Can Parenting Practices Explain the Differences in Beverage Intake According to Socio-Economic Status: The Toybox-Study

 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Background
2.2. Participants
2.3. Measures
2.3.1. Core Questionnaire
Socio-Demographic Variables
Parenting Practices
2.3.2. Food Frequency Questionnaire
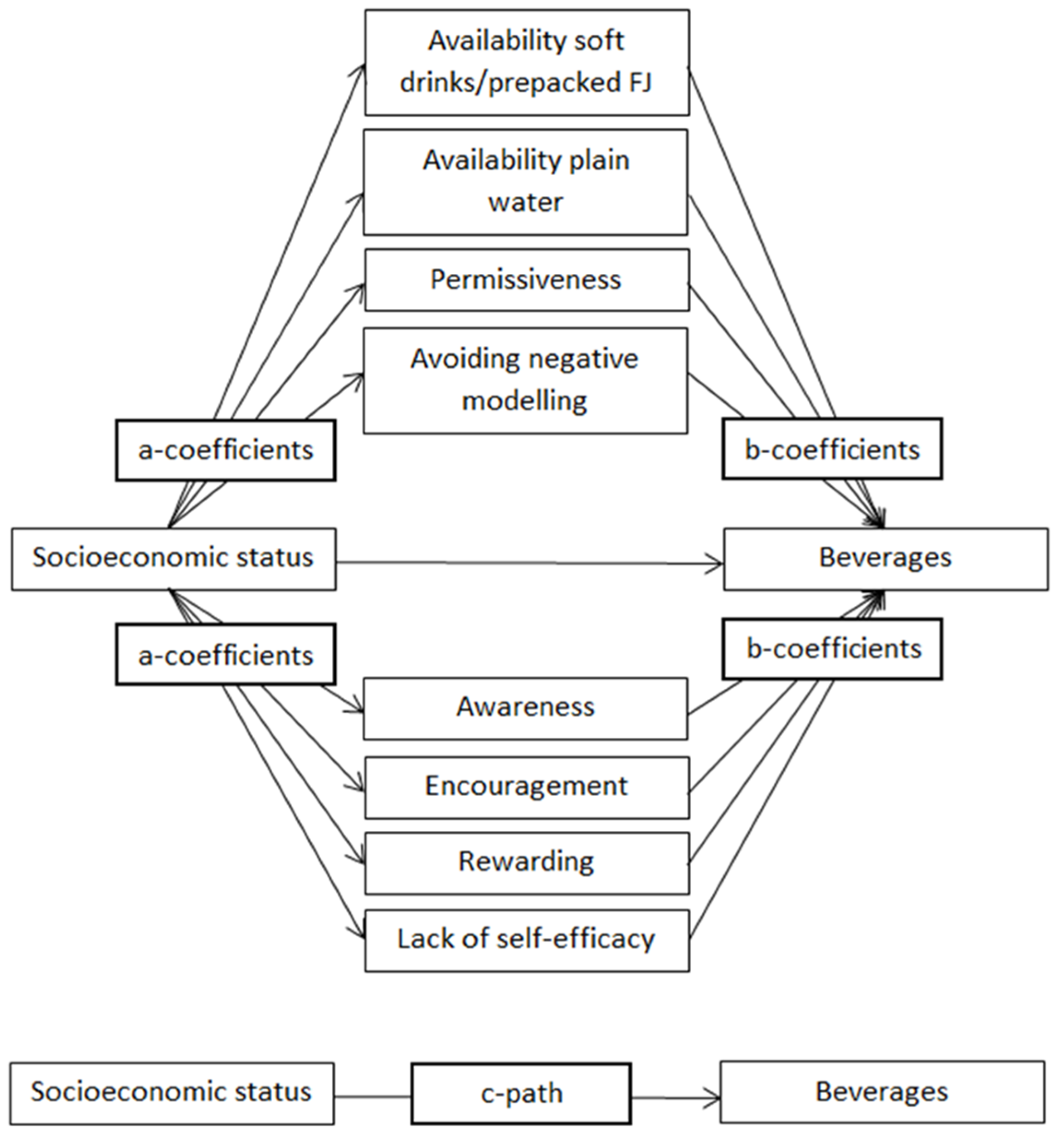
2.4. Statistical Analyses
3. Results
3.1. Population Characteristics
3.2. Mediation Analyses on the Country-Specific Samples (See also Table 3)
3.2.1. Associations between SES and Beverage Intake (c-Path)
3.2.2. Associations between SES and Potential Mediators (a-Coefficients)
3.2.3. Associations between Potential Mediators and Beverage Intake Controlled for SES (b-Coefficients)
Plain Water
Soft Drinks
Prepacked Fruit Juice
3.2.4. Mediating Effect of Parenting Practices on the Associations between SES and Beverage Intake (ab-Coefficients)
3.3. Mediation Analyses on the Country-Specific Samples (See also Table 4, the Most Important Results Are Discussed Below)
3.3.1. Associations between SES and Beverage Intake (c-Path)
3.3.2. Associations between SES and Potential Mediators (a-Coefficients)
3.3.3. Associations between Potential Mediators and Beverage Intake (b-Coefficients)
3.3.4. Mediating Effect of Parenting Practices on the Associations between SES and Beverage Intake (ab-Coefficients)
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pinket, A.S.; De Craemer, M.; Maes, L.; De Bourdeaudhuij, I.; Cardon, G.; Androutsos, O.; Koletzko, B.; Moreno, L.; Socha, P.; Iotova, V.; et al. Water intake and beverage consumption of preschoolers from six European countries and associations with socio-economic status: The ToyBox-study. Public Health Nutr. 2015, 18, 1–11. [Google Scholar]
- DeBoer, M.D.; Scharf, R.J.; Demmer, R.T. Sugar-sweetened beverages and weight gain in 2- to 5-year-old children. Pediatrics 2013, 132, 413–420. [Google Scholar] [CrossRef] [PubMed]
- De Ruyter, J.C.; Olthof, M.R.; Seidell, J.C.; Katan, M.B. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N. Engl. J. Med. 2012, 367, 1397–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, A.K.; Birch, L.L. Does parenting affect children’s eating and weight status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Maccoby, E.D.; Martin, J.A. Socialization in the context of the family: Parent-child interaction. In Socialization, Personality and Social Development; Mussen, P.H., Hetherington, E.M., Eds.; Wiley: New York, NY, USA, 1983; Volume 4. [Google Scholar]
- Darling, N.; Steinberg, L. Parenting style as context: An integrative model. Psychol. Bull. 1993, 113, 487–496. [Google Scholar] [CrossRef]
- Van Lippevelde, W.; te Velde, S.J.; Verloigne, M.; De Bourdeaudhuij, I.; Manios, Y.; Bere, E.; Jan, N.; Fernández-Alvira, J.M.; Chinapaw, M.J.; Bringolf-Isler, B.; et al. Associations between home- and family-related factors and fruit juice and soft drink intake among 10- to 12-year old children. The ENERGY project. Appetite 2013, 61, 59–65. [Google Scholar] [CrossRef] [PubMed]
- De Coen, V.; Vansteelandt, S.; Maes, L.; Huybrechts, I.; De Bourdeaudhuij, I.; Vereecken, C. Parental socioeconomic status and soft drink consumption of the child. The mediating proportion of parenting practices. Appetite 2012, 59, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Grimm, G.C.; Harnack, L.; Story, M. Factors associated with soft drink consumption in school-aged children. J. Am. Diet. Assoc. 2004, 104, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Li, R.; Birch, L. Mothers’ child-feeding practices are associated with children’s sugar-sweetened beverage intake. J. Nutr. 2015, 145, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Van der Horst, K.; Kremers, S.; Ferreira, I.; Singh, A.; Oenema, A.; Brug, J. Perceived parenting style and practices and the consumption of sugar-sweetened beverages by adolescents. Health Educ. Res. 2007, 22, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Van Grieken, A.; Renders, C.M.; van de Gaar, V.M.; Hirasing, R.A.; Raat, H. Associations between the home environment and children’s sweet beverage consumption at 2-year follow-up: The ‘Be active, eat right’ study. Pediatr. Obes. 2015, 10, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Summerbell, C.D.; Walters, E.; Edmunds, L.; Kelly, S.; Brown, T.; Campbell, K.J. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2005, CD001871. [Google Scholar] [CrossRef]
- MacFarlane, A.; Crawford, D.; Ball, K.; Savige, G.; Worsley, A. Adolescent home food environment and socio-economic position. Asia Pac. J. Clin. Nutr. 2007, 16, 748–756. [Google Scholar] [PubMed]
- Manios, Y.; Grammatikaki, E.; Androutsos, O.; Chinapaw, M.J.; Gibson, E.L.; Buijs, G.; Iotova, V.; Socha, P.; Annemans, L.; Wildgruber, A.; et al. A systematic approach for the development of a kindergarten-based intervention for the prevention of obesity in preschool age children: The ToyBox-study. Obes. Rev. 2012, 13, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Androutsos, O.; Katsarou, C.; Iotova, V.; Socha, P.; Geyer, C.; Moreno, L.; Koletzko, B.; De Bourdeaudhuij, I. Designing and implementing a kindergarten-based, family-involved intervention to prevent obesity in early childhood: The ToyBox-study. Obes. Rev. 2014, 15, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Mouratidou, T.; Miguel, M.L.; Androutsos, O.; Manios, Y.; De Bourdeaudhuij, I.; Cardon, G.; Kulaga, Z.; Socha, P.; Galcheva, S.; Iotova, V.; et al. Tools, harmonization and standardization procedures of the impact and outcome evaluation indices obtained during a kindergarten-based, family-involved intervention to prevent obesity in early childhood: The ToyBox-study. Obes. Rev. 2014, 15, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.K.; Kelly, F.D. Relationships among involvement, attachment, and behavioral problems in adolescence: Examining father’s influence. J. Early Adolesc. 2005, 25, 168–196. [Google Scholar]
- De Coen, V.; De Bourdeaudhuij, I.; Verbestel, V.; Maes, L.; Vereecken, C. Risk factors for childhood overweight: A 30-month longitudinal study of 3- to 6-year-old children. Public Health Nutr. 2014, 17, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Brug, J.; van Stralen, M.M.; te Velde, S.J.; Chinapaw, M.J.; De Bourdeaudhuij, I.; Lien, N.; Bere, E.; Maskini, V.; Singh, A.S.; Maes, L.; et al. Differences in weight status and energy-balance related behaviors among schoolchildren across Europe: The ENERGY-project. PLoS ONE 2012, 7, e34742. [Google Scholar]
- Singh, A.S.; Chinapaw, M.J.; Uijtdewilligen, L.; Vik, F.N.; van Lippevelde, W.; Fernández-Alvira, J.M. Test-retest reliability and construct validity of the ENERGY-parent questionnaire on parenting practices, energy balance-related behaviours and their potential behavioural determinants: The ENERGY-project. BMC Res. Notes 2012, 5, 434. [Google Scholar] [PubMed]
- González-Gil, E.M.; Mouratidou, T.; Cardon, G.; Androutsos, O.; De Bourdeaudhuij, I.; Góźdź, M.; Usheva, N.; Birnbaum, J.; Manios, Y.; Moreno, L.A.; et al. Reliability of primary caregivers reports on lifestyle behaviours of European pre-school children: The ToyBox-study. Obes. Rev. 2014, 15, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Huybrechts, I.; De Backer, G.; De Bacquer, D.; Maes, L.; De Henauw, S. Relative validity and reproducibility of a food-frequency questionnaire for estimating food intakes among Flemish preschoolers. Int. J. Environ. Res. Public Health 2009, 6, 382–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, D.P. Introduction to Statistical Mediation Analysis; Erlbaum: New York, NY, USA, 2008. [Google Scholar]
- Vereecken, C.A.; Keukelier, E.; Maes, L. Influence of mother’s educational level on food parenting practices and food habits of young children. Appetite 2009, 43, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Van Ansem, W.J.C.; Van Lenthe, F.J.; Schrijvers, C.T.M.; Rodenburg, G.; van de Mheen, D. Socio-economic inequalities in children’s snack consumption and sugar-sweetened beverage consumption: The contribution of home environmental factors. Br. J. Nutr. 2014, 112, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Bountziouka, V.; Trichopoulou, A. Soft drinks: Time trends and correlates in twenty-four European countries. A cross-national study using the DAFNE (Data Food Networking) databank. Public Health Nutr. 2010, 13, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; De Henauw, S.; González-Gross, M.; Kersting, M.; Molnár, D.; Gottrand, F.; Barrios, L.; Sjöström, M.; Manios, Y.; Gilbert, C.C.; et al. Design and implementation of the Healthy Lifestyle in Europe by Nutrition in Adolescence Cross-Sectional Study. Int. J. Obes. 2008, 32, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Van Stralen, M.M.; te Velde, S.J.; Singh, A.S.; De Bourdeaudhuij, I.; Martens, M.K.; van der Sluis, M.; Manios, Y.; Grammatikaki, E.; Chinapaw, M.J.M.; Maes, L.; et al. European Energy balance Research to prevent excessive weight Gain among Youth (ENERGY) project: Design and methodology of the ENERGY cross-sectional survey. BMC Public Health 2011, 11, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raaijmakers, L.G.; Gevers, D.W.; Teuscher, D.; Kremers, S.P.; van Assema, P. Emotional and instrumental feeding practices of Dutch mothers regarding foods eaten between main meals. BMC Public Health 2014, 14, 171. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Factor | Question Item | Answer Categories |
|---|---|---|
| Availability soft drinks/prepacked fruit juice (Cronbach α = 0.68) |
| 1 = strongly disagree– 5 = strongly agree |
| Availability plain water (Cronbach α = 0.41) |
| 1 = strongly disagree– 5 = strongly agree |
| Permissiveness towards soft drinks/prepacked fruit juice (Cronbach α = 0.62) |
| 1 = strongly disagree– 5 = strongly agree |
| Avoiding negative modelling | If I would like to drink soft drinks or prepacked juices, I would try to restrain myself because of the presence of my child. | 1 = strongly disagree– 5 = strongly agree |
| Awareness (Cronbach α = 0.60) |
| 1 = strongly disagree– 5 = strongly agree |
| Encouragement | I encourage my child to drink water. | 1 = strongly disagree– 5 = strongly agree |
| Rewarding | I give soft drinks or prepacked juices to my child as a reward or to comfort him/her. | 1 = strongly disagree– 5 = strongly agree |
| Lack of self-efficacy | I find it difficult to give my child water if he/she wants soft drinks or prepacked juices. | 1 = strongly disagree– 5 = strongly agree |
| Total | Belgium | Bulgaria | Germany | Greece | Poland | Spain | |
|---|---|---|---|---|---|---|---|
| N | 6776 | 917 | 752 | 1139 | 1733 | 1384 | 851 |
| Age | 4.8 ± 0.4 | 4.4 ± 0.5 | 4.9 ± 0.3 | 4.5 ± 0.5 | 4.9 ± 0.3 | 4.9 ± 0.3 | 4.9 ± 0.3 |
| Gender (% male) | 52.1% | 52.2% | 50.5% | 51.9% | 50.8% | 53.0% | 54.8% |
| SES *, % lower SES (=≤14 years of education) | 39.8% | 34.4% | 40.8% | 51.6% | 51.3% | 21.0% | 36.1% |
| Ethnicity (One or both parents are not born in the country of residence) | 16% | 12.4% | 3.5% | 29.9% | 24.4% | 3.7% | 15.6% |
| Plain water intake (mL/day) | 546 | 414 | 658 | 490 | 629 | 394 | 739 |
| Soft drink intake (mL/day) | 56 | 61 | 35 | 42 | 13 | 155 | 14 |
| Prepacked FJ intake (mL/day) | 104 | 93 | 99 | 103 | 70 | 174 | 75 |
| Availability soft drinks/prepacked FJ [1,2,3,4,5,6,7,8,9,10] | 3.8 ± 1.8 | 3.9 ± 1.9 | 4.0 ± 1.9 | 3.9 ± 1.9 | 3.4 ± 1.4 | 4.2 ± 1.8 | 3.5 ± 1.5 |
| Availability plain water [1,2,3,4,5,6,7,8,9,10] | 8.9 ± 1.4 | 9.1 ± 1.3 | 8.4 ± 1.5 | 9.0 ± 1.3 | 9.1 ± 1.1 | 8.2 ± 1.6 | 9.5 ± 1.0 |
| Permissiveness [1,2,3,4,5,6,7,8,9,10] | 3.9 ± 1.7 | 4.1 ± 1.6 | 4.2 ± 1.9 | 3.7 ± 1.8 | 3.4 ± 1.2 | 4.1 ± 1.8 | 4.0 ± 1.6 |
| Avoiding negative modelling [1,2,3,4,5] | 3.5 ± 1.1 | 3.2 ± 1.1 | 3.3 ± 1.2 | 3.8 ± 1.1 | 4.0 ± 1.0 | 3.2 ± 1.1 | 3.3 ± 1.1 |
| Awareness [1,2,3,4,5,6,7,8,9,10] | 8.1 ± 1.9 | 8.1 ± 1.7 | 7.7 ± 2.2 | 8.1 ± 1.8 | 8.5 ± 1.7 | 8.0 ± 1.8 | 7.8 ± 1.9 |
| Encouragement [1,2,3,4,5] | 4.5 ± 0.7 | 4.5 ± 0.6 | 4.5 ± 0.8 | 4.4 ± 0.8 | 4.5 ± 0.7 | 4.5 ± 0.8 | 4.6 ± 0.7 |
| Rewarding [1,2,3,4,5] | 1.6 ± 0.8 | 1.6 ± 0.8 | 1.7 ± 0.9 | 1.5 ± 0.8 | 1.5 ± 0.8 | 1.8 ± 0.9 | 1.5 ± 0.8 |
| Lack of self-efficacy [1,2,3,4,5] | 2.3 ± 1.2 | 2.0 ± 1.0 | 2.1 ± 1.1 | 2.5 ± 1.2 | 1.9 ± 1.0 | 3.1 ± 1.2 | 1.8 ± 1.0 |
| Parenting Practices | a † (SE) | b ‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | |
|---|---|---|---|---|---|
| Plain water | |||||
| Availability soft drinks/prepacked FJ | −0.541 (0.050) | −20.888 (3.014) | 11.300 (1.936) | 7.505 to 15.096 | 42.5 |
| Availability plain water | 0.177 (0.038) | 43.443 (3.228) | 7.689 (1.747) | 4.265 to 11.113 | 29.0 |
| Permissiveness | −0.430 (0.047) | −9.496 (3.103) | 4.083 (1.407) | 1.326 to 6.841 | 15.4 |
| Avoiding negative modelling | 0.185 (0.032) | −7.407 (3.839) | −1.370 (0.749) | −2.838 to 0.097 | - |
| Awareness | 0.430 (0.053) | −2.111 (2.288) | −0.908 (0.990) | −2.848 to 1.033 | - |
| Encouragement | 0.080 (0.021) | 40.167 (5.758) | 3.213 (0.961) | 1.330 to 5.097 | 12.1 |
| Rewarding | −0.129 (0.024) | 13.527 (4.865) | −1.745 (0.707) | −3.130 to −0.360 | −6.6 |
| Lack of self-efficacy | −0.139 (0.031) | −32.995 (3.790) | 4.586 (1.151) | 2.331 to 6.841 | 17.3 |
| Total | - | - | 26.850 (2.817) | 21.329 to 32.370 | 101.1 |
| Soft drinks | |||||
| Availability soft drinks/prepacked FJ | −0.541 (0.050) | 8.297 (1.325) | −4.489 (0.828) | −6.112 to −2.865 | 18.1 |
| Availability plain water | 0.177 (0.038) | −9.164 (1.418) | −1.622 (0.429) | −2.463 to −0.781 | 6.5 |
| Permissiveness | −0.430 (0.047) | 8.643 (1.364) | −3.716 (0.713) | −5.115 to −2.318 | 15.0 |
| Avoiding negative modelling | 0.185 (0.032) | −2.562 (1.688) | −0.474 (0.323) | −1.107 to 0.159 | - |
| Awareness | 0.430 (0.053) | −0.461 (1.004) | −0.198 (0.432) | −1.046 to 0.649 | - |
| Encouragement | 0.080 (0.021) | −0.684 (2.532) | −0.055 (0.203) | −0.453 to 0.343 | - |
| Rewarding | −0.129 (0.024) | 1.822 (2.139) | −0.235 (0.279) | −0.783 to 0.313 | - |
| Lack of self-efficacy | −0.139 (0.031) | 7.199 (1.662) | −1.001 (0.321) | −1.630 to −0.371 | 4.0 |
| Total | - | - | −11.790 (0.955) | −13.662 to −9.918 | 47.6 |
| Prepacked FJ | |||||
| Availability soft drinks/prepacked FJ | −0.541 (0.050) | 16.755 (1.461) | −9.064 (1.152) | −11.322 to −6.807 | 124.0 |
| Availability plain water | 0.177 (0.038) | −4.623 (1.563) | −0.818 (0.328) | −1.461 to −0.176 | 11.2 |
| Permissiveness | −0.430 (0.047) | 8.222 (1.504) | −3.535 (0.753) | −5.012 to −2.059 | 48.4 |
| Avoiding negative modelling | 0.185 (0.032) | 1.709 (1.860) | 0.316 (0.348) | −0.367 to 0.999 | - |
| Awareness | 0.430 (0.053) | −7.705 (1.108) | −3.313 (0.628) | −4.543 to −2.083 | 45.3 |
| Encouragement | 0.080 (0.021) | −1.663 (2.791) | −0.133 (0.226) | −0.576 to 0.310 | - |
| Rewarding | −0.129 (0.024) | −11.066 (2.358) | 1.428 (0.404) | 0.636 to 2.219 | −19.5 |
| Lack of self-efficacy | −0.139 (0.031) | 6.776 (1.833) | −0.942 (0.330) | −1.589 to −0.295 | 12.9 |
| Total | - | - | −16.063 (1.278) | −18.567 to −13.558 | 219.7 |
| Belgium | Bulgaria | |||||||||
| (n = 917) | (n = 752) | |||||||||
| Parenting Practices | a † (SE) | b ‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | | a † (SE) | b ‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | |
| Plain water | ||||||||||
| Availability soft drinks/prepacked FJ | −1.110 (0.139) | −14.708 (6.012) | 16.326 (6.979) | 2.646 to 30.006 | 33.7 | −0.450 (0.147) | −2.952 (8.585) | 1.328 (3.888) | −6.291 to 8.948 | - |
| Availability plain water | 0.380 (0.096) | 17.284 (7.667) | 6.568 (3.353) | −0.004 to 13.139 | - | −0.073 (0.119) | 34.688 (7.914) | −2.532 (4.168) | −10.702 to 5.637 | - |
| Permissiveness | −0.742 (0.120) | −4.837 (6.727) | 3.589 (5.025) | −6.260 to 13.438 | - | −0.323 (0.145) | 0.255 (8.434) | −0.082 (2.724) | −5.422 to 5.258 | - |
| Avoiding negative modelling | 0.232 (0.087) | −19.683 (7.619) | −4.566 (2.461) | −9.390 to 0.257 | - | 0.040 (0.095) | 16.252 (10.676) | 0.650 (1.602) | −2.490 to 3.790 | - |
| Awareness | 0.792 (0.127) | 7.243 (5.619) | 5.736 (4.544) | −3.170 to 14.643 | - | −0.059 (0.175) | −5.934 (5.934) | 0.350 (1.096) | −1.798 to 2.498 | - |
| Encouragement | 0.193 (0.049) | 80.420 (15.585) | 15.521 (4.957) | 5.805 to 25.238 | 32.1 | 0.040 (0.064) | 17.492 (14.739) | 0.700 (1.265) | −1.780 to 3.180 | - |
| Rewarding | −0.184 (0.059) | −11.023 (10.872) | 2.028 (2.104) | −2.095 to 6.151 | - | −0.200 (0.069) | 3.330 (13.625) | −0.666 (2.735) | −6.026 to 4.694 | - |
| Lack of self-efficacy | −0.383 (0.077) | −23.291 (9.248) | 8.920 (3.970) | 1.139 to 16.702 | 18.4 | −0.185 (0.085) | −45.731 (10.715) | 8.460 (4.636) | −0.092 to 17.012 | - |
| Total | - | - | 54.123 (7.700) | 39.031 to 69.214 | 111.8 | - | - | 8.208 (7.135) | −5.776 to 22.192 | - |
| Availability soft drinks/prepacked FJ | −1.110 (0.139) | 9.252 (2.784) | −10.270 (3.347) | −16.830 to −3.709 | 20.7 | −0.450 (0.147) | 5.707 (2.352) | −2.568 (1.351) | −5.215 to 0.079 | - |
| Availability plain water | 0.380 (0.096) | −4.340 (3.554) | −1.649 (1.413) | −4.419 to 1.121 | - | −0.073 (0.119) | 0.330 (2.170) | −0.024 (0.163) | −0.344 to 0.296 | - |
| Permissiveness | −0.742 (0.120) | 9.253 (3.114) | −6.866 (2.564) | −11.890 to −1.841 | 13.8 | −0.323 (0.145) | 6.583 (2.317) | −2.126 (1.213) | −4.504 to 0.251 | - |
| Avoiding negative modelling | 0.232 (0.087) | −5.740 (3.538) | −1.332 (0.961) | −3.215 to 0.551 | - | 0.040 (0.095) | 2.024 (2.932) | 0.081 (0.225) | −0.360 to 0.522 | - |
| Awareness | 0.792 (0.127) | −10.105 (2.601) | −8.003 (2.427) | −12.760 to −3.246 | 16.1 | −0.059 (0.175) | −1.623 (1.480) | 0.096 (0.297) | −0.487 to 0.678 | - |
| Encouragement | 0.193 (0.049) | −13.970 (7.214) | −2.696 (1.551) | −5.737 to 0.345 | - | 0.040 (0.064) | 5.115 (4.063) | 0.205 (0.365) | −0.512 to 0.921 | - |
| Rewarding | −0.184 (0.059) | −1.199 (5.043) | 0.221 (0.931) | −1.603 to 2.045 | - | −0.200 (0.069) | 1.791 (3.748) | −0.358 (0.760) | −1.847 to 1.131 | - |
| Lack of self-efficacy | −0.383 (0.077) | 5.390 (4.276) | −2.064 (1.689) | −5.376 to 1.247 | - | −0.185 (0.085) | 10.252 (2.945) | −1.897 (1.028) | −3.911 to 0.118 | - |
| Total | - | - | −32.659 (3.435) | −39.392 to −25.927 | 65.7 | - | - | −6.592 (1.901) | −10.318 to −2.866 | 62.8 |
| Prepacked FJ | ||||||||||
| Availability soft drinks/prepacked FJ | −1.110 (0.139) | 7.004 (3.430) | −7.774 (3.930) | −15.477 to −0.072 | 97.5 | −0.450 (0.147) | 11.377 (3.503) | −5.120 (2.298) | −9.624 to −0.615 | −50.3 |
| Availability plain water | 0.380 (0.096) | −7.547 (4.379) | −2.868 (1.815) | −6.425 to 0.689 | - | −0.073 (0.119) | −1.511 (3.232) | 0.110 (0.297) | −0.471 to 0.692 | - |
| Permissiveness | −0.742 (0.120) | 5.662 (3.845) | −4.201 (2.933) | −9.946 to 1.547 | - | −0.323 (0.145) | 10.896 (3.450) | −3.519 (1.933) | −7.309 to 0.270 | - |
| Avoiding negative modelling | 0.232 (0.087) | −8.341 (4.349) | −1.935 (1.243) | −4.371 to 0.501 | - | 0.040 (0.095) | 5.255 (4.365) | 0.210 (0.529) | −0.826 to 1.247 | - |
| Awareness | 0.792 (0.127) | −9.358 (0.208) | −7.412 (1.200) | −9.763 to 5.060 | 93.0 | −0.059 (0.175) | −3.883 (2.204) | 0.229 (0.692) | −1.127 to 1.585 | - |
| Encouragement | 0.193 (0.049) | −0.455 (8.892) | −0.080 (1.716) | −3.452 to 3.276 | - | 0.040 (0.064) | −17.616 (6.043) | −0.705 (1.153) | −2.965 to 1.555 | - |
| Rewarding | −0.184 (0.059) | 0.526 (6.208) | −0.097 (1.143) | −2.336 to 2.143 | - | −0.200 (0.069) | −14.639 (5.577) | 2.928 (1.505) | −0.022 to 5.877 | - |
| Lack of self-efficacy | −0.383 (0.077) | −0.426 (5.280) | 0.163 (2.023) | −3.801 to 4.127 | −0.185 (0.085) | 15.931 (4.384) | −2.947 (1.578) | −6.041 to 0.147 | - | |
| Total | - | - | −24.212 (2.650) | −29.405 to −19.018 | 303.7 | - | - | −8.814 (3.518) | −15.709 to −1.918 | −86.6 |
| Germany | Greece | |||||||||
| (n = 1139) | (n = 1733) | |||||||||
| Parenting Practices | a † (SE) | b ‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | | a † (SE) | b‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | |
| Plain water | ||||||||||
| Availability soft drinks/prepacked FJ | −0.366 (0.122) | −38.176 (6.360) | 13.972 (5.207) | 3.767 to 24.178 | 23.2 | −0.492 (0.086) | −2.838 (8.146) | 1.396 (4.015) | −6.474 to 9.266 | - |
| Availability plain water | 0.166 (0.082) | 46.512 (7.989) | 7.721 (4.038) | −0.193 to 15.635 | - | 0.193 (0.070) | 24.297 (9.047) | 4.689 (2.438) | −0.088 to 9.467 | - |
| Permissiveness | −0.471 (0.111) | −7.866 (6.881) | 3.705 (3.357) | −2.874 to 10.284 | - | −0.208 (0.074) | −13.552 (9.003) | 2.819 (2.124) | −1.345 to 6.982 | - |
| Avoiding negative modelling | 0.136 (0.069) | 0.183 (9.315) | 0.025 (1.267) | −2.458 to 2.508 | - | 0.146 (0.060) | −13.490 (10.573) | −1.970 (1.743) | −5.386 to 1.447 | - |
| Awareness | 0.041 (0.114) | 3.688 (5.558) | 0.151 (0.478) | −0.786 to 1.089 | - | 0.560 (0.104) | −3.672 (5.955) | −2.056 (3.357) | −8.635 to 4.523 | - |
| Encouragement | 0.091 (0.049) | 16.528 (13.049) | 1.504 (1.437) | −1.313 to 4.321 | - | 0.022 (0.040) | 62.420 (16.189) | 1.373 (2.522) | −3.570 to 6.317 | - |
| Rewarding | −0.111 (0.052) | 25.691 (11.269) | −2.852 (1.830) | −6.439 to 0.735 | - | −0.114 (0.048) | 8.519 (13.636) | −0.971 (1.607) | −4.122 to 2.179 | - |
| Lack of self-efficacy | −0.086 (0.074) | −53.431 (8.511) | 4.595 (4.021) | −3.286 to 12.476 | - | −0.126 (0.061) | −14.569 (10.424) | 1.836 (1.586) | −1.273 to 4.944 | - |
| Total | - | - | 28.822 (7.913) | 13.313 to 44.330 | 47.8 | - | - | 7.116 (5.552) | −3.766 to 17.998 | - |
| Soft drinks | ||||||||||
| Availability soft drinks/prepacked FJ | −0.366 (0.122) | 6.070 (2.338) | −2.222 (1.132) | −4.440 to −0.004 | 8.7 | −0.492 (0.086) | 5.234 (1.202) | −2.575 (0.743) | −4.032 to −1.118 | 67.6 |
| Availability plain water | 0.166 (0.082) | −1.786 (2.930) | −0.296 (0.508) | −1.292 to 0.699 | - | 0.193 (0.070) | 0.662 (1.336) | 0.128 (0.262) | −0.386 to 0.641 | - |
| Permissiveness | −0.471 (0.111) | 11.060 (2.530) | −5.209 (1.711) | −8.563 to −1.856 | 20.5 | −0.208 (0.074) | 1.851 (1.328) | −0.385 (0.308) | −0.989 to 0.219 | - |
| Avoiding negative modelling | 0.136 (0.069) | −3.950 (3.407) | −0.537 (0.538) | −1.591 to 0.516 | - | 0.146 (0.060) | 1.809 (1.561) | 0.264 (0.252) | −0.231 to 0.759 | - |
| Awareness | 0.041 (0.114) | 3.697 (2.036) | 0.152 (0.430) | −0.691 to 0.994 | - | 0.560 (0.104) | −3.600 (0.878) | −2.016 (0.618) | −3.227 to −0.805 | 52.9 |
| Encouragement | 0.091 (0.049) | 1.683 (4.793) | 0.153 (0.444) | −0.717 to 1.023 | - | 0.022 (0.040) | 4.831 (2.389) | 0.106 (0.200) | −0.286 to 0.499 | - |
| Rewarding | −0.111 (0.052) | 10.193 (4.130) | −1.131 (0.701) | −2.505 to 0.242 | - | −0.114 (0.048) | 5.227 (2.011) | −0.596 (0.340) | −1.262 to 0.070 | - |
| Self-efficacy | −0.086 (0.074) | 0.443 (3.108) | −0.038 (0.269) | −0.566 to 0.490 | - | −0.126 (0.061) | −0.547 (1.538) | 0.069 (0.197) | −0.316 to 0.454 | - |
| Total | - | - | −9.129 (1.899) | −12.851 to −5.407 | 35.9 | - | - | −5.005 (0.942) | −6.851 to −3.159 | 131.4 |
| Prepacked FJ | ||||||||||
| Availability soft drinks/prepacked FJ | −0.366 (0.122) | 16.400 (3.370) | −6.002 (2.350) | −10.609 to −1.396 | 71.1 | −0.492 (0.086) | 18.474 (2.552) | −9.089 (2.025) | −13.058 to −5.120 | 217.4 |
| Availability plain water | 0.166 (0.082) | −7.248 (4.219) | −1.203 (0.919) | −3.004 to 0.597 | - | 0.193 (0.070) | 4.589 (2.883) | 0.886 (0.634) | −0.357 to 2.129 | - |
| Permissiveness | −0.471 (0.111) | 6.426 (3.643) | −3.027 (1.858) | −6.669 to 0.165 | - | −0.208 (0.074) | 6.686 (2.822) | −1.391 (0.768) | −2.895 to 0.114 | - |
| Avoiding negative modelling | 0.136 (0.069) | −3.391 (4.899) | −0.461 (0.706) | −1.845 to 0.923 | - | 0.146 (0.060) | 1.1015 (3.311) | 0.148 (0.487) | −0.807 to 1.103 | - |
| Awareness | 0.041 (0.114) | −8.335 (2.934) | −0.342 (0.958) | −2.219 to 1.536 | - | 0.560 (0.104) | −9.032 (1.868) | −5.058 (1.406) | −7.814 to −2.302 | 121.0 |
| Encouragement | 0.091 (0.049) | −2.379 (6.896) | −0.216 (0.638) | −1.468 to 1.035 | - | 0.022 (0.040) | 5.465 (5.073) | 0.120 (0.245) | −0.361 to 0.601 | - |
| Rewarding | 0.111 (0.052) | −15.956 (5.945) | −1.771 (1.060) | −3.849 to 0.307 | - | −0.114 (0.048) | −1.094 (4.274) | 0.125 (0.490) | −0.836 to 1.085 | - |
| Lack of self-efficacy | −0.086 (0.074) | 7.078 (4.472) | −0.609 (0.650) | −1.882 to 0.665 | - | −0.126 (0.061) | −0.628 (3.267) | 0.079 (0.413) | −0.731 to 0.889 | - |
| Total | - | - | −13.631 (3.089) | −19.686 to −7.577 | 161.4 | - | - | −14.180 (2.381) | −18.846 to −9.514 | 339.2 |
| Poland | Spain | |||||||||
| (n = 1384) | (n = 851) | |||||||||
| Parenting Practices | a † (SE) | b ‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | | a † (SE) | b ‡ (SE) | ab § (SE) | 95% CI of ab | % Mediated Effect | |
| Plain water | ||||||||||
| Availability soft drinks/prepacked FJ | −0.607 (0.122) | −19.416 (6.719) | 11.786 (4.716) | 2.541 to 21.030 | −52.2 | −0.316 (0.119) | −33.204 (9.262) | 10.492 (4.917) | 0.855 to 20.130 | −72.9 |
| Availability plain water | 0.308 (0.111) | 57.431 (5.688) | 17.689 (6.611) | 4.731 to 30.647 | −78.4 | 0.051 (0.078) | 41.809 (11.830) | 2.132 (3.316) | −4.368 to 8.632 | - |
| Permissiveness | −0.536 (0.123) | −21.935 (6.478) | 11.757 (4.397) | 3.139 to 20.376 | −52.1 | −0.325 (0.128) | 5.594 (8.515) | −1.818 (2.859) | −7.421 to 3.785 | - |
| Avoiding negative modelling | 0.418 (0.077) | −6.202 (7.743) | −2.592 (3.272) | −9.005 to 3.820 | - | 0.148 (0.088) | −12.604 (10.581) | −1.865 (1.919) | −5.627 to 1.896 | - |
| Awareness | 0.796 (0.125) | 1.435 (4.611) | 1.142 (3.675) | −6.060 to 8.345 | - | 0.473 (0.145) | −11.161 (6.626) | −5.279 (3.527) | −12.193 to 1.634 | - |
| Encouragement | 0.121 (0.058) | 33.635 (10.731) | 4.070 (2.343) | −0.523 to 8.663 | - | 0.028 (0.057) | 49.545 (16.011) | 1.387 (2.859) | −4.217 to 6.992 | - |
| Rewarding | −0.146 (0.063) | 7.428 (8.688) | −1.084 (1.352) | −3.734 to 1.565 | - | −0.033 (0.057) | 28.869 (16.076) | −0.953 (1.729) | −4.341 to 2.436 | - |
| Lack of self-efficacy | 0.031 (0.082) | −26.286 (7.033) | −0.815 (2.166) | −5.061 to 3.431 | - | −0.140 (0.082) | −30.859 (11.138) | 4.320 (2.972) | −1.505 to 10.146 | - |
| Total | - | - | 41.952 (90.098) | 24.120 to 59.784 | −186.0 | - | - | 8.417 (7.826) | −6.921 to 23.755 | - |
| Soft drinks | ||||||||||
| Availability soft drinks/prepacked FJ | −0.607 (0.122) | 11.553 (5.164) | −7.013 (3.437) | −13.749 to −0.276 | 12.4 | −0.316 (0.119) | 3.963 (1.158) | −1.252 (0.597) | −2.422 to −0.082 | 34.0 |
| Availability plain water | 0.308 (0.111) | −20.685 (4.367) | −6.371 (2.661) | −11.587 to −1.155 | 11.2 | 0.051 (0.078) | −1.601 (1.479) | −0.082 (0.146) | −0.368 to 0.204 | - |
| Permissiveness | −0.536 (0.123) | 13.441 (4.979) | −7.204 (3.139) | −13.357 to −1.051 | 12.7 | −0.325 (0.128) | 0.147 (1.064) | −0.048 (0.346) | −0.727 to 0.631 | - |
| Avoiding negative modelling | 0.418 (0.077) | −7.722 (5.958) | −3.228 (2.560) | −8.246 to 1.791 | - | 0.148 (0.088) | 0.109 (1.324) | 0.016 (0.196) | −0.368 to 0.401 | - |
| Awareness | 0.796 (0.125) | 2.022 (3.543) | 1.610 (2.832) | −56.661 to 15.324 | - | 0.473 (0.145) | −1.310 (0.829) | −0.620 (0.436) | −1.474 to 0.234 | - |
| Encouragement | 0.121 (0.058) | 1.180 (8.245) | 0.143 (1.000) | −1.817 to 2.103 | - | 0.028 (0.057) | −0.703 (2.002) | −0.020 (0.069) | −0.155 to 0.115 | - |
| Rewarding | −0.146 (0.063) | 0.868 (6.681) | −0.127 (0.977) | −2.042 to 1.788 | - | −0.033 (0.057) | 4.657 (2.010) | −0.154 (0.274) | −0.690 to 0.383 | - |
| Lack of self-efficacy | 0.031 (0.082) | 18.526 (5.388) | 0.574 (1.528) | −2.421 to 3.570 | - | −0.140 (0.082) | 1.740 (1.389) | −0.244 (0.241) | −0.716 to 0.229 | - |
| Total | - | - | −21.616 (4.973) | −31.363 to −11.869 | 38.1 | - | - | −2.402 (0.736) | −3.844 to −0.960 | 65.3 |
| Prepacked FJ | ||||||||||
| Availability soft drinks/prepacked FJ | −0.607 (0.122) | 25.879 (4.361) | −15.709 (4.120) | −23.784 to −7.633 | 85.1 | −0.316 (0.119) | 15.517 (3.355) | −4.903 (2.129) | −9.077 to −0.730 | 35.9 |
| Availability plain water | 0.308 (0.111) | −8.804 (3.691) | −2.712 (1.499) | −5.650 to 0.227 | - | 0.051 (0.078) | 7.612 (4.281) | 0.388 (0.633) | −0.852 to 1.628 | - |
| Permissiveness | −0.536 (0.123) | 9.648 (4.205) | −5.171 (2.547) | −10.164 to −0.179 | 28.0 | −0.325 (0.128) | 4.072 (3.085) | −1.323 (1.130) | −3.538 to 0.891 | - |
| Avoiding negative modelling | 0.418 (0.077) | 9.848 (5.028) | 4.116 (2.234) | −0.263 to 8.496 | - | 0.148 (0.088) | 2.492 (3.829) | 0.369 (0.608) | −0.822 to 1.560 | - |
| Awareness | 0.796 (0.125) | −9.656 (2.993) | −7.686 (2.671) | −12.921 to −2.452 | 41.7 | 0.473 (0.145) | −8.826 (2.398) | −4.175 (1.710) | −7.526 to −0.823 | 30.5 |
| Encouragement | 0.121 (0.058) | 2.761 (6.965) | 0.334 (0.858) | −1.347 to 2.015 | - | 0.028 (0.057) | 1.977 (5.791) | 0.055 (0.197) | −0.332 to 0.442 | - |
| Rewarding | −0.146 (0.063) | −18.721 (5.641) | 2.733 (1.439) | −0.086 to 5.553 | - | −0.033 (0.057) | 1.356 (5.808) | −0.045 (0.207) | −0.450 to 0.360 | - |
| Lack of self-efficacy | 0.031 (0.082) | 6.325 (4.559) | 0.196 (0.538) | −0.858 to 1.250 | - | −0.140 (0.082) | 8.454 (4.018) | −1.184 (0.893) | −2.933 to 0.566 | - |
| Total | - | - | −23.898 (4.961) | −33.621 to −14.175 | 129.5 | - | - | −10.817 (2.770) | −16.247 to −5.388 | 79.1 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinket, A.-S.; De Craemer, M.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G.; Androutsos, O.; Koletzko, B.; Moreno, L.A.; Socha, P.; Iotova, V.; et al. Can Parenting Practices Explain the Differences in Beverage Intake According to Socio-Economic Status: The Toybox-Study. Nutrients 2016, 8, 591. https://doi.org/10.3390/nu8100591
Pinket A-S, De Craemer M, De Bourdeaudhuij I, Deforche B, Cardon G, Androutsos O, Koletzko B, Moreno LA, Socha P, Iotova V, et al. Can Parenting Practices Explain the Differences in Beverage Intake According to Socio-Economic Status: The Toybox-Study. Nutrients. 2016; 8(10):591. https://doi.org/10.3390/nu8100591
Chicago/Turabian StylePinket, An-Sofie, Marieke De Craemer, Ilse De Bourdeaudhuij, Benedicte Deforche, Greet Cardon, Odysseas Androutsos, Berthold Koletzko, Luis A. Moreno, Piotr Socha, Violeta Iotova, and et al. 2016. "Can Parenting Practices Explain the Differences in Beverage Intake According to Socio-Economic Status: The Toybox-Study" Nutrients 8, no. 10: 591. https://doi.org/10.3390/nu8100591