
Short-Term Protein Supplementation Does Not Alter Energy Intake, Macronutrient Intake and Appetite in 50–75 Year Old Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Ethics
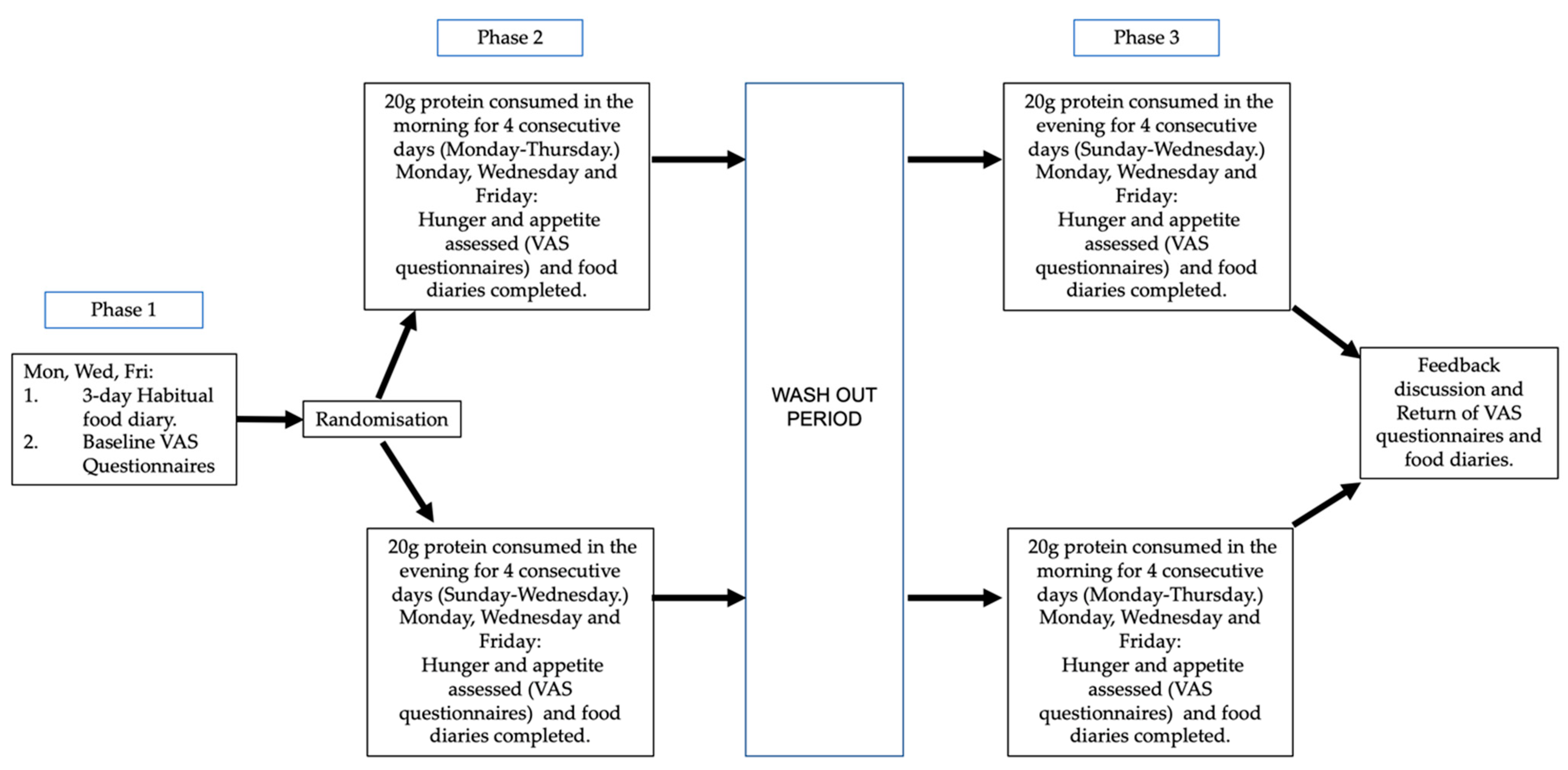
2.2. Design and Intervention
2.3. Data Analysis
3. Results
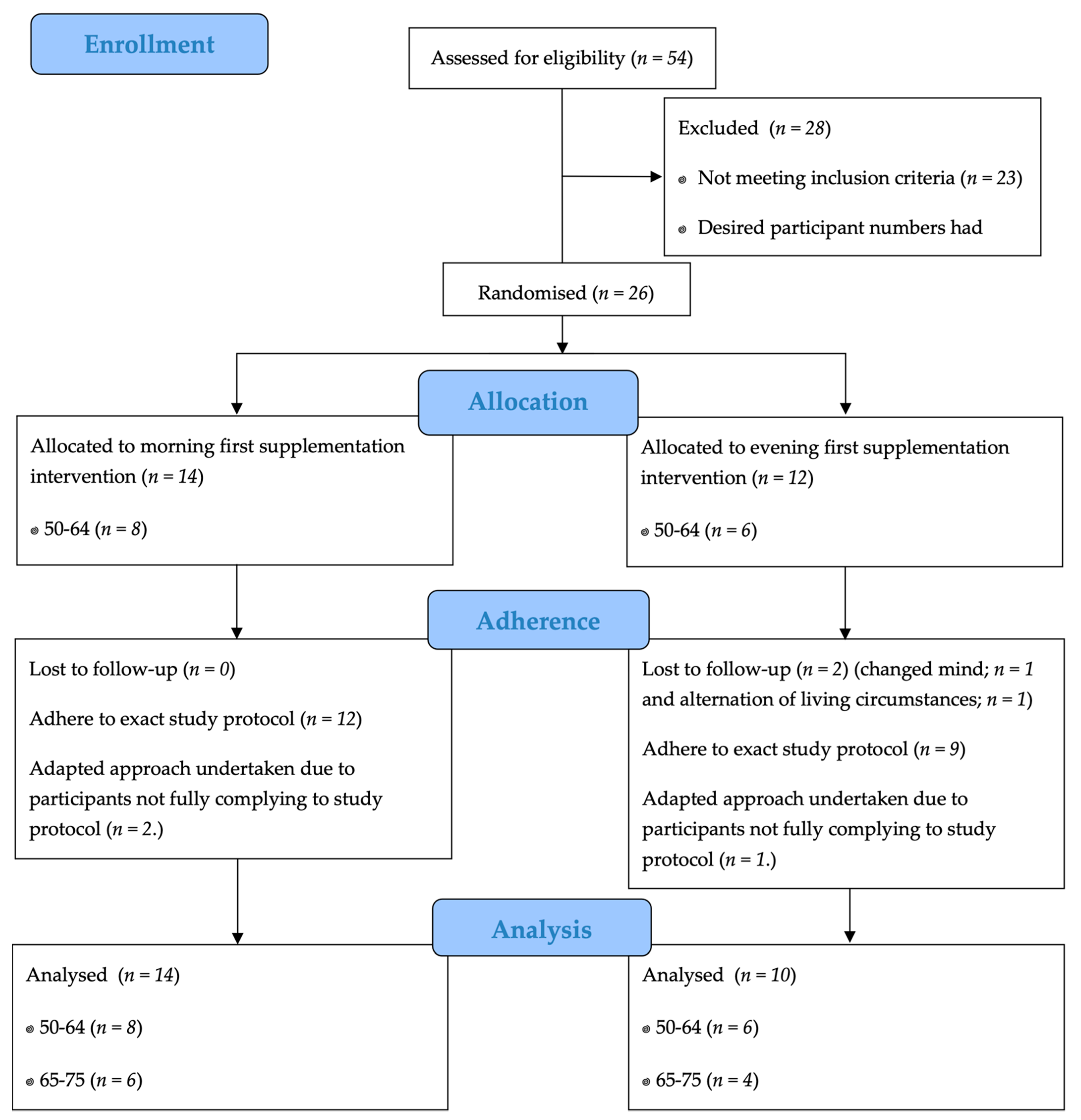
3.1. Participants
3.2. Self-Reported Appetite Ratings
3.3. Nutrient Intakes
3.3.1. Energy and Macronutrient Intake
3.3.2. Further Protein Analysis, Following Adjustments for Body Mass
3.3.3. Fibre and Micronutrient Intake
4. Discussion
4.1. Limitations
4.2. Future Work
5. Conclusions
- There is negligible effect of protein supplementation on appetite and energy intake, in middle-older aged adults.
- Protein supplementation either in the evening or after breakfast may provide a viable strategy for increasing dietary protein intake in the middle-older age population.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Beasley, J.M.; Shikany, J.M.; Thomson, C.A. The role of dietary protein. Intake in the prevention of sarcopenia of aging. Nutr. Clin. Pract. 2013, 28, 684–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, S.; Cooper, C.; Aihie Sayer, A. Nutrition and sarcopenia: A review of the evidence and implications for preventive strategies. J. Aging Res. 2012, 12, 510801. [Google Scholar] [CrossRef] [PubMed]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Health ABC Study. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, C.M.; Austin, S.; Corfe, B.M.; Green, M.A.; Johnstone, A.M.; Stevenson, E.J.; Brunstrom, J.M. Protein Valuation in Food Choice Is Positively Associated with Lean Mass in Older Adults. J. Nutr. 2019, 149, 2056–2064. [Google Scholar] [CrossRef]
- Bradlee, M.L.; Mustafa, J.; Singer, M.R.; Moore, L.L. High-protein foods and physical activity protect against age-related muscle loss and functional decline. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 88–94. [Google Scholar] [CrossRef]
- Department of Health. Dietary Reference Values for Food Energy and Nutrients Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy; Report on Health and Social Subjects 41; HMSO: London, UK, 1991. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Nutr. Metab. Care 2010, 12, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Marzetti, E. Anorexia of aging: Risk factors, consequences, and potential treatments. Nutrients 2016, 8, 69. [Google Scholar] [CrossRef]
- Astrup, A. The satiating power of protein—A key to obesity prevention? Am. J. Clin. Nutr. 2005, 82, 1–2. [Google Scholar] [CrossRef]
- Westerterp-Plantenga, M.S.; Lemmens, S.G.; Westerterp, K.R. Dietary protein—Its role in satiety, energetics, weight loss and health. Br. J. Nutr. 2012, 108, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigle, D.S.; Breen, P.A.; Matthys, C.C.; Callahan, H.S.; Meeuws, K.E.; Burden, V.R.; Purnell, J.Q. A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. Am. J. Clin. Nutr. 2005, 82, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Irvine, P.; Mouzet, J.B.; Marteau, C.; Sallé, A.; Genaitay, M.; Favreau, A.M.; Ritz, P. Short-term effect of a protein load on appetite and food intake in diseased mildly undernourished elderly people. Clin. Nutr. 2004, 23, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Ben-Harchache, S.; Roche, H.M.; Corish, C.A.; Horner, K. Does protein supplementation impact appetite and energy intake in older adults? A systematic review. Proc. Nutr. Soc. 2020, 79, 610. [Google Scholar] [CrossRef]
- Soenen, S.; Giezenaar, C.; Hutchison, A.T.; Horowitz, M.; Chapman, I.; Luscombe-Marsh, N.D. Effects of intraduodenal protein on appetite, energy intake, and antropyloroduodenal motility in healthy older compared with young men in a randomized trial. Am. J. Clin. Nutr. 2014, 100, 1108–1115. [Google Scholar] [CrossRef] [Green Version]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Distribution but not amount of protein intake is associated with frailty: A cross-sectional investigation in the region of Nürnberg. Nutr. J. 2013, 12, 109. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.; Cater, J.D.; Green, M.A.; Johnstone, A.M.; Brunstrom, J.M.; Stevenson, E.J.; Corfe, B.M. Inadequacy of protein intake in older UK adults. Geriatrics 2020, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Lonnie, M.; Hooker, E.; Brunstrom, J.M.; Corfe, B.M.; Green, M.A.; Watson, A.W.; Johnstone, A.M. Protein for life: Review of optimal protein intake, sustainable dietary sources and the effect on appetite in ageing adults. Nutrients 2018, 10, 360. [Google Scholar] [CrossRef] [Green Version]
- Nelson, M. Food Portion Sizes: A Photographic Atlas; MAFF Publications: London, UK, 1997. [Google Scholar]
- Flint, A.; Raben, A.; Blundell, J.E.; Astrup, A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int. J. Obes. 2000, 24, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, W.L.; Millward, D.J.; Long, S.J.; Morgan, L.M. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br. J. Nutr. 2003, 89, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Westman, E.; Mattes, R.D.; Wolfe, R.R.; Astrup, A.; Westerterp-Plantenga, M. Protein, weight management, and satiety. Am. J. Clin. Nutr. 2008, 87, 1558S–1561S. [Google Scholar] [CrossRef] [Green Version]
- Snijders, T.; Trommelen, J.; Kouw, I.W.K.; Holwerda, A.M.; Verdijk, L.B.; van Loon, L.J.C. The impact of pre-sleep protein ingestion on the skeletal muscle adaptive response to exercise in humans: An update. Front. Nutr. 2019, 6, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morehen, S.; Smeuninx, B.; Perkins, M.; Morgan, P.; Breen, L. Pre-Sleep Casein Protein Ingestion Does Not Impact Next-Day Appetite, Energy Intake and Metabolism in Older Individuals. Nutrients 2020, 12, 90. [Google Scholar] [CrossRef] [Green Version]
- Holt, G.M.; Owen, L.J.; Till, S.; Cheng, Y.; Grant, V.A.; Harden, C.J. Systematic literature review shows that appetite rating does not predict energy intake. Crit. Rev. Food Sci. Nutr. 2017, 57, 3577–3582. Available online: https://www.tandfonline.com/doi/abs/10.1080/10408398.2016.1246414 (accessed on 8 April 2021). [CrossRef] [PubMed]
- Krok-Schoen, J.L.; Archdeacon Price, A.; Luo, M.; Kelly, O.J.; Taylor, C.A. Low Dietary Protein Intakes and Associated Dietary Patterns and Functional Limitations in an Aging Population: A NHANES Analysis. J. Nutr. Health Aging 2019, 23, 338–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Self-Reported Measure | Participants (n = 24) | ||||
|---|---|---|---|---|---|
| Baseline | Morning Supplementation | Evening Supplementation | |||
| Median (IQR) Response (mm) | Median (IQR) Response (mm) | p-Value $ | Median (IQR) Response (mm) | p-Value # | |
| Hunger | 41 (29–48) | 36 (16–48) | 0.267 | 38 (24–44) | 0.520 |
| Satisfaction | 53 (45–60) | 52 (49–69) | 0.415 | 50 (43–57) | 0.709 |
| Intent to eat | 49 (43–58) | 36 (26–51) | 0.012 * | 44 (35–54) | 0.035 |
| Eating desire | 35 (23–58) | 41 (22–49) | 0.506 | 37 (21–46) | 0.189 |
| Intake | Baseline | Morning Supplementation | Evening Supplementation | ||
|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | p-Value $ | Median (IQR) | p-Value # | |
| Energy (kJ/d) | 7804 (6868–9317) | 7420 (6419–9093) | 0.376 | 7712 (6303–9344) | 0.338 |
| Carbohydrate (g/d) | 216.4 (177.6–248.0) | 202.8 (177.2–246.1) | 0.587 | 204.5 (168.7–259.7) | 0.361 |
| % of energy from carbohydrate | 46.8 | 46.9 | 0.987 | 45.4 | 0.658 |
| Fat (g/d) | 75.2 (63.2–99.1) | 73.4 (59.5–95.4) | 0.407 | 76.7 (65.1–96.4) | 0.597 |
| % of energy from fat | 37.6 | 37.2 | 0.638 | 38.5 | 0.779 |
| Protein (g/d) | 80.6 (62.6–97.4) | 74.1 (70.0–91.0) | 0.753 | 73.1 (64.8–93.1) | 0.700 |
| % of energy from protein. | 16.7 | 17.5 | 0.224 | 17.4 | 0.475 |
| Protein after body mass adjustments (g/kg BM) | 1.21 (1.03–1.45) | 1.14 (1.03–1.45) | 0.876 | 1.20 (0.94–1.39) | 0.957 |
| Percentage of participants consuming ≥ 0.75 g of protein per kg body mass. (%) | 95.8 | 95.8 | >0.999 | 91.7 | 0.885 |
| Percentage of participants consuming ≥ 1 g of protein per kg body mass. (%) | 66.7 | 79.2 | 0.615 | 66.7 | >0.999 |
| Percentage of participants consuming ≥ 1.2 g of protein per kg body mass. (%) | 50.0 | 45.8 | >0.832 | 45.8 | 0.832 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuttiett, E.R.; Green, D.J.; Stevenson, E.J.; Hill, T.R.; Corfe, B.M.; Williams, E.A. Short-Term Protein Supplementation Does Not Alter Energy Intake, Macronutrient Intake and Appetite in 50–75 Year Old Adults. Nutrients 2021, 13, 1711. https://doi.org/10.3390/nu13051711
Tuttiett ER, Green DJ, Stevenson EJ, Hill TR, Corfe BM, Williams EA. Short-Term Protein Supplementation Does Not Alter Energy Intake, Macronutrient Intake and Appetite in 50–75 Year Old Adults. Nutrients. 2021; 13(5):1711. https://doi.org/10.3390/nu13051711
Chicago/Turabian StyleTuttiett, Esme R., Dan J. Green, Emma J. Stevenson, Thomas R. Hill, Bernard M. Corfe, and Elizabeth A. Williams. 2021. "Short-Term Protein Supplementation Does Not Alter Energy Intake, Macronutrient Intake and Appetite in 50–75 Year Old Adults" Nutrients 13, no. 5: 1711. https://doi.org/10.3390/nu13051711