

Breastfeeding Protects from Overjet in Adolescence by Reducing Pacifier Use: A Birth Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
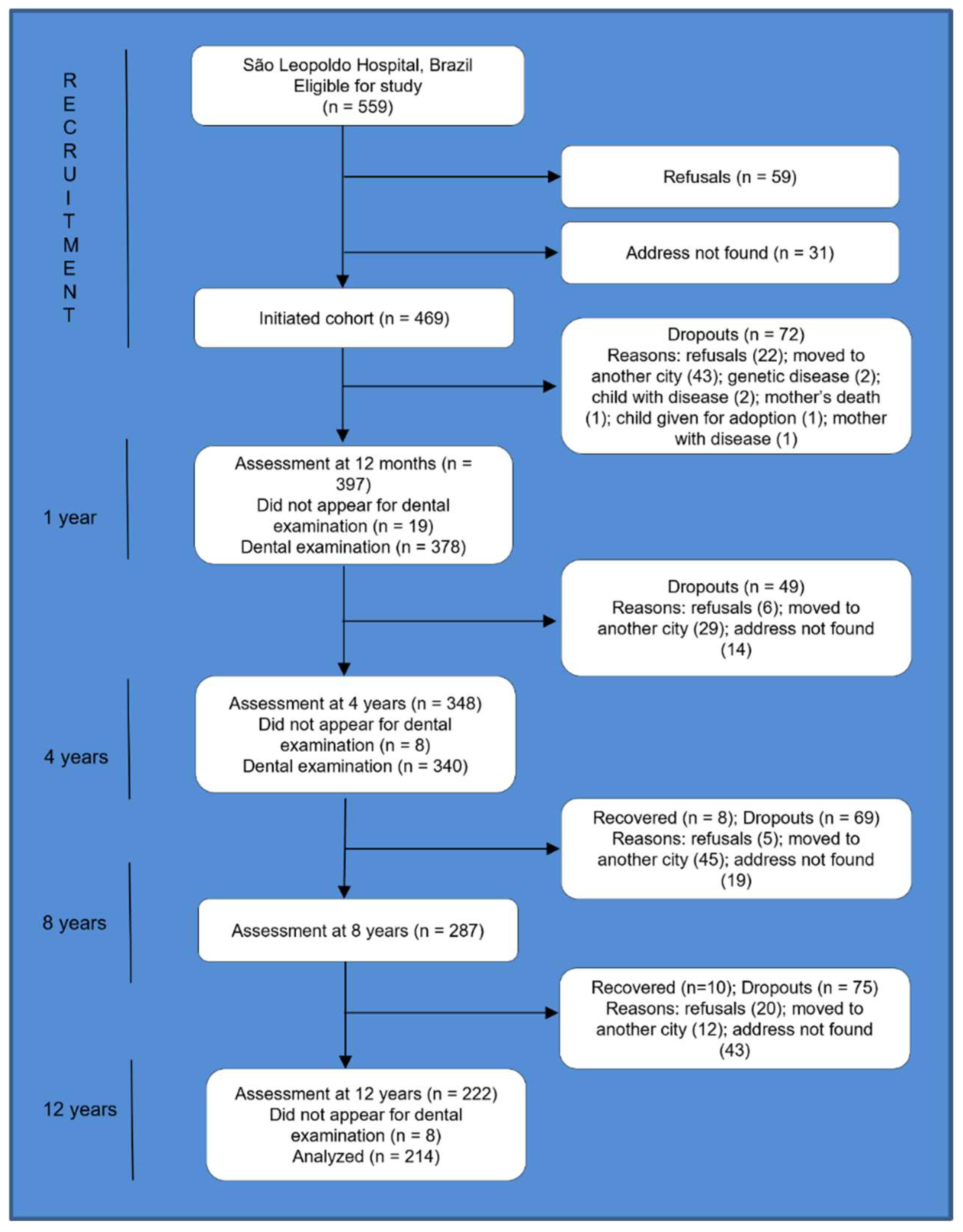
2.1. Setting, Study Design, and Participants
2.2. Data Collection
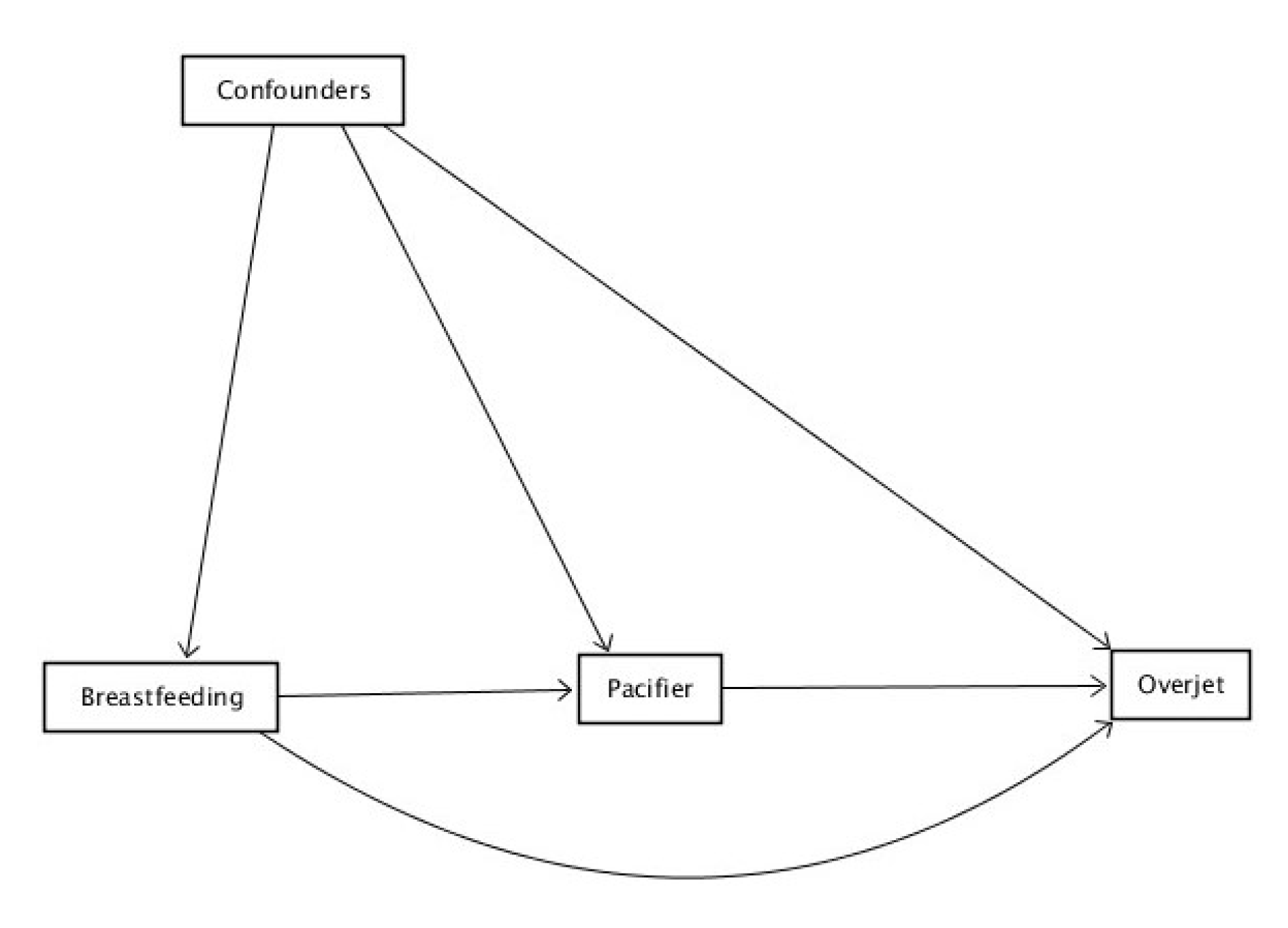
2.3. Data Analysis
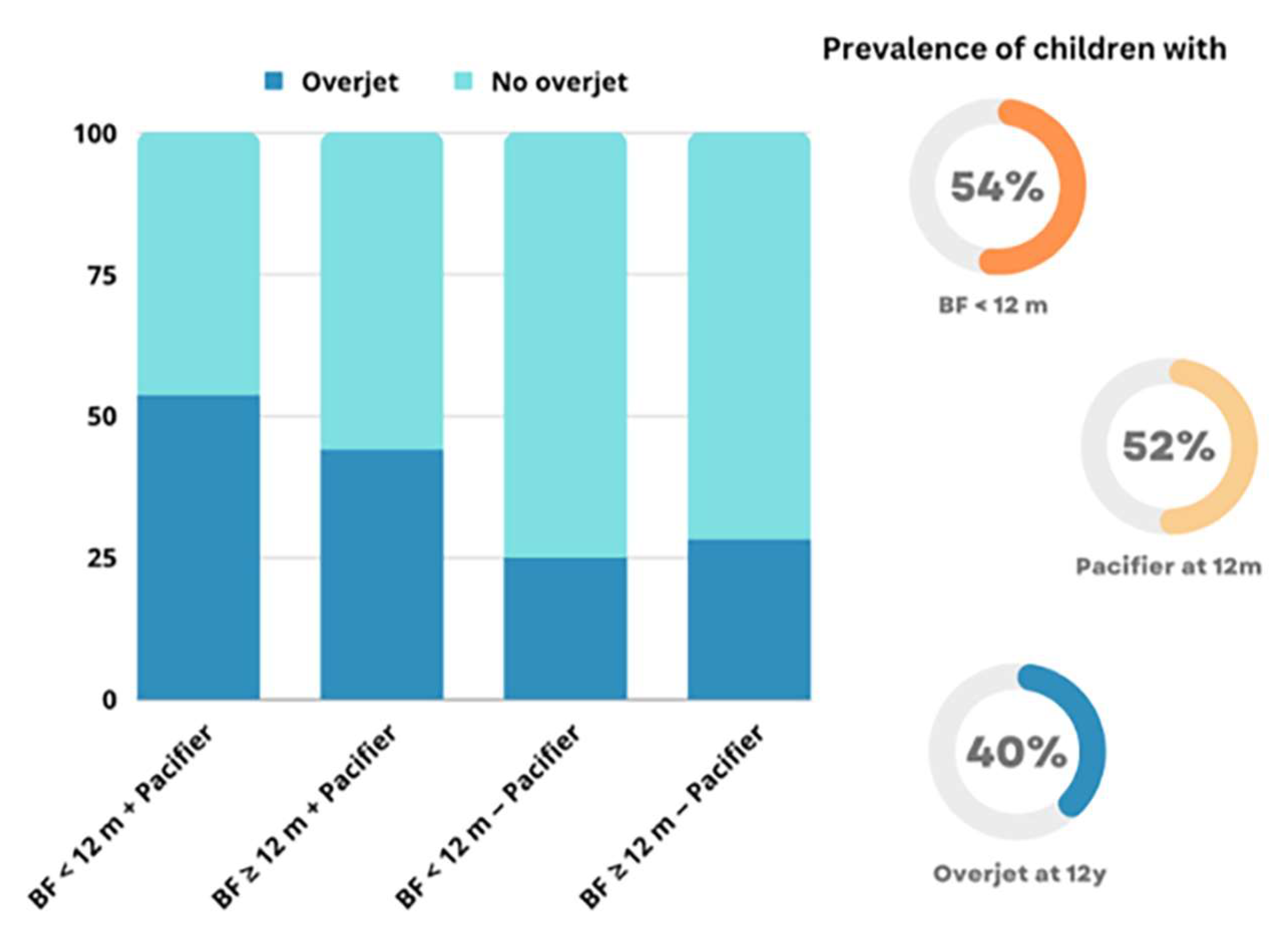
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization/FDI World Dental Federation. Oral Health Surveys: Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Proffit, W.R.; Fields, H.W.; Larson, B.E.; Sarver, D.M. Contemporary Orthodontics, 6th ed.; Elsevier: Philadelphia, PA, USA, 2019; pp. 2–16. [Google Scholar]
- Nguee, A.A.M.; Ongkosuwito, E.M.; Jaddoe, V.W.V.; Wolvius, E.B.; Kragt, L. Impact of orthodontic treatment need and deviant occlusal traits on oral health–related quality of life in children: A cross-sectional study in the Generation R cohort. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Piovesan, C.; Antunes, J.L.F.; Guedes, R.S.; Ardenghi, T.M.H. Impact of socioeconomic and clinical factors on child oral health-related quality of life (COHRQoL). Qual. Life Res. 2010, 19, 1359–1366. [Google Scholar] [CrossRef]
- Masood, M.; Suominen, A.L.; Pietila, T.; Lahti, S. Malocclusion traits and oral health-related quality of life in Finnish adults. Community Dent. Oral Epidemiol. 2017, 45, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Araki, M.; Yasuda, Y.; Ogawa, T.; Tumurkhuu, T.; Ganburged, G.; Bazar, A.; Fujiwara, T.; Moriyama, K. Associations between malocclusion and oral health-related quality of life among Mongolian adolescents. Int. J. Environ. Res. Public Health 2017, 14, 902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seehra, J.; Fleming, P.S.; Newton, T.; Di Biase, A.T. Bullying in orthodontic patients and its relationship to malocclusion, self-esteem and oral health-related quality of life. J. Orthod. 2011, 38, 247–256. [Google Scholar] [CrossRef]
- Ramos, I.T.M.; Nabarrette, M.; Vedovello-Filho, M.; de Menezes, C.C.; Meneghim, M.d.C.; Vedovello, S.A.S. Correlation between malocclusion and history of bullying in vulnerable adolescents. Angle Orthod. 2022, 92, 677–682. [Google Scholar] [CrossRef]
- Dalaie, K.; Behnaz, M.; Khodabakhshi, Z.; Hosseinpour, S. Impact of malocclusion severity on oral health-related quality of life in an Iranian young adult population. Eur. J. Dent. 2018, 12, 129–135. [Google Scholar] [CrossRef]
- Petti, S. Over two hundred million injuries to anterior teeth attributable to large overjet: A meta-analysis. Dent. Traumatol. 2015, 31, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Petrone, J.; Fishell, J.; Berk, N.W.; Kapur, R.; Sciote, J.; Weyant, R.J. Relationship of malocclusion severity and treatment fee to consumer’s expectation of treatment outcome. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 41–45. [Google Scholar] [CrossRef]
- Chambers, D.W.; Zitterkopf, J.G. How people make decisions about whether or not to seek orthodontic care: Upstream in the treatment chain. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 826–831. [Google Scholar] [CrossRef]
- Santana, L.G.; Flores-Mir, C.; Iglesias-Linares, A.; Pithon, M.M.; Marques, L.S. Influence of heritability on occlusal traits: A systematic review of studies in twins. Prog. Orthod. 2020, 21, 29. [Google Scholar] [CrossRef] [PubMed]
- Peres, K.G.; Cascaes, A.M.; Peres, M.A.; Demarco, F.F.; Santos, I.S.; Matijasevich, A.; Barros, A.J. Exclusive breastfeeding and risk of dental malocclusion. Pediatrics 2015, 136, e60–e67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, K.G.; Cascaes, A.M.; Nascimento, G.G.; Victora, C.G. Effect of breastfeeding on malocclusions: A systematic review and meta-analysis. Acta Paediatr. Int. J. Paediatr. 2015, 104, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Dimberg, L.; Lennartsson, B.; Söderfeldt, B.; Bondemark, L. Malocclusions in children at 3 and 7 years of age: A longitudinal study. Eur. J. Orthod. 2013, 35, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Victora, C.G.; Behague, D.P.; Barros, F.C.; Olinto, M.T.A.; Weiderpass, E. Pacifier use and short breastfeeding duration: Cause, consequence, or coincidence? Pediatrics 1997, 99, 445–453. [Google Scholar] [CrossRef]
- Feldens, C.A.; Vitolo, M.R.; Rauber, F.; Cruz, L.N.; Hilgert, J.B. Risk factors for discontinuing breastfeeding in Southern Brazil: A survival analysis. Matern. Child Health J. 2012, 16, 1257–1265. [Google Scholar] [CrossRef]
- Braga, V.S.; Vítolo, M.R.; Kramer, P.F.; Feldens, E.G.; Feldens, C.A. Breastfeeding in the First Hours of Life Protects against Pacifier Use: A Birth Cohort Study. Breastfeed Med. 2020, 15, 516–521. [Google Scholar] [CrossRef]
- Robins, J.M.; Hernán, M.Á.; Brumback, B. Marginal Structural Models and Causal Inference in Epidemiology. Epidemiology 2000, 11, 550–560. [Google Scholar] [CrossRef]
- Louzada, M.L.D.C.; Campagnolo, P.D.B.; Rauber, F.; Vitolo, M.R. Long-term effectiveness of maternal dietary counseling in a low-income population: A randomized field trial. Pediatrics 2012, 129, e1477–e1484. [Google Scholar] [CrossRef] [Green Version]
- Peres, K.; Thomson, W.; Chaffee, B.; Peres, M.; Birungi, N.; Do, L.; Feldens, C.; Fontana, M.; Marshall, T.; Pitiphat, W.; et al. Oral health birth cohort studies: Achievements, challenges, and potential. J. Dent. Res. 2020, 99, 1321–1331. [Google Scholar] [CrossRef]
- Shi, B.; Choirat, C.; Coull, B.A.; VanderWeele, T.J.; Valeri, L. CMAverse: A Suite of Functions for Reproducible Causal Mediation Analyses. Epidemiology 2021, 32, e20–e22. [Google Scholar] [CrossRef]
- Van Der Weele, T.J.; Ding, P. Sensitivity analysis in observational research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, P. The serial organization of sucking in the young infant. Pediatrics 1968, 42, 943–956. [Google Scholar] [CrossRef] [PubMed]
- Woolridge, M.W. The “anatomy” of infant sucking. Midwifery 1986, 2, 164–171. [Google Scholar] [CrossRef]
- Palmer, B. The Influence of breastfeeding on the development of the oral cavity: A commentary. J. Hum. Lact. 1998, 13, 93–98. [Google Scholar] [CrossRef]
- D’Onofrio, L. Oral dysfunction as a cause of malocclusion. Orthod. Craniofacial Res. 2019, 22 (Suppl. 1), 43–48. [Google Scholar] [CrossRef]
- Page, D.C. Breastfeeding is early functional jaw orthopedics (an introduction). Funct. Orthod. 2001, 18, 24–27. [Google Scholar]
- Mathew, O.; Bhatia, J. Sucking and breathing patterns during breast- and bottle-feeding. Ajdc 1989, 143, 588–592. [Google Scholar]
- Lopes, S.S.; Laignier, M.R.; Primo, C.C.; Leite, F.M.C. Baby-Friendly hospital initiative: Evaluation of the ten steps to successful breastfeeding. Rev. Paul. Pediatr. 2013, 31, 488–493. [Google Scholar] [CrossRef]
- Kair, L.R.; Kenron, D.; Etheredge, K.; Jaffe, A.C.; Phillipi, C.A. Pacifier restriction and exclusive breastfeeding. Pediatrics 2013, 131, e1101–e1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, L.G.; Paiva, S.M.; Pordeus, I.A.; Martins, C.C. Breastfeeding, bottle feeding and risk of malocclusion in mixed and permanent dentitions: A systematic review. Braz. Oral Res. 2016, 30, e22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, A.A.; Alves, C.M.; Ribeiro, C.C.; Pereira, A.L.; da Silva, A.A.; Silva, L.F.; Thomaz, E.B. Effects of conventional and orthodontic pacifiers on the dental occlusion of children aged 24–36 months old. Int. J. Paediatr. Dent. 2017, 27, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Belitz, G.S.; Furlan, L.J.N.; Knorst, J.K.; Berwig, L.C.; Ardenghi, T.M.; Ferrazzo, V.A.; Marquezan, M. Association between malocclusion in the mixed dentition with breastfeeding and past nonnutritive sucking habits in school-age children. Angle Orthod. 2022, 92, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E.; Khadivi, P.; Jakobsen, J.R. Changes in tooth size-arch length relationships from the deciduous to the permanent dentition: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 607–613. [Google Scholar] [CrossRef]
- Onyeaso, C.O.; Isiekwe, M.C. Occlusal changes from primary to mixed dentitions in Nigerian children. Angle Orthod. 2008, 78, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Peres, K.G.; Peres, M.A.; Thomson, W.M.; Broadbent, J.; Hallal, P.C.; Menezes, A.B. Deciduous-dentition malocclusion predicts orthodontic treatment needs later: Findings from a population-based birth cohort study. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 492–498. [Google Scholar] [CrossRef]
- Peres, K.G.; Chaffee, B.W.; Feldens, C.A.; Flores-Mir, C.; Moynihan, P.; Rugg-Gunn, A. Breastfeeding and Oral Health: Evidence and Methodological Challenges. J. Dent. Res. 2018, 97, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Feldens, C.A.; Braga, V.S.; Kramer, P.F.; Vítolo, M.R.; Rodrigues, P.H.; de Barros Coelho, E.M.R.; Chaffee, B.W. Primary Dentition caries patterns as predictors of permanent dentition caries: A prospective cohort study. Caries Res. 2023, 57, 167–176. [Google Scholar] [CrossRef]
- Feldens, C.A.; Ardenghi, T.M.; Cruz, L.N.; Scalco, G.; Vítolo, M.R. Advising mothers about breastfeeding and weaning reduced pacifier use in the first year of life: A randomized trial. Community Dent. Oral Epidemiol. 2013, 41, 317–326. [Google Scholar] [CrossRef]
- Scudine, K.G.O.; de Freitas, C.N.; Nascimento de Moraes, K.S.G.; Bommarito, S.; Possobon, R.F.; Boni, R.C.; Castelo, P.M. Multidisciplinary Evaluation of Pacifier Removal on Oro-Dentofacial Structures: A Controlled Clinical Trial. Front. Pediatr. 2021, 9, 703695. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | Overjet (Yes) | ||
|---|---|---|---|
| Frequency (Proportion) | Frequency (Proportion) | 95% CI | |
| Sex | |||
| Male | 127 (59.3%) | 52 (40.9%) | 34.4%, 47.5% |
| Female | 87 (40.7%) | 34 (39.1%) | 32.5%, 45.6% |
| Maternal Age | |||
| <20 years old | 36 (16.8%) | 12 (33.3%) | 27.0%, 39.6% |
| 20–30 years old | 124 (57.9%) | 54 (43.5%) | 36.9%, 50.2% |
| >30 years old | 54 (25.2%) | 20 (37.0%) | 30.6%, 43.5% |
| Maternal Schooling | |||
| ≤8 years | 111 (52.1%) | 45 (40.5%) | 33.9%, 47.1% |
| >8 years | 102 (47.9%) | 41 (40.2%) | 33.6%, 46.8% |
| Household monthly income (BMW) | |||
| <2 | 91 (43.8%) | 43 (47.3%) | 40.5%, 54.0% |
| 2–3 | 52 (25.0%) | 19 (36.5%) | 30.0%, 43.1% |
| >3 | 65 (31.2%) | 21 (32.3%) | 26.0%, 38.7% |
| Birth Weight (g) | |||
| ≤3350 | 108 (51.2%) | 40 (37.0%) | 30.5%, 43.6% |
| >3350 | 103 (48.8%) | 45 (43.7%) | 37.0%, 50.4% |
| Birth Length (cm) | |||
| ≤49 | 133 (63.0%) | 57 (42.9%) | 36.2%, 49.5% |
| >49 | 78 (37.0%) | 28 (35.9%) | 29.4%, 42.4% |
| Head Circumference (cm) | |||
| ≤35 | 123 (58.9%) | 51 (41.5%) | 34.8%, 48.1% |
| >35 | 86 (41.1%) | 32 (37.2%) | 30.7%, 43.8% |
| Breastfeeding ≥ 12 months | |||
| No | 113 (53.8%) | 53 (46.9%) | 40.2%, 53.7% |
| Yes | 97 (46.2%) | 31 (32.0%) | 25.7%, 38.3% |
| Pacifier at age 12 months | |||
| No | 99 (47.6%) | 27 (27.3%) | 18.8%, 37.1% |
| Yes | 109 (52.4%) | 56 (51.4%) | 41.6%, 61.1% |
| OR (95% CI) | p-Value | |
|---|---|---|
| Natural Direct Effect | 0.81 (0.41–1.60) | 0.533 |
| Natural Indirect Effect | 0.61 (0.44–0.87) | 0.005 |
| Total Effect | 0.49 (0.28–0.96) | 0.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feldens, C.A.; Petracco, L.B.; Nascimento, G.G.; Li, H.; Vítolo, M.R.; Peres, K.G. Breastfeeding Protects from Overjet in Adolescence by Reducing Pacifier Use: A Birth Cohort Study. Nutrients 2023, 15, 3403. https://doi.org/10.3390/nu15153403
Feldens CA, Petracco LB, Nascimento GG, Li H, Vítolo MR, Peres KG. Breastfeeding Protects from Overjet in Adolescence by Reducing Pacifier Use: A Birth Cohort Study. Nutrients. 2023; 15(15):3403. https://doi.org/10.3390/nu15153403
Chicago/Turabian StyleFeldens, Carlos Alberto, Laura Boianovsky Petracco, Gustavo G. Nascimento, Huihua Li, Márcia Regina Vítolo, and Karen Glazer Peres. 2023. "Breastfeeding Protects from Overjet in Adolescence by Reducing Pacifier Use: A Birth Cohort Study" Nutrients 15, no. 15: 3403. https://doi.org/10.3390/nu15153403