
Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey
 , , , , , , , , , ,
, , , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Method
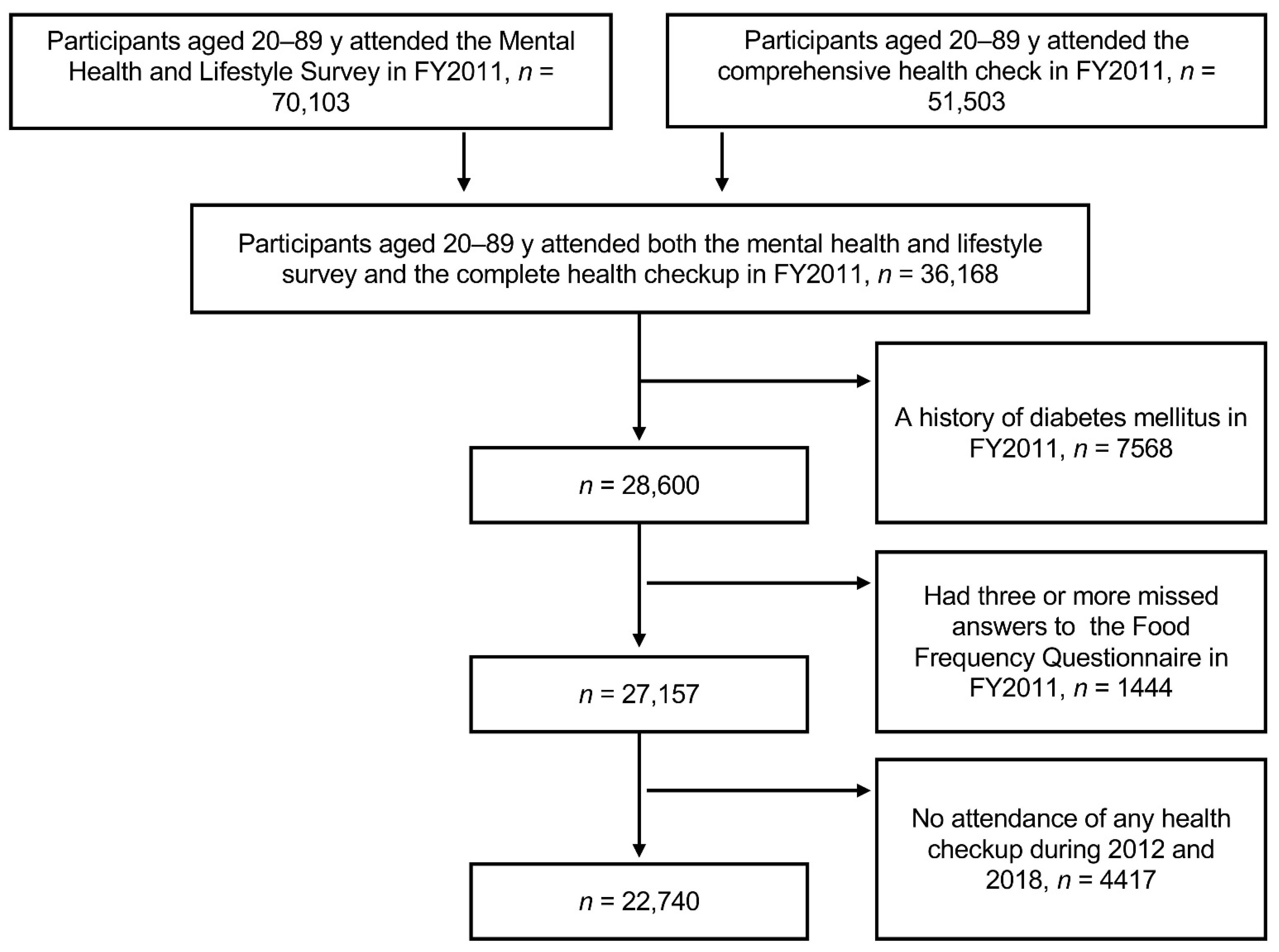
2.1. Study Design and Study Participants
2.2. Dietary Intake Assessment
2.3. Diabetes- and Disaster-Related Variables
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observational studies. BMJ 2019, 366, l2368. [Google Scholar] [CrossRef] [Green Version]
- Churuangsuk, C.; Hall, J.; Reynolds, A.; Griffin, S.J.; Combet, E.; Lean, M.E.J. Diets for weight management in adults with type 2 diabetes: An umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission. Diabetologia 2022, 65, 14–36. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.M.; Knüppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boushey, C.; Ard, J.; Bazzano, L.; Heymsfield, S.; Mayer-Davis, E.; Sabaté, J.; Snetselaar, L.; Van Horn, L.; Schneeman, B.; English, L.K.; et al. USDA nutrition evidence systematic reviews. In Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review; USDA Nutrition Evidence Systematic Review: Alexandria, VA, USA, 2020. [Google Scholar]
- Sasaki, S. What is the scientific definition of the Japanese diet from the viewpoint of nutrition and health? Nutr. Rev. 2020, 78, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Mizoue, T.; Yamaji, T.; Tabata, S.; Yamaguchi, K.; Ogawa, S.; Mineshita, M.; Kono, S. Dietary patterns and glucose tolerance abnormalities in Japanese men. J. Nutr. 2006, 136, 1352–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, E.; Takahashi, K.; Nakamura, K.; Ukawa, S.; Takabayashi, S.; Nakamura, M.; Sasaki, S.; Tamakoshi, A.; Takimoto, H. Dietary patterns and abnormal glucose tolerance among Japanese: Findings from the National Health and Nutrition Survey, 2012. Public Health Nutr. 2019, 22, 2460–2468. [Google Scholar] [CrossRef]
- Yasumura, S.; Abe, M. Fukushima Health Management Survey and Related Issues. Asia Pac. J. Public Health 2017, 29, 29S–35S. [Google Scholar] [CrossRef] [Green Version]
- Nagai, M.; Ohira, T.; Takahashi, H.; Nakano, H.; Sakai, A.; Hashimoto, S.; Yasumura, S.; Abe, M. Impact of evacuation on trends in the prevalence, treatment, and control of hypertension before and after a disaster. J. Hypertens. 2018, 36, 924–932. [Google Scholar] [CrossRef]
- Ohira, T.; Nakano, H.; Nagai, M.; Yumiya, Y.; Zhang, W.; Uemura, M.; Sakai, A.; Hashimoto, S.; Fukushima Health Management Survey Group. Changes in Cardiovascular Risk Factors After the Great East Japan Earthquake. Asia Pac. J. Public Health 2017, 29, 47S–55S. [Google Scholar] [CrossRef]
- Takahashi, S.; Nakamura, M.; Yonekura, Y.; Tanno, K.; Sakata, K.; Ogawa, A.; Kobayashi, S. Association between relocation and changes in cardiometabolic risk factors: A longitudinal study in tsunami survivors of the 2011 Great East Japan Earthquake. BMJ Open 2016, 6, e011291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirai, H.; Nagao, M.; Ohira, T.; Maeda, M.; Okazaki, K.; Nakano, H.; Hayashi, F.; Harigane, M.; Suzuki, Y.; Takahashi, A.; et al. Psychological burden predicts new-onset diabetes in men: A longitudinal observational study in the Fukushima Health Management Survey after the Great East Japan Earthquake. Front. Endocrinol. 2022, 13, 2840. [Google Scholar]
- Gohardehi, F.; Seyedin, H.; Moslehi, S. Prevalence rate of diabetes and hypertension in disaster-exposed populations: A systematic review and meta-analysis. Ethiop. J. Health Sci. 2020, 30, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Ohira, T.; Sakai, A.; Yasumura, S.; Takahashi, A.; Kazama, J.; Shimabukuro, M.; Nakano, H.; Okazaki, K.; Maeda, M.; et al. Associations between dietary patterns and cardiometabolic risks in Japan: A cross-sectional study from the Fukushima Health Management Survey, 2011–2015. Nutrients 2020, 12, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Ohira, T.; Abe, M.; Kamiya, K.; Yamashita, S.; Yasumura, S.; Ohtsuru, A.; Maeda, M.; Harigane, M.; Horikoshi, N.; et al. Evacuation after the Great East Japan Earthquake was associated with poor dietary intake: The Fukushima Health Management Survey. J. Epidemiol. 2017, 27, 14–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauvaget, C.; Allen, N.; Hayashi, M.; Spencer, E.; Nagano, J. Validation of a food frequency questionnaire in the Hiroshima/Nagasaki Life Span Study. J. Epidemiol. 2002, 12, 394–401. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Uemura, M.; Ohira, T.; Yasumura, S.; Otsuru, A.; Maeda, M.; Harigane, M.; Horikoshi, N.; Suzuki, Y.; Yabe, H.; Takahashi, H.; et al. Association between psychological distress and dietary intake among evacuees after the Great East Japan Earthquake in a cross-sectional study: The Fukushima Health Management Survey. BMJ Open 2016, 6, e011534. [Google Scholar] [CrossRef]
- Luger, E.; Aspalter, R.; Luger, M.; Longin, R.; Rieder, A.; Dorner, T.E. Changes of dietary patterns during participation in a web-based weight-reduction programme. Public Health Nutr. 2016, 19, 1211–1221. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Fung, T.T.; Hu, F.B.; Curhan, G.C. Association of dietary patterns with albuminuria and kidney function decline in older white women: A subgroup analysis from the Nurses’ Health Study. Am. J. Kidney Dis. 2011, 57, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Htun, N.C.; Suga, H.; Imai, S.; Shimizu, W.; Takimoto, H. Food intake patterns and cardiovascular risk factors in Japanese adults: Analyses from the 2012 National Health and nutrition survey, Japan. Nutr. J. 2017, 16, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003(-)2015: Continuous Westernization of the Japanese Diet. Nutrients 2018, 10, 994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Montero, C.; Fraile-Martinez, O.; Gomez-Lahoz, A.M.; Pekarek, L.; Castellanos, A.J.; Noguerales-Fraguas, F.; Coca, S.; Guijarro, L.G.; Garcia-Honduvilla, N.; Asunsolo, A.; et al. Nutritional Components in Western Diet Versus Mediterranean Diet at the Gut Microbiota-Immune System Interplay. Implications for Health and Disease. Nutrients 2021, 13, 699. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.J.; Abed, B.; Corpuz, G.G.; Spoden, M. Dietary patterns: What’s in a name? Nutr. Today 2017, 52, 137–142. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef] [Green Version]
- Muraki, I.; Imamura, F.; Manson, J.E.; Hu, F.B.; Willett, W.C.; van Dam, R.M.; Sun, Q. Fruit consumption and risk of type 2 diabetes: Results from three prospective longitudinal cohort studies. BMJ 2013, 347, f5001. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Kawakami, R.; Tanisawa, K.; Miyawaki, R.; Ishii, K.; Torii, S.; Suzuki, K.; Sakamoto, S.; Muraoka, I.; Oka, K.; et al. Dietary patterns and abdominal obesity in middle-aged and elderly Japanese adults: Waseda Alumni’s Sports, Exercise, Daily Activity, Sedentariness and Health Study (WASEDA’S Health Study). Nutrition 2019, 58, 149–155. [Google Scholar] [CrossRef]
- Shimabukuro, M. Cardiac adiposity and global cardiometabolic risk: New concept and clinical implication. Circ. J. 2009, 73, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Tanabe, H.; Masuzaki, H.; Shimabukuro, M. Novel strategies for glycaemic control and preventing diabetic complications applying the clustering-based classification of adult-onset diabetes mellitus: A perspective. Diabetes Res. Clin. Pract. 2021, 180, 109067. [Google Scholar] [CrossRef]
- Bertoia, M.L.; Mukamal, K.J.; Cahill, L.E.; Hou, T.; Ludwig, D.S.; Mozaffarian, D.; Willett, W.C.; Hu, F.B.; Rimm, E.B. Changes in Intake of Fruits and Vegetables and Weight Change in United States Men and Women Followed for Up to 24 Years: Analysis from Three Prospective Cohort Studies. PLoS Med. 2015, 12, e1001878. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, R.E.; Elvestad, M.; Molin, M.; Aune, D. Fruit and vegetable consumption and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis of prospective studies. BMJ Nutr. Prev. Health 2021, 4, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Woo, H.D.; Cho, M.J.; Park, J.K.; Kim, S.S. Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults. Nutrients 2019, 11, 1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Shi, Z. Dietary Pattern during 1991–2011 and Its Association with Cardio Metabolic Risks in Chinese Adults: The China Health and Nutrition Survey. Nutrients 2017, 9, 1218. [Google Scholar] [CrossRef] [Green Version]
- Hermansen, K.; Sondergaard, M.; Hoie, L.; Carstensen, M.; Brock, B. Beneficial effects of a soy-based dietary supplement on lipid levels and cardiovascular risk markers in type 2 diabetic subjects. Diabetes Care 2001, 24, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Wakita Asano, A.; Hayashi, F.; Miyoshi, M.; Arai, Y.; Yoshita, K.; Yamamoto, S.; Yoshiike, N. Demographics, health-related behaviors, eating habits and knowledge associated with vegetable intake in Japanese adults. Eur. J. Clin. Nutr. 2009, 63, 1335–1344. [Google Scholar] [CrossRef]
- Northstone, K. Dietary patterns: The importance of sex differences. Br. J. Nutr. 2012, 108, 393–394. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.H.; Qiao, N.; Huang, J.J.; Sun, C.M.; Cui, Y.; Tian, S.S.; Wang, C.; Liu, X.M.; Zhang, H.X.; Wang, H.; et al. Gender Differences in Dietary Patterns and Their Association with the Prevalence of Metabolic Syndrome among Chinese: A Cross-Sectional Study. Nutrients 2016, 8, 180. [Google Scholar] [CrossRef] [Green Version]
- Sharkey, T.; Whatnall, M.C.; Hutchesson, M.J.; Haslam, R.L.; Bezzina, A.; Collins, C.E.; Ashton, L.M. Effectiveness of gender-targeted versus gender-neutral interventions aimed at improving dietary intake, physical activity and/or overweight/obesity in young adults (aged 17–35 years): A systematic review and meta-analysis. Nutr. J. 2020, 19, 78. [Google Scholar] [CrossRef]
- Eshak, E.S.; Iso, H.; Mizoue, T.; Inoue, M.; Noda, M.; Tsugane, S. Soft drink, 100% fruit juice, and vegetable juice intakes and risk of diabetes mellitus. Clin. Nutr. 2013, 32, 300–308. [Google Scholar] [CrossRef]
- Ulven, S.M.; Holven, K.B.; Gil, A.; Rangel-Huerta, O.D. Milk and Dairy Product Consumption and Inflammatory Biomarkers: An Updated Systematic Review of Randomized Clinical Trials. Adv. Nutr. 2019, 10, S239–S250. [Google Scholar] [CrossRef] [PubMed]
- Savaiano, D.A.; Hutkins, R.W. Yogurt, cultured fermented milk, and health: A systematic review. Nutr. Rev. 2021, 79, 599–614. [Google Scholar] [CrossRef] [PubMed]
- Companys, J.; Pla-Paga, L.; Calderon-Perez, L.; Llaurado, E.; Sola, R.; Pedret, A.; Valls, R.M. Fermented Dairy Products, Probiotic Supplementation, and Cardiometabolic Diseases: A Systematic Review and Meta-analysis. Adv. Nutr. 2020, 11, 834–863. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef] [Green Version]
- den Braver, N.R.; Lakerveld, J.; Rutters, F.; Schoonmade, L.J.; Brug, J.; Beulens, J.W.J. Built environmental characteristics and diabetes: A systematic review and meta-analysis. BMC Med. 2018, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, D.C.; Threapleton, D.E.; Evans, C.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Burley, V.J. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: Systematic review and dose-response meta-analysis of prospective studies. Br. J. Nutr. 2014, 112, 725–734. [Google Scholar] [CrossRef]
- Guess, N.D. Dietary Interventions for the Prevention of Type 2 Diabetes in High-Risk Groups: Current State of Evidence and Future Research Needs. Nutrients 2018, 10, 1245. [Google Scholar] [CrossRef] [Green Version]
- Goto, A.; Goto, M.; Noda, M.; Tsugane, S. Incidence of type 2 diabetes in Japan: A systematic review and meta-analysis. PLoS ONE 2013, 8, e74699. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Arisawa, K.; Katsuura-Kamano, S.; Uemura, H.; Tsukamoto, M.; Kadomatsu, Y.; Okada, R.; Hishida, A.; Tanaka, K.; Hara, M.; et al. Associations of Nutrient Patterns with the Prevalence of Metabolic Syndrome: Results from the Baseline Data of the Japan Multi-Institutional Collaborative Cohort Study. Nutrients 2019, 11, 990. [Google Scholar] [CrossRef] [Green Version]
- Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Honkura, K.; Watanabe, T.; Zhang, S.; Sugawara, Y.; Tsuji, I. Dietary Patterns and Incident Dementia in Elderly Japanese: The Ohsaki Cohort 2006 Study. J. Gerontol. Ser. A 2016, 71, 1322–1328. [Google Scholar] [CrossRef] [Green Version]
- Fung, T.T.; Schulze, M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dietary patterns, meat intake, and the risk of type 2 diabetes in women. Arch. Intern. Med. 2004, 164, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; et al. Novel subgroups of adult-onset diabetes and their association with outcomes: A data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018, 6, 361–369. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (n = 22,740) | Men (n = 8465) | Women (n = 14,275) | p Value | |
|---|---|---|---|---|
| Age (years) | 55.9 (15.7) | 58.2 (15.4) | 54.6 (15.8) | <0.001 |
| Education ≥ vocational university | 25.8 | 22.6 | 27.7 | <0.001 |
| Current smoker | 16.4 | 29.4 | 8.7 | <0.001 |
| Current alcohol drinking | 45.0 | 69.8 | 30.3 | <0.001 |
| Physical activity ≥ 2 times/week | 34.6 | 39.0 | 32.0 | <0.001 |
| K6 ≥ 13 | 13.7 | 10.6 | 15.5 | <0.001 |
| Live at shelter/temporary house | 43.6 | 43.9 | 43.5 | 0.193 |
| BMI (kg/m2) | 23.4 (3.6) | 24.2 (3.3) | 22.9 (3.7) | <0.001 |
| BMI ≥ 25 kg/m2 | 29.8 | 37.6 | 25.1 | <0.001 |
| Hypertension | 39.8 | 49.3 | 34.1 | <0.001 |
| SBP (mmHg) | 127.0 (16.9) | 130.9 (15.8) | 124.7 (17.1) | <0.001 |
| DBP (mmHg) | 76.7 (10.9) | 79.8 (10.4) | 74.8 (10.7) | <0.001 |
| Fasting blood glucose (mg/dL) | 93 [88, 100] | 96 [90, 103] | 92 [87, 98] | <0.001 |
| LDL-C (mg/dL) | 124.3 (32.4) | 122.8 (32.0) | 125.1 (32.6) | <0.001 |
| LDL-C ≥ 140 mg/dL | 30.2 | 29.2 | 30.8 | 0.008 |
| HDL-C (mg/dL) | 61.3 (15.3) | 55.7 (14.4) | 64.6 (14.9) | <0.001 |
| HDL-C < 40 mg/dL | 5.6 | 10.3 | 2.8 | <0.001 |
| Triglycerides (mg/dL) | 91 [64, 130] | 105 [74, 151] | 83 [60, 118] | <0.001 |
| Triglycerides ≥ 150 mg/dL | 17.8 | 25.8 | 13.1 | <0.001 |
| Typical Japanese pattern score | −0.02 [−0.71, 0.71] | −0.02 [−0.69, 0.70] | −0.02 [−0.71, 0.71] | 0.817 |
| Juice pattern score | −0.18 [−0.69, 0.46] | −0.17 [−0.69, 0.45] | −0.19 [−0.69, 0.46] | 0.657 |
| Meat pattern score | −0.21 [−0.67, 0.50] | −0.23 [−0.66, 0.46] | −0.20 [−0.68, 0.53] | 0.383 |
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total | Person -Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | New onset T2DM | 142 | (19.4) | 136 | (18.6) | 92 | (12.6) | 114 | (15.6) | 104 | (14.2) | 83 | (11.4) | 60 | (8.2) | 731 | 40,688 |
| Fasting blood glucose, ≥126 mg/dL | 84 | (19.2) | 66 | (15.1) | 51 | (11.7) | 60 | (13.7) | 65 | (14.9) | 52 | (11.9) | 59 | (13.5) | 437 | 41,450 | |
| HbA1c, >6.5% | 64 | (16.0) | 81 | (20.3) | 42 | (10.5) | 59 | (14.8) | 50 | (12.5) | 56 | (14.0) | 48 | (12) | 400 | 41,558 | |
| Women | New onset T2DM | 113 | (15.8) | 132 | (18.4) | 87 | (12.1) | 114 | (15.9) | 106 | (14.8) | 99 | (13.8) | 66 | (9.2) | 717 | 73,082 |
| Fasting blood glucose, ≥126 mg/dL | 59 | (15.6) | 57 | (15.1) | 55 | (14.6) | 52 | (13.8) | 56 | (14.9) | 47 | (12.5) | 51 | (13.5) | 377 | 73,946 | |
| HbA1c, >6.5% | 52 | (12.1) | 86 | (20.0) | 47 | (11.0) | 61 | (14.2) | 63 | (14.7) | 66 | (15.4) | 54 | (12.6) | 429 | 73,854 | |
| Dietary Pattern Scores | All (n = 22,740) | Men (n = 8465) | Women (n = 14,275) | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | HR | 95% CI | ||
| Typical Japanese | |||||||
| Model 1 a | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 0.79 | (0.68, 0.92) | 0.78 | (0.63, 0.97) | 0.80 | (0.64, 1.00) | |
| Q3 | 0.79 | (0.68, 0.92) | 0.73 | (0.58, 0.90) | 0.86 | (0.70, 1.07) | |
| Q4 | 0.71 | (0.60, 0.83) | 0.78 | (0.63, 0.97) | 0.64 | (0.51, 0.80) | |
| P for trend | <0.001 | 0.048 | <0.001 | ||||
| Model 2 b | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 0.81 | (0.69, 0.94) | 0.79 | (0.64, 0.98) | 0.82 | (0.66, 1.03) | |
| Q3 | 0.80 | (0.69, 0.93) | 0.72 | (0.58, 0.90) | 0.89 | (0.72, 1.10) | |
| Q4 | 0.74 | (0.63, 0.86) | 0.78 | (0.63, 0.97) | 0.70 | (0.56, 0.88) | |
| P for trend | 0.011 | 0.042 | 0.005 | ||||
| Model 3 c | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 0.82 | (0.70, 0.96) | 0.81 | (0.65, 1.01) | 0.84 | (0.67, 1.05) | |
| Q3 | 0.83 | (0.71, 0.97) | 0.74 | (0.60, 0.92) | 0.93 | (0.75, 1.15) | |
| Q4 | 0.80 | (0.68, 0.94) | 0.85 | (0.68, 1.06) | 0.76 | (0.60, 0.95) | |
| P for trend | 0.015 | 0.181 | 0.04 | ||||
| Juice | |||||||
| Model 1 a | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.01 | (0.88, 1.17) | 1.03 | (0.84, 1.27) | 1.00 | (0.82, 1.23) | |
| Q3 | 0.90 | (0.78, 1.05) | 0.97 | (0.79, 1.20) | 0.85 | (0.68, 1.05) | |
| Q4 | 0.96 | (0.83, 1.11) | 0.97 | (0.79, 1.20) | 0.96 | (0.78, 1.18) | |
| P for trend | 0.427 | 0.690 | 0.563 | ||||
| Model 2 b | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.00 | (0.86, 1.16) | 1.01 | (0.82, 1.24) | 1.00 | (0.82, 1.23) | |
| Q3 | 0.89 | (0.76, 1.03) | 0.95 | (0.77, 1.16) | 0.84 | (0.68, 1.04) | |
| Q4 | 0.95 | (0.83, 1.11) | 0.94 | (0.77, 1.16) | 0.99 | (0.80, 1.21) | |
| P for trend | 0385 | 0.503 | 0.728 | ||||
| Model 3 c | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.01 | (0.87, 1.17) | 1.02 | (0.83, 1.26) | 0.99 | (0.81, 1.22) | |
| Q3 | 0.90 | (0.78, 1.05) | 0.97 | (0.79, 1.20) | 0.83 | (0.67, 1.03) | |
| Q4 | 0.99 | (0.86, 1.15) | 0.99 | (0.80, 1.23) | 1.01 | (0.82, 1.24) | |
| P for trend | 0.773 | 0.832 | 0.912 | ||||
| Meat | |||||||
| Model 1 a | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.14 | (0.99, 1.30) | 1.13 | (0.94, 1.37) | 1.15 | (0.95, 1.39) | |
| Q3 | 0.89 | (0.76, 1.03) | 0.89 | (0.72, 1.10) | 0.89 | (0.73, 1.10) | |
| Q4 | 1.01 | (0.87, 1.17) | 1.04 | (0.84, 1.29) | 0.97 | (0.79, 1.20) | |
| P for trend | 0.455 | 0.846 | 0.415 | ||||
| Model 2 b | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.13 | (0.99, 1.29) | 1.12 | (0.92, 1.35) | 1.15 | (0.95, 1.39) | |
| Q3 | 0.90 | (0.78, 1.05) | 0.91 | (0.74, 1.13) | 0.89 | (0.73, 1.10) | |
| Q4 | 1.03 | (0.88, 1.19) | 1.07 | (0.87, 1.33) | 0.98 | (0.80, 1.21) | |
| P for trend | 0.694 | 0.898 | 0.465 | ||||
| Model 3 c | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.13 | (0.99, 1.29) | 1.11 | (0.91, 1.34) | 1.17 | (0.96, 1.41) | |
| Q3 | 0.91 | (0.78, 1.06) | 0.90 | (0.72, 1.11) | 0.92 | (0.74, 1.13) | |
| Q4 | 1.05 | (0.90, 1.22) | 1.06 | (0.86, 1.32) | 1.03 | (0.83, 1.27) | |
| P for trend | 0.883 | 0.959 | 0.747 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, E.; Ohira, T.; Hirai, H.; Okazaki, K.; Nagao, M.; Hayashi, F.; Nakano, H.; Suzuki, Y.; Sakai, A.; Takahashi, A.; et al. Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey. Nutrients 2022, 14, 4872. https://doi.org/10.3390/nu14224872
Ma E, Ohira T, Hirai H, Okazaki K, Nagao M, Hayashi F, Nakano H, Suzuki Y, Sakai A, Takahashi A, et al. Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey. Nutrients. 2022; 14(22):4872. https://doi.org/10.3390/nu14224872
Chicago/Turabian StyleMa, Enbo, Tetsuya Ohira, Hiroyuki Hirai, Kanako Okazaki, Masanori Nagao, Fumikazu Hayashi, Hironori Nakano, Yuriko Suzuki, Akira Sakai, Atsushi Takahashi, and et al. 2022. "Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey" Nutrients 14, no. 22: 4872. https://doi.org/10.3390/nu14224872