Hydrolyzed Rice Protein-Based Formulas, a Vegetal Alternative in Cow’s Milk Allergy


 , and
, and
Abstract
:1. Introduction
2. Cow’s Milk Protein Allergy (CMPA) and Its Nutritional Hazards
2.1. Height and Weight Problem
2.2. Micronutrients and Macronutrients Deficiency
2.3. Feeding Difficulties
2.4. The Need for a Precise Dietary Follow-Up
3. Plant Proteins in Infant Nutrition
3.1. Protein and Amino Acid Requirements and Reference Patterns for Infants
3.2. Nutritional Quality of Plant Proteins for Infants
3.3. Manufacturing Hydrolyzed Rice Proteins
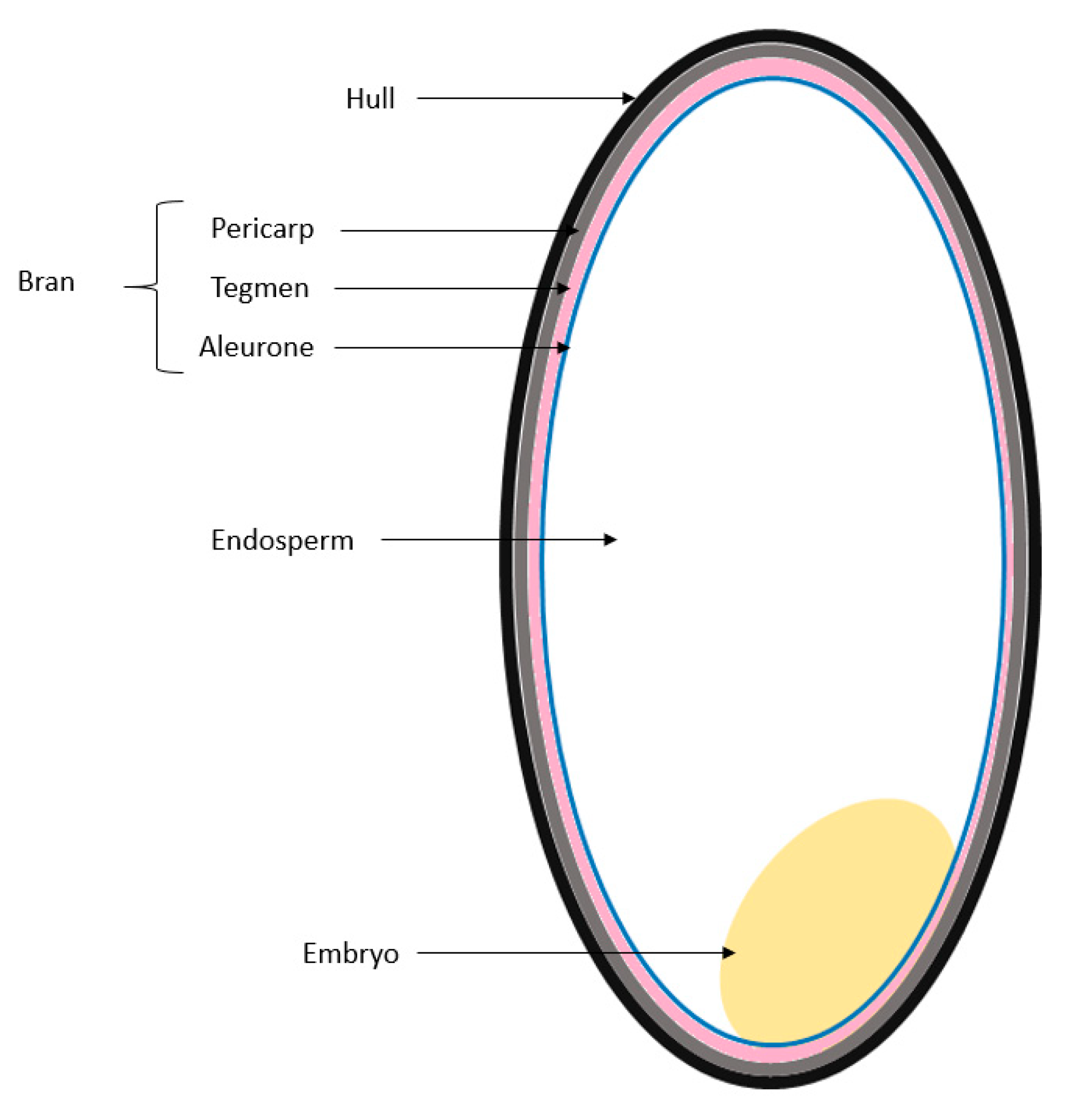
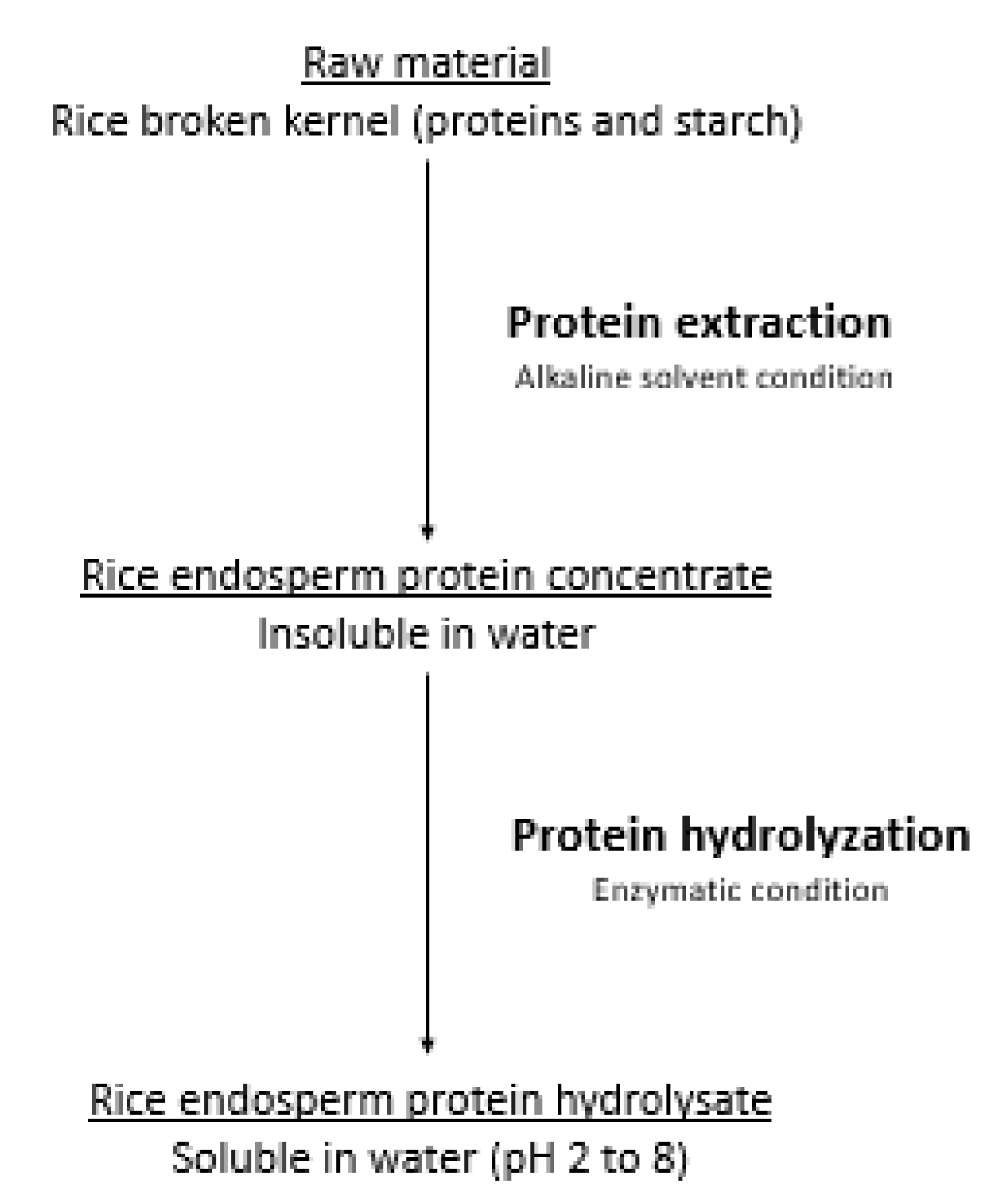
3.3.1. Extraction
3.3.2. Hydrolyzation
4. The Development of Hydrolyzed Rice Protein Formulas (HRPF) during CMPA
4.1. Legal Framework
4.2. HRPF Market Availability
4.3. HRPF’s Occupancy in the CMPA Market
5. Nutritional Properties of HRPFs
5.1. Energy, Protein, Lipid, and Carbohydrate Content of HRPF
5.2. Nutritional Efficiency of HRPFs
5.3. Acceptability and Palatability of HRPFs
5.4. Digestive Tolerance of HRPFs
5.5. Allergenic Tolerance of Rice and of HRPFs
6. HRPFs in the Treatment of CMPA
6.1. Allergenic Efficiency of HRPFs in CMPA
6.2. Nutritional Efficiency of HRPF in CMPA
6.2.1. Growth evolution and protein nutritional status
6.2.2. Bone mineralization
6.3. Efficiency of HRPF in the Acquisition of Tolerance
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AAF | amino acid formula |
| BMI | body mass index |
| BMD | bone mineral density |
| CMP | cow’s milk protein |
| CMPA | cow’s milk protein allergy |
| CMP-eHF | cow’s milk protein-based extensively hydrolyzed formula |
| DBPCFC | double-blind placebo-controlled food challenge |
| DIAAS | Digestible Indispensable Amino Acid Score |
| EoE | eosinophilic esophagitis |
| ESPGHAN | European Society for Paediatric Gastroenterology Hepatology and Nutrition |
| FA | food allergy |
| FSMP | food for specific medical purpose |
| HRP | hydrolyzed rice protein |
| HRPF | hydrolyzed rice protein formula |
| IAA | indispensable amino acids |
| MW | molecular weight |
| NPR | net protein retention |
| NPU | net protein utilization |
| OFC | oral food challenge |
| PDCAAS | Protein Digestibility-Corrected Amino Acid Score |
| PER | protein efficiency ratio |
| RAST | radioallergosorbent test |
| RANKL | receptor activator of nuclear factor kB ligand level |
| SF | standard formula |
| SPT | skin prick test |
| WHO | World Health Organization |
References
- Schoemaker, A.A.; Sprikkelman, A.B.; Grimshaw, K.E.; Roberts, G.; Grabenhenrich, L.; Rosenfeld, L.; Siegert, S.; Dubakiene, R.; Rudzeviciene, O.; Reche, M.; et al. Incidence and natural history of challenge-proven cow’s milk allergy in European children—Euro-Prevall birth cohort. Allergy 2015, 70, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Meyer, R. Nutritional disorders resulting from food allergy in children. Pediatr. Allergy Immunol. 2018, 29, 689–704. [Google Scholar] [CrossRef]
- Bocquet, A.; Dupont, C.; Chouraqui, J.P.; Darmaun, D.; Feillet, F.; Frelut, M.L.; Girardet, J.P.; Hankard, R.; Lapillonne, A.; Committee on Nutrition of the French Society of Pediatrics (CNSFP); et al. Efficacy and safety of hydrolyzed rice-protein formulas for the treatment of cow’s milk protein allergy. Arch. Pediatr. 2019, 26, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Willett, M.D.; David, S.; Ludwig, M.D. Milk and health. N. Engl. J. Med. 2020, 382, 644–654. [Google Scholar]
- Dupont, C.; Chouraqui, J.P.; de Boissieu, D.; Bocquet, A.; Bresson, J.L.; Briend, A.; Darmaun, D.; Frelut, M.L.; Ghisolfi, J.; Girardet, J.P.; et al. Dietary treatment of cow’s milk protein allergy in childhood: A commentary by the committee on nutrition of the french society of paediatrics. Br. J. Nutr. 2012, 107, 325–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isolauri, E.; Sutas, Y.; Salo, M.K.; Isosomppi, R.; Kaila, M. Elimination diet in cow’s milk allergy: Risk for impaired growth in young children. J. Pediatr. 1998, 132, 1004–1009. [Google Scholar] [CrossRef]
- Robbins, K.A.; Wood, R.A.; Keet, C.A. Milk allergy is associated with decreased growth in US children. J. Allergy Clin. Immunol. 2014, 134, 1466–1468. [Google Scholar] [CrossRef] [Green Version]
- Dupont, C.; Chouraqui, J.P.; Linglart, A.; Bocquet, A.; Darmaun, D.; Feillet, F.; Frelut, M.L.; Girardet, J.P.; Hankard, R.; Rozé, J.C.; et al. Committee on nutrition of the French society of pediatrics. Nutritional management of cow’s milk allergy in chidren: An update. Arch. Pediatr. 2018, 25, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Venter, C.; Mazzocchi, A.; Maslin, K.; Agostoni, C. Impact of elimination diets on nutrition and growth in children with multiple food allergies. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 220–226. [Google Scholar] [CrossRef]
- Pavić, I.; Kolaček, S. Growth of children with food allergy. Horm. Res. Paediatr. 2017, 88, 91–100. [Google Scholar] [CrossRef]
- Meyer, R.; Groetch, M.; Venter, C. When should infants with cow’s milk protein allergy use an amino acid formula? A practical guide. J. Allergy Clin. Immunol. Pract. 2018, 6, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Flammarion, S.; Santos, C.; Guimber, D.; Jouannic, L.; Thumerelle, C.; Gottrand, F.; Deschildre, A. Diet and nutritional status of children with food allergies. Pediatr. Allergy Immunol. 2011, 22, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Sova, C.; Feuling, M.B.; Baumler, M.; Gleason, L.; Tam, J.S.; Zafra, H.; Goday, P.S. Systematic review of nutrient intake and growth in children with multiple IgE-mediated food allergies. Nutr. Clin. Pract. 2013, 28, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Christie, L.; Hine, R.J.; Parker, J.G.; Burks, W. Food allergies in children affect nutrient intake and growth. J. Am. Diet. Assoc. 2002, 102, 1648–1651. [Google Scholar] [CrossRef]
- Maslin, K.; Grimshaw, K.; Oliver, E.; Roberts, G.; Arshad, S.H.; Dean, T.; Grundy, J.; Glasbey, G.; Venter, C. Taste preference, food neophobia and nutritional intake in children consuming a cow’s milk exclusion diet: A prospective study. J. Hum. Nutr. Diet. 2016, 29, 786–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mailhot, G.; Perrone, V.; Alos, N.; Dubois, J.; Delvin, E.; Paradis, L.; Des Roches, A. Cow’s milk allergy and bone mineral density in prepubertal children. Pediatrics 2016, 137, e20151742. [Google Scholar] [CrossRef] [Green Version]
- Ambroszkiewicz, J.; Rowicka, G.; Chelchowska, M.; Gajewska, J.; Strucińska, M.; Laskowska-Klita, T. Biochemical markers of bone metabolism in children with cow’s milk allergy. Arch. Med. Sci. 2014, 10, 1135–1141. [Google Scholar] [CrossRef]
- Auestad, N.; Hurley, J.S.; Fulgoni, V.L., 3rd; Schweitzer, C.M. Contribution of food groups to energy and nutrient intakes in five developed countries. Nutrients 2015, 7, 4593–4618. [Google Scholar] [CrossRef]
- Grimes, C.A.; Szymlek-Gay, E.A.; Campbell, K.J.; Nicklas, T.A. Food sources of total energy and nutrients among U.S. infants and toddlers: National health and nutrition examination survey 2005–2012. Nutrients 2015, 7, 6797–6836. [Google Scholar] [CrossRef] [Green Version]
- Rizzoli, R.; Bianchi, M.L.; Garabédian, M.; McKay, H.A.; Moreno, L.A. Maximizing bone mineral mass gain during growth for the prevention of fractures in the adolescents and the elderly. Bone 2010, 46, 294–305. [Google Scholar] [CrossRef]
- Berni, C.R.; Leone, L.; D’Auria, E.; Riva, E.; Nocerino, R.; Ruotolo, S.; Terrin, G.; Cosenza, L.; Di Costanzo, M.; Passariello, A.; et al. The effects of dietary counseling on children with food allergy: A prospective, multicenter intervention study. J. Acad. Nutr. Diet. 2014, 114, 1432–1439. [Google Scholar] [CrossRef] [PubMed]
- Maslin, K.; Grundy, J.; Glasbey, G.; Dean, T.; Arshad, S.H.; Grimshaw, K.; Oliver, E.; Roberts, G.; Venter, C. Cow’s milk exclusion diet during infancy: Is there a long-term effect on children’s eating behavior and food preferences? Pediatr. Allergy Immunol. 2016, 27, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukkada, V.A.; Haas, A.; Greskoff, M.N.; Capocelli, K.E.; Henry, M.; Gilman, N.; Petersburg, S.; Moore, W.; Lovell, M.A.; Fleischer, D.M.; et al. Feeding dysfunction in children with eosinophilic gastrointestinal diseases. Pediatrics 2011, 126, 672–677. [Google Scholar] [CrossRef] [Green Version]
- Berry, M.J.; Adams, J.; Voutilainen, H.; Feustel, P.J.; Celestin, J.; Järvinen, K.M. Impact of elimination diets on growth and nutritional status in children with multiple food allergies. Pediatr. Allergy Immunol. 2015, 26, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Mehta, H.; Ramesh, M.; Feuille, E.; Groetch, M.; Wang, J. Growth comparison in children with and without food allergies in 2 different demographic populations. J. Pediatr. 2014, 165, 842–848. [Google Scholar] [CrossRef]
- Rosendahl, J.; Fogelholm, M.; Pelkonen, A.; Mäkelä, M.J.; Mäkitie, O.; Erkkola, M. A history of cow’s milk allergy is associated with lower vitamin D status in schoolchildren. Horm. Res. Paediatr. 2017, 88, 244–250. [Google Scholar] [CrossRef]
- WHO/FAO/UNU Expert Consultation. Protein and Amino Acid Requirements in Human Nutrition. Report of a Joint WHO/FAO/UNU Expert Consultation; Paper No 935; WHO Technical Report Series: Geneva, Switzerland, 2007. [Google Scholar]
- Tome, D. Criteria and markers for protein quality assessment—A review. Br. J. Nutr. 2012, 108, S222–S229. [Google Scholar] [CrossRef] [Green Version]
- FAO/WHO. Protein Quality Evaluation: Report of the Joint FAO/WHO Expert Consultation, FAO Food and Nutrition; Paper No. 51; FAO: Rome, Italy, 1991. [Google Scholar]
- FAO. Dietary Protein Quality Evaluation in Human Nutrition: Report of an FAO Expert Consultation, FAO Food and Nutrition; Paper No. 92; FAO: Rome, Italy, 2013. [Google Scholar]
- FAO. Research Approaches and Methods for Evaluating the Protein Quality of Human Foods. Report of a FAO Expert Working Group; FAO: Rome, Italy, 2014. [Google Scholar]
- FAO. Protein Quality Assessment in Follow-Up Formula for Young Children and Ready to Use Therapeutic Foods; FAO: Rome, Italy, 2018; p. 50. [Google Scholar]
- Young, V.R.; Pellett, P.L. Plant proteins in relation to human protein and amino acid nutrition. Am. J. Clin. Nutr. 1994, 59, 1203S–1212S. [Google Scholar] [CrossRef]
- Van Vliet, S.; Burd, N.A.; Van Loon, L.J. The skeletal muscle anabolic response to plant-versus animal-based protein consumption. J. Nutr. 2015, 145, 1981–1991. [Google Scholar] [CrossRef] [Green Version]
- Bos, C.; Juillet, B.; Fouillet, H.; Turlan, L.; Daré, S.; Luengo, C.; N’tounda, R.; Benamouzig, R.; Gausserès, N.; Tomé, D.; et al. Postprandial metabolic utilization of wheat protein in humans. Am. J. Clin. Nutr. 2005, 81, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Gaudichon, C.; Bos, C.; Morens, C.; Petzke, K.J.; Mariotti, F.; Everwand, J.; Benamouzig, R.; Dare, S.; Tomé, D.; Metges, C.C. Ileal losses of nitrogen and amino acids in humans and their importance to the assessment of amino acid requirements. Gastroenterology 2002, 123, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Gilani, G.S.; Xiao, C.W.; Cockell, K.A. Impact of antinutritional factors in food proteins on the digestibility of protein and the bioavailability of amino acids and on protein quality. Br. J. Nutr. 2012, 108, S315–S332. [Google Scholar] [CrossRef]
- Juliano, B.O. Starch: Chemistry and Technology; Whistler, R.L., BeMiller, J.N., Paschall, E.F., Eds.; Academic Press: Orlando, FL, USA, 1984; pp. 507–528. [Google Scholar]
- Champagne, E.T.; Wood, D.F.; Juliano, B.O.; Bechtel, D.B. The rice grain and its gross composition. In Rice: Chemistry and Technology, 3rd ed.; American Association of Cereal Chemists: St. Paul, MN, USA, 2004; pp. 77–107. [Google Scholar]
- Osborn, T.B. The Vegetable Proteins; Longmans, Green and Co.: London, UK, 1924. [Google Scholar]
- Amagliani, L.; O’Regan, J.; Kelly, A.L.; O’Mahony, J.A. The composition, extraction, functionality and applications of rice proteins: A review. Trends Food Sci. Technol. 2017, 64, 1–12. [Google Scholar] [CrossRef]
- Champagne, E.T. (Ed.) Rice bran and oil. In Rice: Chemistry and Technology, 3rd ed.; American Association of Cereal Chemists: St. Paul, MN, USA, 2004; pp. 732–781. [Google Scholar]
- Han, S.W.; Chee, K.M.; Cho, S.J. Nutritional quality of rice bran protein in comparison to animal and vegetable protein. Food Chem. 2015, 172, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Shih, F.F. An update on the processing of high-protein rice products. Nahrung/Food 2003, 47, 420–424. [Google Scholar] [CrossRef]
- Khan, S.H.; Butt, M.S.; Sharif, M.K.; Sameen, A.; Mumtaz, S.; Sultan, M.T. Functional properties of protein isolates extracted from stabilized rice bran by microwave, dry heat and parboiling. J. Agric. Food Chem. 2011, 59, 2416–2420. [Google Scholar] [CrossRef]
- Lakkakula, N.R.; Lima, M.; Walker, T. Rice bran stabilization and rice bran oil extraction using hmic heating. Bioresour. Technol. 2004, 92, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Tanaka, K.; Kasai, Z. Molecular species in the protein body II (PB-II) of developing rice endosperm. Agric. Biol. Chem. 1986, 50, 3031–3035. [Google Scholar]
- Tecson, E.M.S.; Esmama, B.V.; Lontok, L.P.; Juliano, B.O. Studies on the extraction and composition of rice endosperm glutelin and prolamin. Cereal Chem. 1971, 48, 168–181. [Google Scholar]
- Otterburn, M.S. Protein crosslinking. In Protein Quality and the Effects of Processing; Phillips, R.D., Finley, J.W., Eds.; Marcel Dekker: New York, NY, USA, 1989. [Google Scholar]
- Wang, M.; Hettiarachchy, N.S.; Qi, M.; Burks, W.; Siebenmorgen, T. Preparation and functional properties of rice bran protein isolate. J. Agric. Food Chem. 1999, 47, 411–416. [Google Scholar] [CrossRef]
- Kubota, M.; Saito, Y.; Masamura, T.; Kumagai, T.; Watanabe, R.; Fujimura, S.; Kumagai, T.; Watanabe, R.; Fujimura, S.; Kadowaki, M. Improvement in the in vivo digestibility of rice protein by alkali extraction is due to structural changes in prolamin/protein body-I particle. Biosci. Biotechnol. Biochem. 2010, 74, 614–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumagai, T.; Watanabe, R.; Saito, M.; Watanabe, T.; Kubota, M.; Kadowaki, M. Superiority of alkali-extracted rice protein in bioavailability to starch degraded rice protein comes from digestion of prolamin in growing rats. J. Nutr. Sci. Vitaminol. 2009, 55, 170–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amagliani, L.; O’Reganb, J.; Schmittc, C.; Kellya, K.L.; O’Mahonya, J.A. Characterisation of the physicochemical properties of intact and hydrolysed rice protein ingredients. J. Cereal Sci. 2019, 88, 16–23. [Google Scholar] [CrossRef]
- Directive 2013/46/UE de la Commission du 28 Août 2013 Modifiant la Directive 2006/141/CE en ce qui Concerne les Exigences en Matière de Protéines Pour les Préparations Pour Nourrissons et les Préparations de suite. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2013:230:0016:0019:FR:PDF (accessed on 21 January 2020).
- Hojsak, I.; Kljaić-Turkalj, M.; Misak, Z.; Kolacek, S. Rice protein-induced enterocolitis syndrome. Clin. Nutr. 2006, 25, 533–536. [Google Scholar] [CrossRef]
- Commission Regulation (EU) 2015/1006 of 25 June 2015 Amending Regulation (EC) No 1881/2006 as Regards Maximum Levels of Inorganic Arsenic in Foodstuffs. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ:JOL_2015_161_R_0006 (accessed on 25 August 2018).
- Lasekan, J.B.; Koo, W.K.; Walters, J.; Neylan, M.; Luebbers, S. Growth, tolerance and biochemical measures in healthy infants fed a partially hydrolyzed rice protein-based formula: A randomized, blinded, prospective trial. J. Am. Coll. Nutr. 2006, 25, 12–19. [Google Scholar] [CrossRef]
- Commission Directive 2006/141/EC of 22 December 2006 on Infant Formulae and Follow-on Formulae and Amending Directive 1999/21/EC. Annexe 4. Official Journal of the European Union of 30 December 2006. L. 401/1. Available online: https://op.europa.eu/en/publication-detail/-/publication/567a62e1-1843-4b5c-908c-998cd61f228c/language-en (accessed on 29 August 2020).
- Anonymous. American Academy of Pediatrics, Committee on Nutrition. Hypoallergenic infant formulas. Pediatrics 2000, 106, 346–349. [Google Scholar] [CrossRef] [Green Version]
- IQVIA Pharmacy. Available online: https://www.iqvia.com/our-customers/pharmacies-and-wholesalers (accessed on 21 January 2020).
- Fiocchi, A.; Dahda, L.; Dupont, C.; Campoy, C.; Fierro, V.; Nieto, A. Cow’s milk allergy: Towards an update of DRACMA guidelines. World Allergy Organ. J. 2016, 9, 35. [Google Scholar] [CrossRef] [Green Version]
- Fiocchi, A.; Dahdah, L.; Albarini, M.; Martelli, A. Cow’s milk allergy in children and adults. Chem. Immunol. Allergy 2015, 101, 114–123. [Google Scholar]
- Miraglia del, G.M.; D’Auria, E.; Peroni, D. Flavor, relative palatability and components of cow’s milk hydrolysed formulas and amino acid-based formula. Ital. J. Pediatr. 2015, 41, 42. [Google Scholar] [CrossRef] [Green Version]
- Fiocchi, A.; Restani, P.; Bernardini, R.; Lucarelli, S.; Lombardi, G.; Magazzù, G.; Marseglia, G.L.; Pittschieler, K.; Tripodi, S.; Troncone, R.; et al. A hydrolysed rice-based formula is tolerated by children with cow’s milk allergy: A multi-centre study. Clin. Exp. Allergy 2006, 36, 311–316. [Google Scholar] [CrossRef]
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.M.; et al. European Society of Pediatric Gastroenterology, Hepatology, and Nutrition; Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Savino, F.; Castagno, E.; Monti, G.; Serraino, P.; Peltran, A.; Oggero, R.; Fanaro, S.; Vigi, V.; Silvestro, L. Z-score of weight for age of infants with atopic dermatitis and cow’s milk allergy ed with a rice-hydrolysate formula during the first two years of life. Acta Pediatr. 2005, 94, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Reche, M.; Pascual, C.; Fiandor, A.; Polanco, I.; Rivero-Urgell, M.; Chifre, R.; Johnston, S.; Martín-Esteban, M. The effect of a partially hydrolysed formula based on rice protein in the treatment of Infants with cow’s milk protein allergy. Pediatr. Allergy Immunol. 2010, 21, 577–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenplas, Y.; Greef de, E.; Hauser, B. Paradice study group. Safety and tolerance of a new extensively hydrolyzed rice protein-based formula in the management of infants with cow’s milk protein allergy. Eur. J. Pediatr. 2014, 173, 1209–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Energy and Protein Requirements. Report of a Joint FAO/WHO/UNU Expert Consultation; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 1985; Available online: http://www.fao.org/3/aa040e/AA040E08.htm (accessed on 21 January 2020).
- Association française de pédiatrie ambulatoire. Composition Des Laits Pour Nourrissons Et Enfants En Bas Age: AFPA. 2018. Available online: www.laits.fr (accessed on 25 August 2018).
- United States Department of Agriculture. National Nutrient Database for Standard Reference Release 28; United States Department of Agriculture: Washington, DC, USA, 2016. Available online: https://data.nal.usda.gov/system/files/sr28_doc.pdf (accessed on 21 January 2020).
- European Food Safety Authority Panel on Dietetic Products, Nutrition Allergies (NDA). Scientific opinion on dietary reference values for protein. EFSA J. 2012, 10, 2557. [Google Scholar] [CrossRef]
- Koo, W.W.; Lasekan, J.B. Rice protein-based infant formula: Current status and future development. Minerva Pediatr. 2007, 59, 35–41. [Google Scholar]
- Girardet, J.P.; Rivero, M.; Orbegozo, J.; David, T.; Boulanger, S.; Moisson de Vaux, A.; Johnston, S.; Marin, V. Tolérance d’une formule infantile de protéines de riz hydrolysées. Arch. Pediatr. 2010, 17, 90. [Google Scholar] [CrossRef]
- World Health Organization. Child Growth Standards; World Health Organization: Albany, NY, USA, 2020; Available online: http://www.who.int/childgrowth/en/ (accessed on 21 January 2020).
- D’Auria, E.; Sala, M.; Lodi, F.; Radaelli, G.; Riva, E.; Giovannini, M. Nutritional value of a rice-hydrolysate formula in infants with cow’s milk protein allergy: A randomized pilot study. J. Int. Med. Res. 2003, 31, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Fiocchi, A.; Travaini, M.; D’Auria, E.; Banderali, G.; Bernardo, L.; Riva, E. Tolerance to a rice hydrolysate formula in children allergic to cow’s milk and soy. Clin. Exp. Allergy 2003, 33, 1576–1580. [Google Scholar] [CrossRef]
- Medjad, G.N.; Henocq, A.; Arnaud, B.F. Does the hydrolysis of proteins change the acceptability and the digestive tolerance of milk for infants? The results of a comparative and randomized prospective study. Ann. Pediatr. 1992, 39, 202–206. [Google Scholar]
- Pedrosa, M.; Pascual, C.Y.; Larco, J.L.; & Esteban, M.M. Palatability of hydrolysates and other substitution formulas for cow’s milk-allergic children: A comparative study of taste, smell, and texture evaluated by healthy volunteers. J. lnvestig. Allergol. Clin. Immunol. 2006, 16, 351–356. [Google Scholar]
- Lombardo, G.; Barberio, G.; Pajno, G.B.; La Rosa, M.; Barberi, I. Nutritional adequacy of cow’s milk substitutes. Allergy 1998, 53, 118–121. [Google Scholar] [CrossRef]
- Gray, H.C.; Foy, T.M.; Becker, B.A.; Knutsen, A.P. Rice-induced enterocolitis in an infant: TH1/TH2 cellular hypersensitivity and absent IgE reactivity. Ann. Allergy Asthma. Immunol. 2004, 93, 601–605. [Google Scholar] [CrossRef]
- Helm, R.M.; Burks, A.W. Hypoallergenicity of rice protein. Cereal Foods World 1996, 41, 839–843. [Google Scholar]
- Mehr, S.; Kakakios, A.; Frith, K.; Kemp, A.S. Food protein-induced enterocolitis syndrome: 16 years experience. Pediatrics 2009, 123, 459–464. [Google Scholar] [CrossRef]
- Mehr, S.S.; Kakakios, A.M.; Kemp, A.S. Rice: A common and severe cause of food protein-induced enterocolitis syndrome. Arch. Dis. Child. 2009, 94, 220–223. [Google Scholar] [CrossRef]
- Piacentini, G.L.; Vicentini, L.; Bodini, A.; Mazzi, P.; Peroni, D.G.; Maffeis, C.; Boner, A.L. Allergenicity of a hydrolyzed rice infant formula in a guinea pig model. Ann. Allergy Asthma Immunol. 2003, 91, 61–64. [Google Scholar] [CrossRef]
- Berni, C.R.; Nocerino, R.; Terrin, G. Formula selection for management of children with cow milk allergy influences the rate of acquisition of tolerance: A prospective multicenter study. Pediatrics 2013, 163, 771–777. [Google Scholar] [CrossRef]
- Agostoni, C.; Fiocchi, A.; Riva, E.; Terracciano, L.; Sarratud, T.; Martelli, A.; Lodi, F.; D’Auria, E.; Zuccotti, G.; Giovannini, M. Growth of infants with IgE-mediated cow’s milk allergy fed different formulas in the complementary feeding period. Pediatr. Allergy Immunol. 2007, 11, 1–8. [Google Scholar] [CrossRef]
- Terracciano, L.; Bouygue, G.R.; Veglia, F.; Veglia, F.; Martelli, A.; Fiocchi, A. Impact of dietary regimen on the duration of cows’ milk allergy: A random allocation study. Clin. Exp. Allergy 2010, 40, 637–642. [Google Scholar]



{kind=link}
{kind=link}
| Average Protein Requirement | IAA Reference Pattern (mg/g Protein) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| g/kg/day | His | Ile | Leu | Lys | SAA | AAA | Thr | Trp | Val | |
| Human milk | - | 21 | 55 | 96 | 69 | 33 | 94 | 44 | 17 | 55 |
| 1–2.9 years | 0.86 | 18 | 31 | 63 | 52 | 26 | 46 | 27 | 7.4 | 42 |
| Adult | 0.66 | 15 | 30 | 59 | 45 | 22 | 38 | 23 | 6 | 39 |
| Protein Source | First Limiting IAA | Protein Digestibility % | PDCAAS | ||
|---|---|---|---|---|---|
| Adult | 1–3 Years | Human Milk | |||
| Soja | SAA | 75–90 | 0.8–1.0 | 0.7–0.8 | 0.6–0.7 |
| Pea | SAA | 75–90 | 0.8–0.9 | 0.7–0.8 | 0.6–0.7 |
| Chickpea | SAA | 75–85 | 0.8–0.9 | 0.6–0.7 | 0.5–0.6 |
| Lupine | valine | 85–90 | 0.8–0.9 | 0.7–0.8 | 0.6–0.7 |
| Lentil | SAA | 75–80 | 0.6–0.7 | 0.5–0.6 | 0.4–0.5 |
| Peanut | Lysine | 85–90 | 0.6–0.7 | 0.5–0.6 | 0.4–0.5 |
| Wheat | Lysine | 75–85 | 0.4–0.6 | 0.3–0.5 | 0.2–0.3 |
| Rice | Lysine | 75–85 | 0.5–0.7 | 0.4–0.6 | 0.3–0.5 |
| Formula | Energy/100 mL | Proteins/100 mL | Peptides Molecular Weight (MW) | Addition of Free Amino-Acids | Lipids | Carbohydrates/100 mL | |||
|---|---|---|---|---|---|---|---|---|---|
| Lysin | Threonine | Tryptophan | |||||||
| Risolac® 0–3 years [66] | 69 kcal | 2.1 g | 44%: MW < 1000 Da 43%: 1000 Da < MW < 2000 Da 13%: 2000 Da < MW < 4000 Da | Yes | Yes | Yes | Similar to standard formulas | Lactose free | Dextrin-maltose: 5.3 g Corn Starch: 0.5 g Glucose + saccharose syrup: 1.5 g |
| Blemil Arroz 1® Modilac Expert Riz 1® [67] | 71 kcal | 1.7 g | 10%: Free amino acids 26.8%: MW < 300 Da 29.9%: 300 Da < MW < 1000 Da 35.2%: 1000 Da < MW < 5000 Da | Yes | Yes | Yes | Dextrin-maltose: 6 g Corn Starch: 1.6 g | ||
| Blemil Arroz 2® Modilac Expert Riz 2® [67] | 69 kcal | 2 g | Yes | No | Yes | Dextrin-maltose: 6.4 g Corn Starch: 1.7 g | |||
| Novalac® 0–3 years [68] | 68 kcal | 1.8 g | 95%: MW < 1000 Da | Yes | No | Yes | Dextrin-maltose: 5.7 g Corn Starch: 1.9g | ||
| Ross Formula [57] | 68 kcal | 1.9 g | Unknown | Yes | Yes | No | 40% rice syrup + 60% saccharose syrup: 6.7 g | ||
| Study | Patients | Type of Study | Intervention | Outcomes |
|---|---|---|---|---|
| Lasekan et al., 2006 [57] | 65 healthy infants (without CMPA) Age: 0 to 16 weeks | Randomized double-blind trial | HRPF (Ross formula) or standard formula for 4 months | Height, weight, BMI, and cranial girth within normal limits No difference between groups |
| Girardet et al., 2010 [74] | 78 healthy full-term infants Age: <1 month | Open multicenter prospective study | Lactose-containing HRPF (Modilac®) from the 1st month to the age of 4 to 6 months (after starting complementary feeding) | Average daily weight gain: 23.2 ± 4.3 g (PP population), with no difference with WHO standards [75] Height, weight, and BMI z-scores (intent to treat population): between 1.1 and −0.5 DS during the study period |
| Study | Patients | Type of Study | Study Duration | Intervention | Outcomes |
|---|---|---|---|---|---|
| Fiocchi et al., 2003 [77] | 18 infants CMPA confirmed by a double-blind placebo-controlled food challenge (DBPCFC) Age: 1–9 years (average 5 years) | Clinical trial | 1 test | HRPF (Risolac®) | Skin Prick Test: CMP: positive in all children Soy: positive in all children Rice: positive for 8/18 children HRPF: positive for 2/18 children Specific IgEs: CMP: positive in all children Soy: positive in 13/18 children Rice: positive in 7/18 children HRPF: permanently negative Double-blind placebo-controlled food challenge (DBPCFC) with HRPF: negative in all cases |
| Fiocchi et al., 2006 [69] | 100 infants CMPA confirmed by DBPCFC Age: 3.2 ± 2.93 years | Prospective study | 1 test | HRPF (Risolac®) | Skin Prick Test: Cow’s milk and/or CMP fraction: positive in 87/99 children Rice: positive in 4/90 children HRPF: positive in 4/86 children Specific IgEs > 0.35 KU/L: Cow’s milk and/or for a CMP fraction: in 92/95 children Rice: in 21/91 children HRP: in 4/91 children Rice specific IgEs: Rice: positive in 21/91 children (Pharmacia—Upjohn Diagnostic) and in 70/96 children (immunotransfer) HRPF: weakly positive in 6 children DBPCFC with HRPF was always negative. |
| Reche et al., 2010 [67] | 92 infants CMPA IgE-mediated confirmed by a positive Oral Food Challenge (OFC) Age: average 4.3 months (1.1 to 10) | Prospective, open and randomized clinical trial | 2 years | 46 fed a HRPF (Blemil Arroz®/Modilac Expert Riz 1®) 46 fed a CMP-eHF | HRPF: well tolerated in all children CMP-eHF: 1 child developed allergy to this -CMP-eHF Evolution of number of children remaining allergic: similar in both groups. |
| Vandenplas et al., 2014 [68] | 40 infants CMPA confirmed by OFC CMPA IgE-mediated or not Age: average 3.4 month (1 to 6) | Prospective trial | 6 months | HRPF (Novalac Riz®) | Significant decrease of the allergy symptoms after 1 month Benefit confirmed after 3 and 6 months Clinical tolerance was assessed with the symptom-based score (SBS) [81], now published as the COMISS score [82,83] |
| Study | Patients | Type of Study | Height and Weight z-Scores at Inclusion | Intervention | Outcomes |
|---|---|---|---|---|---|
| D’Auria et al. 2003 [76] | 16 infants CMPA + atopic dermatitis (DBPCFC or an open OFC or an open test) Age: 6–14 months | Observation | Weight: HRPF: −0.30 (−0.34) Soy formula: −0.21 (−0.14) Height: HRPF: −0.10 (−0.21) Soy formula: −0.12 (−0.23) | HRPF or soy formula | Weight: HRPF: 0.09 (−0.08). Soy formula: 0.11 (0.15). Height: HRPF: 0.07 (0.12) Soy formula: 0.27 (0.37). Protein nutritional status: Blood markers of protein homeostasis (albumin, pre-albumin, total plasma proteins, urea): similar in both groups |
| Savino et al., 2005 [66] | 58 infants CMPA + atopic dermatitis 30 controls (without CMPA) Age: 1–24 months | Prospective, non-randomized, mono-centric, open | HRPF (Risolac®) Or a soy formula Or CMP-eHF Or free diet in control group | Weight; Weight z-score were similar in the 3 groups with CMPA during the first 2 years. Weight gain was smaller in the HRPF group (p 0.025) vs control group. | |
| Agostoni et al., 2007 [87] | 93 infants CMPA 32 controls Age: 6–12 months | Multi-center-forward, randomized, comparative, open | Weight: RHPF: −0.30 (−0.34) Control: −0.10 Height: RHPF: −0.21 Control: −0.12 | soy formula (n-32), CMP-eHF (n-31) and HRPF (Risolac®) (n-30) | Weight: RHPF: −0.09 Control: 0.07 Height: RHPF: 0.11 Control: 0.27 |
| Reche et al. 2010 [67] | 92 infants CMPA (skin prick tests) Age: 1.5–9 months | Prospective open, randomized | CMP-eHF and HRPF | Weight: similar Height: similar | |
| Vandenplas et al., 2014) [68] | 42 infants Age: 3.4 ± 1.5 months | Weight: HRPF: −0.7 ± 1.0 Height: HRPF: −0.1 ± 1.0 | HRPF | Weight: HRPF: −0.1 ± 0.9 Height: HRPF: −0.1 ± 1.1 | |
| Lasekan et al., 2006 [57] | 65 infants Healthy infants (without CMPA) Age: 0 to 16 weeks | Randomized double-blind trial | HRPF (Ross formula) or standard formula for 4 months | Weight: similar Height: similar Protein nutritional status: Plasma protein concentrations, particularly for total plasma proteins, serum albumin, and pre-albumin/transthyretin: comparable in both groups |
| Study | Patients | Type of Study | Intervention | Outcomes |
|---|---|---|---|---|
| Reche et al., 2010 [67] | 92 infants CMPA IgE-mediated confirmed by a positive OFC Age: average 4.3 months (1.1 to 10) | Prospective, open and randomized clinical trial | 46 fed a HRPF (Blemil Arroz®/Modilac Expert Riz 1®) 46 a CMP-eHF for 2 years | Percentage of children becoming tolerant: similar with the HRPF and the—CMP-eHF after 12, 18, and 24 months of feeding |
| Terraciano et al., 2010 [88] | 72 infants CMPA Age: 14.1 ± 8.6 months | Prospective cohort | Fed with CMP-eHF or soya formula or HRPF For 26 months (median duration) | Time before tolerance was acquired (median duration of the disease): CMP-eHF group: 56 months (IC 95% not applicable) (average—ES: 40.2–4.8 months) Soy formula group: 28 months (IC 95% 11–37) (average—ES: 24.3–2.6) HRPF group: 20 months (IC 95% 10–33) (average—ES: 24.3–3.6) This beneficial effect was not observed in polysensitized children |
| Berni Canani et al., 2013 [86] | 260 infants CMPA confirmed by DBPCFC with milk Age: 1 to 12 months | Multicenter retrospective observational study | 71 fed with a CMP-eHF- Lactobacillus Rhamnosus GG (LGG) 55 with a CMP-eHF, 46 with a HRPF (Risolac®) 55 with a soy formula 33 with an amino-acids-based formula (AAF) | Percentage of patients having outgrown CMPA after 12 months: Similar with the CMP-eHF, the HRPF, soy formula and the AAF Significantly shorter in-CMP-eHF-LGG group (OR 4.8; 95% CI 2.2–10.5; p 0. 001) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dupont, C.; Bocquet, A.; Tomé, D.; Bernard, M.; Campeotto, F.; Dumond, P.; Essex, A.; Frelut, M.-L.; Guénard-Bilbault, L.; Lack, G.; et al. Hydrolyzed Rice Protein-Based Formulas, a Vegetal Alternative in Cow’s Milk Allergy. Nutrients 2020, 12, 2654. https://doi.org/10.3390/nu12092654
Dupont C, Bocquet A, Tomé D, Bernard M, Campeotto F, Dumond P, Essex A, Frelut M-L, Guénard-Bilbault L, Lack G, et al. Hydrolyzed Rice Protein-Based Formulas, a Vegetal Alternative in Cow’s Milk Allergy. Nutrients. 2020; 12(9):2654. https://doi.org/10.3390/nu12092654
Chicago/Turabian StyleDupont, Christophe, Alain Bocquet, Daniel Tomé, Marie Bernard, Florence Campeotto, Pascale Dumond, Anna Essex, Marie-Laure Frelut, Lydie Guénard-Bilbault, Gideon Lack, and et al. 2020. "Hydrolyzed Rice Protein-Based Formulas, a Vegetal Alternative in Cow’s Milk Allergy" Nutrients 12, no. 9: 2654. https://doi.org/10.3390/nu12092654