
The Microbiome in the Obesity-Breast Cancer Axis: Diagnostic and Therapeutic Potential
by
 , , and
, , and
Dimiter Avtanski
1,2,3,*,
Varun Reddy
4,
Radoslav Stojchevski
1,2,3,
Nikola Hadzi-Petrushev
5 and
Mitko Mladenov
5 1
Friedman Diabetes Institute, Lenox Hill Hospital, Northwell Health, New York, NY 10022, USA
2
Feinstein Institutes for Medical Research, Manhasset, NY 11030, USA
3
Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY 11549, USA
4
New York Institute of Technology, College of Osteopathic Medicine, Old Westbury, NY 11545, USA
5
Faculty of Natural Sciences and Mathematics, Institute of Biology, Ss. Cyril and Methodius University, 1000 Skopje, North Macedonia
*
Author to whom correspondence should be addressed.
Pathogens 2023, 12(12), 1402; https://doi.org/10.3390/pathogens12121402
Submission received: 5 November 2023
/
Revised: 25 November 2023
/
Accepted: 27 November 2023
/
Published: 29 November 2023
(This article belongs to the Special Issue Role of Microorganisms in Breast Cancer)
{kind=link}
Abstract
:A growing body of evidence has demonstrated a relationship between the microbiome, adiposity, and cancer development. The microbiome is emerging as an important factor in metabolic disease and cancer pathogenesis. This review aimed to highlight the role of the microbiome in obesity and its association with cancer, with a particular focus on breast cancer. This review discusses how microbiota dysbiosis may contribute to obesity and obesity-related diseases, which are linked to breast cancer. It also explores the potential of the gut microbiome to influence systemic immunity, leading to carcinogenesis via the modulation of immune function. This review underscores the potential use of the microbiome profile as a diagnostic tool and treatment target, with strategies including probiotics, fecal microbiota transplantation, and dietary interventions. However, this emphasizes the need for more research to fully understand the complex relationship between the microbiome, metabolic disorders, and breast cancer. Future studies should focus on elucidating the mechanisms underlying the impact of the microbiome on breast cancer and exploring the potential of the microbiota profile as a biomarker and treatment target.
Keywords:
microbiome; obesity; breast cancer; dysbiosis; diagnostic; therapeutic; diet; antibiotics; breast; inflammation1. Introduction
A large body of evidence has demonstrated a significant link between obesity and cancer risk. Adipose tissue, conventionally viewed as a passive reservoir for energy storage, is now recognized as a highly secretory endocrine organ that produces various pro- and anti-inflammatory cytokines, estrogens, and other bioactive molecules [1,2]. Obesity, characterized by adipose tissue hypertrophy (increase in adipocyte size) and hyperplasia (increase in adipocyte number), causes the dysregulation of adipose tissue hormonal production, leading to chronic low-grade inflammation that can contribute to the initiation and progression of breast cancer, particularly among postmenopausal women [3,4,5,6,7,8,9]. Furthermore, obesity-related metabolic changes can influence the composition of the gut microbiome, leading to dysbiosis, which may further affect breast cancer risk and outcomes.
Over the past two decades, following advancements in DNA sequencing technologies, the microbiome has been recognized as a major factor in maintaining health. The interaction between the microbiome and the host organism is a dynamic bidirectional relationship, where disruptions in the microbiome reflect the host’s health and vice versa: modifications to the health status of the host lead to corresponding microbiome changes.
Breast cancer is the most common type of cancer in women worldwide, increasingly affecting the younger population. While patients with breast cancer are currently experiencing higher survival and decreasing recurrence rates, the mortality remains high [10]. Despite well-known risk factors for breast cancer development, such as genetic predisposition, sex, age, estrogen levels, and obesity, the cause of more than half of new cases remains unknown [11]. Ample evidence suggests that the microbiome may play a significant role, among multiple factors. As most studies have concentrated on the gut microbiome, little is known about the influence of other microbial communities residing throughout the body. The microbiome in the breast is characterized by a different composition, and it is not incorrect to speculate that it plays various roles.
This review aims to present a brief, up-to-date overview of the role of the microbiome in breast cancer pathogenesis and explore how factors influencing its composition may impact disease development and progression, thus providing an evolutionary perspective on breast cancer.
2. Characteristics of the Breast Microbiome
Our bodies are complex entities composed of trillions of individual cells, including entire communities of symbiotic microorganisms (bacteria, archaea, and eukarya) that collectively constitute our microbiome [12]. The microbiome is now recognized as a pivotal determinant of an individual’s health, as its disturbance has been linked to various diseases [10,13,14,15,16].
The breast microbiome is a unique niche characterized by distinct microbial communities, composition, and characteristics [17,18]. It is believed to be formed predominantly from the migration of bacteria from the areola, as well as through the entero-mammary pathway, via immune cells translocating gut bacteria to secondary lymph nodes and progressing to the breast tissue through the lymphatic circulation or the blood [19,20,21]. The breast microbiome is shaped by the maternal diet, most prominently by dietary soluble fibers and plant and animal proteins [22]. Extensive studies of the breast milk microbiota have revealed a vast diversity of microbes, such as Staphylococcus, Streptococcus, Lactobacillus, Pseudomonas, Bifidobacterium, Corynebacterium, Enterococcus, Acinetobacter, Rothia, Cutibacterium, Veillonella, and Bacteroides [23]. The breast microbiome varies among races and ethnicities, as reported by Smith et al. [24] and others.
Although the role of the microbiome in breast cancer pathogenesis is gaining increasing attention, it is critical to recognize the inherent obstacles associated with microbiome research in this context [25]. These obstacles include, but are not limited to, variations in sample collection methods, differences in DNA extraction protocols, potential contamination issues, and the need for robust bioinformatics and statistical analyses to interpret complex datasets [26]. All these factors affect the replicability of published findings and need to be addressed adequately to guarantee the consistency and comparability of the obtained results. Functional testing of the statistical correlations is necessary to validate these findings [18,20].
3. Role of the Microbiome in Obesity-Induced Inflammation
Obesity is currently a pandemic affecting 650 million individuals worldwide, in addition to almost two billion categorized as overweight [27]. Predictions project that overweight and obesity will continue to increase in the foreseeable future.
The consistent energy overload mainly affects visceral white adipose tissue. Adipose tissue hypertrophy impairs normal adipocyte differentiation and secretion and stimulates tissue infiltration of immune cells, resulting in elevated proinflammatory cytokine secretion and chronic low-grade inflammation [28], leading to the development of metabolic conditions such as metabolic syndrome, dyslipidemia, insulin resistance, and type 2 diabetes [29,30,31]. The level of adiposity also strongly correlates with an increased incidence and worse outcomes in many different types of cancer [32]. Obesity is thought to be related to a 30% increase in breast cancer risk [33,34], and various studies have found intriguing associations between microbiota and obesity [35]. Although obesity plays a protective role in the development of breast cancer in premenopausal (particularly European) women, it shows a strong positive correlation with breast cancer risk in postmenopausal settings [36]. Among the multiple factors involved in this association, cytokines released by the white adipocytes per se, or activated macrophages, may directly promote the invasive potential and aggressiveness of breast cancer cells [37,38].
The gut microbiome composition is tightly modulated by metabolic signals and plays a significant role in the development of obesity. The level of adiposity is positively associated with changes in the microbiome composition (referred to as dysbiosis), characterized by generally reduced diversity and a shift in the abundance of dominant species [39,40,41,42]. For example, a cohort study involving primary school students in China revealed that obese children had lower species diversity and a relative abundance of typically dominant bacterial strands but a higher abundance of other genera [43]. Obese leptin-deficient (ob/ob) mice have a higher Firmicutes/Bacteroidetes (F/B) bacterial ratio than their wild-type counterparts [44]. Similar changes in the F/B ratio were observed in obese and lean humans [39,44,45]. Differences in abundance between lean and obese individuals have also been detected in other bacterial groups, such as those from the Oscillospira genus or the Christensenellaceae family [46,47]. Lv et al. [42] demonstrated a linear relationship between the body mass index (BMI) and several bacterial families (Porphyromonadaceae, Acidaminococcaceae, Rikenellaceae, and Desulfovibrionaceae). White et al. [48] suggested that gut microbiota is a modifiable factor linked to early rapid weight gain during infancy, and early weight gain has been identified as a risk factor for obesity during adulthood. The connection between the gut microbiome and adiposity extends to preterm infants, where the microbial composition was found to correlate with weight gain and subsequent growth, showing the influence of the microbiota from the earliest stages of life [49]. Similar to the gut microbiome, the breast tissue microbiome shows disparities between lean and obese individuals, with obese individuals exhibiting reduced bacterial diversity [17,18].
Dietary patterns may cause gut dysbiosis, which can lead to chronic inflammation [12]. A growing body of evidence has revealed that obesity-induced inflammation is associated with changes in microbiome composition. For example, using a high-fat diet (HFD)-induced obesity C57Bl/6 mouse model, Albornoz et al. [50] showed that obesity increases the susceptibility, pulmonary inflammation, and interferon-gamma (INF-γ) levels, following an infection with Mycobacterium tuberculosis. Gut bacteria metabolize dietary fiber into short-chain fatty acids (SCFAs), primarily butyrate, acetate, and propionate [51]. Butyrate has beneficial effects against obesity, including the promotion of lipolysis and an increase in energy expenditure. It also possesses anti-inflammatory properties by inhibiting proinflammatory cytokine production and reducing the translocation of lipopolysaccharides (LPSs) from the gut lumen to the bloodstream [52,53]. Butyrate also inhibits the expression of nitric oxide synthase (NOS) in intestinal cells by activating peroxisome proliferator-activated receptor gamma (PPARγ) signaling, thus limiting the growth of certain bacteria (such as those of the Enterobacteriaceae family) [54].
4. Microbiota and Breast Cancer
The microbiome profile has been linked to many types of cancers (stomach, colon, liver, lung, and skin, among others). The most robust connections are observed in cancers of the gastrointestinal tract, which are primarily associated with Helicobacter pylori and Fusobacterium bacteria [18,55,56,57,58,59,60].
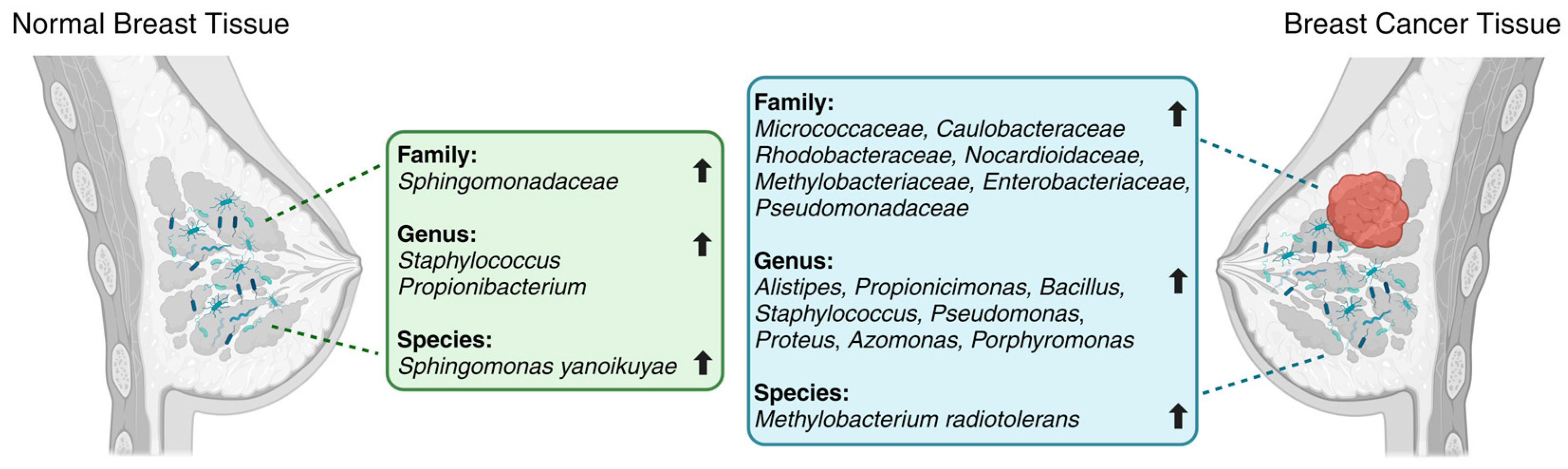
Breast cancer patients are characterized by decreased microbial diversity, as reported in several studies [19,61,62,63]. Early observational studies detected impaired intestinal microbiota in breast cancer patients, represented by a higher proportion of fecal Enterobacteriaceae, aerobic Streptococci, Lactobacilli, and anaerobic species such as Clostridia, Lactobacilli, and Bacteroides [64]. A comparative analysis by Xuan et al. [19] showed the enrichment of Methylobacterium radiotolerans in breast tumor tissues and Sphingomonas yanoikuyae in paired normal breast tissues (Figure 1). Using 16S rRNA gene amplicon sequencing, Chan et al. [65] investigated microbiota from nipple aspirates from healthy women and those with breast cancer and reported a higher incidence of Sphingomonadaceae in the healthy subject group and a higher proportion of the genus Alistipes in breast cancer patients (Figure 1). The microbiota of breast tissue adjacent to the tumor showed higher levels of the phylum Bacteroidetes and the genera Bacillus and Staphylococcus than those in healthy tissues [20]. Similarly, Meng et al. [66] analyzed breast tissue samples using needle biopsies from patients with breast cancer and benign tumors and observed an increase in the genus Propionicimonas and the families Micrococcaceae, Caulobacteraceae, Rhodobacteraceae, Nocardioidaceae, and Methylobacteriaceae (Figure 1). The microbial characterization of samples from 25 breast cancer patients showed lower levels of Firmicutes and Bacteroidetes and higher levels of Proteobacteria, Actinobacteria, and Verrucomicrobia, accompanied by a reduction in Faecalibacterium prausnitzii [67]. Another comparative study between patients with breast cancer and healthy individuals [11] demonstrated greater levels of Enterobacteriaceae and Pseudomonadaceae families (such as the genera Pseudomonas, Proteus, Azomonas, and Porphyromonas) in breast tumors and predominance of the genera Staphylococcus and Propionibacterium in healthy controls (Figure 1). A comparison of the breast tissues adjacent to the tumor showed a higher abundance of Bacteroidetes (Bacillus and Staphylococcus). Additionally, the F/B ratio was found to be significantly higher in patients with breast cancer than in controls [67].
Furthermore, microbial profiles vary during the progression of breast cancer. A comparison of the microbiome profiles of malignant tissues of different histological grades revealed that the development of breast cancer was associated with a decreased proportion of bacteria from the Bacteroidaceae family and an increased proportion of bacteria from the Agrococcus genus [66]. Stage I breast cancers exhibit an abundance of Proteobacteria, Ruminococcaceae, and Hyphomicrobium; stage II breast cancers show higher levels of Euryarchaeota, Firmicutes, Spirochaetes, and Sporosarcina, whereas stages III and IV breast cancers have high levels of Thermi, Gemmatimonadetes, Tenericutes, and Bosea [24].
Evidence suggests that shifts in microbial assemblages in the breast are related to breast cancer development, aggressiveness, and progression [18]. Using next-generation sequencing techniques and quantitative PCR analysis, Xuan et al. [19] demonstrated that breast tumor tissue has a reduced expression of antibacterial response genes, compared with adjacent healthy breast tissue. The observed dysbiosis in breast cancer suggests that bacteria may play a role in maintaining the normal cellular processes in the breast. Thus, it is speculated that the microbial components present in the breast may influence the local microenvironment. It is hypothesized that chronic exposure to low-residue antimicrobial drugs ingested from the diet could disrupt the gut microbiota equilibrium, which can contribute to corresponding physiological changes [68]. Dysbiosis caused by antibiotic use may increase the risk of breast cancer; however, more extensive studies are needed to confirm this hypothesis [69,70].
5. Etiology of Microbiome Dysbiosis in Breast Cancer
There are various mechanisms by which microbiota can influence breast cancer initiation and development. These include changes in adiposity, systemic estrogen levels, insulin resistance, dyslipidemia, and inflammation [71].
Adipose status is a major factor that affects microbial communities. Low gut microbial diversity occurs with obesity, insulin resistance, dyslipidemia, leukocytosis, and elevated levels of C-reactive protein (CRP), which are linked to breast cancer [71]. Hossain et al. [72] demonstrated that obesity is associated with increased incidence and worse prognosis in triple-negative breast cancer (TNBC) through various potential mechanisms, including the modulation of the gut microbiome. Using 16S rRNA sequencing and metagenomic analyses, the authors showed that obesity in TNBC decreases alpha diversity in the gut microbiome and is strongly correlated with functional profiles [72]. TNBC has been found to have the least taxonomic diversity among all breast cancer types, indicating a potential link between TNBC and the breast microbiome [73]. Levels of sex hormones have been shown to regulate the diversity of the gut microbiome [74]. Moreover, antimicrobial exposure during curative-intent treatment of TNBC has been linked to gut microbiome dysbiosis and decreased survival, suggesting a possible relationship between hormone levels and gut microbiome in TNBC [75]. Increased levels of hormones such as estrogens, insulin, insulin-like growth factor (IGF), and leptin have been associated with an increased cancer risk in obese individuals [76]. Studies have shown that the breast microbiome biomass decreases in breast cancer patients [77]. Additionally, distinct microbial communities have been observed in breast tissues of non-Hispanic Black and non-Hispanic White women, with differences in microbiome composition by race, breast cancer stage, or breast tumor subtype [24,78]. Dysbiosis of microbiota may contribute to obesity and obesity-related diseases through various mechanisms, including energy harvesting, direct effects on gene expression, and direct or indirect effects of chronic inflammation [79]. Dysbiosis of obesity is associated with hormonal changes. For example, estrogens (a risk factor for breast cancer) are elevated in obese individuals and modulated by microbiota [80]. Therefore, concomitant dysbiosis and obesity may increase the risk of breast cancer [81]. The enterohepatic recycling of estrogens by gut bacteria with increased β-glucuronidase (β-GUS) or β-glucosidase (β-Gluc) activity (Firmicutes (Clostridium coccoides, Clostridium leptum), Actinobacteria (Bifidobacterium sp.), or Bacteroidetes (Bacteroides sp.)) causes deconjugation of estrogen, which leads to increased levels of estrogens in circulation and an increased risk of breast cancer [82,83]. Several studies suggested that β-GUS may have a role in breast cancer development and progression [82,84,85,86]. The increase in β-GUS and β-Gluc activities in feces was found to be highly associated with bacteria from the Clostridia and Ruminococcaceae families [87].
The difference in the breast microbiota profile between lean and obese individuals suggests that the microbiome may contribute to chronic low-grade inflammation of adipose tissue, thus affecting the development, progression, and outcome of breast cancer [88]. The composition of the breast microbiota is influenced by multilayered interactions with the immune system [62]. The difference in breast microbiota between breast cancer subtypes and disease severity suggests a potential role for immunosuppression and tumor evasion by the immune system.
Gut bacteria influence systemic immunity [89,90,91]. In mice, targeted orogastric infection with Helicobacter hepaticus causes mammary neoplasia with an increased frequency [92,93]. The diversity of the gastrointestinal microbiome is closely associated with lymphocyte infiltration. Shi et al. [94] compared the gastrointestinal microbiome with the number of tumor-infiltrating lymphocytes (TILs) and found that breast cancer patients with higher gut microbial diversity showed an increased number of TILs. Disruption of the gut microbiota may lead to carcinogenesis via the modulation of immune function [95]. Animal model studies have shown that changes in immune function led to the initiation and progression of breast tumors. Mouse models with antibiotic-induced dysbiosis showed an increase in fibrosis and collagen deposition and induced higher myeloid cell infiltration into tumors, as well as normal adjacent breast tissue, at both the early and late stages of breast tumor progression [96]. The microbiome also affects tumor necrosis factor-alpha (TNFα)-mediated innate immune inflammatory responses, CD25+ regulatory T cells, and neutrophils [92,93]. Mice with advanced tumors showed elevated expression of CCL2 (s. MCP-1), IL-23, IL-6, and arginase-1 (ARG1). An unbalanced host immune response to enteric bacteria may promote the development of cancer within the gastrointestinal tract and epithelial cells distant from the gut [92,97,98,99,100,101,102,103].
Gut microbiome influences the development and progression of breast cancer. Perturbations in the gut microbiota (for example, due to antibiotic use) can provoke the elevation of free estrogen levels, thereby increasing the risk of breast cancer initiation [34]. The gut microbiome also affects the response to breast cancer treatment, including hormone therapy and chemotherapy [104].
Increased levels of bile acids have been observed in breast tumors and have been found to positively impact cancer survival by inhibiting tumor growth [105]. The intestinal microbiota converts bile acids from primary to secondary via deconjugation and 7α-dehydroxylation. Certain bile acids act like hormones by exerting their action in distant tissues by activating specific receptors such as the vitamin D receptor (VDR), Farnesoid X receptor (FXR), pregnane X receptor (PXR), and Takeda G-protein coupled receptor-5 (TGR5) [106]. For example, lithocholic acid, in particular, was found to decrease cancer cell proliferation due to its immune effects, partly through the activation of TGR5 [107]. Triggered by bile acids, FXR mediates breast cancer cell apoptosis and reduces aromatase expression, which is a local source of pro-proliferative estrogens [108].
6. The Microbiome as a Biomarker and Treatment Target
Based on current knowledge, the microbiome has emerged as a promising biomarker for evaluating breast cancer risk and prognosis or predicting the surgical outcomes and survival of patients with breast cancer [62,109,110,111]. For example, the F/B ratio can be used as an indicator of breast cancer risk [20,85]. Evaluation of the microbiome profile could have broad implications for the diagnosis and staging of breast cancer [66]. Meng et al. [66] showed that glycerophospholipid levels and ribosome biogenesis are higher in grade III breast cancers than in grades I and II. Additionally, the microbiome involved in human estrogen metabolism (also known as the estrobolome) can be used as another target for breast cancer treatment [85]. Microbial communities can alter the response to breast cancer therapy [112]. Gut microbe dysbiosis undermines the outcome of both immune and non-immune chemotherapeutic cancer treatment modalities [93,113,114]. The microbiota may potentially be targeted to enhance the efficacy and reduce the toxicity of conventional anticancer therapies. Taken together, the complex scenario linking microbiome composition to oncogenesis and the response to anticancer treatments defines the frame of a new “oncobiotic” perspective.
Probiotics have been shown to improve gut microbiota composition and function, suggesting their potential implications in cancer prevention and treatment [115]. Lactobacillus bacteria can modulate dysregulated SCFA levels in obesity by influencing other gut microbiota, energy absorption, and chronic low-grade inflammation [116]. Lactic acid bacteria (LAB) have been reported to exert anti-obesity effects. Thus, targeting the microbiome could be considered a potential treatment option for obesity [79]. Animal and cell-based studies have shown that probiotics may have anticancer effects because they can modulate the immune system and reduce obesity-induced low-grade chronic inflammation, potentially inhibiting cancer cell growth [115,117]. A study investigating the effect of oral administration of probiotics for 12 weeks, involving 18 patients with breast cancer, demonstrated an improved microbiome profile and serum tests (ANC (absolute neutrophil count), fasting blood glucose (FBG), and low-density lipoprotein cholesterol (LDL-C) levels) [118]. The most prominent changes observed in this study were for Ruminococcus and Streptococcus spp. The effects of probiotics, prebiotics, and synbiotics on breast cancer have been reviewed in randomized controlled trials [115,119]. A systematic review and meta-analysis of randomized clinical trials of probiotic and prebiotic use in breast cancer patients and survivors by Thu et al. [120] demonstrated the beneficial effects of a combination of pro- and prebiotics on obesity and dyslipidemia, as well as the reduction of TNFα levels, thus highlighting their potential against breast cancer. However, using probiotics to improve the gut microbiome as a treatment strategy for obesity is likely more complicated than anticipated and may require a long-term complex program [116].
Fecal microbiota transplantation (FMT) is another promising strategy for reducing obesity. Dietary interventions or FMT have emerged as promising strategies to help patients maintain a healthy weight [121]. FMT has been shown to reverse the effects of antibiotics and re-establish microbiota balance, resulting in the restoration of the normal functioning microbiome [122].
Furthermore, diet is known to influence the microbiota. The Mediterranean diet (characterized by a high content of plant-based foods and healthy fats) has been associated with a distinctive shift in the mammary gland microbiota, suggesting possible anti-breast cancer effects [123]. Long-term breast cancer risk is associated with diet-related plasma metabolic signatures involving exogenous steroid metabolites and microbiota-related compounds [124]. SCFAs are produced by two major groups of bacteria: Firmicutes bacteria produce butyrate, and Bacteroidetes bacteria produce acetate and propionate. It has been shown that SCFAs, more specifically butyrate, inhibit tumor growth [125]. A typical Western diet decreases the generation of SCFAs, causing a leaky gut and leading to an increase in inflammatory marker levels in the bloodstream, which results in the progression of breast cancer. Conversely, healthy diets with a higher fiber content may decrease inflammation by increasing SCFA production [126].
7. Conclusions
The microbiome comprises a significant proportion of multicellular organisms and is currently recognized as an essential contributor to the pathogenesis of metabolic diseases and cancer. The mechanisms by which microbiota influence breast cancer initiation and development are complex. Dysbiosis of the microbiome may contribute to obesity and obesity-related diseases associated with breast cancer. Furthermore, the microbiome can influence systemic immunity, potentially leading to carcinogenesis via the modulation of immune function. Patients with breast cancer often exhibit decreased microbial diversity, and accumulating evidence suggests that shifts in microbial assemblages are related to the development, aggressiveness, and progression of the disease.
The microbiome profile varies during breast cancer progression, indicating its potential as a biomarker for diagnosis and staging. This microbiome may also offer novel treatment options for patients with breast cancer. Treatment strategies include probiotics, FMT, and dietary intervention. Probiotics have shown promise in improving the composition and function of gut microbiota, which may result in the inhibition of cancer cell growth. Nutritional interventions, on the other hand, can influence microbiota, potentially decreasing inflammation and inhibiting tumor growth.
However, despite these promising findings, further research is needed to fully understand the complex relationship between the microbiome, metabolic disorders, and breast cancer [126]. This requires a multidisciplinary systems biology approach and evolutionary medicine thinking, combined with microbial ecology, immunology, cancer cell biology, and computational biology [127]. Future studies should focus on elucidating the mechanisms underlying the impact of the microbiome on breast cancer and exploring its potential as a biomarker and treatment target.
Author Contributions
Conceptualization, D.A.; resources, D.A.; writing—original draft preparation, D.A.; writing—review and editing, V.R., R.S., N.H.-P., and M.M.; visualization, R.S.; supervision, D.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ANC | Absolute neutrophil count |
| ARG1 | Arginase-1 |
| β-Gluc | β-glucosidase |
| β-GUS | β-glucuronidase |
| CCL2 | Chemokine (C-C motif) ligand 2 (s. Monocyte chemoattractant protein-1, MCP-1) |
| CRP | C-reactive protein |
| F/B | Firmicutes/Bacteroidetes bacterial ratio |
| FBG | Fasting blood glucose |
| FMT | Fecal microbiota transplantation |
| FXR | Farnesoid X receptor |
| HFD | High-fat diet |
| IGF | Insulin-like growth factor |
| IL | Interleukin |
| INF-γ | Interferon-gamma |
| LAB | Lactic acid bacteria |
| LDL-C | Low-density lipoprotein cholesterol |
| LPS | Lipopolysaccharide |
| NOS | Nitric oxide synthase |
| ob/ob mice | Leptin-deficient mice |
| PPARγ | Peroxisome proliferator-activated receptor gamma |
| PXR | Pregnane X receptor |
| SCFA | Short-chain fatty acid |
| TGR5 | Takeda G-protein coupled receptor-5 |
| TNBC | Triple-negative breast cancer |
| TNFα | Tumor necrosis factor-alpha |
| VDR | Vitamin D receptor |
References
- Ahima, R.S.; Flier, J.S. Adipose Tissue as an Endocrine Organ. Trends Endocrinol. Metab. 2000, 11, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Dong, H.; Balaz, M.; Slyper, M.; Drokhlyansky, E.; Colleluori, G.; Giordano, A.; Kovanicova, Z.; Stefanicka, P.; Balazova, L.; et al. snRNA-seq reveals a subpopulation of adipocytes that regulates thermogenesis. Nature 2020, 587, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Agnoli, C.; Berrino, F.; Abagnato, C.A.; Muti, P.; Panico, S.; Crosignani, P.; Krogh, V. Metabolic syndrome and postmenopausal breast cancer in the ORDET cohort: A nested case–control study. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Melvin, J.C.; Seth, D.; Holmberg, L.; Garmo, H.; Hammar, N.; Jungner, I.; Walldius, G.; Lambe, M.; Wigertz, A.; Van Hemelrijck, M. Lipid Profiles and Risk of Breast and Ovarian Cancer in the Swedish AMORIS Study. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1381–1384. [Google Scholar] [CrossRef]
- Agnoli, C.; Grioni, S.; Sieri, S.; Sacerdote, C.; Ricceri, F.; Tumino, R.; Frasca, G.; Pala, V.; Mattiello, A.; Chiodini, P.; et al. Metabolic Syndrome and Breast Cancer Risk: A Case-Cohort Study Nested in a Multicentre Italian Cohort. PLoS ONE 2015, 10, e0128891. [Google Scholar] [CrossRef]
- Wani, B.; Aziz, S.A.; Ganaie, M.A.; Mir, M.H. Metabolic Syndrome and Breast Cancer Risk. Indian J. Med. Paediatr. Oncol. 2017, 38, 434–439. [Google Scholar] [CrossRef]
- Colonna, S.V.; Douglas Case, L.; Lawrence, J.A. A retrospective review of the metabolic syndrome in women diagnosed with breast cancer and correlation with estrogen receptor. Breast Cancer Res. Treat. 2012, 131, 325–331. [Google Scholar] [CrossRef]
- Hwang, K.-T.; Han, K.-D.; Oh, S.; Koo, B.K.; Lee, S.K.; Kim, J.; Seo, H.J.; Jung, J.; Kim, B.H.; Hur, H. Influence of Metabolic Syndrome on Risk of Breast Cancer: A Study Analyzing Nationwide Data from Korean National Health Insurance Service. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2038–2047. [Google Scholar] [CrossRef]
- Nuri, R.; Akochakian, M.; Mahmudieh, B. Metabolic Syndrome, Breast Cancer and Exercise. Endocrinol. Metab. Syndr. 2016, 5, 6. [Google Scholar] [CrossRef]
- Song, X.; Wei, C.; Li, X. The Relationship Between Microbial Community and Breast Cancer. Front. Cell. Infect. Microbiol. 2022, 12, 849022. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, A.; Sangwan, N.; Jia, M.; Liu, C.-C.; Keslar, K.S.; Downs-Kelly, E.; Fairchild, R.L.; Al-Hilli, Z.; Grobmyer, S.R.; Eng, C. Human breast microbiome correlates with prognostic features and immunological signatures in breast cancer. Genome Med. 2021, 13, 60. [Google Scholar] [CrossRef]
- Reddy, V.; Avtanski, D. Environmental and Lifestyle Factors Influencing Inflammation and Type 2 Diabetes. In Obesity, Diabetes and Inflammation: Molecular Mechanisms and Clinical Management; Springer International Publishing: Cham, Switzerland, 2023; pp. 165–183. [Google Scholar]
- Marchesi, J.R.; Adams, D.H.; Fava, F.; Hermes, G.D.A.; Hirschfield, G.M.; Hold, G.; Quraishi, M.N.; Kinross, J.; Smidt, H.; Tuohy, K.M.; et al. The gut microbiota and host health: A new clinical frontier. Gut 2016, 65, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Malla, M.A.; Dubey, A.; Kumar, A.; Yadav, S.; Hashem, A.; Abd Allah, E.F. Exploring the Human Microbiome: The Potential Future Role of Next-Generation Sequencing in Disease Diagnosis and Treatment. Front. Immunol. 2018, 9, 2868. [Google Scholar] [CrossRef] [PubMed]
- Lee-Sarwar, K.A.; Lasky-Su, J.; Kelly, R.S.; Litonjua, A.A.; Weiss, S.T. Metabolome-Microbiome Crosstalk and Human Disease. Metabolites 2020, 10, 181. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The Human Respiratory System and its Microbiome at a Glimpse. Biology 2020, 9, 318. [Google Scholar] [CrossRef]
- Cabrera-Rubio, R.; Collado, M.C.; Laitinen, K.; Salminen, S.; Isolauri, E.; Mira, A. The human milk microbiome changes over lactation and is shaped by maternal weight and mode of delivery. Am. J. Clin. Nutr. 2012, 96, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Hieken, T.J.; Chen, J.; Hoskin, T.L.; Walther-Antonio, M.; Johnson, S.; Ramaker, S.; Xiao, J.; Radisky, D.C.; Knutson, K.L.; Kalari, K.R.; et al. The Microbiome of Aseptically Collected Human Breast Tissue in Benign and Malignant Disease. Sci. Rep. 2016, 6, 30751. [Google Scholar] [CrossRef] [PubMed]
- Xuan, C.; Shamonki, J.M.; Chung, A.; Dinome, M.L.; Chung, M.; Sieling, P.A.; Lee, D.J. Microbial dysbiosis is associated with human breast cancer. PLoS ONE 2014, 9, e83744. [Google Scholar] [CrossRef]
- Urbaniak, C.; Gloor, G.B.; Brackstone, M.; Scott, L.; Tangney, M.; Reid, G. The Microbiota of Breast Tissue and Its Association with Breast Cancer. Appl. Environ. Microbiol. 2016, 82, 5039–5048. [Google Scholar] [CrossRef]
- Rodríguez, J.M.; Fernández, L.; Verhasselt, V. The Gut–Breast Axis: Programming Health for Life. Nutrients 2021, 13, 606. [Google Scholar] [CrossRef]
- Cortes-Macías, E.; Selma-Royo, M.; García-Mantrana, I.; Calatayud, M.; González, S.; Martínez-Costa, C.; Collado, M.C. Maternal Diet Shapes the Breast Milk Microbiota Composition and Diversity: Impact of Mode of Delivery and Antibiotic Exposure. J. Nutr. 2021, 151, 330–340. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Breast milk microbiota: A review of the factors that influence composition. J. Infect. 2020, 81, 17–47. [Google Scholar] [CrossRef]
- Smith, A.; Pierre, J.F.; Makowski, L.; Tolley, E.; Lyn-Cook, B.; Lu, L.; Vidal, G.; Starlard-Davenport, A. Distinct microbial communities that differ by race, stage, or breast-tumor subtype in breast tissues of non-Hispanic Black and non-Hispanic White women. Sci. Rep. 2019, 9, 11940. [Google Scholar] [CrossRef]
- Sinha, R.; Abu-Ali, G.; Vogtmann, E.; Fodor, A.A.; Ren, B.; Amir, A.; Schwager, E.; Crabtree, J.; Ma, S.; Microbiome Quality Control Project Consortium; et al. Assessment of variation in microbial community amplicon sequencing by the Microbiome Quality Control (MBQC) project consortium. Nat. Biotechnol. 2017, 35, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Manzoor, S.S.; Doedens, A.; Burns, M.B. The promise and challenge of cancer microbiome research. Genome Biol. 2020, 21, 131. [Google Scholar] [CrossRef]
- World Health Organization. World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240051157 (accessed on 16 October 2023).
- Sengupta, S.; Avtanski, D. Obesity and Inflammation. In Obesity, Diabetes and Inflammation: Molecular Mechanisms and Clinical Management; Springer International Publishing: Cham, Switzerland, 2023; pp. 15–53. [Google Scholar]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef] [PubMed]
- Avtanski, D.; Pavlov, V.A.; Tracey, K.J.; Poretsky, L. Characterization of inflammation and insulin resistance in high-fat diet-induced male C57BL/6J mouse model of obesity. Anim. Model. Exp. Med. 2019, 2, 252–258. [Google Scholar] [CrossRef]
- Colditz, G.A.; Peterson, L.L. Obesity and Cancer: Evidence, Impact, and Future Directions. Clin. Chem. 2018, 64, 154–162. [Google Scholar] [CrossRef]
- Vainio, H.; Kaaks, R.; Bianchini, F. Weight control and physical activity in cancer prevention: International evaluation of the evidence. Eur. J. Cancer Prev. 2002, 11 (Suppl. 2), S94–S100. [Google Scholar]
- Stone, S.A.; Han, C.J.; Senn, T.; Korde, L.A.; Allott, K.; Reding, S.; Whittington, D.; Reding, K.W. Sex Hormones in Women With Elevated Breast Cancer Risk Undergoing Weight Loss. West. J. Nurs. Res. 2019, 41, 1602–1622. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Altemus, J.; Niazi, F.; Green, H.; Calhoun, B.C.; Sturgis, C.; Grobmyer, S.R.; Eng, C. Breast tissue, oral and urinary microbiomes in breast cancer. Oncotarget 2017, 8, 88122–88138. [Google Scholar] [CrossRef] [PubMed]
- Dehesh, T.; Fadaghi, S.; Seyedi, M.; Abolhadi, E.; Ilaghi, M.; Shams, P.; Ajam, F.; Mosleh-Shirazi, M.A.; Dehesh, P. The relation between obesity and breast cancer risk in women by considering menstruation status and geographical variations: A systematic review and meta-analysis. BMC Womens. Health 2023, 23, 392. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Avtanski, D.; Saxena, N.K.; Sharma, D. Leptin-induced epithelial-mesenchymal transition in breast cancer cells requires β-catenin activation via Akt/GSK3- and MTA1/Wnt1 protein-dependent pathways. J. Biol. Chem. 2012, 287, 8598–8612. [Google Scholar] [CrossRef] [PubMed]
- Avtanski, D.; Garcia, A.; Caraballo, B.; Thangeswaran, P.; Marin, S.; Bianco, J.; Lavi, A.; Poretsky, L. Resistin induces breast cancer cells epithelial to mesenchymal transition (EMT) and stemness through both adenylyl cyclase-associated protein 1 (CAP1)-dependent and CAP1-independent mechanisms. Cytokine 2019, 120, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Verdam, F.J.; Fuentes, S.; de Jonge, C.; Zoetendal, E.G.; Erbil, R.; Greve, J.W.; Buurman, W.A.; de Vos, W.M.; Rensen, S.S. Human intestinal microbiota composition is associated with local and systemic inflammation in obesity. Obesity (Silver Spring) 2013, 21, E607–E615. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S. Connecting Female Infertility to Obesity, Inflammation, and Maternal Gut Dysbiosis. Endocrinology 2016, 157, 1725–1727. [Google Scholar] [CrossRef]
- Tam, J.; Hoffmann, T.; Fischer, S.; Bornstein, S.; Gräßler, J.; Noack, B. Obesity alters composition and diversity of the oral microbiota in patients with type 2 diabetes mellitus independently of glycemic control. PLoS ONE 2018, 13, e0204724. [Google Scholar] [CrossRef]
- Lv, Y.; Qin, X.; Jia, H.; Chen, S.; Sun, W.; Wang, X. The association between gut microbiota composition and BMI in Chinese male college students, as analysed by next-generation sequencing. Br. J. Nutr. 2019, 122, 986–995. [Google Scholar] [CrossRef]
- Jiang, L.F.; Wang, Y.Y.; Peng, H.; Li, R.; Zhang, F.; Wang, N.; Shao, Q.W.; Jiang, Q. Association between obesity with the diversity and genus of gut microbiota in school-aged children. Zhonghua Liu Xing Bing Xue Za Zhi 2022, 43, 260–268. [Google Scholar] [CrossRef]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Microbial ecology: Human gut microbes associated with obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Leeming, E.R.; Johnson, A.J.; Spector, T.D.; Le Roy, C.I. Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration. Nutrients 2019, 11, 2862. [Google Scholar] [CrossRef]
- Konikoff, T.; Gophna, U. Oscillospira: A Central, Enigmatic Component of the Human Gut Microbiota. Trends Microbiol. 2016, 24, 523–524. [Google Scholar] [CrossRef]
- Goodrich, J.K.; Waters, J.L.; Poole, A.C.; Sutter, J.L.; Koren, O.; Blekhman, R.; Beaumont, M.; Van Treuren, W.; Knight, R.; Bell, J.T.; et al. Human genetics shape the gut microbiome. Cell 2014, 159, 789–799. [Google Scholar] [CrossRef] [PubMed]
- White, R.A.; Bjørnholt, J.V.; Baird, D.D.; Midtvedt, T.; Harris, J.R.; Pagano, M.; Hide, W.; Rudi, K.; Moen, B.; Iszatt, N.; et al. Novel developmental analyses identify longitudinal patterns of early gut microbiota that affect infant growth. PLoS Comput. Biol. 2013, 9, e1003042. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Zhou, C.; Xiang, S.; Dong, J.; Zhu, Q.; Yin, J.; Lu, X.; Xiao, Z. Association Between Trajectory Patterns of Body Mass Index Change Up to 10 Months and Early Gut Microbiota in Preterm Infants. Front. Microbiol. 2022, 13, 828275. [Google Scholar] [CrossRef]
- Palma Albornoz, S.P.; Fraga-Silva, T.F.D.C.; Gembre, A.F.; de Oliveira, R.S.; de Souza, F.M.; Rodrigues, T.S.; Kettelhut, I.D.C.; Manca, C.S.; Jordao, A.A.; Ramalho, L.N.Z.; et al. Obesity-Induced Dysbiosis Exacerbates IFN-γ Production and Pulmonary Inflammation in the Mycobacterium tuberculosis Infection. Cells 2021, 10, 1732. [Google Scholar] [CrossRef]
- Jia, Y.; Hong, J.; Li, H.; Hu, Y.; Jia, L.; Cai, D.; Zhao, R. Butyrate stimulates adipose lipolysis and mitochondrial oxidative phosphorylation through histone hyperacetylation-associated β 3 -adrenergic receptor activation in high-fat diet-induced obese mice. Exp. Physiol. 2017, 102, 273–281. [Google Scholar] [CrossRef]
- Lührs, H.; Gerke, T.; Schauber, J.; Dusel, G.; Melcher, R.; Scheppach, W.; Menzel, T. Cytokine-activated degradation of inhibitory κB protein α is inhibited by the short-chain fatty acid butyrate. Int. J. Color. Dis. 2001, 16, 195–201. [Google Scholar] [CrossRef]
- Hartstra, A.V.; Bouter, K.E.C.; Bäckhed, F.; Nieuwdorp, M. Insights Into the Role of the Microbiome in Obesity and Type 2 Diabetes. Diabetes Care 2015, 38, 159–165. [Google Scholar] [CrossRef]
- Byndloss, M.X.; Olsan, E.E.; Rivera-Chávez, F.; Tiffany, C.R.; Cevallos, S.A.; Lokken, K.L.; Torres, T.P.; Byndloss, A.J.; Faber, F.; Gao, Y.; et al. Microbiota-activated PPAR-γ signaling inhibits dysbiotic Enterobacteriaceae expansion. Science 2017, 357, 570–575. [Google Scholar] [CrossRef]
- Forman, D.; Newell, D.G.; Fullerton, F.; Yarnell, J.W.; Stacey, A.R.; Wald, N.; Sitas, F. Association between infection with Helicobacter pylori and risk of gastric cancer: Evidence from a prospective investigation. BMJ 1991, 302, 1302–1305. [Google Scholar] [CrossRef]
- Wotherspoon, A.C.; Doglioni, C.; Diss, T.C.; Pan, L.; Moschini, A.; de Boni, M.; Isaacson, P.G. Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori. Lancet 1993, 342, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Kostic, A.D.; Gevers, D.; Pedamallu, C.S.; Michaud, M.; Duke, F.; Earl, A.M.; Ojesina, A.I.; Jung, J.; Bass, A.J.; Tabernero, J.; et al. Genomic analysis identifies association of Fusobacterium with colorectal carcinoma. Genome Res. 2012, 22, 292–298. [Google Scholar] [CrossRef]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Sinha, R.; Pei, Z.; Dominianni, C.; Wu, J.; Shi, J.; Goedert, J.J.; Hayes, R.B.; Yang, L. Human gut microbiome and risk for colorectal cancer. J. Natl. Cancer Inst. 2013, 105, 1907–1911. [Google Scholar] [CrossRef]
- Wang, F.; Meng, W.; Wang, B.; Qiao, L. Helicobacter pylori-induced gastric inflammation and gastric cancer. Cancer Lett. 2014, 345, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Klann, E.; Williamson, J.M.; Tagliamonte, M.S.; Ukhanova, M.; Asirvatham, J.R.; Chim, H.; Yaghjyan, L.; Mai, V. Microbiota composition in bilateral healthy breast tissue and breast tumors. Cancer Causes Control 2020, 31, 1027–1038. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, S.; Aarnoutse, R.; Ziemons, J.; Kooreman, L.; Boleij, A.; Smidt, M. Exploring the Potential of Breast Microbiota as Biomarker for Breast Cancer and Therapeutic Response. Am. J. Pathol. 2021, 191, 968–982. [Google Scholar] [CrossRef]
- Wang, N.; Sun, T.; Xu, J. Tumor-related Microbiome in the Breast Microenvironment and Breast Cancer. J. Cancer 2021, 12, 4841–4848. [Google Scholar] [CrossRef]
- Minelli, E.B.; Beghini, A.M.; Vesentini, S.; Marchiori, L.; Nardo, G.; Cerutti, R.; MORTANI, E. Intestinal Microflora as an Alternative Metabolic Source of Estrogens in Women with Uterine Leiomyoma and Breast Cancer. Ann. N. Y. Acad. Sci. 1990, 595, 473–479. [Google Scholar] [CrossRef]
- Chan, A.A.; Bashir, M.; Rivas, M.N.; Duvall, K.; Sieling, P.A.; Pieber, T.R.; Vaishampayan, P.A.; Love, S.M.; Lee, D.J. Characterization of the microbiome of nipple aspirate fluid of breast cancer survivors. Sci. Rep. 2016, 6, 28061. [Google Scholar] [CrossRef] [PubMed]
- Meng, S.; Chen, B.; Yang, J.; Wang, J.; Zhu, D.; Meng, Q.; Zhang, L. Study of Microbiomes in Aseptically Collected Samples of Human Breast Tissue Using Needle Biopsy and the Potential Role of in situ Tissue Microbiomes for Promoting Malignancy. Front. Oncol. 2018, 8, 318. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Liu, Y.; Ye, S.; Yin, S.; Gu, J. Changes of intestinal microflora of breast cancer in premenopausal women. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 503–513. [Google Scholar] [CrossRef]
- Riley, L.W.; Raphael, E.; Faerstein, E. Obesity in the United States—Dysbiosis from exposure to low-dose antibiotics? Front. public Health 2013, 1, 69. [Google Scholar] [CrossRef] [PubMed]
- Velicer, C.M.; Heckbert, S.R.; Lampe, J.W.; Potter, J.D.; Robertson, C.A.; Taplin, S.H. Antibiotic use in relation to the risk of breast cancer. JAMA 2004, 291, 827–835. [Google Scholar] [CrossRef]
- McKee, A.M.; Kirkup, B.M.; Madgwick, M.; Fowler, W.J.; Price, C.A.; Dreger, S.A.; Ansorge, R.; Makin, K.A.; Caim, S.; Le Gall, G.; et al. Antibiotic-induced disturbances of the gut microbiota result in accelerated breast tumor growth. iScience 2021, 24, 103012. [Google Scholar] [CrossRef]
- Goedert, J.J.; Jones, G.; Hua, X.; Xu, X.; Yu, G.; Flores, R.; Falk, R.T.; Gail, M.H.; Shi, J.; Ravel, J.; et al. Investigation of the association between the fecal microbiota and breast cancer in postmenopausal women: A population-based case-control pilot study. J. Natl. Cancer Inst. 2015, 107, djv147. [Google Scholar] [CrossRef]
- Hossain, F.; Majumder, S.; David, J.; Bunnell, B.A.; Miele, L. Obesity Modulates the Gut Microbiome in Triple-Negative Breast Cancer. Nutrients 2021, 13, 3656. [Google Scholar] [CrossRef]
- Devoy, C.; Flores Bueso, Y.; Tangney, M. Understanding and harnessing triple-negative breast cancer-related microbiota in oncology. Front. Oncol. 2022, 12, 1020121. [Google Scholar] [CrossRef]
- He, S.; Li, H.; Yu, Z.; Zhang, F.; Liang, S.; Liu, H.; Chen, H.; Lü, M. The Gut Microbiome and Sex Hormone-Related Diseases. Front. Microbiol. 2021, 12. [Google Scholar] [CrossRef]
- Ransohoff, J.D.; Ritter, V.; Purington, N.; Andrade, K.; Han, S.; Liu, M.; Liang, S.-Y.; John, E.M.; Gomez, S.L.; Telli, M.L.; et al. Antimicrobial exposure is associated with decreased survival in triple-negative breast cancer. Nat. Commun. 2023, 14, 2053. [Google Scholar] [CrossRef]
- Kado, T.; Nawaz, A.; Takikawa, A.; Usui, I.; Tobe, K. Linkage of CD8+ T cell exhaustion with high-fat diet-induced tumourigenesis. Sci. Rep. 2019, 9, 12284. [Google Scholar] [CrossRef]
- Mikó, E.; Kovács, T.; Sebő, É.; Tóth, J.; Csonka, T.; Ujlaki, G.; Sipos, A.; Szabó, J.; Méhes, G.; Bai, P. Microbiome—Microbial Metabolome—Cancer Cell Interactions in Breast Cancer—Familiar, but Unexplored. Cells 2019, 8, 293. [Google Scholar] [CrossRef]
- Smith, A.; Cao, X.; Gu, Q.; Kubi Amos-Abanyie, E.; Tolley, E.A.; Vidal, G.; Lyn-Cook, B.; Starlard-Davenport, A. Characterization of the Metabolome of Breast Tissues from Non-Hispanic Black and Non-Hispanic White Women Reveals Correlations between Microbial Dysbiosis and Enhanced Lipid Metabolism Pathways in Triple-Negative Breast Tumors. Cancers 2022, 14, 4075. [Google Scholar] [CrossRef] [PubMed]
- Li, H. Diet, Gut Microbiota and Obesity. J. Nutr. Health Food Sci. 2015, 3, 1–6. [Google Scholar] [CrossRef]
- Parida, S.; Sharma, D. Microbial Alterations and Risk Factors of Breast Cancer: Connections and Mechanistic Insights. Cells 2020, 9, 1091. [Google Scholar] [CrossRef] [PubMed]
- Shapira, I.; Sultan, K.; Lee, A.; Taioli, E. Evolving concepts: How diet and the intestinal microbiome act as modulators of breast malignancy. ISRN Oncol. 2013, 2013, 693920. [Google Scholar] [CrossRef] [PubMed]
- Dabek, M.; McCrae, S.I.; Stevens, V.J.; Duncan, S.H.; Louis, P. Distribution of beta-glucosidase and beta-glucuronidase activity and of beta-glucuronidase gene gus in human colonic bacteria. FEMS Microbiol. Ecol. 2008, 66, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Parida, S.; Sharma, D. The Microbiome-Estrogen Connection and Breast Cancer Risk. Cells 2019, 8, 1642. [Google Scholar] [CrossRef] [PubMed]
- Sui, Y.; Wu, J.; Chen, J. The Role of Gut Microbial β-Glucuronidase in Estrogen Reactivation and Breast Cancer. Front. cell Dev. Biol. 2021, 9, 631552. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Kwon, H.; Lim, W.; Moon, B.-I. Staphylococcus aureus-Derived Extracellular Vesicles Enhance the Efficacy of Endocrine Therapy in Breast Cancer Cells. J. Clin. Med. 2022, 11, 2030. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Shaikh, N.N.; Khan, K.M.; Kiran, S.; Naz, S.; Ul-Haq, Z.; Perveen, S.; Choudhary, M.I. Synthesis of 2-Aminopyrimidine Derivatives and Their Evaluation as β-Glucuronidase Inhibitors: In Vitro and In Silico Studies. Molecules 2022, 27, 7786. [Google Scholar] [CrossRef] [PubMed]
- Flores, R.; Shi, J.; Fuhrman, B.; Xu, X.; Veenstra, T.D.; Gail, M.H.; Gajer, P.; Ravel, J.; Goedert, J.J. Fecal microbial determinants of fecal and systemic estrogens and estrogen metabolites: A cross-sectional study. J. Transl. Med. 2012, 10, 253. [Google Scholar] [CrossRef] [PubMed]
- Danforth, D.N. The Role of Chronic Inflammation in the Development of Breast Cancer. Cancers 2021, 13, 3918. [Google Scholar] [CrossRef] [PubMed]
- Lakritz, J.R.; Poutahidis, T.; Levkovich, T.; Varian, B.J.; Ibrahim, Y.M.; Chatzigiagkos, A.; Mirabal, S.; Alm, E.J.; Erdman, S.E. Beneficial bacteria stimulate host immune cells to counteract dietary and genetic predisposition to mammary cancer in mice. Int. J. Cancer 2014, 135, 529–540. [Google Scholar] [CrossRef]
- Poutahidis, T.; Kleinewietfeld, M.; Smillie, C.; Levkovich, T.; Perrotta, A.; Bhela, S.; Varian, B.J.; Ibrahim, Y.M.; Lakritz, J.R.; Kearney, S.M.; et al. Microbial reprogramming inhibits Western diet-associated obesity. PLoS ONE 2013, 8, e68596. [Google Scholar] [CrossRef]
- Poutahidis, T.; Kearney, S.M.; Levkovich, T.; Qi, P.; Varian, B.J.; Lakritz, J.R.; Ibrahim, Y.M.; Chatzigiagkos, A.; Alm, E.J.; Erdman, S.E. Microbial symbionts accelerate wound healing via the neuropeptide hormone oxytocin. PLoS ONE 2013, 8, e78898. [Google Scholar] [CrossRef]
- Rao, V.P.; Poutahidis, T.; Ge, Z.; Nambiar, P.R.; Boussahmain, C.; Wang, Y.Y.; Horwitz, B.H.; Fox, J.G.; Erdman, S.E. Innate immune inflammatory response against enteric bacteria Helicobacter hepaticus induces mammary adenocarcinoma in mice. Cancer Res. 2006, 66, 7395–7400. [Google Scholar] [CrossRef]
- Lakritz, J.R.; Poutahidis, T.; Mirabal, S.; Varian, B.J.; Levkovich, T.; Ibrahim, Y.M.; Ward, J.M.; Teng, E.C.; Fisher, B.; Parry, N.; et al. Gut bacteria require neutrophils to promote mammary tumorigenesis. Oncotarget 2015, 6, 9387–9396. [Google Scholar] [CrossRef]
- Shi, J.; Geng, C.; Sang, M.; Gao, W.; Li, S.; Yang, S.; Li, Z. Effect of gastrointestinal microbiome and its diversity on the expression of tumor-infiltrating lymphocytes in breast cancer. Oncol. Lett. 2019, 17, 5050–5056. [Google Scholar] [CrossRef]
- Vivarelli, S.; Salemi, R.; Candido, S.; Falzone, L.; Santagati, M.; Stefani, S.; Torino, F.; Banna, G.L.; Tonini, G.; Libra, M. Gut Microbiota and Cancer: From Pathogenesis to Therapy. Cancers 2019, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Buchta Rosean, C.; Bostic, R.R.; Ferey, J.C.M.; Feng, T.-Y.; Azar, F.N.; Tung, K.S.; Dozmorov, M.G.; Smirnova, E.; Bos, P.D.; Rutkowski, M.R. Preexisting Commensal Dysbiosis Is a Host-Intrinsic Regulator of Tissue Inflammation and Tumor Cell Dissemination in Hormone Receptor-Positive Breast Cancer. Cancer Res. 2019, 79, 3662–3675. [Google Scholar] [CrossRef] [PubMed]
- Erdman, S.E.; Poutahidis, T.; Tomczak, M.; Rogers, A.B.; Cormier, K.; Plank, B.; Horwitz, B.H.; Fox, J.G. CD4+ CD25+ regulatory T lymphocytes inhibit microbially induced colon cancer in Rag2-deficient mice. Am. J. Pathol. 2003, 162, 691–702. [Google Scholar] [CrossRef]
- Erdman, S.E.; Rao, V.P.; Poutahidis, T.; Ihrig, M.M.; Ge, Z.; Feng, Y.; Tomczak, M.; Rogers, A.B.; Horwitz, B.H.; Fox, J.G. CD4(+)CD25(+) regulatory lymphocytes require interleukin 10 to interrupt colon carcinogenesis in mice. Cancer Res. 2003, 63, 6042–6050. [Google Scholar] [PubMed]
- Erdman, S.E.; Rao, V.P.; Poutahidis, T.; Rogers, A.B.; Taylor, C.L.; Jackson, E.A.; Ge, Z.; Lee, C.W.; Schauer, D.B.; Wogan, G.N.; et al. Nitric oxide and TNF-alpha trigger colonic inflammation and carcinogenesis in Helicobacter hepaticus-infected, Rag2-deficient mice. Proc. Natl. Acad. Sci. USA 2009, 106, 1027–1032. [Google Scholar] [CrossRef]
- Li, Y.; Kundu, P.; Seow, S.W.; de Matos, C.T.; Aronsson, L.; Chin, K.C.; Kärre, K.; Pettersson, S.; Greicius, G. Gut microbiota accelerate tumor growth via c-jun and STAT3 phosphorylation in APCMin/+ mice. Carcinogenesis 2012, 33, 1231–1238. [Google Scholar] [CrossRef]
- Nagamine, C.M.; Rogers, A.B.; Fox, J.G.; Schauer, D.B. Helicobacter hepaticus promotes azoxymethane-initiated colon tumorigenesis in BALB/c-IL10-deficient mice. Int. J. Cancer 2008, 122, 832–838. [Google Scholar] [CrossRef]
- Arthur, J.C.; Perez-Chanona, E.; Mühlbauer, M.; Tomkovich, S.; Uronis, J.M.; Fan, T.-J.; Campbell, B.J.; Abujamel, T.; Dogan, B.; Rogers, A.B.; et al. Intestinal inflammation targets cancer-inducing activity of the microbiota. Science 2012, 338, 120–123. [Google Scholar] [CrossRef]
- Rao, V.P.; Poutahidis, T.; Fox, J.G.; Erdman, S.E. Breast cancer: Should gastrointestinal bacteria be on our radar screen? Cancer Res. 2007, 67, 847–850. [Google Scholar] [CrossRef]
- Bruce, E.; Makaranka, S.; Urquhart, G.; Elsberger, B. Does the gut microbiome environment influence response to systemic breast cancer treatment? Explor. Target. Anti-Tumor Ther. 2021, 2, 374–384. [Google Scholar] [CrossRef]
- Tang, W.; Putluri, V.; Ambati, C.R.; Dorsey, T.H.; Putluri, N.; Ambs, S. Liver- and Microbiome-derived Bile Acids Accumulate in Human Breast Tumors and Inhibit Growth and Improve Patient Survival. Clin. Cancer Res. 2019, 25, 5972–5983. [Google Scholar] [CrossRef]
- de Aguiar Vallim, T.Q.; Tarling, E.J.; Edwards, P.A. Pleiotropic roles of bile acids in metabolism. Cell Metab. 2013, 17, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Mikó, E.; Vida, A.; Kovács, T.; Ujlaki, G.; Trencsényi, G.; Márton, J.; Sári, Z.; Kovács, P.; Boratkó, A.; Hujber, Z.; et al. Lithocholic acid, a bacterial metabolite reduces breast cancer cell proliferation and aggressiveness. Biochim. Biophys. Acta Bioenerg. 2018, 1859, 958–974. [Google Scholar] [CrossRef] [PubMed]
- Swales, K.E.; Korbonits, M.; Carpenter, R.; Walsh, D.T.; Warner, T.D.; Bishop-Bailey, D. The farnesoid X receptor is expressed in breast cancer and regulates apoptosis and aromatase expression. Cancer Res. 2006, 66, 10120–10126. [Google Scholar] [CrossRef] [PubMed]
- Terrisse, S.; Derosa, L.; Iebba, V.; Ghiringhelli, F.; Vaz-Luis, I.; Kroemer, G.; Fidelle, M.; Christodoulidis, S.; Segata, N.; Thomas, A.M.; et al. Intestinal microbiota influences clinical outcome and side effects of early breast cancer treatment. Cell Death Differ. 2021, 28, 2778–2796. [Google Scholar] [CrossRef]
- Sholl, J.; Sepich-Poore, G.D.; Knight, R.; Pradeu, T. Redrawing therapeutic boundaries: Microbiota and cancer. Trends Cancer 2022, 8, 87–97. [Google Scholar] [CrossRef] [PubMed]
- El Bairi, K.; Jabi, R.; Trapani, D.; Boutallaka, H.; Ouled Amar Bencheikh, B.; Bouziane, M.; Amrani, M.; Afqir, S.; Maleb, A. Can the microbiota predict response to systemic cancer therapy, surgical outcomes, and survival? The answer is in the gut. Expert Rev. Clin. Pharmacol. 2020, 13, 403–421. [Google Scholar] [CrossRef] [PubMed]
- Parida, S.; Sharma, D. The power of small changes: Comprehensive analyses of microbial dysbiosis in breast cancer. Biochim. Biophys. Acta Rev. cancer 2019, 1871, 392–405. [Google Scholar] [CrossRef]
- Iida, N.; Dzutsev, A.; Stewart, C.A.; Smith, L.; Bouladoux, N.; Weingarten, R.A.; Molina, D.A.; Salcedo, R.; Back, T.; Cramer, S.; et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science 2013, 342, 967–970. [Google Scholar] [CrossRef]
- Viaud, S.; Saccheri, F.; Mignot, G.; Yamazaki, T.; Daillère, R.; Hannani, D.; Enot, D.P.; Pfirschke, C.; Engblom, C.; Pittet, M.J.; et al. The intestinal microbiota modulates the anticancer immune effects of cyclophosphamide. Science 2013, 342, 971–976. [Google Scholar] [CrossRef]
- Mendoza, L. Potential effect of probiotics in the treatment of breast cancer. Oncol. Rev. 2019, 13, 422. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M. Obesity and Dysbiosis. Korean J. Obes. 2015, 24, 121–125. [Google Scholar] [CrossRef]
- Abd El-Atti, S.; Wasicek, K.; Mark, S.; Hegazi, R. Use of probiotics in the management of chemotherapy-induced diarrhea: A case study. JPEN. J. Parenter. Enteral Nutr. 2009, 33, 569–570. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Moon, B. 85P Microbiome analysis in patients with breast cancer via an oral prebiotics therapy. ESMO Open 2023, 8, 101308. [Google Scholar] [CrossRef]
- Duan, D.; Chen, M.; Cui, W.; Liu, W.; Chen, X. Application of probiotics, prebiotics and synbiotics in patients with breast cancer: A systematic review and meta-analysis protocol for randomised controlled trials. BMJ Open 2022, 12, e064417. [Google Scholar] [CrossRef] [PubMed]
- Thu, M.S.; Ondee, T.; Nopsopon, T.; Farzana, I.A.K.; Fothergill, J.L.; Hirankarn, N.; Campbell, B.J.; Pongpirul, K. Effect of Probiotics in Breast Cancer: A Systematic Review and Meta-Analysis. Biology 2023, 12, 280. [Google Scholar] [CrossRef] [PubMed]
- Torres-Fuentes, C.; Schellekens, H.; Dinan, T.G.; Cryan, J.F. The microbiota-gut-brain axis in obesity. Lancet Gastroenterol. Hepatol. 2017, 2, 747–756. [Google Scholar] [CrossRef]
- Guirro, M.; Costa, A.; Gual-Grau, A.; Herrero, P.; Torrell, H.; Canela, N.; Arola, L. Effects from diet-induced gut microbiota dysbiosis and obesity can be ameliorated by fecal microbiota transplantation: A multiomics approach. PLoS ONE 2019, 14, e0218143. [Google Scholar] [CrossRef]
- Newman, T.M.; Vitolins, M.Z.; Cook, K.L. From the Table to the Tumor: The Role of Mediterranean and Western Dietary Patterns in Shifting Microbial-Mediated Signaling to Impact Breast Cancer Risk. Nutrients 2019, 11, 2565. [Google Scholar] [CrossRef]
- Lécuyer, L.; Dalle, C.; Lefevre-Arbogast, S.; Micheau, P.; Lyan, B.; Rossary, A.; Demidem, A.; Petera, M.; Lagree, M.; Centeno, D.; et al. Diet-Related Metabolomic Signature of Long-Term Breast Cancer Risk Using Penalized Regression: An Exploratory Study in the SU.VI.MAX Cohort. Cancer Epidemiol. Biomarkers Prev. 2020, 29, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Bouzari, B.; Hosseini-Fard, S.R.; Mazaheri, M.; Ahmadyousefi, Y.; Abdi, M.; Jalalifar, S.; Karimitabar, Z.; Teimoori, A.; Keyvani, H.; et al. Role of microbiota-derived short-chain fatty acids in nervous system disorders. Biomed. Pharmacother. 2021, 139, 111661. [Google Scholar] [CrossRef] [PubMed]
- Bodai, B.I.; Nakata, T.E. Breast Cancer: Lifestyle, the Human Gut Microbiota/Microbiome, and Survivorship. Perm. J. 2020, 24. [Google Scholar] [CrossRef] [PubMed]
- Xavier, J.B.; Young, V.B.; Skufca, J.; Ginty, F.; Testerman, T.; Pearson, A.T.; Macklin, P.; Mitchell, A.; Shmulevich, I.; Xie, L.; et al. The Cancer Microbiome: Distinguishing Direct and Indirect Effects Requires a Systemic View. Trends Cancer 2020, 6, 192–204. [Google Scholar] [CrossRef]
Figure 1.
Differences in microbial taxa between normal breast tissue (on the left) and breast cancer tissue (on the right) per various studies. (Created with BioRender).
Figure 1.
Differences in microbial taxa between normal breast tissue (on the left) and breast cancer tissue (on the right) per various studies. (Created with BioRender).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Avtanski, D.; Reddy, V.; Stojchevski, R.; Hadzi-Petrushev, N.; Mladenov, M. The Microbiome in the Obesity-Breast Cancer Axis: Diagnostic and Therapeutic Potential. Pathogens 2023, 12, 1402. https://doi.org/10.3390/pathogens12121402
AMA Style
Avtanski D, Reddy V, Stojchevski R, Hadzi-Petrushev N, Mladenov M. The Microbiome in the Obesity-Breast Cancer Axis: Diagnostic and Therapeutic Potential. Pathogens. 2023; 12(12):1402. https://doi.org/10.3390/pathogens12121402
Chicago/Turabian StyleAvtanski, Dimiter, Varun Reddy, Radoslav Stojchevski, Nikola Hadzi-Petrushev, and Mitko Mladenov. 2023. "The Microbiome in the Obesity-Breast Cancer Axis: Diagnostic and Therapeutic Potential" Pathogens 12, no. 12: 1402. https://doi.org/10.3390/pathogens12121402
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.