
Associations of Food Insecurity with Dietary Inflammatory Potential and Risk of Low Muscle Strength
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
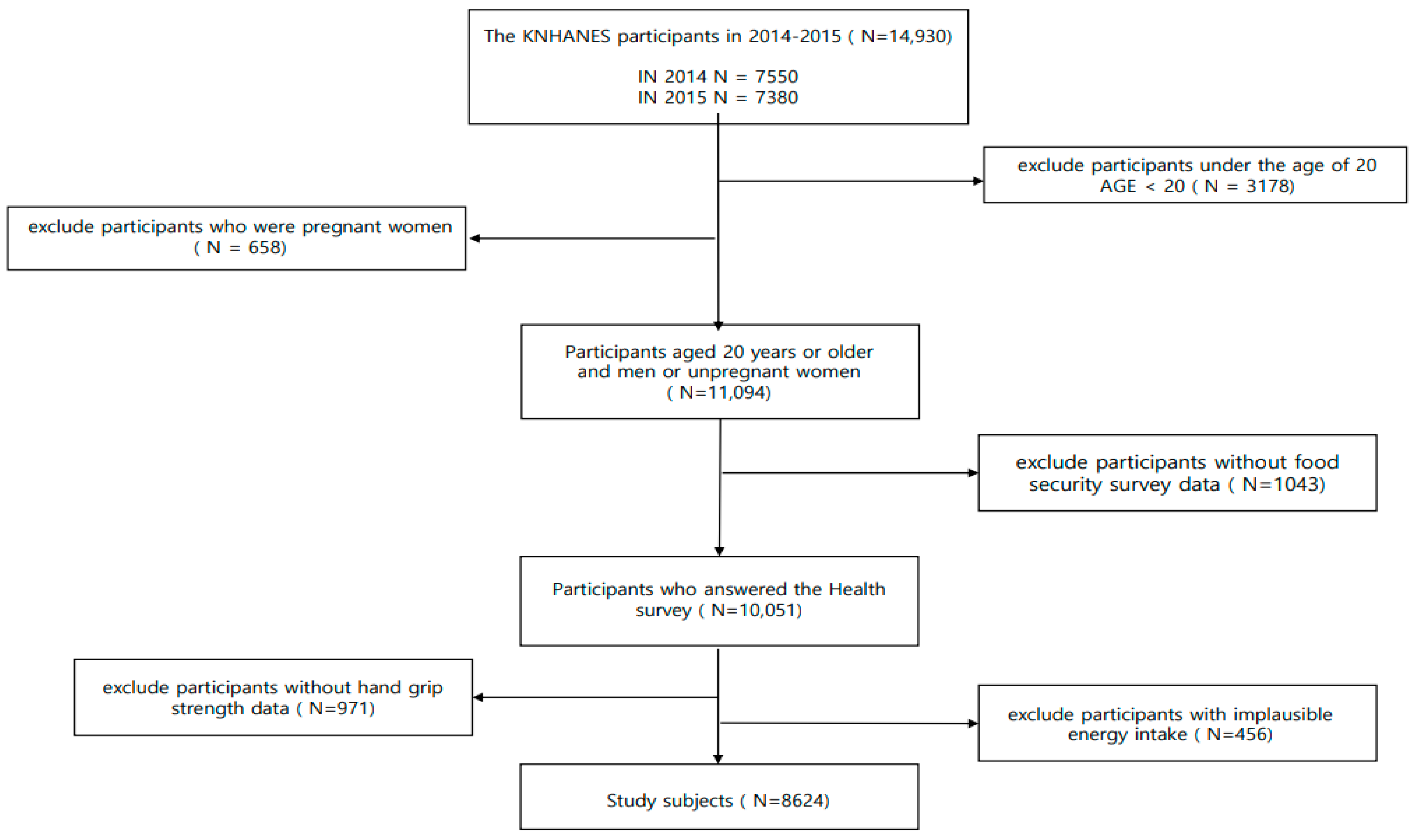
2.1. Study Population
2.2. Assessment of Food Insecurity
2.3. Measurement of Dietary Inflammatory Potential
2.4. Ascertainment of Low Muscle Strength
2.5. Assessment of Covariates
3. Statistical Analyses
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Wolfe, R.R. The underappreciated role of muscle in health and disease. Am. J. Clin. Nutr. 2006, 84, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celis-Morales, C.A.; Welsh, P.; Lyall, D.M.; Steell, L.; Petermann, F.; Anderson, J.; Iliodromiti, S.; Sillars, A.; Graham, N.; Mackay, D.F.; et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: Prospective cohort study of half a million UK Biobank participants. Bmj 2018, 361, k1651. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A.J.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Artero, E.G.; Lee, D.C.; Lavie, C.J.; España-Romero, V.; Sui, X.; Church, T.S.; Blair, S.N. Effects of muscular strength on cardiovascular risk factors and prognosis. J. Cardiopulm. Rehabil. Prev. 2012, 32, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Lee, Y.; Chung, Y.S.; Lee, D.J.; Joo, N.S.; Hong, D.; Song, G.; Kim, H.J.; Choi, Y.J.; Kim, K.M. Prevalence of sarcopenia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1107–1113. [Google Scholar] [CrossRef]
- Moon, S.W.; Kim, K.J.; Lee, H.S.; Yun, Y.M.; Kim, J.E.; Chun, Y.J.; Kim, C.O. Low muscle mass, low muscle function, and sarcopenia in the urban and rural elderly. Sci. Rep. 2022, 12, 14314. [Google Scholar] [CrossRef]
- Hanson, K.L.; Connor, L.M. Food insecurity and dietary quality in US adults and children: A systematic review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Food Insecurity And Health Outcomes. Health Affairs 2015, 34, 1830–1839. [CrossRef] [PubMed] [Green Version]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2022 Repurposing Food and Agricultural Policies to Make Healthy Diets More Affordable; FAO: Rome, Italy, 2022. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Dawson Hughes, B.; Scott, D.; Sanders, K.M.; Rizzoli, R. Nutritional strategies for maintaining muscle mass and strength from middle age to later life: A narrative review. Maturitas 2020, 132, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R.; Philp, A. Editorial: Nutritional Strategies to Promote Muscle Mass and Function Across the Health Span. Front. Nutr. 2020, 7, 569270. [Google Scholar] [CrossRef]
- Lynch, D.H.; Petersen, C.L.; Van Dongen, M.J.; Spangler, H.B.; Berkowitz, S.A.; Batsis, J.A. Association between food insecurity and probable sarcopenia: Data from the 2011–2014 National Health and nutrition examination survey. Clin. Nutr. 2022, 41, 1861–1873. [Google Scholar] [CrossRef] [PubMed]
- Dassie, G.A.; Motlagh, A.D.; Chamari, M.; Mohammadreza, E. Prevalence of Food Insecurity and its Association with Muscle Mass, Hand Grip Strength and Gait Speed among Elderly In Tehran. Int. J. Pharm. Sci. Res. 2016, 7, 2889–2895. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Wiedmer, P.; Jung, T.; Castro, J.P.; Pomatto, L.C.D.; Sun, P.Y.; Davies, K.J.A.; Grune, T. Sarcopenia—Molecular mechanisms and open questions. Ageing Res. Rev. 2021, 65, 101200. [Google Scholar] [CrossRef]
- Afzali, A.M.; Müntefering, T.; Wiendl, H.; Meuth, S.G.; Ruck, T. Skeletal muscle cells actively shape (auto)immune responses. Autoimmun. Rev. 2018, 17, 518–529. [Google Scholar] [CrossRef]
- Costamagna, D.; Costelli, P.; Sampaolesi, M.; Penna, F. Role of Inflammation in Muscle Homeostasis and Myogenesis. Mediators Inflamm. 2015, 2015, 805172. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Gao, X.; Shi, Y.; Wang, H.; Wang, W.; Li, Y.; Zheng, Z. Association between Handgrip Strength and the Systemic Immune-Inflammation Index: A Nationwide Study, NHANES 2011–2014. Int. J. Environ. Res. Public Health 2022, 19, 13616. [Google Scholar] [CrossRef] [PubMed]
- Bawaked, R.A.; Schröder, H.; Ribas-Barba, L.; Izquierdo-Pulido, M.; Pérez-Rodrigo, C.; Fíto, M.; Serra-Majem, L. Association of diet quality with dietary inflammatory potential in youth. Food Nutr. Res. 2017, 61, 1328961. [Google Scholar] [CrossRef] [Green Version]
- Bagheri, A.; Soltani, S.; Hashemi, R.; Heshmat, R.; Motlagh, A.D.; Esmaillzadeh, A. Inflammatory potential of the diet and risk of sarcopenia and its components. Nutr. J. 2020, 19, 129. [Google Scholar] [CrossRef]
- Shin, D.; Lee, K.W.; Brann, L.; Shivappa, N.; Hébert, J.R. Dietary inflammatory index is positively associated with serum high-sensitivity C-reactive protein in a Korean adult population. Nutrition 2019, 63–64, 155–161. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; Ramírez-Vélez, R.; Izquierdo, M.; García-Hermoso, A. Handgrip Strength and Its Relationship with White Blood Cell Count in U.S. Adolescents. Biology 2021, 10, 884. [Google Scholar] [CrossRef] [PubMed]
- Son, D.H.; Song, S.A.; Lee, Y.J. Association between C-Reactive Protein and Relative Handgrip Strength in Postmenopausal Korean Women Aged 45–80 Years: A Cross-Sectional Study. Clin. Interv. Aging 2022, 17, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Bergmans, R.S.; Palta, M.; Robert, S.A.; Berger, L.M.; Ehrenthal, D.B.; Malecki, K.M. Associations between Food Security Status and Dietary Inflammatory Potential within Lower-Income Adults from the United States National Health and Nutrition Examination Survey, Cycles 2007 to 2014. J. Acad. Nutr. Diet 2018, 118, 994–1005. [Google Scholar] [CrossRef]
- Daneshzad, E.; Ghorabi, S.; Hasani, H.; Omidian, M.; Jane Pritzl, T.; Yavari, P. Food Insecurity is positively related to Dietary Inflammatory Index in Iranian high school girls. Int. J. Vitam. Nutr. Res. 2020, 90, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.S. Food Insecurity and Related Risk Factors in the Elderly: Korea National Health and Nutrition Examination Survey 2013 Data. J. Korean Diet. Assoc. 2015, 21, 308–319. [Google Scholar] [CrossRef] [Green Version]
- Bickel, G.; Nord, M.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security, Revised 2000; U.S. Department of Agriculture, Food and Nutrition Service: Alexandria VA, USA, March 2000. [Google Scholar]
- Kim, K.; Hong, S.A.; Kwon, S.O.; Choi, B.Y.; Kim, G.-Y.; Oh, S.-Y. Validation of Food Security Measures for the Korean National Health and Nutrition Examination Survey. Korean J. Community Nutr. 2011, 16, 771–781. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.G.; Yook, S.M.; Hwang, J.Y. Is It What They Eat or How Much They Eat That Matters More in Adults with Food Insecurity in a Wealthy-Country Context? Nutrients 2021, 13, 851. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [Green Version]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.; Kim, J.; Kim, S.; Park, S.; Lim, H.; Koh, H. Trends in measures of handgrip strength from 2014 to 2017 among Korean adolescents using the Korean National Health and Nutrition Examination Survey Data. BMC Res. Notes 2020, 13, 307. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.R.; Jeon, Y.J.; Kim, M.C.; Jeong, T.; Koo, W.R. Reference values for hand grip strength in the South Korean population. PLoS ONE 2018, 13, e0195485. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- de Almeida Marques, R.; de Souza, V.F.; do Rosario, T.C.; da Silva Garcia, M.R.P.; Pereira, T.S.S.; Marques-Rocha, J.L.; Guandalini, V.R. Agreement between maximum and mean handgrip strength measurements in cancer patients. PLoS ONE 2022, 17, e0270631. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.Y.; Yang, Y.J.; Kim, B.S.; Kang, J.H. Validity and Reliability of Korean Version of International Physical Activity Questionnaire (IPAQ) Short Form. J. Korean Acad. Fam. Med. 2007, 28, 532–541. [Google Scholar]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Colbert, L.H.; Pahor, M.; Rubin, S.M.; Tylavsky, F.A.; et al. Higher inflammatory marker levels in older persons: Associations with 5-year change in muscle mass and muscle strength. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 1183–1189. [Google Scholar] [CrossRef] [Green Version]
- Korean National Academy of Agricultural Science. Food Composition Table, 7th ed.; Rural Development Administration, Republic of Korea: Suwon, Republic of Korea, 2006. [Google Scholar]
- Lee, Y.L.; Lee, B.H.; Lee, S.Y. Handgrip Strength in the Korean Population: Normative Data and Cutoff Values. Ann. Geriatr. Med. Res. 2019, 23, 183–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, C.W.; Wolfson, J.A. Food Insecurity among Older Adults: 10-Year National Trends and Associations with Diet Quality. J. Am. Geriatr. Soc. 2021, 69, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Llanaj, E.; Vincze, F.; Kósa, Z.; Sándor, J.; Diószegi, J.; Ádány, R. Dietary Profile and Nutritional Status of the Roma Population Living in Segregated Colonies in Northeast Hungary. Nutrients 2020, 12, 2836. [Google Scholar] [CrossRef] [PubMed]
- Llanaj, E.; Vincze, F.; Kósa, Z.; Bárdos, H.; Diószegi, J.; Sándor, J.; Ádány, R. Deteriorated Dietary Patterns with Regards to Health and Environmental Sustainability among Hungarian Roma Are Not Differentiated from Those of the General Population. Nutrients 2021, 13, 721. [Google Scholar] [CrossRef]
- Lee, S.E.; Song, Y.J.; Kim, Y.; Choe, J.; Paik, H.Y. Household food insufficiency is associated with dietary intake in Korean adults. Public Health Nutr. 2016, 19, 1112–1121. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, S.I.; Dodd, K.W.; Parsons, R.; Ng, C.; Garriguet, D.; Tarasuk, V. Household Food Insecurity Is a Stronger Marker of Adequacy of Nutrient Intakes among Canadian Compared to American Youth and Adults. J. Nutr. 2015, 145, 1596–1603. [Google Scholar] [CrossRef] [Green Version]
- Kubo, S.; da Costa, T.H.M.; Gubert, M.B. Intakes of energy, macronutrients and micronutrients of a population in severe food insecurity risk in Brazil. Public Health Nutr. 2020, 23, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Hart, M.J.; Torres, S.J.; McNaughton, S.A.; Milte, C.M. Dietary patterns and associations with biomarkers of inflammation in adults: A systematic review of observational studies. Nutr. J. 2021, 20, 24. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Wang, X.; Hu, Z.; Hu, J.; Du, J.; Mitch, W.E. Insulin resistance accelerates muscle protein degradation: Activation of the ubiquitin-proteasome pathway by defects in muscle cell signaling. Endocrinology 2006, 147, 4160–4168. [Google Scholar] [CrossRef] [Green Version]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.N. Interleukin-6 induces skeletal muscle protein breakdown in rats. Proc. Soc. Exp. Biol. Med. 1994, 205, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Tayek, J.A. Effects of tumor necrosis factor alpha on skeletal muscle amino acid metabolism studied in-vivo. J. Am. Coll. Nutr. 1996, 15, 164–168. [Google Scholar] [CrossRef]
- Amakye, W.K.; Zhang, Z.; Wei, Y.; Shivappa, N.; Hebert, J.R.; Wang, J.; Su, Y.; Mao, L. The relationship between dietary inflammatory index (DII) and muscle mass and strength in Chinese children aged 6–9 years. Asia. Pac. J. Clin. Nutr. 2018, 27, 1315–1324. [Google Scholar] [CrossRef]
- Smith, L.; Jacob, L.; Barnett, Y.; Butler, L.T.; Shin, J.I.; López-Sánchez, G.F.; Soysal, P.; Veronese, N.; Haro, J.M.; Koyanagi, A. Association between Food Insecurity and Sarcopenia among Adults Aged ≥65 Years in Low- and Middle-Income Countries. Nutrients 2021, 13, 1879. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Zhao, L.; Guo, Q.; Yu, D.; Yang, Y.; Cao, Q.; Yuan, X.; Ju, L.; Li, S.; Cheng, X.; et al. Comparison of the 24 h Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult. Nutrients 2022, 14, 1960. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Food Insecurity Level | ||||
|---|---|---|---|---|
| Characteristics | All | Food Secure (N = 7995) | Mildly Food Insecure (N = 529) | Moderate-to-Severe Food Insecure (N = 100) |
| Sociodemographic factors | ||||
| Age, years | 46.6 ± (0.3) | 46.5 ± (0.3) | 48.4 ± (1.0) | 49.1 ± (2.1) |
| Sex | ||||
| Male | 3675 (50.8) | 3424 (51.0) | 210 (47.8) | 41 (52.0) |
| Female | 4949 (49.2) | 4571 (49.0) | 319 (52.2) | 59 (48.0) |
| Marital status | ||||
| Married | 7434 (78.5) | 6900 (78.6) | 448 (77.9) | 86 (79.3) |
| Never married | 1190 (21.5) | 1095 (21.4) | 81 (22.1) | 14 (20.7) |
| Residence | ||||
| Urban | 2479 (30.3) | 2294 (30.4) | 157 (29.6) | 28 (31.0) |
| Rural | 6145 (69.7) | 5701 (69.6) | 372 (70.4) | 72 (69.0) |
| Education level | ||||
| Less than elementary school | 1861 (14.1) | 1638 (13.2) | 185 (24.5) | 38 (26.3) |
| Middle school graduate | 879 (8.3) | 802 (8.0) | 61 (11.6) | 16 (16.0) |
| High school graduate | 2523 (33.2) | 2350 (33.1) | 153 (35.9) | 20 (25.6) |
| College graduate or higher | 2596 (35.4) | 2501 (36.7) | 86 (19.6) | 9 (14.3) |
| Missing | 765 (9.1) | 704 (9.0) | 44 (8.5) | 17 (18.0) |
| Income | ||||
| Quartile 1 | 2073 (24.4) | 1752 (22.2) | 255 (49.5) | 66 (71.0) |
| Quartile 2 | 2142 (24.6) | 1960 (24.3) | 157 (30.2) | 25 (20.7) |
| Quartile 3 | 2164 (24.6) | 2081 (25.6) | 77 (13.2) | 6 (5.8) |
| Quartile 4 | 2206 (25.9) | 2169 (27.4) | 35 (6.3) | 2 (1.1) |
| Missing | 39 (0.5) | 33 (0.5) | 5 (0.8) | 1 (1.3) |
| Behavioral factors | ||||
| BMI (kg/m2) | ||||
| Underweight | 331 (4.1) | 299 (4.0) | 26 (4.6) | 6 (6.6) |
| Normal | 3282 (38.5) | 3057 (38.6) | 193 (37.8) | 32 (30.8) |
| Overweight | 2037 (23.0) | 1889 (23.1) | 120 (21.0) | 28 (29.9) |
| Obese | 2962 (34.3) | 2738 (34.2) | 190 (36.7) | 34 (32.7) |
| Missing | 12 (0.1) | 12 (0.1) | 0 | 0 |
| Smoking status | ||||
| Never | 5051 (54.0) | 4716 (54.4) | 286 (49.5) | 49 (50.5) |
| Past | 1739 (20.2) | 1620 (20.4) | 100 (19.4) | 19 (14.2) |
| Current | 1416 (21.1) | 1283 (20.7) | 110 (26.3) | 23 (27.4) |
| Missing | 418 (4.6) | 376 (4.5) | 33 (4.9) | 9 (8.0) |
| Alcohol drinking status | ||||
| Never | 1034 (8.8) | 949 (8.6) | 74 (11.5) | 11 (7.0) |
| Past | 1374 (13.7) | 1239 (13.4) | 111 (17.3) | 24 (22.7) |
| Current | 5806 (73.0) | 5437 (73.5) | 313 (66.5) | 56 (62.3) |
| Missing | 410 (4.5) | 370 (4.5) | 31 (4.7) | 9 (8.0) |
| Physical activity 2 | ||||
| High | 28 (0.4) | 26 (0.5) | 1 (0.08) | 1 (1.1) |
| Medium | 2965 (35.8) | 2772 (36.2) | 164 (31.1) | 29 (28.3) |
| Low | 5631 (63.8) | 5197 (63.4) | 364(68.9) | 70 (70.6) |
| Clinical health conditions | ||||
| The number of chronic disease 3 | ||||
| 0 | 5835 (75.3) | 5445 (75.7) | 329 (69.8) | 61 (71.4) |
| 1 | 1568 (14.2) | 1431 (14.0) | 115 (18.1) | 22 (13.4) |
| ≥2 | 1036 (8.3) | 946 (8.1) | 13 (11.2) | 13 (11.2) |
| Missing | 185 (2.1) | 173 (2.1) | 4 (4.0) | 4 (4.0) |
| Food Insecurity Level | P-Trend 2 | |||
|---|---|---|---|---|
| Food Secure (Referent) | Mildly Food Insecure | Moderate-to-Severe Food Insecure | ||
| Age-adjusted DII mean difference (95% CI) | 0.00 (ref) | 0.36 (0.21–0.51) | 0.69 (0.28–1.10) | 0.01 |
| MV-adjusted DII mean difference (95% CI) | 0.00 (ref) | 0.15 (0.01–0.30) | 0.43 (0.06–0.80) | <0.001 |
| Food Insecurity Level | P-Trend 2 | |||
|---|---|---|---|---|
| Food Secure (Referent) | Mildly Food Insecure | Moderate-to-Severe Food Insecure | ||
| No. cases/No. non-cases | 622/7373 | 67/462 | 19/81 | |
| Age-adjusted OR (95% CI) | 1.00 (ref) | 1.38 (0.98–1.95) | 2.76 (1.55–4.92) | <0.001 |
| MV-adjusted OR (95% CI) | 1.00 (ref) | 1.18 (0.83–1.70) | 2.06 (1.07–3.96) | 0.005 |
| No. Cases /No. Non-Cases | Food Insecurity Levels | P-Trend 2 | P-Interaction 3 | |||
|---|---|---|---|---|---|---|
| Food Secure (Reference) | Mildly Food Insecure OR (95% CI) | Moderate-to-Severe Food Insecure OR (95% CI) | ||||
| Sex | ||||||
| Male | 251/3424 | 1.00 (ref) | 1.19 (0.77–1.84) | 1.64 (0.71–3.8) | 0.03 | 0.50 |
| Female | 457/4492 | 1.00 (ref) | 1.12 (0.73–1.72) | 1.47 (0.68–3.14) | 0.08 | |
| Age | ||||||
| ≥60 years | 129/5519 | 1.00 (ref) | 1.31 (0.74–2.33) | 1.36 (0.39–4.77) | 0.21 | 0.84 |
| <60 years | 579/2397 | 1.00 (ref) | 1.11 (0.75–1.63) | 2.22 (1.05–4.66) | 0.08 | |
| Physical activity 4 | ||||||
| ≥ Medium | 156/2837 | 1.00 (ref) | 1.88 (0.98–3.62) | 2.34 (0.84–6.52) | 0.98 | 0.87 |
| Low | 552/5079 | 1.00 (ref) | 1.03 (0.71–1.50) | 0.91 (1.03–3.54) | 0.04 | |
| BMI | ||||||
| ≥25 (kg/m2) | 491/2640 | 1.00 (ref) | 1.20 (0.64–2.26) | 2.62 (0.98–7.01) | 0.10 | 0.64 |
| <25 (kg/m2) | 217/5276 | 1.00 (ref) | 0.97 (0.49–1.90) | 3.36 (1.10–10.27) | 0.03 | |
| Smoking status | ||||||
| No current | 564/6245 | 1.00 (ref) | 1.08 (0.74–1.58) | 1.48 (0.81–2.67) | 0.06 | 0.43 |
| Current | 51/1346 | 1.00 (ref) | 1.50 (0.5–4.43) | 4.71 (1.23–18.1) | 0.005 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.M.; Park, Y.J.; Kim, H.; Kwon, O.; Ko, K.S.; Kim, Y.; Kim, Y.; Park, H.; Jung, S. Associations of Food Insecurity with Dietary Inflammatory Potential and Risk of Low Muscle Strength. Nutrients 2023, 15, 1120. https://doi.org/10.3390/nu15051120
Kim SM, Park YJ, Kim H, Kwon O, Ko KS, Kim Y, Kim Y, Park H, Jung S. Associations of Food Insecurity with Dietary Inflammatory Potential and Risk of Low Muscle Strength. Nutrients. 2023; 15(5):1120. https://doi.org/10.3390/nu15051120
Chicago/Turabian StyleKim, Su Min, Yoon Jung Park, Hyesook Kim, Oran Kwon, Kwang Suk Ko, Yuri Kim, Yangha Kim, Hyesook Park, and Seungyoun Jung. 2023. "Associations of Food Insecurity with Dietary Inflammatory Potential and Risk of Low Muscle Strength" Nutrients 15, no. 5: 1120. https://doi.org/10.3390/nu15051120