Effects of Consumption of Alcohol on Intraocular Pressure: Korea National Health and Nutrition Examination Survey 2010 to 2011


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Participants
2.2. Data Collection and Definitions of Variables
2.3. Ophthalmological Examination
2.4. Definitions of OAG and Control Groups
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
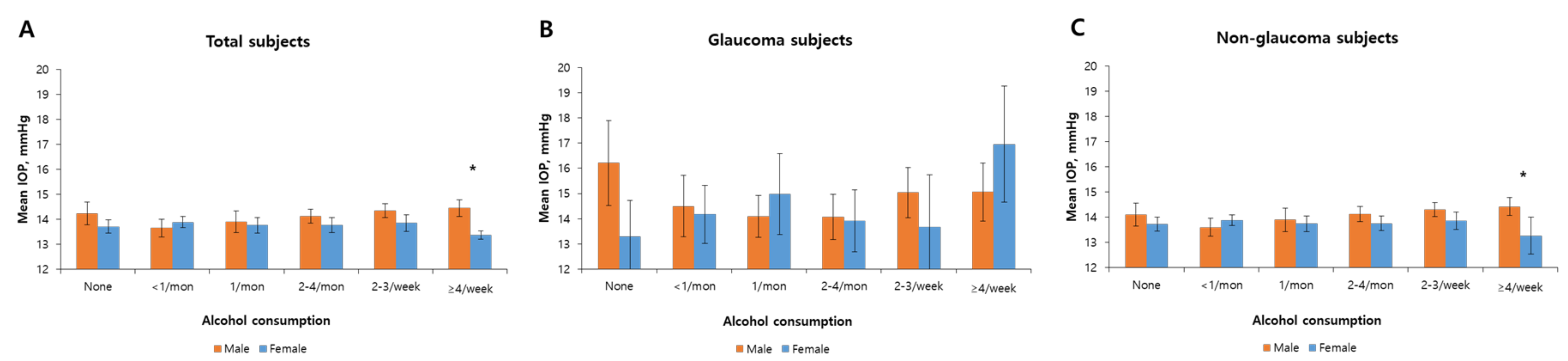
3.2. The Association between Alcohol Consumption and IOP
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Hoyng, P.F.J.; Kitazawa, Y. Medical treatment of normal tension glaucoma. Surv. Ophthalmol. 2002, 47 (Suppl. 1), S116–S124. [Google Scholar] [CrossRef]
- Lin, S.C.; Pasquale, L.R.; Singh, K.; Lin, S.C. The association between body mass index and open-angle glaucoma in a South Korean population-based sample. J. Glaucoma 2018, 27, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.H.; Cho, Y.H.; Kim, Y.J.; Lee, S.Y.; Lee, J.G.; Kong, E.H.; Cho, B.M.; Tak, Y.J.; Hwang, H.R.; Lee, S.H.; et al. Metabolic syndrome as a risk factor for high intraocular pressure: The Korea National Health and Nutrition Examination Survey 2008–2010. Diabetes Metab. Syndr. Obes. 2019, 12, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Bao, X. Hyperlipidemia, Blood Lipid Level, and the Risk of Glaucoma: A Meta-Analysis. Investig. Ophthalmol. Vis. Sci. 2019, 60, 1028–1043. [Google Scholar] [CrossRef] [Green Version]
- Shim, S.H.; Sung, K.R.; Kim, J.M.; Kim, H.T.; Jeong, J.; Kim, C.Y.; Lee, M.Y.; Park, K.H. The prevalence of open-angle glaucoma by age in myopia: The Korea National Health and Nutrition Examination Survey. Curr. Eye Res. 2017, 42, 65–71. [Google Scholar] [CrossRef]
- Yoon, J.Y.; Sung, K.R.; Yun, S.C.; Shin, J.W. Progressive Optic Disc Tilt in Young Myopic Glaucomatous Eyes. Korean J. Ophthalmol. 2019, 33, 520–527. [Google Scholar] [CrossRef] [Green Version]
- Elyadari, M.; Azennoud, S.; Elmerrouni, S.; Harchali, S.; Zarrouki, M.; Jebbar, Z.; El Hassan, A.; Berraho, A. Lens induced glaucoma: Report of 60 cases. J. Fr. Ophtalmol. 2017, 40, e343–e346. [Google Scholar] [CrossRef]
- Vera, J.; Jimenez, R.; Garcia-Ramos, A.; Cardenas, D. Muscular strength is associated with higher intraocular pressure in physically active males. Optom. Vis. Sci. 2018, 95, 143–149. [Google Scholar] [CrossRef]
- Chiotoroiu, S.M.; de Popa, D.P.; Ştefăniu, G.I.; Secureanu, F.A.; Purcărea, V.L. The importance of alcohol abuse and smoking in the evolution of glaucoma disease. J. Med. Life 2013, 6, 226–229. [Google Scholar]
- Haorah, J.; Knipe, B.; Leibhart, J.; Ghorpade, A.; Persidsky, Y. Alcohol-induced oxidative stress in brain endothelial cells causes blood-brain barrier dysfunction. J. Leukoc. Biol. 2005, 78, 1223–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protection of Neurons Against Glutamate-Induced Damage in Glaucoma and other Conditions. Available online: http://www.freepatentsonline.com/y2002/0077322.html (accessed on 1 May 2020).
- Altura, B.M.; Altura, B.T. Alcohol, the cerebral circulation and strokes. Alcohol 1984, 1, 325–331. [Google Scholar] [CrossRef]
- Battey, L.L.; Heyman, A.; Patterson, J.L., Jr. Effects of ethyl alcohol on cerebral blood flow and metabolism. J. Am. Med. Assoc. 1953, 152, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kim, M.S.; Jang, H.J.; Park, K.H.; Caprioli, J. The association between retinal vessel diameter and retinal nerve fiber layer thickness in asymmetric normal tension glaucoma patients. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5609–5614. [Google Scholar] [CrossRef] [PubMed]
- Houle, R.E.; Grant, W.M. Alcohol, vasopressin, and intraocular pressure. Investig. Ophthalmol. Vis. Sci. 1967, 6, 145–154. [Google Scholar]
- Leydhecker, W.; Krieglstein, G.K.; Uhlich, E. Experimental investigations on the mode of action of alcoholic liquor on the intra-ocular pressure (author’s transl). Klin. Monbl. Augenheilkd. 1978, 173, 75–79. [Google Scholar]
- Leske, M.C.; Warheit-Roberts, L.; Wu, S.Y. Open-angle glaucoma and ocular hypertension: The Long Island Glaucoma Case-control Study. Ophthalmic Epidemiol. 1996, 3, 85–96. [Google Scholar] [CrossRef]
- Lin, H.Y.; Hsu, W.M.; Chou, P.; Liu, C.J.; Chou, J.C.; Tsai, S.Y.; Cheng, C.Y. Intraocular pressure measured with a noncontact tonometer in an elderly Chinese population: The Shihpai Eye Study. Arch. Ophthalmol. 2005, 123, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, M.; Ishikawa, M.; Kokaze, A.; Sekine, Y.; Matsunaga, N.; Uchida, Y.; Takashima, Y. Association of life-style with intraocular pressure in middle-aged and older Japanese residents. Jpn. J. Ophthalmol. 2003, 47, 191–198. [Google Scholar] [CrossRef]
- Kahn, H.A.; Milton, R.C. Alternative definitions of open-angle glaucoma. Effect on prevalence and associations in the Framingham eye study. Arch. Ophthalmol. 1980, 98, 2172–2177. [Google Scholar] [CrossRef]
- Seddon, J.M.; Schwartz, B.; Flowerdew, G. Case-control study of ocular hypertension. Arch. Ophthalmol. 1983, 101, 891–894. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.J.; Leung, Y.F.; Wang, N.; Lam, S.C.; Liu, Y.; Tam, O.S.; Pang, C.P. Genetic and environmental risk factors for primary open-angle glaucoma. Chin. Med. J. (Engl.) 2004, 117, 706–710. [Google Scholar] [PubMed]
- Klein, B.E.; Klein, R.; Ritter, L.L. Relationship of drinking alcohol and smoking to prevalence of open-angle glaucoma. The Beaver Dam Eye Study. Ophthalmology 1993, 100, 1609–1613. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Foster, P.J.; Buhrmann, R.; Quigley, H.A.; Johnson, G.J. The definition and classification of glaucoma in prevalence surveys. Br. J. Ophthalmol. 2002, 86, 238–242. [Google Scholar] [CrossRef] [Green Version]
- Chon, B.; Qiu, M.; Lin, S.C. Myopia and glaucoma in the South Korean population. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6570–6577. [Google Scholar] [CrossRef]
- Kim, M.J.; Kim, M.J.; Kim, H.S.; Jeoung, J.W.; Park, K.H. Risk factors for open-angle glaucoma with normal baseline intraocular pressure in a young population: The Korea National Health and Nutrition Examination Survey. Clin. Exp. Ophthalmol. 2014, 42, 825–832. [Google Scholar] [CrossRef]
- The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am. J. Ophthalmol. 2000, 130, 429–440. [Google Scholar] [CrossRef]
- Kim, K.E.; Kim, J.M.; Lee, J.; Lee, M.Y.; Park, K.H. Significant intraocular pressure associated with open-angle glaucoma: Korea National Health and Nutrition Examination Survey 2010–2011. PLoS ONE 2020, 15, e0235701. [Google Scholar] [CrossRef]
- Gonzalez-Reimers, E.; Santolaria-Fernandez, F.; Martin-Gonzalez, M.C.; Fernandez-Rodriguez, C.M.; Quintero-Platt, G. Alcoholism: A systemic proinflammatory condition. World J. Gastroenterol. 2014, 20, 14660–14671. [Google Scholar] [CrossRef]
- Takagi, S.; Baba, S.; Iwai, N.; Fukuda, M.; Katsuya, T.; Higaki, J.; Mannami, T.; Ogata, J.; Goto, Y.; Ogihara, T.J.H.R. The aldehyde dehydrogenase 2 gene is a risk factor for hypertension in Japanese but does not alter the sensitivity to pressor effects of alcohol: The Suita study. Hypertens. Res. 2001, 24, 365–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieber, C.S. Metabolism of alcohol. Clin. Liver Dis. 2005, 9, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Walker, J.; Momenan, R.; Rawlings, R.; Heilig, M.; Hommer, D.W. Relationship between liver function and brain shrinkage in patients with alcohol dependence. Alcohol. Clin. Exp. Res. 2012, 36, 625–632. [Google Scholar] [CrossRef] [PubMed]
- de la Monte, S.M.; Longato, L.; Tong, M.; DeNucci, S.; Wands, J.R. The liver-brain axis of alcohol-mediated neurodegeneration: Role of toxic lipids. Int. J. Environ. Res. Public Health 2009, 6, 2055–2075. [Google Scholar] [CrossRef] [PubMed]
- Lambuk, L.; Jafri, A.J.A.; Iezhitsa, I.; Agarwal, R.; Bakar, N.S.; Agarwal, P.; Abdullah, A.; Ismail, N.M. Dose-dependent effects of NMDA on retinal and optic nerve morphology in rats. Int. J. Ophthalmol 2019, 12, 746–753. [Google Scholar] [PubMed]
- Sandell, J.H. GABA as a developmental signal in the inner retina and optic nerve. Perspect. Dev. Neurobiol. 1998, 5, 269–278. [Google Scholar]
- Yeh, H.H.; Kolb, J.E. Ethanol modulation of GABA-activated current responses in acutely dissociated retinal bipolar cells and ganglion cells. Alcohol. Clin. Exp. Res. 1997, 21, 647–655. [Google Scholar] [CrossRef]
- Chandrasekar, R. Alcohol and NMDA receptor: Current research and future direction. Front. Mol. Neurosci. 2013, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Criqui, M.H.; Wallace, R.B.; Mishkel, M.; Barrett-Connor, E.; Heiss, G. Alcohol consumption and blood pressure. The lipid research clinics prevalence study. Hypertension 1981, 3, 557–565. [Google Scholar] [CrossRef] [Green Version]
- Veerappan, R.M.; Senthil, S.; Rao, M.R.; Ravikumar, R.; Pugalendi, K.V. Redox status and lipid peroxidation in alcoholic hypertensive patients and alcoholic hypertensive patients with diabetes. Clin. Chim. Acta 2004, 340, 207–212. [Google Scholar] [CrossRef]
- Grieshaber, M.C.; Pienaar, A.; Olivier, J.; Stegmann, R. Clinical evaluation of the aqueous outflow system in primary open-angle glaucoma for canaloplasty. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1498–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pexczon, J.D.; Grant, W.M. Glaucoma, Alcohol, and Intraocular pressure. Arch. Ophthalmol. 1965, 73, 495–501. [Google Scholar] [CrossRef]
- Kiyosawa, K. Studies on the effects of alcohols on membrane water permeability of Nitella. Protoplasma 1975, 86, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Lang, F. Osmotic diuresis. Ren. Physiol. 1987, 10, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Brien, S.E.; Ronksley, P.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: Systematic review and meta-analysis of interventional studies. BMJ 2011, 342, d636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dufour, M.C.; Caces, M.F.; Whitmore, C.C.; Hanna, E.Z. Alcohol consumption and death from acute myocardial infarction in a national longitudinal cohort. Alcohol. Clin. Exp. Res. 1996, 20, 97A. [Google Scholar]
- Elkind, M.S.; Sciacca, R.; Boden-Albala, B.; Rundek, T.; Paik, M.C.; Sacco, R.L. Moderate alcohol consumption reduces risk of ischemic stroke: The Northern Manhattan Study. Stroke 2006, 37, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Kojima, S.; Sugiyama, T.; Kojima, M.; Azuma, I.I.; Ito, S. Effect of the consumption of ethanol on the microcirculation of the human optic nerve head in the acute phase. Jpn. J. Ophthalmol. 2000, 44, 318–319. [Google Scholar] [CrossRef]
- Rhee, D.J.; Gupta, M.; Moncavage, M.B.; Moster, M.L.; Moster, M.R. Idiopathic elevated episcleral venous pressure and open-angle glaucoma. Br. J. Ophthalmol. 2009, 93, 231–234. [Google Scholar] [CrossRef]
- Bukiya, A.N.; Seleverstov, O.; Bisen, S.; Dopico, A.M. Age-Dependent Susceptibility to Alcohol-Induced Cerebral Artery Constriction. J. Drug Alcohol. Res. 2016, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Eby, J.M.; Majetschak, M. Effects of ethanol and ethanol metabolites on intrinsic function of mesenteric resistance arteries. PLoS ONE 2019, 14, e0214336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Fedinec, A.L.; Kuntamallappanavar, G.; Leffler, C.W.; Bukiya, A.N.; Dopico, A.M. Endothelial nitric oxide mediates caffeine antagonism of alcohol-induced cerebral artery constriction. J. Pharmacol. Exp. Ther. 2016, 356, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Gordon, E.L.; Nguyen, T.S.; Ngai, A.C.; Winn, H.R. Differential effects of alcohols on intracerebral arterioles. Ethanol alone causes vasoconstriction. J. Cereb. Blood Flow Metab. 1995, 15, 532–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gherghel, D.; Orgul, S.; Gugleta, K.; Gekkieva, M.; Flammer, J. Relationship between ocular perfusion pressure and retrobulbar blood flow in patients with glaucoma with progressive damage. Am. J. Ophthalmol. 2000, 130, 597–605. [Google Scholar] [CrossRef]
- Kim, H.T.; Kim, J.M.; Kim, J.H.; Lee, J.H.; Lee, M.Y.; Lee, J.Y.; Won, Y.S.; Park, K.H.; Kwon, H.S. Relationships Between Anthropometric Measurements and Intraocular Pressure: The Korea National Health and Nutrition Examination Survey. Am. J. Ophthalmol. 2017, 173, 23–33. [Google Scholar] [CrossRef]
- Frezza, M.; di Padova, C.; Pozzato, G.; Terpin, M.; Baraona, E.; Lieber, C.S. High blood alcohol levels in women. The role of decreased gastric alcohol dehydrogenase activity and first-pass metabolism. N. Engl. J. Med. 1990, 322, 95–99. [Google Scholar] [CrossRef]
- Alfonso-Loeches, S.; Pascual, M.; Guerri, C. Gender differences in alcohol-induced neurotoxicity and brain damage. Toxicology 2013, 311, 27–34. [Google Scholar] [CrossRef]
- Komarekova, I.; Straka, L.; Novomesky, F.; Hejna, P. Gender differences in alcohol affection on an individual. Soud. Lek. 2013, 58, 36–38. [Google Scholar]
- Mukherjee, S. Alcoholism and its effects on the central nervous system. Curr. Neurovasc. Res. 2013, 10, 256–262. [Google Scholar] [CrossRef]
- Khachatryan, N.; Pistilli, M.; Maguire, M.G.; Salowe, R.J.; Fertig, R.M.; Moore, T.; Gudiseva, H.V.; Chavali, V.R.M.; Collins, D.W.; Daniel, E.; et al. Primary Open-Angle African American Glaucoma Genetics (POAAGG) Study: Gender and risk of POAG in African Americans. PLoS ONE 2019, 14, e0218804. [Google Scholar] [CrossRef] [Green Version]
- Giovannucci, E.; Colditz, G.; Stampfer, M.J.; Rimm, E.B.; Litin, L.; Sampson, L.; Willett, W.C. The assessment of alcohol consumption by a simple self-administered questionnaire. Am. J. Epidemiol. 1991, 133, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Malarcher, A.M.; Giles, W.H.; Croft, J.B.; Wozniak, M.A.; Wityk, R.J.; Stolley, P.D.; Stern, B.J.; Sloan, M.A.; Sherwin, R.; Price, T.R.; et al. Alcohol intake, type of beverage, and the risk of cerebral infarction in young women. Stroke 2001, 32, 77–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.F. Lunch eating behavior of preschool children. Effects of age, gender, and type of beverage served. Physiol. Behav. 2000, 70, 27–33. [Google Scholar] [CrossRef]
- Lee, S.; Kim, J.S.; Kim, S.S.; Jung, J.G.; Yoon, S.J.; Seo, Y.; Kim, J.; Bae, Y.K.; Lee, J.Y. Relationship between Alcohol Consumption and Ocular Pressure according to Facial Flushing in Korean Men with Obesity. Korean J. Fam. Med. 2019, 40, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Ota, M.; Hisada, A.; Lu, X.; Nakashita, C.; Masuda, S.; Katoh, T. Associations between aldehyde dehydrogenase 2 (ALDH2) genetic polymorphisms, drinking status, and hypertension risk in Japanese adult male workers: A case-control study. Environ. Health Prev. Med. 2016, 21, 1–8. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 6504) | p Value | Male (n = 2983, 45.9%) | p Value | Female (n = 3521, 54.1%) | p Value | |||
|---|---|---|---|---|---|---|---|---|---|
| Non-Glaucoma (n = 6216, 96.1%) | Glaucoma (n = 288, 3.9%) | Non-Glaucoma (n = 2803, 95.2%) | Glaucoma (n = 180; 4.8%) | Non-Glaucoma (n = 3413, 97.0%) | Glaucoma (n = 108, 3.0%) | ||||
| Age, years | 41.1 (0.3) | 49.2 (1.2) | <0.001 | 41 (0.4) | 49.2 (1.4) | <0.001 | 41.3 (0.3) | 49.1 (1.9) | <0.001 |
| Current smoker, % | 30 (0.8) | 31.5 (3.44) | 0.678 | 50.5 (1.21) | 44.8 (4.45) | 0.227 | 7.6 (0.58) | 7.4 (3.08) | 0.958 |
| Drinker, % | 68 (0.78) | 68.8 (3.35) | 0.814 | 83.2 (0.87) | 78.9 (3.9) | 0.248 | 51.5 (1.09) | 50.7 (6.2) | 0.907 |
| BMI, kg/m2 | 23.7 (0.1) | 23.9 (0.2) | 0.496 | 24.2 (0.1) | 23.7 (0.2) | 0.032 | 23.1 (0.1) | 24.2 (0.5) | 0.025 |
| Waist circumference, cm | 81 (0.2) | 82.2 (0.7) | 0.095 | 84.5 (0.2) | 83.5 (0.7) | 0.201 | 77.1 (0.2) | 79.9 (1.3) | 0.044 |
| Systolic blood pressure, mmHg | 116.3 (0.3) | 122.8 (1.3) | <0.001 | 119.5 (0.3) | 123.9 (1.6) | 0.008 | 112.7 (0.4) | 120.9 (2) | <0.001 |
| Diastolic blood pressure, mmHg | 76.7 (0.2) | 80.1 (0.8) | <0.001 | 79.7 (0.3) | 81.7 (1.1) | 0.078 | 73.3 (0.2) | 77.2 (1.1) | 0.001 |
| Serum glucose, mg/dL | 94.9 (0.3) | 99.9 (1.9) | 0.009 | 97.5 (0.5) | 102 (2.8) | 0.111 | 92.1 (0.3) | 96.2 (1.7) | 0.02 |
| Total cholesterol, mg/dL | 187.1 (0.6) | 188.6 (3.4) | 0.666 | 188.8 (0.9) | 186.4 (4.7) | 0.621 | 185.3 (0.7) | 192.6 (3.7) | 0.049 |
| HDL-C, mg/dL | 53.3 (0.2) | 51 (1.02) | 0.026 | 50 (0.3) | 48.8 (1.3) | 0.389 | 56.9 (0.3) | 54.8 (1.3) | 0.121 |
| LDL-C, mg/dL | 111.9 (0.8) | 110.1 (4.5) | 0.694 | 113.9 (1.1) | 109 (5.5) | 0.387 | 109.1 (1.2) | 113.1 (7.9) | 0.605 |
| Triglycerides, mg/dL | 132.2 (1.9) | 154 (14.4) | 0.132 | 158.5 (3.2) | 172 (21.7) | 0.536 | 103.4 (1.6) | 121.5 (7.2) | 0.015 |
| Diabetic, % | 21.8 (0.74) | 31.1 (3.24) | 0.002 | 27.1 (1.11) | 36.5 (4.74) | 0.038 | 16.1 (0.8) | 21.7 (4.14) | 0.147 |
| Hypertension, % | 42.1 (0.92) | 58.8 (3.74) | <0.001 | 52.9 (1.29) | 62.3 (4.86) | 0.064 | 30.2 (1.02) | 52.4 (5.72) | <0.001 |
| IOP (mmHg) | 14 (0.1) | 14.5 (0.2) | 0.019 | 14.1 (0.1) | 14.7 (0.2) | 0.021 | 13.8 (0.1) | 14.1 (0.3) | 0.391 |
| Variables | Total (n = 6504) | p Value | Non-Glaucoma (n = 6216, 96.1%) | p Value | Glaucoma (n = 288, 3.9%) | p Value | |||
|---|---|---|---|---|---|---|---|---|---|
| IOP ≥ 18 mmHg (n = 730, 11.3%) | IOP < 18 mmHg (n = 5774, 88.7%) | IOP ≥ 18 mmHg (n = 683; 11.1%) | IOP < 18 mmHg (n = 5533, 88.9%) | IOP ≥ 18 mmHg (n = 47, 16.9%) | IOP < 18 mmHg (n = 241, 83.1%) | ||||
| Age, years | 41.8 (0.6) | 41.4 (0.3) | 0.523 | 41.2 (0.6) | 41.1 (0.3) | 0.905 | 51.8 (2.3) | 48.6 (1.3) | 0.236 |
| Male, % | 59.1 (2.2) | 51.9 (0.75) | 0.004 | 58.6 (2.3) | 51.5 (0.76) | 0.056 | 67.6 (8.46) | 63.5 (3.64) | 0.665 |
| Current smoker, % | 35.1 (2.43) | 29.4 (0.82) | 0.021 | 34.6 (2.56) | 29.5 (0.82) | 0.044 | 43.3 (9.12) | 29 (3.7) | 0.13 |
| Drinker, % | 73.7 (2.05) | 67.3 (0.8) | 0.005 | 73.3 (2.15) | 67.4 (0.81) | 0.011 | 79.6 (7.23) | 66.7 (3.55) | 0.14 |
| BMI, kg/m2 | 24.3 (0.2) | 23.6 (0.1) | 0.002 | 24.3 (0.2) | 23.6 (0.1) | 0.002 | 24.1 (0.6) | 23.8 (0.3) | 0.592 |
| Waist circumference, cm | 82.7 (0.5) | 80.8 (0.2) | 0.001 | 82.6 (0.5) | 80.8 (0.2) | 0.001 | 84.6 (2.3) | 81.8 (0.7) | 0.226 |
| Systolic blood pressure, mmHg | 120 (0.7) | 116.1 (0.3) | <0.001 | 119.6 (0.7) | 115.9 (0.3) | <0.001 | 126.9 (3.6) | 121.9 (1.3) | 0.181 |
| Diastolic blood pressure, mmHg | 78.9 (0.5) | 76.5 (0.2) | <0.001 | 78.7 (0.5) | 76.4 (0.2) | <0.001 | 82.5 (2.5) | 79.6 (0.8) | 0.267 |
| Serum glucose, mg/dL | 97.3 (1.2) | 94.8 (0.3) | 0.052 | 97.4 (1.3) | 94.6 (0.3) | 0.033 | 95.7 (3.7) | 100.8 (2.2) | 0.249 |
| Total cholesterol, mg/dL | 191.4 (1.6) | 186.6 (0.6) | 0.004 | 191.4 (1.7) | 186.6 (0.6) | 0.007 | 192.5 (7.2) | 187.8 (3.7) | 0.552 |
| HDL-C, mg/dL | 52.4 (0.6) | 53.3 (0.2) | 0.138 | 52.4 (0.6) | 53.4 (0.2) | 0.1 | 52.5 (2.1) | 50.7 (1.1) | 0.417 |
| LDL-C, mg/dL | 120.1 (2.2) | 110.8 (0.8) | <0.001 | 120.8 (2.3) | 110.9 (0.8) | <0.001 | 111.7 (6.7) | 109.7 (5.3) | 0.806 |
| Triglycerides, mg/dL | 143.4 (5.4) | 131.7 (2.1) | 0.049 | 142.8 (5.7) | 130.8 (2) | 0.056 | 152.5 (18.2) | 154.2 (17) | 0.945 |
| Diabetic, % | 25.9 (2.05) | 21.7 (0.76) | 0.038 | 25.7 (2.18) | 21.3 (0.77) | 0.04 | 29.3 (7.7) | 31.5 (3.71) | 0.811 |
| Hypertension, % | 53.1 (2.14) | 41.4 (0.95) | <0.001 | 52.1 (2.21) | 40.8 (0.98) | <0.001 | 70.2 (8.38) | 56.5 (3.94) | 0.151 |
| IOP (mmHg) | 18.7 (0.04) | 13.4 (0.1) | <0.001 | 18.7 (0.04) | 13.4 (0.1) | <0.001 | 18.6 (0.2) | 13.6 (0.2) | <0.001 |
| Variables | Drinker | p Value | |
|---|---|---|---|
| IOP ≥ 18 mmHg | IOP < 18 mmHg | ||
| Male | |||
| Number, % | 328 (13.32) | 2113 (86.7) | |
| Age, years | 41.73 (0.82) | 40.69 (0.41) | 0.227 |
| Current smoker, % | 170 (56.39) | 996 (52.11) | 0.255 |
| BMI, kg/m2 | 24.5 (0.28) | 24.21 (0.08) | 0.301 |
| Waist circumference, cm | 85.1 (0.75) | 84.51 (0.26) | 0.450 |
| Systolic blood pressure, mmHg | 123.76 (0.93) | 119.67 (0.38) | <0.001 |
| Diastolic blood pressure, mmHg | 82.13 (0.66) | 79.87 (0.32) | 0.002 |
| Serum glucose, mg/dL | 100.64 (1.98) | 97.35 (0.53) | 0.112 |
| Total cholesterol, mg/dL | 193.56 (2.42) | 187.92 (1.02) | 0.023 |
| HDL-C, mg/dL | 50.69 (0.71) | 50.55 (0.35) | 0.849 |
| LDL-C, mg/dL | 121.59 (3.26) | 110.93 (1.23) | 0.002 |
| Triglycerides, mg/dL | 169.13 (9.66) | 165.57 (4.13) | 0.734 |
| Diabetic, % | 121 (33.04) | 650 (26.81) | 0.043 |
| Hypertension, % | 213 (62.33) | 1215 (53.44) | 0.011 |
| IOP (mmHg) | 18.83 (0.06) | 13.52 (0.08) | <0.001 |
| Female | |||
| Number, % | 185 (10.3) | 1518 (89.7) | |
| Age, years | 39.74 (1.08) | 39.94 (0.38) | 0.866 |
| Current smoker, % | 17 (10.51) | 132 (10.58) | 0.981 |
| BMI, kg/m2 | 23.83 (0.39) | 22.97 (0.11) | 0.031 |
| Waist circumference, cm | 78.64 (1.1) | 76.74 (0.31) | 0.097 |
| Systolic blood pressure, mmHg | 113.52 (1.22) | 112.51 (0.56) | 0.439 |
| Diastolic blood pressure, mmHg | 74.53 (0.81) | 73.23 (0.36) | 0.130 |
| Serum glucose, mg/dL | 93.4 (1.24) | 92.07 (0.44) | 0.319 |
| Total cholesterol, mg/dL | 183.12 (2.47) | 183.72 (1.12) | 0.821 |
| HDL-C, mg/dL | 56.95 (1.33) | 58.37 (0.39) | 0.308 |
| LDL-C, mg/dL | 108.12 (4.31) | 105.86 (1.79) | 0.618 |
| Triglycerides, mg/dL | 100.31 (4.64) | 101.16 (2.19) | 0.868 |
| Diabetic, % | 35 (16.35) | 274 (16.08) | 0.94 |
| Hypertension, % | 69 (33.56) | 480 (28.13) | 0.165 |
| IOP (mmHg) | 18.6 (0.08) | 13.21 (0.08) | <0.001 |
| Alcohol Drinking | Total | Male | Female |
|---|---|---|---|
| None | 3.78 (2.49–5.69) | 6.33 (3.38–11.56) | 2.67 (1.51–4.65) |
| <1 time/month | 3.86 (2.72–5.45) | 5.65 (3.37–9.32) | 3.21 (2.07–4.95) |
| 1 time/month | 4.06 (2.58–6.33) | 6.68 (3.71–11.73) | 2.36 (1.25–4.41) |
| 2–4 times/month | 3.31 (2.46–4.45) | 3.51 (2.39–5.12) | 3.01 (1.88–4.79) |
| 2–3 times/week | 4.78 (3.57–6.39) | 5.09 (3.58–7.18) | 3.82 (2.18–6.61) |
| ≥4 times/week | 4.42 (2.78–6.94) | 4.71 (2.87–7.65) | 2.56 (0.89–7.17) |
| Total | 3.93 (3.35–4.61) | 4.78 (3.94–5.8) | 2.98 (2.36–3.74) |
| Alcohol Drinking | Unadjusted β Coefficient | Model 1 * | Model 2 † | Model 3 ‡ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total β (95% CI) | Male β (95% CI) | Female β (95% CI) | Total β (95% CI) | Male β (95% CI) | Female β (95% CI) | Total β (95% CI) | Male β (95% CI) | Female β (95% CI) | Total β (95% CI) | Male β (95% CI) | Female β (95% CI) | |
| IOP (β coefficient); Non-glaucoma subjects | ||||||||||||
| None | 0.03 (−0.24 to 0.3) | 0.51 (−0.07 to 1.08) | −0.15 (−0.46 to 0.15) | 0.01 (−0.27 to 0.28) | 0.51 (−0.06 to 1.09) | −0.17 (−0.47 to 0.14) | 0.01 (−0.27 to 0.28) | 0.52 (−0.06 to 1.09) | −0.17 (−0.47 to 0.14) | 0.001 (−0.27 to 0.27) | 0.48 (−0.12 to 1.07) | −0.16 (−0.47 to 0.14) |
| <1 time/month | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) |
| 1 time/month | −0.002 (−0.31 to 0.31) | 0.3 (−0.27 to 0.87) | −0.14 (−0.47 to 0.19) | −0.02 (−0.33 to 0.29) | 0.33 (−0.24 to 0.91) | −0.13 (−0.47 to 0.2) | −0.02 (−0.33 to 0.29) | 0.33 (−0.24 to 0.91) | −0.14 (−0.48 to 0.19) | −0.06 (−0.37 to 0.25) | 0.3 (−0.28 to 0.88) | −0.19 (−0.52 to 0.14) |
| 2–4 times/month | 0.19 (−0.07 to 0.44) | 0.54 (0.08 to 0.99) | −0.12 (−0.45 to 0.21) | 0.1 (−0.16 to 0.36) | 0.53 (0.08 to 0.98) | −0.09 (−0.43 to 0.24) | 0.1 (−0.16 to 0.36) | 0.53 (0.08 to 0.98) | −0.09 (−0.43 to 0.25) | 0.06 (−0.2 to 0.32) | 0.46 (−0.00 to 0.91) | −0.1 (−0.44 to 0.24) |
| 2–3 times/week | 0.4 (0.12 to 0.67) | 0.71 (0.29 to 1.13) | −0.02 (−0.43 to 0.39) | 0.24 (−0.05 to 0.53) | 0.69 (0.27 to 1.11) | −0.01 (−0.42 to 0.4) | 0.24 (−0.05 to 0.54) | 0.68 (0.26 to 1.10) | 0.0 (−0.42 to 0.43) | 0.19 (−0.11 to 0.48) | 0.59 (0.18 to 1.01) | −0.02 (−0.45 to 0.41) |
| ≥4 times/week | 0.45 (0.1 to 0.81) | 0.82 (0.33 to 1.32) | −0.6 (−1.34 to 0.14) | 0.28 (−0.1 to 0.66) | 0.82 (0.33 to 1.32) | −0.66 (−1.43 to 0.1) | 0.28 (−0.1 to 0.66) | 0.82 (0.32 to 1.31) | −0.64 (−1.41 to 0.13) | 0.25 (−0.14 to 0.63) | 0.73 (0.22 to 1.23) | −0.53 (−1.28 to 0.21) |
| p for trend | 0.001 | 0.002 | 0.611 | 0.049 | 0.002 | 0.698 | 0.052 | 0.003 | 0.764 | 0.116 | 0.011 | 0.741 |
| IOP (β coefficient); Glaucoma subjects | ||||||||||||
| None | 0.47 (−1.19 to 2.14) | 1.71 (−0.4 to 3.82) | −0.89 (−2.75 to 0.98) | 0.43 (−1.09 to 1.95) | 1.79 (−0.01 to 3.59) | −0.98 (−2.68 to 0.73) | 0.43 (−1.1 to 1.95) | 1.8 (−0.01 to 3.58) | −0.98 (−2.69 to 0.73) | 0.49 (−1 to 1.98) | 1.84 (0.11 to 3.57) | −0.82 (−2.53 to 0.9) |
| <1 time/month | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) | 0 (reference) |
| 1 time/month | 0.1 (−1.2 to 1.39) | −0.42 (−1.93 to 1.1) | 0.8 (−1.19 to 2.8) | 0.01 (−1.36 to 1.39) | −0.33 (−1.76 to 1.1) | 0.91 (−1.07 to 2.89) | 0.03 (−1.35 to 1.41) | −0.37 (−1.81 to 1.07) | 0.91 (−1.07 to 2.89) | 0.18 (−1.15 to 1.51) | 0.21 (−1.52 to 1.1) | 1.08 (−0.95 to 3.11) |
| 2–4 times/month | −0.29 (−1.38 to 0.8) | −0.43 (−1.95 to 1.09) | −0.27 (−1.98 to 1.44) | −0.51 (−1.61 to 0.59) | −0.65 (−2.05 to 0.75) | −0.28 (−1.86 to 1.31) | −0.51 (−1.62 to 0.59) | −0.63 (−2.07 to 0.82) | −0.28 (−1.83 to 1.27) | −0.5 (−1.63 to 0.63) | −0.6 (−2.06 to 0.86) | −0.17 (−1.7 to 1.36) |
| 2–3 times/week | 0.48 (−0.88 to 1.84) | 0.54 (−1.16 to 2.24) | −0.5 (−2.89 to 1.89) | 0.21 (−1.19 to 1.61) | 0.57 (−0.92 to 2.06) | −0.14 (−2.44 to 2.17) | 0.25 (−1.11 to 1.61) | 0.49 (−0.95 to 1.93) | −0.16 (−2.57 to 2.24) | −0.01 (−1.34 to 1.32) | 0.21 (−1.22 to 1.65) | −0.07 (−2.45 to 2.31) |
| ≥4 times/week | 0.91 (−0.53 to 2.35) | 0.56 (−1.12 to 2.24) | 2.79 (0.19 to 5.38) | 0.5 (−0.9 to 2.03) | 0.64 (−1.01 to 2.28) | 2.55 (−0.0 to 5.1) | 0.6 (−0.85 to 2.06) | 0.56 (−1.07 to 2.2) | 2.55 (−0.0 to 5.1) | 0.42 (−0.99 to 1.82) | 0.37 (−1.24 to 1.98) | 2.83 (0.28 to 5.38) |
| p for trend | 0.546 | 0.837 | 0.579 | 0.982 | 0.823 | 0.378 | 0.967 | 0.596 | 0.336 | 0.627 | 0.331 | 0.305 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.E.; Kim, J.M.; Lee, M.Y.; Jang, H.J.; Park, K.H. Effects of Consumption of Alcohol on Intraocular Pressure: Korea National Health and Nutrition Examination Survey 2010 to 2011. Nutrients 2020, 12, 2420. https://doi.org/10.3390/nu12082420
Song JE, Kim JM, Lee MY, Jang HJ, Park KH. Effects of Consumption of Alcohol on Intraocular Pressure: Korea National Health and Nutrition Examination Survey 2010 to 2011. Nutrients. 2020; 12(8):2420. https://doi.org/10.3390/nu12082420
Chicago/Turabian StyleSong, Ji Eun, Joon Mo Kim, Mi Yeon Lee, Hye Joo Jang, and Ki Ho Park. 2020. "Effects of Consumption of Alcohol on Intraocular Pressure: Korea National Health and Nutrition Examination Survey 2010 to 2011" Nutrients 12, no. 8: 2420. https://doi.org/10.3390/nu12082420