Selenium and Coenzyme Q10 Supplementation Improves Renal Function in Elderly Deficient in Selenium: Observational Results and Results from a Subgroup Analysis of a Prospective Randomised Double-Blind Placebo-Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Ethical Approval
2.3. Blood Sampling
2.4. Determination of Selenium
2.5. Determination of Creatinine and Cystatin-C
2.6. Determination of Renal Function
- eGFRCreatinine was estimated in mL/min/1.73 m2 using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation from 2009 [38].
- eGFRCystatin C in mL/min/1.73 m2 was calculated from cystatin-C using the CKD-EPI cystatin-C equation for estimating GFR with standardised serum cystatin-C values [39].
- eGFRCombined in mL/min/1.73 m2 was calculated using the CKD-EPI combined creatinine/cystatin-C equation [40].
2.7. Statistical Methods
3. Results
3.1. Association Between Serum Selenium and Renal Function
3.2. Intervention with Selenium and CoQ10, and Impact on Renal Function
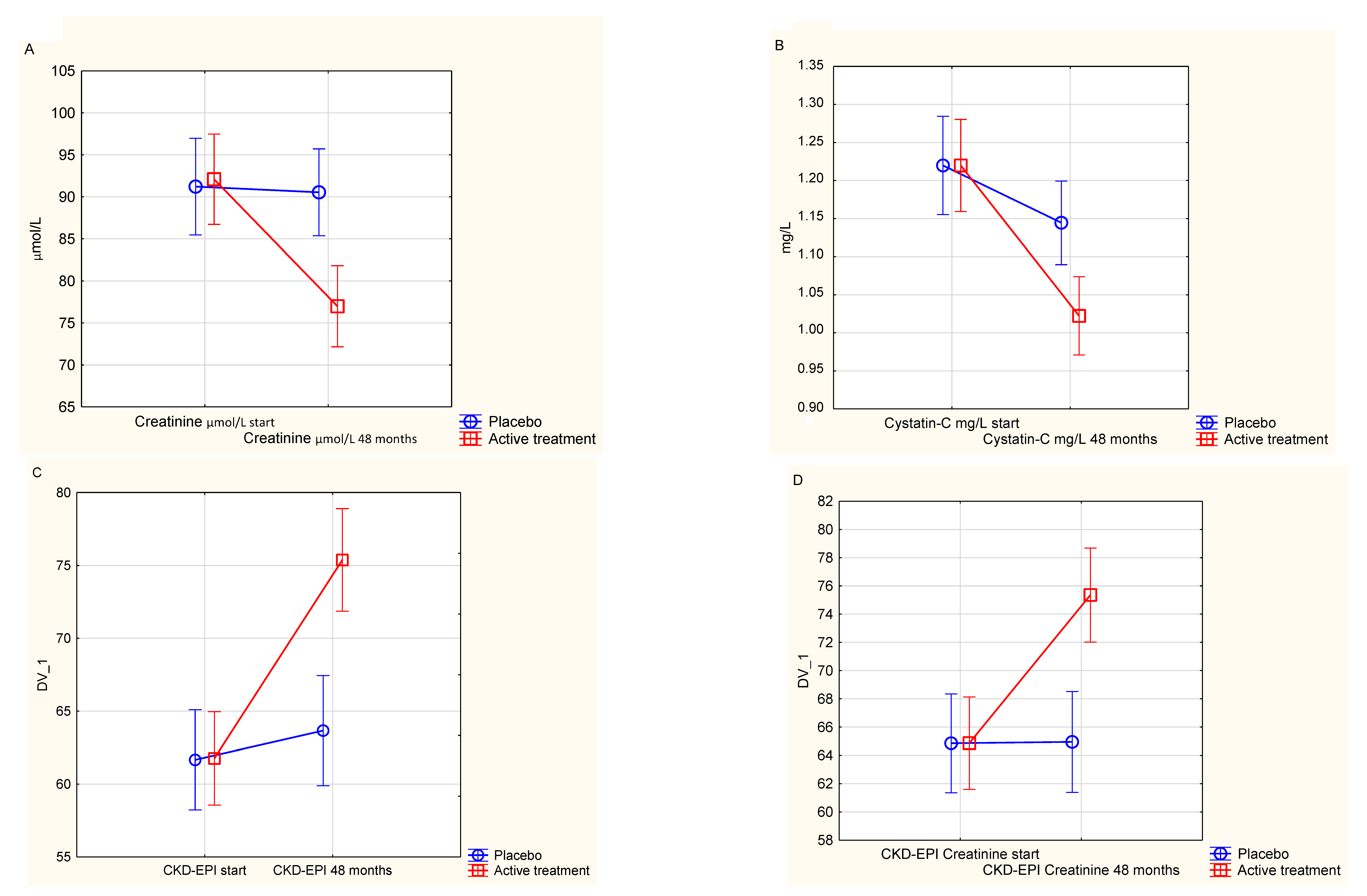
3.3. Evaluating the Effect of Intervention on Creatinine
3.4. Evaluating the Effect of Intervention on Cystatin-C
3.5. Evaluating the Effect of Intervention on CKD-EPI Based on Both Creatinine and Cystatin-C
3.6. Evaluating the Effect of Intervention on CKD-EPI Based on Creatinine
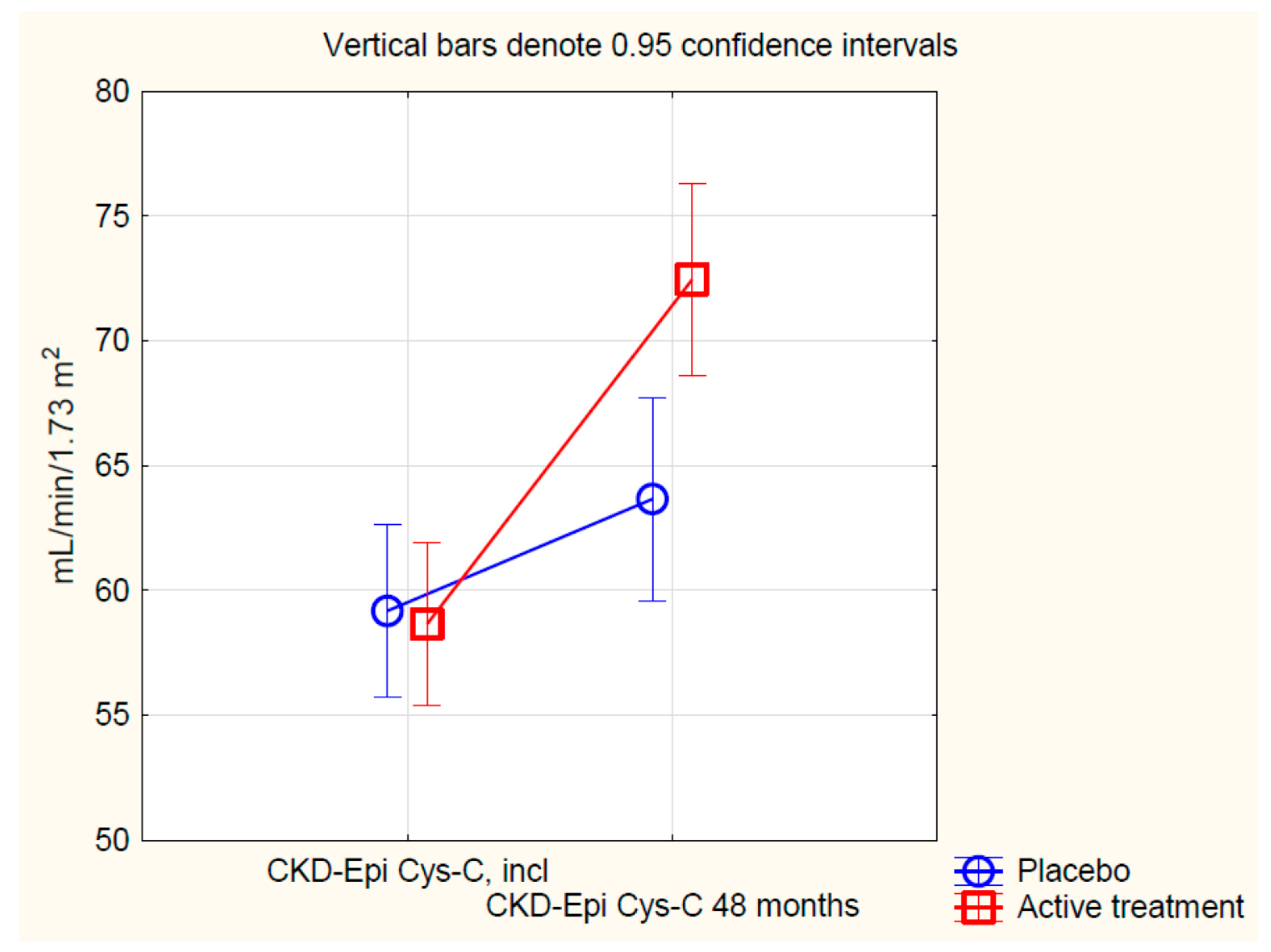
3.7. Evaluating the Effect of Intervention on CKD-EPI Based on Cystatin-C
3.8. Impact of Pre-Intervention Selenium Concentration on the Effect of Supplementation on the Renal Function
3.9. Analysing the Effect of Supplementation Based on Pre-Intervention eGFR
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Kousa, O.; Mullane, R.; Aboeata, A. Cardiorenal Syndrome; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Ovchinnikov, A.G.; Arefieva, T.I.; Potekhina, A.V.; Filatova, A.Y.; Ageev, F.T.; Boytsov, S.A. The Molecular and Cellular Mechanisms Associated with a Microvascular Inflammation in the Pathogenesis of Heart Failure with Preserved Ejection Fraction. Acta Nat. 2020, 12, 40–51. [Google Scholar] [CrossRef]
- Silvis, M.J.M.; Demkes, E.J.; Fiolet, A.T.L.; Dekker, M.; Bosch, L.; van Hout, G.P.J.; Timmers, L.; de Kleijn, D.P.V. Immunomodulation of the NLRP3 Inflammasome in Atherosclerosis, Coronary Artery Disease, and Acute Myocardial Infarction. J. Cardiovasc. Transl. Res. 2020. [Google Scholar] [CrossRef]
- West, H.W.; Antoniades, C. Imaging and Targeting Coronary Artery Inflammation. Antioxid. Redox Signal 2020. [Google Scholar] [CrossRef]
- Ruiz-Ortega, M.; Rayego-Mateos, S.; Lamas, S.; Ortiz, A.; Rodrigues-Diez, R.R. Targeting the progression of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 269–288. [Google Scholar] [CrossRef]
- Lin, T.Y.; Hsu, Y.H. IL-20 in Acute Kidney Injury: Role in Pathogenesis and Potential as a Therapeutic Target. Int. J. Mol. Sci. 2020, 21, 1009. [Google Scholar] [CrossRef] [Green Version]
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and Oxidative Stress in Chronic Kidney Disease-Potential Therapeutic Role of Minerals, Vitamins and Plant-Derived Metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Andres, O.; Sanchez-Nino, M.D.; Moreno, J.A.; Ruiz-Ortega, M.; Ramos, A.M.; Sanz, A.B.; Ortiz, A. Downregulation of kidney protective factors by inflammation: Role of transcription factors and epigenetic mechanisms. Am. J. Physiol. Renal Physiol. 2016, 311, F1329–F1340. [Google Scholar] [CrossRef] [Green Version]
- Fairweather-Tait, S.J.; Bao, Y.; Broadley, M.R.; Collings, R.; Ford, D.; Hesketh, J.E.; Hurst, R. Selenium in human health and disease. Antioxid. Redox Signal. 2011, 14, 1337–1383. [Google Scholar] [CrossRef]
- Selenius, M.; Rundlof, A.K.; Olm, E.; Fernandes, A.P.; Bjornstedt, M. Selenium and the selenoprotein thioredoxin reductase in the prevention, treatment and diagnostics of cancer. Antioxid. Redox Signal. 2010, 12, 867–880. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Xia, Y.; Hill, K.E.; Li, P.; Xu, J.; Zhou, D.; Motley, A.K.; Wang, L.; Byrne, D.W.; Burk, R.F. Optimization of selenoprotein P and other plasma selenium biomarkers for the assessment of the selenium nutritional requirement: A placebo-controlled, double-blind study of selenomethionine supplementation in selenium-deficient Chinese subjects. Am. J. Clin. Nutr. 2010, 92, 525–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bomer, N.; Grote Beverborg, N.; Hoes, M.F.; Streng, K.W.; Vermeer, M.; Dokter, M.M.; IJmker, J.; Anker, S.D.; Cleland, J.G.F.; Hillege, H.L.; et al. Selenium and outcome in heart failure. Eur. J. Heart Fail 2019. [Google Scholar] [CrossRef] [Green Version]
- Manzanares, W.; Biestro, A.; Galusso, F.; Torre, M.H.; Manay, N.; Pittini, G.; Facchin, G.; Hardy, G. Serum selenium and glutathione peroxidase-3 activity: Biomarkers of systemic inflammation in the critically ill? Intensive Care Med. 2009, 35, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Zachara, B.A.; Pawluk, H.; Bloch-Boguslawska, E.; Sliwka, K.M.; Korenkiewicz, J.; Skok, Z.; Ryc, K. Tissue level, distribution, and total body selenium content in healthy and diseased humans in Poland. Arch. Environ. Health 2001, 56, 461–466. [Google Scholar] [CrossRef]
- Ceballos-Picot, I.; Witko-Sarsat, V.; Merad-Boudia, M.; Nguyen, A.T.; Thevenin, M.; Jaudon, M.C.; Zingraff, J.; Verger, C.; Jungers, P.; Descamps-Latscha, B. Glutathione antioxidant system as a marker of oxidative stress in chronic renal failure. Free Radic. Biol. Med. 1996, 21, 845–853. [Google Scholar] [CrossRef]
- Zachara, B.A.; Gromadzinska, J.; Wasowicz, W.; Zbrog, Z. Red blood cell and plasma glutathione peroxidase activities and selenium concentration in patients with chronic kidney disease: A review. Acta Biochim. Pol. 2006, 53, 663–677. [Google Scholar]
- Yoshimura, S.; Suemizu, H.; Nomoto, Y.; Sakai, H.; Katsuoka, Y.; Kawamura, N.; Moriuchi, T. Plasma glutathione peroxidase deficiency caused by renal dysfunction. Nephron 1996, 73, 207–211. [Google Scholar] [CrossRef]
- Lai, H.; Nie, T.; Zhang, Y.; Chen, Y.; Tao, J.; Lin, T.; Ge, T.; Li, F.; Li, H. Selenium Deficiency-Induced Damage and Altered Expression of Mitochondrial Biogenesis Markers in the Kidneys of Mice. Biol. Trace Elem. Res. 2020. [Google Scholar] [CrossRef]
- Hasanvand, A.; Abbaszadeh, A.; Darabi, S.; Nazari, A.; Gholami, M.; Kharazmkia, A. Evaluation of selenium on kidney function following ischemic injury in rats; protective effects and antioxidant activity. J. Renal. Inj. Prev. 2017, 6, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J. Selenium, in Nordberg GF, Fowler BA and Nordberg M, eds. Handbook on the Toxicology of Metals; Elsevier/AP: Amsterdam, The Netherlands, 2015; Volume II, Chapter 52; pp. 1176–1208. [Google Scholar]
- Li, X.; Zhang, H.; Chan, L.; Liu, C.; Chen, T. Nutritionally Available Selenocysteine Derivative Antagonizes Cisplatin-Induced Toxicity in Renal Epithelial Cells through Inhibition of Reactive Oxygen Species-Mediated Signaling Pathways. J. Agric. Food Chem. 2018, 66, 5860–5870. [Google Scholar] [CrossRef]
- Sengul, E.; Gelen, V.; Yildirim, S.; Tekin, S.; Dag, Y. The Effects of Selenium in Acrylamide-Induced Nephrotoxicity in Rats: Roles of Oxidative Stress, Inflammation, Apoptosis, and DNA Damage. Biol. Trace Elem. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Dong, R.; Yang, Y.; Xie, H.; Huang, Y.; Chen, X.; Wang, D.; Zhang, Z. Protective Effect of Organic Selenium on Oxidative Damage and Inflammatory Reaction of Rabbit Kidney Induced by T-2 Toxin. Biol. Trace Elem. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sanoobar, M.; Eghtesadi, S.; Azimi, A.; Khalili, M.; Khodadadi, B.; Jazayeri, S.; Gohari, M.R.; Aryaeian, N. Coenzyme Q10 supplementation ameliorates inflammatory markers in patients with multiple sclerosis: A double blind, placebo, controlled randomized clinical trial. Nutr. Neurosci. 2014. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Nordman, T.; Olsson, J.M.; Damdimopoulos, A.; Bjorkhem-Bergman, L.; Nalvarte, I.; Eriksson, L.C.; Arner, E.S.; Spyrou, G.; Bjornstedt, M. The mammalian cytosolic selenoenzyme thioredoxin reductase reduces ubiquinone. A novel mechanism for defense against oxidative stress. J. Biol. Chem. 2003, 278, 2141–2146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabbatinelli, J.; Orlando, P.; Galeazzi, R.; Silvestri, S.; Cirilli, I.; Marcheggiani, F.; Dludla, P.V.; Giuliani, A.; Bonfigli, A.R.; Mazzanti, L.; et al. Ubiquinol Ameliorates Endothelial Dysfunction in Subjects with Mild-to-Moderate Dyslipidemia: A Randomized Clinical Trial. Nutrients 2020, 12, 1098. [Google Scholar] [CrossRef] [Green Version]
- Ozer, E.K.; Goktas, M.T.; Kilinc, I.; Pehlivan, S.; Bariskaner, H.; Ugurluoglu, C.; Iskit, A.B. Coenzyme Q10 improves the survival, mesenteric perfusion, organs and vessel functions in septic rats. Biomed. Pharmacother. 2017, 91, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, A.; Keseroglu, B.B.; Koca, G.; Yuceturk, C.N.; Ozgur, B.C.; Surer, H.; Ogus, E.; Yumusak, N.; Karakaya, J.; Korkmaz, M. Scintigraphic evaluation of renoprotective effects of coenzyme Q10 in a rat renal ischemia-reperfusion injury. Nucl. Med. Commun. 2019, 40, 1011–1021. [Google Scholar] [CrossRef] [Green Version]
- Alehagen, U.; Johansson, P.; Bjornstedt, M.; Rosen, A.; Dahlstrom, U. Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and coenzyme Q10 supplementation: A 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Int. J. Cardiol. 2013, 167, 1860–1866. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.; Alehagen, U.; Larsson, A.; Aaseth, J. Selenium in clinical medicine and medical biochemistry. Klin. Biokem. I Nord. 2019, 31, 12–19. [Google Scholar]
- Jensen-Urstad, K.; Bouvier, F.; Hojer, J.; Ruiz, H.; Hulting, J.; Samad, B.; Thorstrand, C.; Jensen-Urstad, M. Comparison of different echocardiographic methods with radionuclide imaging for measuring left ventricular ejection fraction during acute myocardial infarction treated by thrombolytic therapy. Am. J. Cardiol. 1998, 81, 538–544. [Google Scholar] [CrossRef]
- van Royen, N.; Jaffe, C.C.; Krumholz, H.M.; Johnson, K.M.; Lynch, P.J.; Natale, D.; Atkinson, P.; Deman, P.; Wackers, F.J. Comparison and reproducibility of visual echocardiographic and quantitative radionuclide left ventricular ejection fractions. Am. J. Cardiol. 1996, 77, 843–850. [Google Scholar] [CrossRef]
- McFadden, E.C.; Hirst, J.A.; Verbakel, J.Y.; McLellan, J.H.; Hobbs, F.D.R.; Stevens, R.J.; O’Callaghan, C.A.; Lasserson, D.S. Systematic Review and Metaanalysis Comparing the Bias and Accuracy of the Modification of Diet in Renal Disease and Chronic Kidney Disease Epidemiology Collaboration Equations in Community-Based Populations. Clin. Chem. 2018, 64, 475–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willey, J.Z.; Moon, Y.P.; Husain, S.A.; Elkind, M.S.V.; Sacco, R.L.; Wolf, M.; Cheung, K.; Wright, C.B.; Mohan, S. Creatinine versus cystatin C for renal function-based mortality prediction in an elderly cohort: The Northern Manhattan Study. PLoS ONE 2020, 15, e0226509. [Google Scholar] [CrossRef] [PubMed]
- Opotowsky, A.R.; Carazo, M.; Singh, M.N.; Dimopoulos, K.; Cardona-Estrada, D.A.; Elantably, A.; Waikar, S.S.; Mc Causland, F.R.; Veldtman, G.; Grewal, J.; et al. Creatinine versus cystatin C to estimate glomerular filtration rate in adults with congenital heart disease: Results of the Boston Adult Congenital Heart Disease Biobank. Am. Heart J. 2019, 214, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Tighiouart, H.; Greene, T.; Inker, L.A. Measured and estimated glomerular filtration rate: Current status and future directions. Nat. Rev. Nephrol. 2020, 16, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Eckfeldt, J.; Levey, A.S.; Leiendecker-Foster, C.; Rynders, G.; Manzi, J.; Waheed, S.; Coresh, J. Expressing the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) cystatin C equations for estimating GFR with standardized serum cystatin C values. Am. J. Kidney Dis. 2011, 58, 682–684. [Google Scholar] [CrossRef] [Green Version]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Alehagen, U.; Lindahl, T.L.; Aaseth, J.; Svensson, E.; Johansson, P. Levels of sP-selectin and hs-CRP Decrease with Dietary Intervention with Selenium and Coenzyme Q10 Combined: A Secondary Analysis of a Randomized Clinical Trial. PLoS ONE 2015, 10, e0137680. [Google Scholar] [CrossRef]
- Alehagen, U.; Alexander, J.; Aaseth, J.; Larsson, A. Decrease in inflammatory biomarker concentration by intervention with selenium and coenzyme Q10: A subanalysis of osteopontin, osteoprotergerin, TNFr1, TNFr2 and TWEAK. J. Inflamm. (Lond.) 2019, 16, 5. [Google Scholar] [CrossRef] [Green Version]
- Alehagen, U.; Aaseth, J.; Johansson, P. Less increase of copeptin and MR-proADM due to intervention with selenium and coenzyme Q10 combined: Results from a 4-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Biofactors 2015, 41, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Alehagen, U.; Alexander, J.; Aaseth, J.; Larsson, A.; Lindahl, T.L. Significant decrease of von Willebrand factor and plasminogen activator inhibitor-1 by providing supplementation with selenium and coenzyme Q10 to an elderly population with a low selenium status. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alehagen, U.; Johansson, P.; Aaseth, J.; Alexander, J.; Brismar, K. Increase in insulin-like growth factor 1 (IGF-1) and insulin-like growth factor binding protein 1 after supplementation with selenium and coenzyme Q10. A prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. PLoS ONE 2017, 12, e0178614. [Google Scholar] [CrossRef]
- Zhang, J.L.; Xu, B.; Huang, X.D.; Gao, Y.H.; Chen, Y.; Shan, A.S. Selenium Deficiency Affects the mRNA Expression of Inflammatory Factors and Selenoprotein Genes in the Kidneys of Broiler Chicks. Biol. Trace Elem. Res. 2016, 171, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhao, Q.; Zhang, K.; Sun, W.; Jia, X.; Yang, Y.; Yin, J.; Tang, C.; Zhang, J. Se deficiency induces renal pathological changes by regulating selenoprotein expression, disrupting redox balance, and activating inflammation. Metallomics 2020. [Google Scholar] [CrossRef]
- Zachara, B.A.; Salak, A.; Koterska, D.; Manitius, J.; Wasowicz, W. Selenium and glutathione peroxidases in blood of patients with different stages of chronic renal failure. J. Trace Elem. Med. Biol. 2004, 17, 291–299. [Google Scholar] [CrossRef]
- Turunen, M.; Wehlin, L.; Sjoberg, M.; Lundahl, J.; Dallner, G.; Brismar, K.; Sindelar, P.J. beta2-Integrin and lipid modifications indicate a non-antioxidant mechanism for the anti-atherogenic effect of dietary coenzyme Q10. Biochem. Biophys. Res. Commun. 2002, 296, 255–260. [Google Scholar] [CrossRef]
- Persson, M.F.; Franzen, S.; Catrina, S.B.; Dallner, G.; Hansell, P.; Brismar, K.; Palm, F. Coenzyme Q10 prevents GDP-sensitive mitochondrial uncoupling, glomerular hyperfiltration and proteinuria in kidneys from db/db mice as a model of type 2 diabetes. Diabetologia 2012, 55, 1535–1543. [Google Scholar] [CrossRef] [Green Version]
- Fliser, D.; Wiecek, A.; Suleymanlar, G.; Ortiz, A.; Massy, Z.; Lindholm, B.; Martinez-Castelao, A.; Agarwal, R.; Jager, K.J.; Dekker, F.W.; et al. The dysfunctional endothelium in CKD and in cardiovascular disease: Mapping the origin(s) of cardiovascular problems in CKD and of kidney disease in cardiovascular conditions for a research agenda. Kidney Int. Suppl. 2011, 1, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Kopel, T.; Kaufman, J.S.; Hamburg, N.; Sampalis, J.S.; Vita, J.A.; Dember, L.M. Endothelium-Dependent and -Independent Vascular Function in Advanced Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 1588–1594. [Google Scholar] [CrossRef]
- Murthy, V.L.; Naya, M.; Foster, C.R.; Hainer, J.; Gaber, M.; Dorbala, S.; Charytan, D.M.; Blankstein, R.; Di Carli, M.F. Coronary vascular dysfunction and prognosis in patients with chronic kidney disease. JACC Cardiovasc. Imaging 2012, 5, 1025–1034. [Google Scholar] [CrossRef] [Green Version]
- Charytan, D.M.; Skali, H.; Shah, N.R.; Veeranna, V.; Cheezum, M.K.; Taqueti, V.R.; Kato, T.; Bibbo, C.R.; Hainer, J.; Dorbala, S.; et al. Coronary flow reserve is predictive of the risk of cardiovascular death regardless of chronic kidney disease stage. Kidney Int. 2018, 93, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, K.; Fukuda, S.; Shimada, K.; Miyazaki, C.; Otsuka, K.; Kawarabayashi, T.; Watanabe, H.; Yoshikawa, J.; Yoshiyama, M. Prognostic value of coronary flow reserve on long-term cardiovascular outcomes in patients with chronic kidney disease. Am. J. Cardiol. 2013, 112, 928–932. [Google Scholar] [CrossRef] [PubMed]
- Schomburg, L.; Orho-Melander, M.; Struck, J.; Bergmann, A.; Melander, O. Selenoprotein-P Deficiency Predicts Cardiovascular Disease and Death. Nutrients 2019, 11, 1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alehagen, U.; Johansson, P.; Aaseth, J.; Alexander, J.; Surowiec, I.; Lundstedt-Enkel, K.; Lundstedt, T. Significant Changes in Metabolic Profiles after Intervention with Selenium and Coenzyme Q10 in an Elderly Population. Biomolecules 2019, 9, 553. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Active Treatment Group n = 117 | Placebo Group n = 98 | p-Value | |
|---|---|---|---|
| Gender, Males/Females | 58/59 | 44/54 | |
| Age years, mean (SD) | 76.2 (3.1) | 76.2 (3.1) | 0.96 |
| History | |||
| Smoking, n (%) | 8 (6.8) | 9 (9.2) | 0.53 |
| Hypertension, n (%) | 81 (69.2) | 71 (72.4) | 0.61 |
| IHD, n (%) | 22 (18.8) | 16 (16.3) | 0.64 |
| Diabetes, n (%) | 20 (17.1) | 17 (17.3) | 0.96 |
| NYHA class I, n (%) | 72 (61.5) | 57 (58.2) | 0.61 |
| NYHA class II, n (%) | 28 (23.9) | 30 (30.6) | 0.27 |
| NYHA class III, n (%) | 17 (14.5) | 10 (10.2) | 0.34 |
| Unclassified, n (%) | 0 | 1 | - |
| Medications | |||
| Beta blockers, n (%) | 42 (35.9) | 33 (33.7) | 0.73 |
| ACEI/ARB, n (%) | 19 (16.2) | 21 (21.4) | 0.33 |
| Digitalis, n (%) | 5 (4.3) | 1 (1.0) | - |
| Diuretics, n (%) | 37 (31.6) | 33 (33.7) | 0.75 |
| Statins, n (%) | 27 (23.1) | 18 (18.4) | 0.40 |
| Examinations | |||
| EF < 40%, n (%) | 7 (6.0) | 4 (4.1) | - |
| s-selenium pre-intervention µg/L, mean (SD) | 65.0 (17.5) | 65.2 (17.1) | 0.91 |
| s-coenzyme Q10 pre-intervention mg/L, mean (SD) | 0.80 (0.30) | 0.83 (0.34) | 0.65 |
| Variable | Β-Coefficient | Standard Error | T-Value | p-Value |
|---|---|---|---|---|
| Age | 0.25 | 0.03 | 7.16 | <0.0001 |
| Male gender | 0.25 | 0.03 | 7.30 | <0.0001 |
| Smoking | 0.05 | 0.03 | 1.50 | 0.13 |
| Diabetes | 0.02 | 0.03 | 0.73 | 0.46 |
| Hypertension | −0.05 | 0.03 | −1.49 | 0.14 |
| Hb < 120 g/L | 0.03 | 0.003 | 0.97 | 0.33 |
| NYHA III | −0.002 | 0.003 | −0.05 | 0.96 |
| IHD | −0.04 | 0.04 | −1.00 | 0.32 |
| ACEI | 0.05 | 0.03 | 1.59 | 0.11 |
| Beta blockers | 0.04 | 0.03 | 1.03 | 0.30 |
| Selenium, incl. | −0.47 | 0.03 | 14.2 | <0.0001 |
| Effects | Degrees of Freedom | F | p |
|---|---|---|---|
| Intercept | 1 | 0.01 | 0.91 |
| Age | 1 | 0.61 | 0.43 |
| Smoker | 1 | 0.03 | 0.86 |
| Hypertension | 1 | 2.07 | 0.15 |
| Diabetes | 1 | 0.13 | 0.71 |
| IHD | 1 | 1.66 | 0.20 |
| NYHA III | 1 | 0.98 | 0.32 |
| Hb < 120 g/L | 1 | 1.01 | 0.32 |
| s-selenium µg/L, incl | 1 | 1.40 | 0.24 |
| s-creatinine, micromol/L, incl | 1 | 61.28 | <0.0001 |
| Active treatment | 1 | 18.11 | <0.0001 |
| Effects | Degrees of Freedom | F | p |
|---|---|---|---|
| Intercept | 1 | 0.01 | 0.90 |
| Age | 1 | 1.12 | 0.29 |
| Smoker | 1 | 0.05 | 0.29 |
| Hypertension | 1 | 3.70 | 0.06 |
| Diabetes | 1 | 0.19 | 0.66 |
| IHD | 1 | 0.08 | 0.78 |
| NYHA III | 1 | 1.72 | 0.19 |
| Hb < 120 g/L | 1 | 4.33 | 0.04 |
| s-selenium µg/L, incl | 1 | 0.07 | 0.79 |
| s-cystatin-C, mg/L, incl | 1 | 66.65 | <0.0001 |
| Active treatment | 1 | 12.92 | 0.0004 |
| Effects | Degrees of Freedom | F | p |
|---|---|---|---|
| Intercept | 1 | 9.64 | 0.002 |
| Age | 1 | 4.17 | 0.04 |
| Smoker | 1 | 0.05 | 0.83 |
| Hypertension | 1 | 6.97 | 0.009 |
| Diabetes | 1 | 0.01 | 0.92 |
| IHD | 1 | 0.95 | 0.33 |
| NYHA III | 1 | 0.98 | 0.32 |
| Hb < 120 g/L | 1 | 1.52 | 0.22 |
| s-selenium µg/L, incl | 1 | 0.001 | 0.97 |
| CKD-EPI, mL/min/1.73 m2, incl | 1 | 63.88 | <0.0001 |
| Active treatment | 1 | 26.06 | <0.0001 |
| Effects | Degrees of Freedom | F | p |
|---|---|---|---|
| Intercept | 1 | 12.53 | 0.0005 |
| Age | 1 | 4.73 | 0.03 |
| Smoker | 1 | 0.02 | 0.89 |
| Hypertension | 1 | 4.45 | 0.04 |
| Diabetes | 1 | 0.54 | 0.46 |
| IHD | 1 | 2.61 | 0.11 |
| NYHA III | 1 | 0.65 | 0.42 |
| Hb < 120 g/L | 1 | 0.25 | 0.62 |
| s-selenium µg/L, incl | 1 | 1.40 | 0.24 |
| CKD-EPI, mL/min/1.73 m2, incl | 1 | 41.92 | <0.0001 |
| Active treatment | 1 | 20.63 | <0.0001 |
| Effects | Degrees of Freedom | F | p |
|---|---|---|---|
| Intercept | 1 | 6.69 | 0.01 |
| Age | 1 | 2.99 | 0.09 |
| Smoker | 1 | 0.20 | 0.65 |
| Hypertension | 1 | 5.31 | 0.02 |
| Diabetes | 1 | 0.27 | 0.61 |
| IHD | 1 | 0.09 | 0.76 |
| NYHA III | 1 | 1.05 | 0.31 |
| Hb < 120 g/L | 1 | 4.44 | 0.04 |
| s-selenium µg/L, incl | 1 | 0.31 | 0.58 |
| CKD-EPI, mL/min/1.73 m2, incl | 1 | 76.43 | <0.0001 |
| Active treatment | 1 | 12.88 | 0.0004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alehagen, U.; Aaseth, J.; Alexander, J.; Brismar, K.; Larsson, A. Selenium and Coenzyme Q10 Supplementation Improves Renal Function in Elderly Deficient in Selenium: Observational Results and Results from a Subgroup Analysis of a Prospective Randomised Double-Blind Placebo-Controlled Trial. Nutrients 2020, 12, 3780. https://doi.org/10.3390/nu12123780
Alehagen U, Aaseth J, Alexander J, Brismar K, Larsson A. Selenium and Coenzyme Q10 Supplementation Improves Renal Function in Elderly Deficient in Selenium: Observational Results and Results from a Subgroup Analysis of a Prospective Randomised Double-Blind Placebo-Controlled Trial. Nutrients. 2020; 12(12):3780. https://doi.org/10.3390/nu12123780
Chicago/Turabian StyleAlehagen, Urban, Jan Aaseth, Jan Alexander, Kerstin Brismar, and Anders Larsson. 2020. "Selenium and Coenzyme Q10 Supplementation Improves Renal Function in Elderly Deficient in Selenium: Observational Results and Results from a Subgroup Analysis of a Prospective Randomised Double-Blind Placebo-Controlled Trial" Nutrients 12, no. 12: 3780. https://doi.org/10.3390/nu12123780