
Serial Interferon-Gamma Release Assay (IGRA) Testing to Monitor Treatment Responses in Cases of Feline Mycobacteriosis

 ,
,  and
and
Abstract
:1. Introduction
2. Results
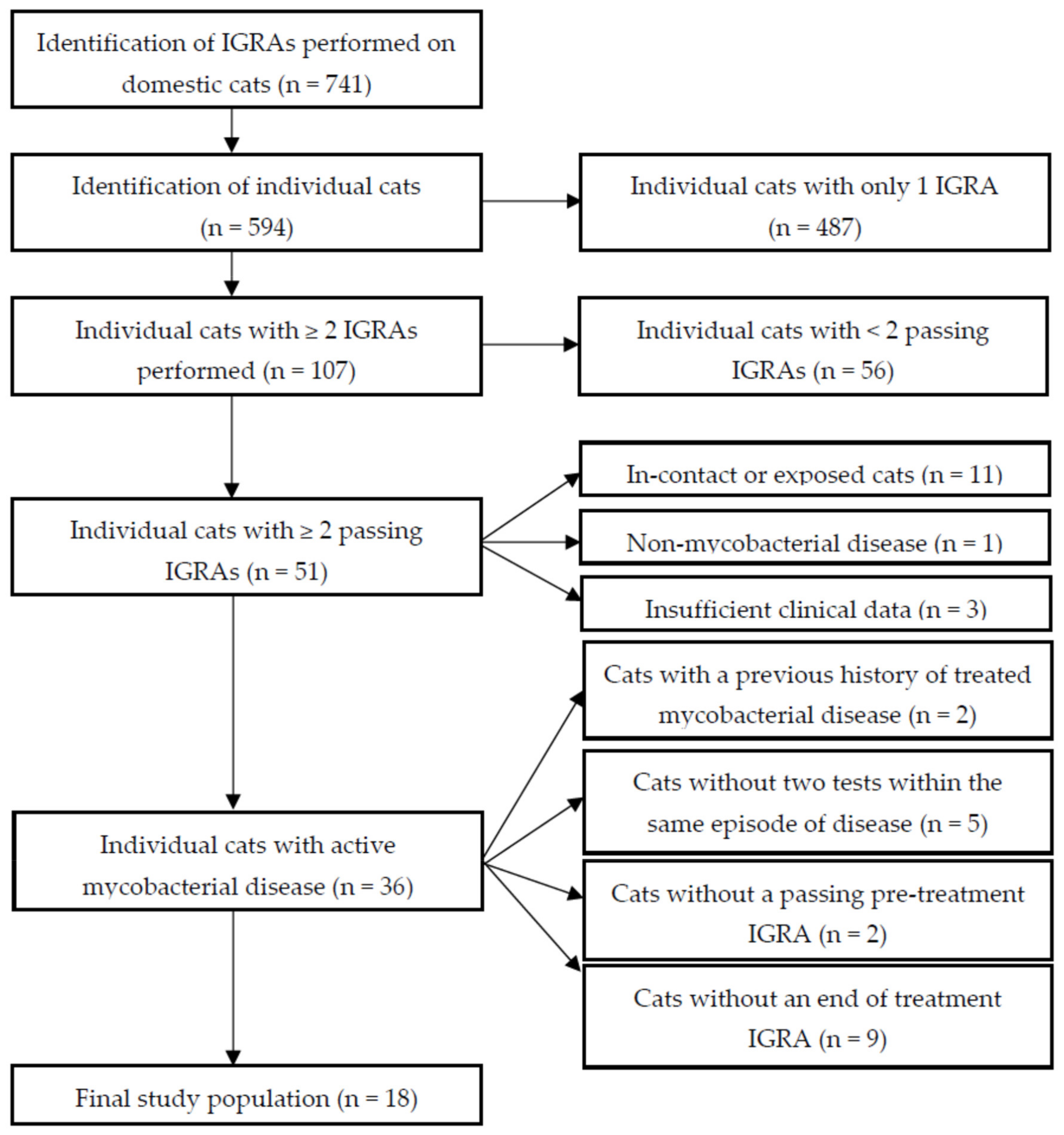
2.1. Study Population Selection and Summary Statistics
2.2. Qualitative Classification of IGRA Results
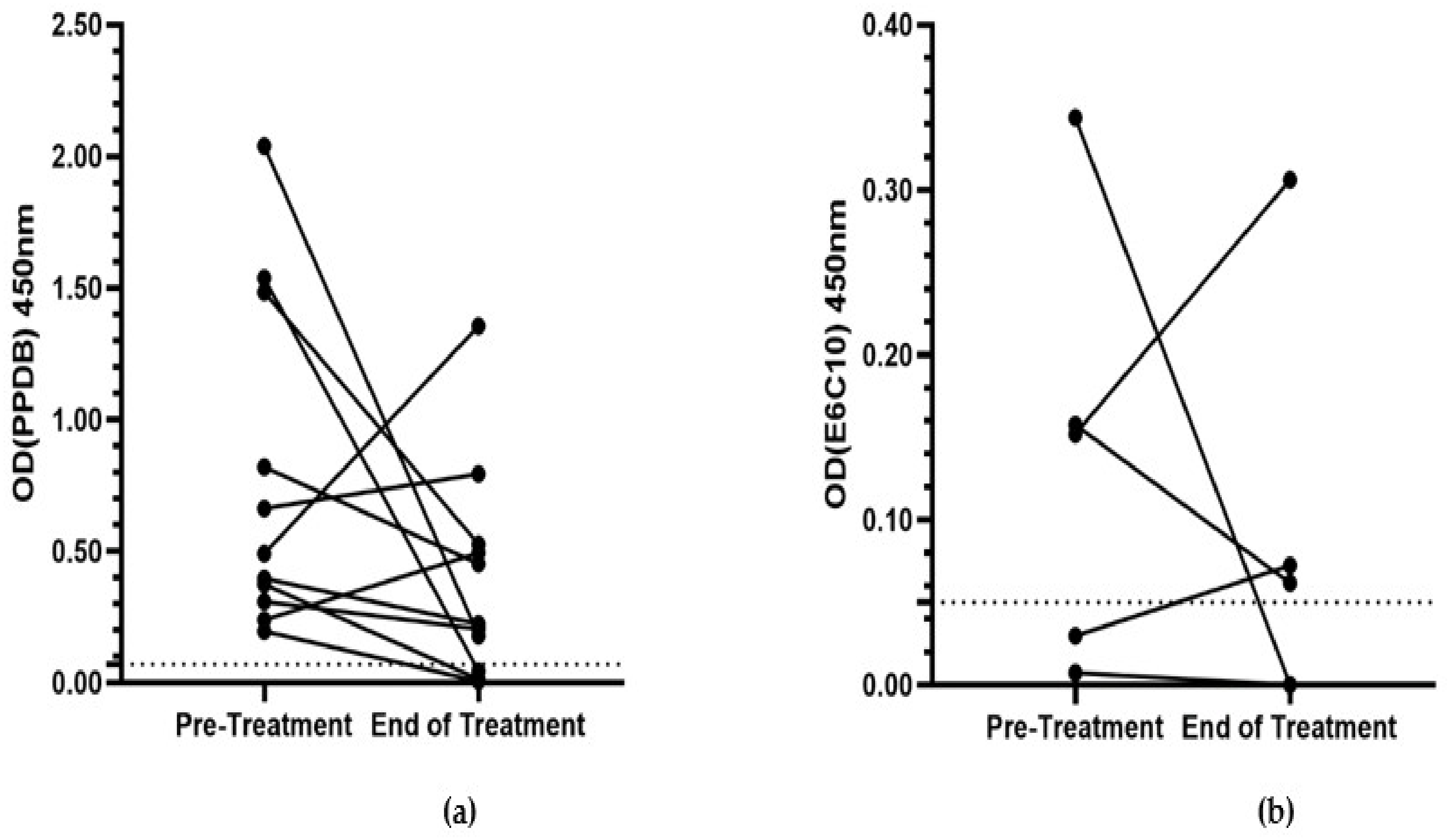
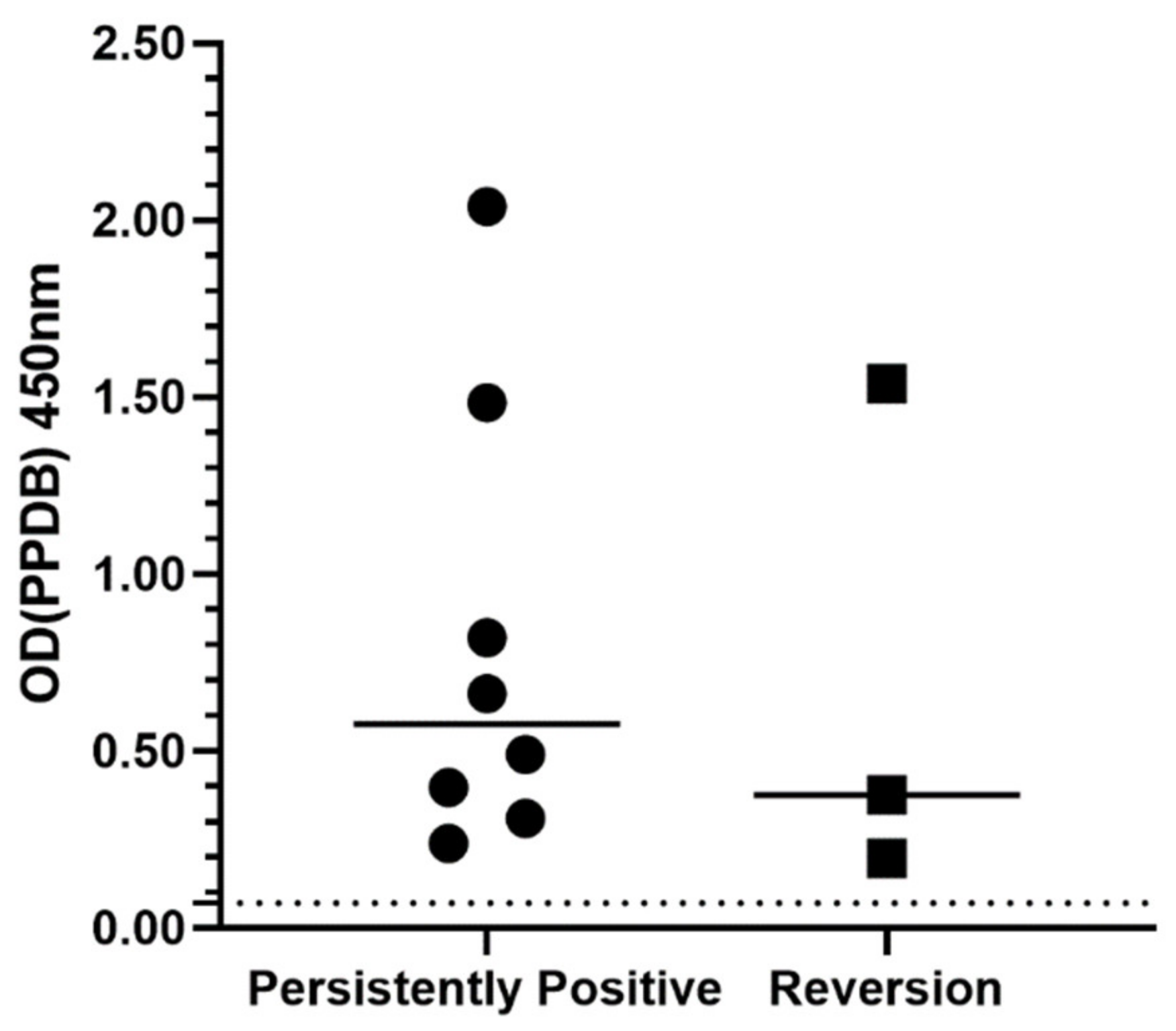
2.3. Quantitative Evaluation of IGRA Responses
2.4. Logistic Regression Analysis
3. Discussion
4. Materials and Methods
4.1. Study Population Selection
4.2. Qualitative Interpretation of Results
4.3. Quantitative Interpretation of Results
4.4. Identification of Factors Associated with IGRA Reversion and Recurrence of Disease
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gunn-Moore, D.A.; Gaunt, C.; Shaw, D.J. Incidence of mycobacterial infections in cats in Great Britain: Estimate from feline tissue samples submitted to diagnostic laboratories. Transbound. Emerg. Dis. 2013, 60, 338–344. [Google Scholar] [CrossRef]
- O’Halloran, C.; Gunn-Moore, D. Mycobacteria in cats: An update. Practice 2017, 39, 399–406. [Google Scholar] [CrossRef]
- Wood, P.R.; Corner, L.A.; Rothel, J.S.; Baldock, C.; Jones, S.L.; Cousins, D.B.; McCormick, B.S.; Francis, B.R.; Creeper, J.; Tweddle, N.E. Field comparison of the interferon-gamma assay and the intradermal tuberculin test for the diagnosis of bovine tuberculosis. Aust. Vet. J. 1991, 68, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Waters, W.R.; Palmer, M.V.; Thacker, T.C.; Orloski, K.; Nol, P.; Harrington, N.P.; Olsen, S.C.; Nonnecke, B.J. Blood culture and stimulation conditions for the diagnosis of tuberculosis in cervids by the Cervigam assay. Vet. Rec. 2008, 162, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pai, M.; Denkinger, C.M.; Kik, S.V.; Rangaka, M.X.; Zwerling, A.; Oxlade, O.; Metcalfe, J.Z.; Cattamanchi, A.; Dowdy, D.W.; Dheda, K.; et al. Gamma Interferon Release Assays for Detection of Mycobacterium tuberculosis Infection. Clin. Microbiol. Rev. 2014, 27, 3–20. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, S.G.; Gruffydd-Jones, T.; Gunn-Moore, D.; Jahans, K. Interferon-γ test for feline tuberculosis. Vet. Rec. 2008, 162, 453–454. [Google Scholar] [CrossRef]
- Andersen, P.; Munk, M.E.; Pollock, J.M.; Doherty, T.M. Specific immune-based diagnosis of tuberculosis. Lancet 2000, 356, 1099–1104. [Google Scholar] [CrossRef]
- Gunn-Moore, D.A.; McFarland, S.E.; Brewer, J.I.; Crawshaw, T.R.; Clifton-Hadley, R.S.; Kovalik, M.; Shaw, D.J. Mycobacterial disease in cats in Great Britain: I. Culture results, geographical distribution and clinical presentation of 339 cases. J. Feline Med. Surg. 2011, 13, 934–944. [Google Scholar] [CrossRef]
- Rhodes, S.G.; Gunn-Moore, D.; Boschiroli, M.L.; Schiller, I.; Esfandiari, J.; Greenwald, R.; Lyashchenko, K.P. Comparative study of IFNγ and antibody tests for feline tuberculosis. Vet. Immunol. Immunopathol. 2011, 144, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Riley, L.W.; Colford, J.M., Jr. Interferon-γ assays in the immunodiagnosis of tuberculosis: A systematic review. Lancet Infect. Dis. 2004, 4, 761–776. [Google Scholar] [CrossRef]
- Kaech, S.M.; Wherry, E.J.; Ahmed, R. Effector and memory T-cell differentiation: Implications for vaccine development. Nat. Rev. Immunol. 2002, 2, 251–262. [Google Scholar] [CrossRef]
- Klenerman, P.; Cerundolo, V.; Dunbar, P.R. Tracking T cells with tetramers: New tales from new tools. Nat. Rev. Immunol. 2002, 2, 263–272. [Google Scholar] [CrossRef]
- Pathan, A.A.; Wilkinson, K.A.; Klenerman, P.; McShane, H.; Davidson, R.N.; Pasvol, G.; Hill, A.V.; Lalvani, A. Direct ex vivo analysis of antigen-specific IFN-γ-secreting CD4 T cells in Mycobacterium tuberculosis-infected individuals: Associations with clinical disease state and effect of treatment. J. Immunol. 2001, 167, 5217–5225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalvani, A. Counting antigen-specific T cells: A new approach for monitoring response to tuberculosis treatment? Clin. Infect. Dis. 2004, 38, 757–759. [Google Scholar] [CrossRef] [Green Version]
- Carrara, S.; Vincenti, D.; Petrosillo, N.; Amicosante, M.; Girardi, E.; Goletti, D. Use of a T cell-based assay for monitoring efficacy of antituberculosis therapy. Clin. Infect. Dis. 2004, 38, 754–756. [Google Scholar] [CrossRef] [Green Version]
- Bosshard, V.; Roux-Lombard, P.; Perneger, T.; Metzger, M.; Vivien, R.; Rochat, T.; Janssens, J.-P. Do results of the T-SPOT.TB interferon- γ release assay change after treatment of tuberculosis? Respir. Med. 2009, 103, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Sauzullo, I.; Mengoni, F.; Lichtner, M.; Massetti, A.P.; Rossi, R.; Iannetta, M.; Marocco, R.; Borgo, C.D.; Soscia, F.; Vullo, V.; et al. In Vivo and In Vitro Effects of Antituberculosis Treatment on Mycobacterial Interferon-γ T Cell Response. PLoS ONE 2009, 4, e5187. [Google Scholar] [CrossRef] [Green Version]
- Bugiani, M.; Bonora, S.; Carosso, A.; Piccioni, P.; Cavallero, M.; Mondo, A.; Ghisetti, V. The effect of antituberculosis treatment on interferon-γ release assay results. Monaldi Arch. Chest Dis. 2011, 75, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Clifford, V.; He, Y.; Zufferey, C.; Connell, T.; Curtis, N. Interferon gamma release assays for monitoring the response to treatment for tuberculosis: A systematic review. Tuberculosis 2015, 95, 639–650. [Google Scholar] [CrossRef] [PubMed]
- Bocchino, M.; Chairadonna, P.; Matarese, A.; Bruzzese, D.; Salvatores, M.; Tronci, M.; Moscariello, E.; Galati, D.; Alma, M.G.; Sanduzzi, A.; et al. Limited usefulness of QuantiFERON-TB Gold In-Tube® for monitoring anti-tuberculosis therapy. Respir. Med. 2010, 104, 1551–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nenadić, N.; Kirin, B.K.; Letoja, I.Z.; Plavec, D.; Topić, R.Z.; Dodig, S. Serial interferon-γ release assay in children with latent tuberculosis infection and children with tuberculosis. Pediatr. Pulmonol. 2012, 47, 401–408. [Google Scholar] [CrossRef]
- Major, A.; O’Halloran, C.; Holmes, A.; Lalor, S.; Littler, R.; Spence, S.; Schwarz, T.; Gunn-Moore, D. Use of computed tomography imaging during long-term follow-up on nine feline tuberculosis cases. J. Feline Med. Surg. 2018, 20, 189–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, E.; Weizenegger, M.; Rüsch-Gerdes, S.; Niemann, S. Evaluation of Genotype MTBC Assay for Differentiation of Clinical Mycobacterium tuberculosis Complex Isolates. J. Clin. Microbiol. 2003, 41, 2672–2675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunn-Moore, D.A.; Jenkins, P.A.; Lucke, V.M. Feline tuberculosis: A literature review and discussion of 19 cases caused by an unusual mycobacterial variant. Vet. Rec. 1996, 138, 53–58. [Google Scholar] [CrossRef]
- Bennett, A.D.; Lalor, S.; Schwarz, T.; Gunn-Moore, D.A. Radiographic findings in cats with mycobacterial infections. J. Feline Med. Surg. 2011, 13, 718–724. [Google Scholar] [CrossRef]
- Major, A.; Holmes, A.; Warren-Smith, C.; Lalor, S.; Littler, R.; Schwarz, T.; Gunn-Moore, D. Computed tomographic findings in cats with mycobacterial infection. J. Feline Med. Surg. 2016, 18, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Gunn-Moore, D.A.; McFarland, S.E.; Schock, A.; Brewer, J.I.; Crawshaw, T.R.; Clifton-Hadley, R.S.; Shaw, D.J. Mycobacterial disease in a population of 339 cats in Great Britain: II. Histopathology of 225 cases, and treatment and outcome of 184 cases. J. Feline Med. Surg. 2011, 13, 945–952. [Google Scholar] [CrossRef]
- Denkinger, C.M.; Pai, M.; Patel, M.; Menzies, D. Gamma Interferon Release Assay for Monitoring of Treatment Response for Active Tuberculosis: An Explosion in the Spaghetti Factory. J. Clin. Microbiol. 2013, 51, 607–610. [Google Scholar] [CrossRef] [Green Version]
- Tapaninen, P.; Korhonen, A.; Pusa, L.; Seppala, I.; Tuuminen, T. Effector memory T-cells dominate immune responses in tuberculosis treatment: Antigen or bacteria persistence? Int. J. Tuberc. Lung Dis. 2010, 14, 347–355. [Google Scholar]
- De La Rua-Domenech, R.; Goodchild, A.T.; Vordermeier, H.M.; Hewinson, R.G.; Christiansen, K.H.; Clifton-Hadley, R.S. Ante mortem diagnosis of tuberculosis in cattle: A review of the tuberculin tests, γ-interferon assay and other ancillary diagnostic techniques. Res. Vet. Sci. 2006, 81, 190–210. [Google Scholar] [CrossRef]
- O’Halloran, C.; Hope, J.C.; Dobromylskyj, M.; Burr, P.; McDonald, K.; Rhodes, S.; Roberts, T.; Dampney, R.; De la Rua-Domenech, R.; Robinson, N.; et al. An outbreak of tuberculosis due to Mycobacterium bovis infection in a pack of English Foxhounds (2016–2017). Transbound. Emerg. Dis. 2018, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Van Zyl-Smit, R.N.; Zwerling, A.; Dheda, K.; Pai, M. Within-Subject Variability of Interferon-g Assay Results for Tuberculosis and Boosting Effect of Tuberculin Skin Testing: A Systematic Review. PLoS ONE 2009, 4, e8517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, V.; Perry, S.; Parsonnet, J.; Banaei, N. Clinical application and limitations of interferon-gamma release assays for the diagnosis of latent tuberculosis infection. Clin. Infect. Dis. 2011, 52, 1031–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chee, C.B.E.; KhinMar, K.W.; Gan, S.H.; Barkham, T.M.; Koh, C.K.; Shen, L.; Wang, Y.T. Tuberculosis treatment effect on T-cell interferon-γ responses to Mycobacterium tuberculosis-specific antigens. Eur. Respir. J. 2010, 36, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Komiya, K.; Ariga, H.; Nagai, H.; Kurashima, A.; Shoji, S.; Ishii, H.; Nakajima, Y. Reversion rates of QuantiFERON-TB Gold are related to pre-treatment IFN-gamma levels. J. Infect. 2011, 63, 48–53. [Google Scholar] [CrossRef]
- Montecino-Rodriguez, E.; Berent-Maoz, B.; Dorshkind, K. Causes, consequences, and reversal of immune system aging. J. Clin. Investig. 2013, 123, 958–965. [Google Scholar] [CrossRef]
- Day, M.J. Ageing, Immunosenescence and Inflammageing in the Dog and Cat. J. Comp. Pathol. 2010, 142, S60–S69. [Google Scholar] [CrossRef]
- Campbell, D.J.; Rawlings, J.M.; Koelsch, S.; Wallace, J.; Strain, J.J.; Hannigan, B.M. Age-related differences in parameters of feline immune status. Vet. Immunol. Immunopathol. 2004, 100, 73–80. [Google Scholar] [CrossRef]
- Dean, G.S.; Rhodes, S.G.; Coad, M.; Whelan, A.O.; Wheeler, P.; Villareal-Ramos, B.; Mead, E.; Johnson, L.; Clifford, D.J.; Hewinson, R.G.; et al. Isoniazid treatment of Mycobacterium bovis in cattle as a model for human tuberculosis. Tuberculosis 2008, 88, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yoon, H.I.; Park, K.U.; Lee, C.T.; Lee, J.H. The impact of previous tuberculosis history on T-SPOT.TB® interferon-gamma release assay results. Int. J. Tuberc. Lung Dis. 2011, 15, 510–516. [Google Scholar] [CrossRef]
- Gunn-Moore, D.A. Feline mycobacterial infections. Vet. J. 2014, 201, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Schiller, I.; Waters, W.R.; Vordermeier, H.M.; Nonnecke, B.; Welsh, M.; Keck, N.; Whelan, A.; Sigafoose, T.; Stamm, C.; Palmer, M.; et al. Optimization of a Whole-Blood Gamma Interferon Assay for Detection of Mycobacterium bovis-Infected Cattle. Clin. Vaccine Immunol. 2009, 16, 1196–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, S.; Holder, T.; Clifford, D.; Dexter, I.; Brewer, J.; Smith, N.; Waring, L.; Crawshaw, T.; Gillgan, S.; Lyashchenko, K.; et al. Evaluation of Gamma Interferon and Antibody Tuberculosis Tests in Alpacas. Clin. Vaccine Immunol. 2012, 19, 1677–1683. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R, 1.2.1335; RStudio, Inc.: Boston, MA, USA, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Case | Age (Years) | Gender | Breed | Culture/PCR | FeLV Ag/FIV Ab | Serum Calcium Concentration | Clinical Disease | Treatment & Duration (Months) | Outcome & Follow-up Duration (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 7 | MN | DSH | MTBC a | NP | NP | Retrobulbar ocular mass, submandibular lymphadenopathy | R/A/P (3); surgery | Resolved (9) |
| 2 | 3 | FN | Siamese | M. bovisb | NP | NP | Lip mass, submandibular lymphadenopathy, bronchointerstitial lung pattern c | R/A/P (6) | Resolved (18) |
| 3 | 0.5 | MN | DSH | MTBC a | NP | Normal (total) | Interstitial lung pattern c | R/A/P (3); R/P (15) | Resolved (3) |
| 4 | 8.5 | MN | DSH | NP | Negative | Increased (total) Normal (ionised) | Nasal mass, submandibular lymphadenopathy | R/A/P (6) | Resolved (48) |
| 5 | 7 | MN | Siamese | M. microtia,b | Negative | Normal (total) | Multiple cutaneous masses, bronchointerstitial lung pattern c | R/A/P (2); R/P (6) | Resolved (12) |
| 6 | 7 | MN | DSH | NP | NP | NP | Bilateral submandibular lymphadenopathy, bronchointerstitial lung pattern c | R/A/P (7) | Recurrence of submandibular lymphadenopathy 27 months later; retreated with R/A/P, lost to follow-up |
| 7 | 6 | MN | Siamese | MTBC a | NP | NP | Submandibular mass, submandibular lymphadenopathy, bronchial lung pattern c | R/A/P (3) | Re-presented with mass on lip 17 months later; retreated with R/A/P for four months, resolved |
| 8 | 11 | MN | Siamese | NP | Negative | Increased (ionised) | Tonsillar lymphoid hyperplasia, alveolar lung pattern c | R/A/M (3); A/M (12) | Resolved (12) |
| 9 | 7 | MN | DSH | M. bovisb | NP | NP | Conjunctival mass | R/A/P (3); A/P (2) | Resolved (6) |
| 10 | 6.5 | FN | DSH | Negative b | NP | NP | Multiple cutaneous masses, peripheral lymphadenopathy bronchointerstitial lung pattern c | R/A/P (8) | Recurrence of cutaneous masses and peripheral lymphadenopathy eight months later; euthanased |
| 11 | 5 | MN | DSH | M. bovisb | NP | Normal (total) | Discharging cutaneous mass, perihilar lymphadenopathy, interstitial lung pattern c | R/A/P (6); A/P (18) | Resolved (42) |
| 12 | 13 | MN | Bengal | NP | NP | Normal (total) | Generalised lymphadenopathy, bronchointerstitial lung pattern d | R/A/P (9) | Recurrence of clinical signs three months later; euthanased |
| 13 | 5.5 | MN | DSH | Negative b | NP | NP | Generalised lymphadenopathy, bronchointerstitial lung pattern c | R/A/P (6) | Resolved (6) |
| 14 | 7.5 | MN | DSH | NP | Negative | NP | Multiple cutaneous masses, submandibular lymphadenopathy | R/P/Cd (3); R/A/P (3) | Resolved (36) |
| 15 | 3 | FN | DSH | NP | NP | NP | Submandibular lymphadenopathy | E/D/P (6) | Resolved (6) |
| 16 | 1.5 | MN | Tonkinese | NP | Negative | Increased (total, ionised) | Diffuse interstitial lung pattern c | R/Ct/P (8) | Recurrence of clinical signs 16 months later; retreated with R/Ct/P for eight months, resolved |
| 17 | 8.5 | MN | DSH | NP | NP | Normal (total) | Generalised lymphadenopathy | R/E/P (4) | Resolved (24) |
| 18 | 2 | MN | DSH | Negative a,b | NP | Increased (total) | Panuveitis, bronchointerstitial lung pattern d | R/A/P (3); surgery | Resolved (12) |
| Case | Pre-Treatment IGRA | IGRA Result | End-of-Treatment IGRA | IGRA Result | Pattern |
|---|---|---|---|---|---|
| 1 | Positive | B > A | Positive | B > A | Persistent positive |
| 2 | Positive | B > A | Positive | B > A | Persistent positive |
| 3 | Positive | B > A | Positive | B > A, E positive | Persistent positive |
| 4 | Positive | B > A | Positive | B > A | Persistent positive |
| 5 | Positive | B > A | Positive | B > A | Persistent positive |
| 6 | Positive | B > A | Positive | B > A | Persistent positive |
| 7 | Positive | B > A | Positive | B > A | Persistent positive |
| 8 | Positive | B > A | Positive | B > A, E positive | Persistent positive |
| 9 | Positive | B > A, E positive | Positive | B > A, E positive | Persistent positive |
| 10 | Positive | B > A | Positive | B > A | Persistent positive |
| 11 | Positive | B > A, E positive | Positive | B > A, E positive | Persistent positive |
| 12 | Positive | B > A | Positive | B > A | Persistent positive |
| 13 | Positive | B > A | Positive | B > A | Persistent positive |
| 14 | Positive | B > A | Positive | B > A | Persistent positive |
| 15 | Positive | B > A | Negative | Negative | Reversion |
| 16 | Positive | B > A | Negative | Negative | Reversion |
| 17 | Positive | B > A | Negative | Negative | Reversion |
| 18 | Positive | B > A, E positive | Negative | Negative | Reversion |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitchell, J.L.; O’Halloran, C.; Stanley, P.; McDonald, K.; Burr, P.; Gunn-Moore, D.A.; Hope, J.C. Serial Interferon-Gamma Release Assay (IGRA) Testing to Monitor Treatment Responses in Cases of Feline Mycobacteriosis. Pathogens 2021, 10, 657. https://doi.org/10.3390/pathogens10060657
Mitchell JL, O’Halloran C, Stanley P, McDonald K, Burr P, Gunn-Moore DA, Hope JC. Serial Interferon-Gamma Release Assay (IGRA) Testing to Monitor Treatment Responses in Cases of Feline Mycobacteriosis. Pathogens. 2021; 10(6):657. https://doi.org/10.3390/pathogens10060657
Chicago/Turabian StyleMitchell, Jordan L., Conor O’Halloran, Paul Stanley, Kieran McDonald, Paul Burr, Danièlle A. Gunn-Moore, and Jayne C. Hope. 2021. "Serial Interferon-Gamma Release Assay (IGRA) Testing to Monitor Treatment Responses in Cases of Feline Mycobacteriosis" Pathogens 10, no. 6: 657. https://doi.org/10.3390/pathogens10060657