17 h, were produced [47,49].
Rautemaa et al. [50] determined both how far airborne bacteria travelled during dental treatment and the level of contamination at various distances. To this end, they collected fall-out samples on blood agar plates situated at six points at distances of 0.5–2 m from the patient. Significant contamination was recorded at all sampling points when high-speed instruments were used (mean concentration on surfaces per hour: 1119 CFU/m2/h at >1.5 m from the patient).
Instead, Zemouri et al. [51] in a more recent study, have found a contamination up to 655 CFU/plate/30 min.
Prospero et al. [52] evaluated the sedimenting bacterial load in dental surgeries during routine procedures. The surfaces with the highest levels of contamination were, in descending order, dental healthcare workers’ surgical masks, lamps, areas near spittoons, and mobile trays. Positive samples taken from the various surfaces presented Streptococcus species (42%), Staphylococcus species (41%) and Gram-negative bacteria (17%).
With regard to Gram-negative bacteria, Pseudomonas aeruginosa is frequently studied in waterlines because of its association with disease in susceptible hosts (e.g., subjects with cystic fibrosis). These pathogens are easily transmitted and originate from the main water pipes. A study conducted by Jensen et al. [53] assessed the presence of P. aeruginosa in samples of water taken from triple-function syringes, turbines, handpiece contra-angles and ultrasonic scalers during dental treatment sessions attended by cystic fibrosis patients. In addition, samples of expectorate taken from each patient affected by cystic fibrosis (CF) were examined for the presence of P. aeruginosa each month, before and after each treatment session. At least in one case, genotypically identical (RFLP, pulsed-field gel electrophoresis) P. aeruginosa strains were found both in water from the dental equipment and in the CF patient’s sputum. In such patients, exposure to P. aeruginosa must be avoided, as this micro-organism is the primary cause of lung destruction and premature death in these patients [54].
Other Gram-negative bacteria frequently encountered in DUWLs are Legionellae. This micro-organism grows at temperatures of 25–50 °C, especially in water that is stagnant and rich in sediments, and causes various clinical manifestations, including the form of pneumonia commonly known as Legionnaires’ disease [55,56,57].
Fortunately, there are few documented cases of legionellosis acquired through a dental unit. In one such case, however, an 82-year-old Italian woman died of pneumonia after exposure to Legionella pneumophila serogroup 1, which was detected in the DUWL. Molecular typing confirmed the clonal relationship between the clinical and environmental strains [58]. Another case of legionellosis linked to dental treatment was reported in an immunocompromised elderly Swedish man who developed Legionnaires’ disease a few days after a dental check-up. Legionella spp. at a concentration of 2000 CFU/L was isolated from the outlet of the water used for oral rinsing. Isolates from the patient’s sputum, collected by means of bronchoscopy, and from the dental unit were of Legionella pneumophila sg 1, subgroup Knoxville and ST9 [59]. Other species, such as Achromobacter species and mycobacteria, have also been associated with infections from waterlines [23,60].
Exposure to bacteria from DUWLs affects not only patients but also dental staff. The occupational risk of Legionella infection is not a marginal issue, since a high number of individuals could be occupationally exposed [61]. In this regard, higher rates of seropositivity for Legionella antibodies have been found among dental personnel than among the general public [62,63], suggesting that the aerosols generated in dental surgeries are a source of exposure to Legionella spp. Moreover, those who spend more years in dental practice have a higher risk [30].
In 1985, a study performed in a US dental school [63] reported the prevalence of Legionella-specific IgG and IgM antibodies in a dental clinic population consisting of 270 dental school personnel. Subjects were subdivided into two groups: those exposed for over two years (Group One) and those exposed for one year or less (Group Two). A control group of 67 individuals without previous clinic exposure was randomly selected from the regional population (Group Three). The incidence of IgG-positivity was highest in Group One (23%), lower in Group Two (16%), and lowest (8%) in Group Three (no exposure to the clinic environment).
Regarding cases of professionally contracted legionellosis, the literature documents only one fatal case of Legionnaires’ disease in an American dentist. This infection was attributed to exposure to DUWL aerosols. L. pneumophilia and L. longbeachae were detected in the dentist’s lung tissue and in the DUWLs; however, the dentist’s domestic water supply also presented Legionella spp., albeit at very low levels [22,64].
Given that the literature data indicate ample contamination of dental unit waterlines by Legionella, it is recommended that sampling for the detection of this micro-organism be carried out every time that a case of disease occurs, and at least once a year if risk-minimization measures are not implemented [65].
5. Treatment of DUWLs
The risk of cross-infections in dental settings can be tackled by implementing appropriate systems of proven efficacy. There are different chemical, physical or chemo-physical treatment systems of DUWLs, (e.g., peracetic acid, gluteraldehyde, chlorhexidine, chlorine dioxide, filtration, flushing, reverse osmosis, etc.), [2,16].
According to the guidelines of Italian Health Ministry for the prevention and control of legionellosis [65], in order to reduce microbial contamination and/or the formation of biofilm in DUWLs, the following recommendations should be implemented:
- Any sections excluded from the flow currents should be eliminated from the network.
- Install anti-stagnation devices to keep the water circulating continuously, particularly during non-working hours.
- Supply the network with sterile solutions, after isolating it from the main water supply.
- Disinfect the water by means of continuous or discontinuous treatments. These latter, which may be carried out periodically or between one patient and the next, prevent chemical contamination of the operating field, reduce the exposure of staff and minimize the risk of selecting resistant micro-organisms; however, they require a greater commitment of resources and attention than continuous treatments.
- All devices that connect to a waterline and enter patients’ mouths, such as handpieces, ultrasonic scalers and air/water syringes, should be switched on and flushed through before use: for at least two minutes at the beginning of each working day and for at least 20–30 s before each patient is treated.
- Filters (≤0.2 μm) that can trap micro-organisms coming from inside the water supply network should be installed immediately upstream of handpieces.
In addition, in the case of invasive surgical procedures, only sterile water should be used, and the supply network should also be sterile. If sterility of the dental unit’s supply network cannot be guaranteed, a bypass system should be created and disposable sterile devices, or sterilizable devices, should be used [9,65].
Various international agencies also recommend implementation of these preventive measures, the efficacy of which has been demonstrated by several scientific studies [6,45,66,67].
The Centers for Disease Control and Prevention (CDC) [9] recommend that manufacturers should provide dental units with a separate reservoir, typically a container of about 1-liter capacity, from which tap water, deionized water and/or distilled water can be fed to the drill in order to cool it. Moreover, these separate reservoirs are also better suited for the input of biocides. This measure was introduced by the CDC in dentistry in order to supply safe treatment water, although some working dental units are still fed directly by municipal water [7]. In these latter cases, it is even more important to adopt the various systems for preventing microbial contamination, such as, for example, the use of handpieces and turbines fitted with anti-reflux valves; these valves are triggered when the turbine stops and prevent liquids, and hence also micro-organisms, from being aspirated when rotating instruments are used.
Particularly recommended by the CDC [9] is flushing, which should always be carried out for 20–30 s after each patient is treated. This should be done for all devices that connect to a waterline and enter patients’ mouths, such as handpieces, ultrasonic scalers and air/water syringes. This procedure is intended to physically flush outpatient material that might have entered the turbine, air or waterlines. A recent study [6] evaluated the impact of flushing on bacterial contamination in dental unit waterlines. Water samples were collected (before flushing, 1 min post-flushing, and 3 min post-flushing) from 24 clinics (Group A: no disinfection, Group B: citric acid disinfectant). High-speed drill handpiece (HP) lines, air/water syringes (WS) and oral rinse (OR) were monitored. All sources tested (HP, OR and WS) from Group A units showed significant levels of bacterial contamination, while no contamination was observed in the water samples from Group B clinics. The bacterial contamination of WS and HP samples was significantly lower 3 min after flushing than before flushing, but was still higher than the recommended limit of 500 CFU/mL. This suggests that flushing alone is not sufficient and that other strategies are required in order to improve water quality in dental practices.
DUWL biofilms may be treated with biocides either periodically or by means of continuous treatment systems. Continuous disinfection systems are more effective and easier to comply with, and require less organization. The chemical agents currently used for disinfecting DUWLs include chlorine dioxide, sodium hypochlorite, hydrogen peroxide and chlorhexidine gluconate. Optimal disinfectant products should be economical and have few side-effects on dental units and the oral cavity. Disinfectants containing sodium hypochlorite or hydrogen peroxide, which have shown the greatest efficacy, are, however, reported to have side-effects, such as corrosion of dental equipment, clogging of the DUWLs, and stimulation of the oral mucosa [68]. Finally, because disinfectants are tested in vitro for registration and the construction features of DUWLs vary widely, field tests and disinfection protocols are tailored to individual devices. It is therefore unusual to find a disinfection protocol that is effective in all cases [31].
In conclusion, reducing the risk of infection in dental-care settings depends on the implementation of combined interventions to prevent the contamination of DUWLs. Equally important, however, are the scheduled technical maintenance of dental units and the monitoring of the quality of DUWL water. Moreover, recommended transmission-based precautions should be incorporated into daily practice, in order to minimize aerosol production through the use of high-velocity air evacuation and air conditioning systems.
Author Contributions
M.L.C. and A.M.S. designed and developed the framework, did literature searches and wrote the manuscript; M.S. contributed to the editing and quality control and helped with literature review. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hoogenkamp, M.A.; Brandt, B.W.; de Soet, J.J.; Crielaard, W. An in-vitro dynamic flow model for translational research into dental unit water system biofilms. J. Microbiol. Methods 2020, 171, 105879. [Google Scholar] [CrossRef]
- Pawar, A.; Garg, S.; Mehta, S.; Dang, R. Breaking the Chain of Infection: Dental Unit Water Quality Control. J. Clin. Diagn. Res. 2016, 10, ZC80–4. [Google Scholar] [CrossRef]
- FDI World Dental Federation. FDI policy statement on Dental Unit Water Systems and microbial contamination: Adopted by the FDI General Assembly: September 2016, Poznan, Poland. Int. Dent. J. 2017, 67, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Szymańska, J.; Sitkowska, J.; Dutkiewicz, J. Microbial contamination of dental unit waterlines. Ann. Agric. Environ. Med. 2008, 15, 173–179. [Google Scholar] [PubMed]
- Wirthlin, M.R.; Marshall, G.W., Jr.; Rowland, R.W. Formation and decontamination of biofilms in dental unit waterlines. J. Periodontol. 2003, 74, 1595–1609. [Google Scholar] [CrossRef] [PubMed]
- Alkhulaifi, M.M.; Alotaibi, D.H.; Alajlan, H.; Binshoail, T. Assessment of nosocomial bacterial contamination in dental unit waterlines: Impact of flushing. Saudi Dent. J. 2020, 32, 68–73. [Google Scholar] [CrossRef]
- Lal, S.; Singhrao, S.K.; Achilles-Day, U.E.; Morton, L.H.; Pearce, M.; Crean, S. Risk Assessment for the Spread of Serratia marcescens Within Dental-Unit Waterline Systems Using Vermamoeba vermiformis. Curr. Microbiol. 2015, 71, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Blake, G. The incidence and control of infection in dental spray reservoirs. Br. Dent. J. 1963, 115, 412–416. [Google Scholar]
- Kohn, W.G.; Collins, A.S.; Cleveland, J.L.; Harte, J.A.; Eklund, K.J.; Malvitz, D.M. Centers for Disease Control and Prevention (CDC). Guidelines for infection control in dental health-care settings-2003. MMWR Recomm. Rep. 2003, 52, 1–61. [Google Scholar]
- American Dental Association. ADA Statement on Dental unit waterlines. J. Am. Dent. Assoc. 1996, 127, 185–186. [Google Scholar] [CrossRef]
- Walker, J.T.; Marsh, P.D. Microbial biofilm formation in DUWS and their control using disinfectants. J. Dent. 2007, 35, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.K.; Mittal, S.; Kaur, P. Dental unit waterline management: Historical perspectives and current trends. J. Investig. Clin. Dent. 2012, 3, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Volgenant, C.M.C.; Persoon, I.F. Microbial water quality management of dental unit water lines at a dental school. J. Hosp. Infect. 2019, 103, e115–e117. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L.; Cervino, G.; Laino, L.; D’Amico, C.; Mauceri, R.; Tozum, T.F.; Gaeta, M.; Cicciù, M. Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review. Dent. J. 2019, 7, 114. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L. We Do Not Eat Alone: Formation and Maturation of the Oral Microbiota. Biology 2020, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M. Water Contamination Risks at the Dental Clinic. Biology 2020, 9, 43. [Google Scholar] [CrossRef] [Green Version]
- Barbeau, J.; Nadeau, C. Dental unit waterline microbiology: A cautionary tale. J. Can. Dent. Assoc. 1997, 63, 775–779. [Google Scholar]
- Shajahan, I.F.; Kandaswamy, D.; Lakshminarayanan, L.; Selvarajan, R. Substantivity of hypochlorous acid-based disinfectant against biofilm formation in the dental unit waterlines. J. Conserv. Dent. 2017, 20, 2–5. [Google Scholar] [CrossRef]
- Sedlata Juraskova, E.; Sedlackova, H.; Janska, J.; Holy, O.; Lalova, I.; Matouskova, I. Legionella spp. in dental unit waterlines. Bratisl. Lek. Listy 2017, 118, 310–314. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Atlanta GA Centers Disease Control Prevention, US Dept of Health and Human Services; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2016. [Google Scholar]
- Abdouchakour, F.; Dupont, C.; Grau, D.; Aujoulat, F.; Mournetas, P.; Marchandin, H.; Parer, S.; Gibert, P.; Valcarcel, J.; Jumas-Bilak, E. Pseudomonas aeruginosa and Achromobacter sp. clonal selection leads to successive waves of contamination of water in dental care units. Appl. Environ. Microbiol. 2015, 81, 7509–7524. [Google Scholar] [CrossRef] [Green Version]
- Tuvo, B.; Totaro, M.; Cristina, M.L.; Spagnolo, A.M.; di Cave, D.; Profeti, S.; Baggiani, A.; Privitera, G.; Casini, B. Prevention and Control of Legionella and Pseudomonas spp. Colonization in Dental Units. Pathogens 2020, 9, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volgenant, C.M.C.; de Soet, J.J. Cross-transmission in the Dental Office: Does This Make You Ill? Curr. Oral Health Rep. 2018, 5, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazari, W.; Boucherit-Otmani, Z.; El Haci, I.A.; Ilahi, A.; Boucherit, K. Risk assessment for the spread of Candida sp. in dental chair unit waterlines using molecular techniques. Int. Dent. J. 2018, 68, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Castro-Artavia, E.; Retana-Moreira, L.; Lorenzo-Morales, J.; Abrahams-Sandí, E. Potentially pathogenic Acanthamoeba genotype T4 isolated from dental units and emergency combination showers. Mem. Inst. Oswaldo Cruz 2017, 112, 817–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Retana-Moreira, L.; Abrahams-Sandí, E.; Castro-Artavia, E.; Fernández-Sánchez, A.; Castro-Castillo, A.; Reyes-Batlle, M.; Lorenzo-Morales, J. Isolation and Molecular Characterization of Acanthamoeba Strains from Dental Units in Costa Rica. J. Eukaryot. Microbiol. 2015, 62, 733–736. [Google Scholar] [CrossRef]
- Vanessa, B.; Virginie, M.; Nathalie, Q.; Marie-Hélène, R.; Christine, I. Hartmannella vermiformis can promote proliferation of Candida spp. in tap-water. Water Res. 2012, 46, 5707–5714. [Google Scholar]
- Spagnolo, A.M.; Cristina, M.L.; Casini, B.; Perdelli, F. Legionellapneumophila in healthcare facilities. Rev. Med. Microbiol. 2013, 2, 70–80. [Google Scholar] [CrossRef]
- Spagnolo, A.M.; Sartini, M.; di Cave, D.; Casini, B.; Tuvo, B.; Cristina, M.L. Evaluation of Microbiological and Free-Living Protozoa Contamination in Dental Unit Waterlines. Int. J. Environ. Res. Public Health 2019, 16, 2648. [Google Scholar] [CrossRef] [Green Version]
- Estrich, C.G.; Gruninger, S.E.; Lipman, R.D. Rates and predictors of exposure to Legionella pneumophila in the United States among dental practitioners: 2002 through 2012. J. Am. Dent. Assoc. 2017, 148, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Lauritano, D.; Nardone, M.; Gaudio, R.M.; Candotto, V.; Carinci, F. Risk assessment of colonization of legionella spp. in dental unit waterlines. Oral Implantol. 2017, 10, 283–288. [Google Scholar] [CrossRef]
- Arvand, M.; Hack, A. Microbial contamination of dental unit waterlines in dental practices in Hesse, Germany: A cross-sectional study. Eur. J. Microbiol. Immunol. 2013, 3, 49–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutil, S.; Tessier, S.; Veillette, M.; Laflamme, C.; Mériaux, A.; Leduc, A.; Barbeau, J.; Duchaine, C. Detection of Legionella spp. by fluorescent in situ hybridization in dental unit waterlines. J. Appl. Microbiol. 2006, 100, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Pankhurst, C.L.; Coulter, W.A. Do contaminated dental unit waterlines pose a risk of infection? J. Dent. 2007, 35, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Szymańska, J. Biofilm and dental unit waterlines. Ann. Agric. Environ. Med. 2003, 10, 151–157. [Google Scholar]
- Gusnaniar, N.; Sjollema, J.; Nuryastuti, T.; Peterson, B.W.; van de Belt-Gritter, B.; de Jong, E.D.; van der Mei, H.C.; Busscher, H.J. Structural changes in S. epidermidis biofilms after transmission between stainless steel surfaces. Biofouling 2017, 33, 712–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonadonna, L.; Memoli, G.; Chiaretti, G. Biofilm Formation on Materials into Contact with Water: Hygienic and Technical Aspects; (Rapporti ISTISAN 08/19); Istituto Superiore di Sanita: Rome, Italy, 2008. [Google Scholar]
- Spagnolo, A.M.; Orlando, P.; Perdelli, F.; Cristina, M.L. Hospital water and prevention of waterborne infections. Rev. Med. Microbiol. 2016, 27, 25–32. [Google Scholar] [CrossRef]
- Fux, C.A.; Costerton, J.W.; Stewart, P.S.; Stoodley, P. Survival strategies of infectious biofilms. Trends Microbiol. 2005, 13, 34–40. [Google Scholar] [CrossRef]
- Sauer, K.; Camper, A.K.; Ehrlich, G.D.; Costerton, J.W.; Davies, D.G. Pseudomonas aeruginosa displays multiple phenotypes during development as a biofilm. J. Bacteriol. 2002, 184, 1140–1154. [Google Scholar] [CrossRef] [Green Version]
- Mills, S.E. The dental unit waterline controversy: Defusing the myths, defining the solutions. J. Am. Dent. Assoc. 2000, 131, 1427–1441. [Google Scholar] [CrossRef] [Green Version]
- Tall, B.D.; Williams, H.N.; George, K.S.; Gray, R.T.; Walch, M. Bacterial succession within a biofilm in water supply lines of dental air-water syringes. Can. J. Microbiol. 1995, 41, 647–654. [Google Scholar] [CrossRef]
- Barbot, V.; Amélie Robert, A.; Rodier, M.H.; Imbert, C. Update on infectious risks associated with dental unit waterlines. FEMS Immunol. Med. Microbiol. 2012, 65, 196–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristina, M.L.; Spagnolo, A.M.; Sartini, M.; Dallera, M.; Ottria, G.; Perdelli, F.; Orlando, P. Investigation of organizational and hygiene features in dentistry: A pilot study. J. Prev. Med. Hyg. 2009, 50, 175–180. [Google Scholar] [PubMed]
- Artini, M.; Scoarughi, G.L.; Papa, R.; Dolci, G.; de Luca, M.; Orsini, G.; Pappalardo, S.; Costerton, J.W.; Selan, L. Specific anti cross-infection measures may help to prevent viral contamination of dental unit waterlines: A pilot study. Infection 2008, 36, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Cristina, M.L.; Spagnolo, A.M.; Sartini, M.; Dallera, M.; Ottria, G.; Lombardi, R.; Perdelli, F. Evaluation of the risk of infection through exposure to aerosols and spatters in dentistry. Am. J. Infect. Control 2008, 36, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Perdelli, F.; Spagnolo, A.M.; Cristina, M.L.; Sartini, M.; Malcontenti, R.; Dallera, M.; Ottria, G.; Lombardi, R.; Orlando, P. Evaluation of contamination by blood aerosols produced during various healthcare procedures. J. Hosp. Infect. 2008, 70, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Orlando, P.; Cristina, M.L.; Dallera, M.; Ottria, G.; Vitale, A.; Badolati, G. Surface disinfection: Evaluation of the efficacy of a nebulization system spraying hydrogen peroxide. J. Prev. Med. Hyg. 2008, 49, 116–119. [Google Scholar]
- Miller, R.L. Characteristics of blood-containing aerosols generated by common powered dental instruments. Am. Ind. Hyg. Assoc. J. 1995, 56, 670–676. [Google Scholar] [CrossRef]
- Rautemaa, R.; Nordberg, A.; Wuolijoki-Saaristo, K.; Meurman, J.H. Bacterial aerosols in dental practice—A potential hospital infection problem? J. Hosp. Infect. 2006, 64, 76–81. [Google Scholar] [CrossRef]
- Zemouri, C.; Volgenant, C.M.C.; Buijs, M.J.; Crielaard, W.; Rosema, N.A.M.; Brandt, B.W.; Laheij, A.M.G.A.; de Soet, J.J. Dental aerosols: Microbial composition and spatial distribution. J. Oral Microbiol. 2020, 12, 1762040. [Google Scholar] [CrossRef]
- Prospero, E.; Savini, S.; Annino, I. Microbial aerosol contamination of dental healthcare workers’ faces and other surfaces in dental practice. Infect. Control. Hosp. Epidemiol. 2003, 24, 139–141. [Google Scholar] [CrossRef]
- Jensen, E.T.; Giwercman, B.; Ojeniyi, B.; Bangsborg, J.M.; Hansen, A.; Koch, C.; Fiehn, N.E.; Høiby, N. Epidemiology of Pseudomonas aeruginosa in cystic fibrosis and the possible role of contamination by dental equipment. J. Hosp. Infect. 1997, 36, 117–122. [Google Scholar] [CrossRef]
- Mainz, J.G.; Gerber, A.; Lorenz, M.; Michl, R.; Hentschel, J.; Nader, A.; Beck, J.F.; Pletz, M.W.; Mueller, A.H. Pseudomonasaeruginosa Acquisition in Cystic Fibrosis Patients in Context of Otorhinolaryngological Surgery or Dentist Attendance: Case Series and Discussion of Preventive Concepts. Case Rep. Infect. Dis. 2015, 2015, 438517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montagna, M.T.; de Giglio, O.; Napoli, C.; Cannova, L.; Cristina, M.L.; Deriu, M.G.; Delia, S.A.; Giuliano, A.; Guida, M.; Laganà, P.; et al. Legionella spp. contamination in indoor air: Preliminary results of an Italian multicenter study. Epidemiol. Prev. 2014, 38, 62–65. [Google Scholar] [PubMed]
- Montagna, M.T.; Cristina, M.L.; de Giglio, O.; Spagnolo, A.M.; Napoli, C.; Cannova, L.; Deriu, M.G.; Delia, S.A.; Giuliano, A.; Guida, M.; et al. Serological and molecular identification of Legionella spp. isolated from water and surrounding air samples in Italian healthcare facilities. Environ. Res. 2016, 146, 47–50. [Google Scholar] [CrossRef]
- Montagna, M.T.; de Giglio, O.; Cristina, M.L.; Napoli, C.; Pacifico, C.; Agodi, A.; Baldovin, T.; Casini, B.; Coniglio, M.A.; D’Errico, M.M.; et al. Evaluation of Legionella Air Contamination in Healthcare Facilities by Different Sampling Methods: An Italian Multicenter Study. Int. J. Environ. Res. Public Health 2017, 14, 670. [Google Scholar] [CrossRef] [Green Version]
- Ricci, M.L.; Fontana, S.; Pinci, F.; Fiumana, E.; Pedna, M.F.; Farolfi, P.; Sabattini, M.A.B.; Scaturro, M. Pneumonia associated with a dental unit waterline. Lancet 2012, 379, 684. [Google Scholar] [CrossRef]
- Schönning, C.; Jernberg, C.; Klingenberg, D.; Andersson, S.; Pääjärvi, A.; Alm, E.; Tano, E.; Lytsy, B. Legionellosis acquired through a dental unit: A case study. J. Hosp. Infect. 2017, 96, 89–92. [Google Scholar] [CrossRef]
- Peralta, G.; Tobin-D’Angelo, M.; Parham, A.; Edison, L.; Lorentzson, L.; Smith, C.; Drenzek, C. Notes from the Field: Mycobacterium abscessus Infections Among Patients of a Pediatric Dentistry Practice—Georgia, 2015. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 355–356. [Google Scholar] [CrossRef] [Green Version]
- Petti, S.; Vitali, M. Occupational risk for Legionella infection among dental healthcare workers: Meta-analysis in occupational epidemiology. BMJ Open 2017, 7, e015374. [Google Scholar] [CrossRef] [Green Version]
- Reinthaler, F.F.; Mascher, F.; Stunzer, D. Serological examinations for antibodies against Legionella species in dental personnel. J. Dent. Res. 1988, 67, 942–943. [Google Scholar] [CrossRef]
- Fotos, P.G.; Westfall, H.N.; Snyder, I.S.; Miller, R.W.; Mutchler, B.M. Prevalence of Legionella specific IgG and IgM antibody in a dental clinic population. J. Dent. Res. 1985, 64, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Atlas, R.M.; Williams, J.F.; Huntington, M.K. Legionella contamination of dental-unit waters. Appl. Environ. Microbiol. 1995, 61, 1208–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian Health Ministry. Guidelines for Prevention and Control of Legionellosis; Rome, Italy, 2015. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2362_allegato.pdf. (accessed on 17 June 2020). (In Italian)
- Costa, D.; Bossard, V.; Brunet, K.; Fradin, B.; Imbert, C. Planktonic free-living amoebae susceptibility to dental unit waterlines disinfectants. Pathog. Dis. 2017, 75, ftx099. [Google Scholar] [CrossRef] [PubMed]
- Baudet, A.; Lizon, J.; Martrette, J.M.; Camelot, F.; Florentin, A.; Clément, C. Efficacy of BRS® and Alpron®/Bilpron® Disinfectants for Dental Unit Waterlines: A Six-Year Study. Int. J. Environ. Res. Public Health 2020, 17, 2634. [Google Scholar] [CrossRef] [Green Version]
- Yoon, H.Y.; Lee, S.Y. Susceptibility of bacteria isolated from dental unit waterlines to disinfecting chemical agents. J. Gen. Appl. Microbiol. 2019, 64, 269–275. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Part of the interior of a dental unit (reproduced with permission from Marshall GW Jr [5]).
Figure 1.
Part of the interior of a dental unit (reproduced with permission from Marshall GW Jr [5]).

Figure 2.
Biofilm formation on dental unit waterline tubing (reproduced with permission from Mills SE [41]).
Figure 2.
Biofilm formation on dental unit waterline tubing (reproduced with permission from Mills SE [41]).

Figure 3.
Phases of biofilm formation on the surface of a dental unit waterline (reproduced with permission from Mills SE [41]): (A) carbonate deposits (which resemble ice floes); (B) initial attachment; (C) division of cells into microcolonies; (D) formation of biofilm.
Figure 3.
Phases of biofilm formation on the surface of a dental unit waterline (reproduced with permission from Mills SE [41]): (A) carbonate deposits (which resemble ice floes); (B) initial attachment; (C) division of cells into microcolonies; (D) formation of biofilm.

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Spagnolo, A.M.; Sartini, M.; Cristina, M.L. Microbial Contamination of Dental Unit Waterlines and Potential Risk of Infection: A Narrative Review. Pathogens 2020, 9, 651. https://doi.org/10.3390/pathogens9080651
AMA Style
Spagnolo AM, Sartini M, Cristina ML. Microbial Contamination of Dental Unit Waterlines and Potential Risk of Infection: A Narrative Review. Pathogens. 2020; 9(8):651. https://doi.org/10.3390/pathogens9080651
Chicago/Turabian StyleSpagnolo, Anna Maria, Marina Sartini, and Maria Luisa Cristina. 2020. "Microbial Contamination of Dental Unit Waterlines and Potential Risk of Infection: A Narrative Review" Pathogens 9, no. 8: 651. https://doi.org/10.3390/pathogens9080651
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.