Dietary Intervention in Pregnant Women with Gestational Diabetes; Protocol for the DiGest Randomised Controlled Trial

 , and
, and
Abstract
:1. Introduction
2. Trial Population and Methods
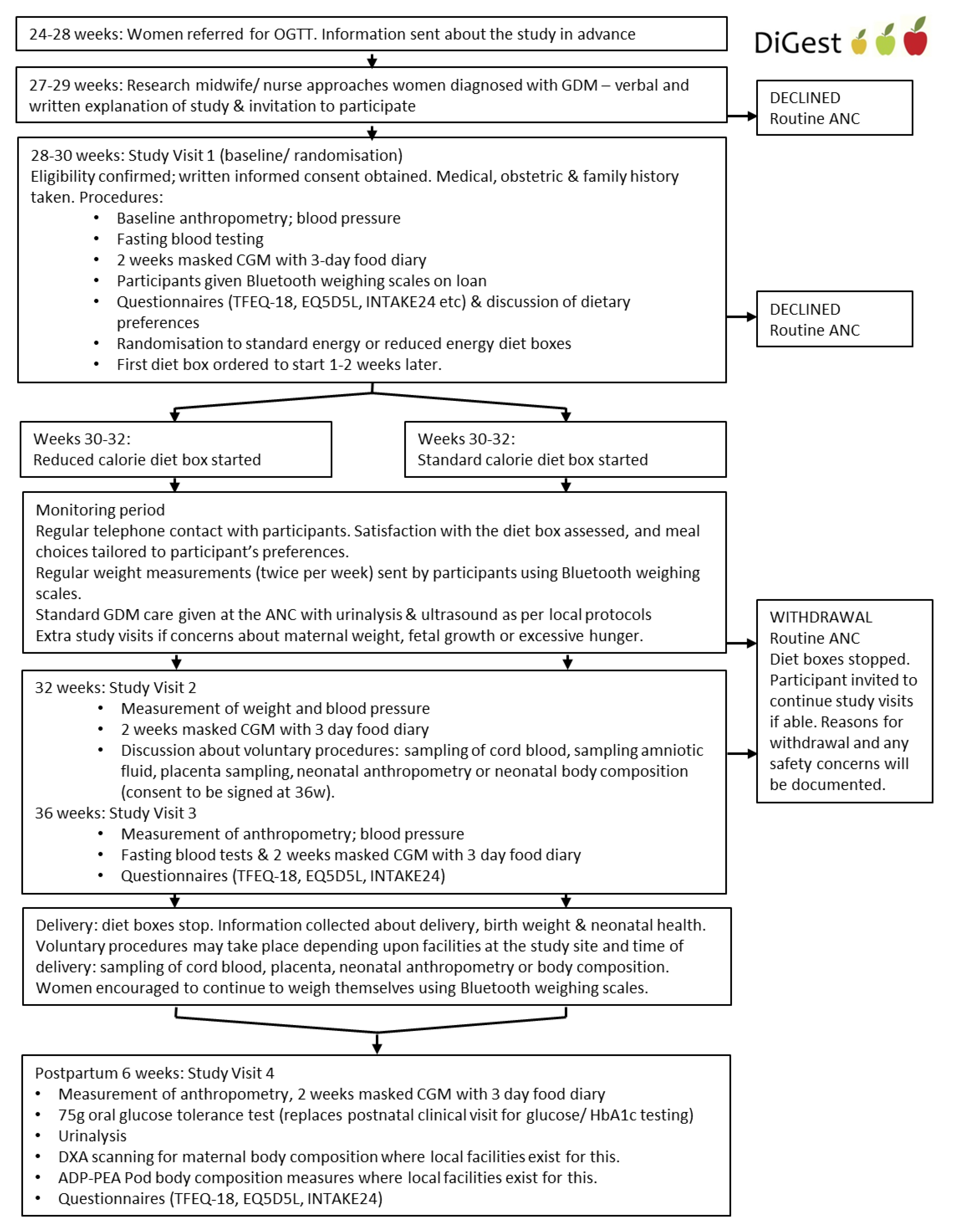
2.1. Trial Design and Ethical Approvals
2.2. Participant Eligibility
2.3. The Following Exclusion Criteria Will Be Applied
2.4. Design of The Intervention
2.5. Baseline Measurements and Randomisation
2.5.1. Clinical Measures
2.5.2. Laboratory Measures
2.6. Dietary Assessment and Compliance
2.6.1. Assessment of Normal Dietary/Energy Intake
2.6.2. Assessment of Adherence to the Diet Boxes
2.6.3. Randomisation and Blinding
2.6.4. Monitoring Period
2.7. Intervention Visits
2.8. Study Outcomes
Secondary Outcomes are Categorised for the Neonate and the Mother as Follows
2.9. Sample Size Justification
- To identify an increase in LGA (odds ratio (OR) 2.25 at 80% power).
- To identify a difference in maternal glycaemia at 36 weeks, for example, differences in mean CGM glucose (0.3 mmol/L difference), time in target (8% difference in time in target (3.5–7.8 mmol/L; >100 min per day), which has been associated with clinically relevant differences in neonatal outcomes) [8].
- To identify a 0.7 mmol/L difference in maternal postnatal two-hour OGTT glucose.
2.10. Statistical Analysis
3. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Diabetes in Pregnancy. Available online: https://www.nice.org.uk/guidance/qs109/chapter/Introduction (accessed on 1 March 2020).
- Albareda, M.; Caballero, A.; Badell, G.; Piquer, S.; Ortiz, A.; de Leiva, A.; Corcoy, R. Diabetes and abnormal glucose tolerance in women with previous gestational diabetes. Diabetes Care 2003, 26, 1199–1205. [Google Scholar] [CrossRef] [Green Version]
- Brunner, S.; Stecher, L.; Ziebarth, S.; Nehring, I.; Rifas-Shiman, S.L.; Sommer, C.; Hauner, H.; von Kries, R. Excessive gestational weight gain prior to glucose screening and the risk of gestational diabetes: A meta-analysis. Diabetologia 2015, 58, 2229–2237. [Google Scholar] [CrossRef] [Green Version]
- Chu, S.Y.; Callaghan, W.M.; Kim, S.Y.; Schmid, C.H.; Lau, J.; England, L.J.; Dietz, P.M. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care 2007, 30, 2070–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzger, B.E.; Contreras, M.; Sacks, D.A.; Watson, W.; Dooley, S.L.; Foderaro, M.; Niznik, C.; Bjaloncik, J.; Catalano, P.M.; Dierker, L.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [PubMed] [Green Version]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine Institute of Medicine Pregnancy Weight Guidelines. National Research Council Committee to Reexamine, the National Academies Collection: Reports funded by National Institutes of Health. In Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press (US), National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- Harper, L.M.; Tita, A.; Biggio, J.R. The institute of medicine guidelines for gestational weight gain after a diagnosis of gestational diabetes and pregnancy outcomes. Am. J. Perinatol. 2015, 32, 239–246. [Google Scholar] [PubMed] [Green Version]
- Feig, D.S.; Palda, V.A. Type 2 diabetes in pregnancy: A growing concern. Lancet 2002, 359, 1690–1692. [Google Scholar] [CrossRef]
- NICE. Diabetes in Pregnancy: Management from Preconception to the Postnatal Period; National Institute of Clinical Excellence (NICE) guideline NG32015: London, UK, 2015. [Google Scholar]
- Macdonald-Wallis, C.; Tilling, K.; Fraser, A.; Nelson, S.M.; Lawlor, D.A. Gestational weight gain as a risk factor for hypertensive disorders of pregnancy. Am. J. Obstet. Gynecol. 2013, 209, 327.e1–327.e17. [Google Scholar] [CrossRef]
- Black, M.H.; Sacks, D.A.; Xiang, A.H.; Lawrence, J.M. The relative contribution of prepregnancy overweight and obesity, gestational weight gain, and IADPSG-defined gestational diabetes mellitus to fetal overgrowth. Diabetes Care 2013, 36, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Alberico, S.; Montico, M.; Barresi, V.; Monasta, L.; Businelli, C.; Soini, V.; Erenbourg, A.; Ronfani, L.; Maso, G. The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: Results from a prospective multicentre study. BMC Pregnancy Childbirth 2014, 14, 23. [Google Scholar] [CrossRef] [Green Version]
- Hartley, E.; McPhie, S.; Skouteris, H.; Fuller-Tyszkiewicz, M.; Hill, B. Psychosocial risk factors for excessive gestational weight gain: A systematic review. Women Birth 2015, 28, e99–e109. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Siminerio, L.L.; Himes, K.P.; Hutcheon, J.A.; Lash, T.L.; Parisi, S.M.; Abrams, B. Maternal obesity and gestational weight gain are risk factors for infant death. Obes. (Silver Spring) 2016, 24, 490–498. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zhang, C.; Zhang, S.; Wang, L.; Leng, J.; Liu, D.; Fang, H.; Li, W.; Yu, Z.; Yang, X.; et al. Prepregnancy body mass index and weight change on postpartum diabetes risk among gestational diabetes women. Obes. (Silver Spring) 2014, 22, 1560–1567. [Google Scholar] [CrossRef]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef]
- Fraser, A.; Nelson, S.M.; Macdonald-Wallis, C.; Sattar, N.; Lawlor, D.A. Hypertensive disorders of pregnancy and cardiometabolic health in adolescent offspring. Hypertension 2013, 62, 614–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karachaliou, M.; Georgiou, V.; Roumeliotaki, T.; Chalkiadaki, G.; Daraki, V.; Koinaki, S.; Dermitzaki, E.; Sarri, K.; Vassilaki, M.; Kogevinas, M.; et al. Association of trimester-specific gestational weight gain with fetal growth, offspring obesity, and cardiometabolic traits in early childhood. Am. J. Obstet. Gynecol. 2015, 212, 502.e1–502.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, J.R.; Perng, W.; Kleinman, K.P.; Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Oken, E. Associations of trimester-specific gestational weight gain with maternal adiposity and systolic blood pressure at 3 and 7 years postpartum. Am. J. Obstet. Gynecol. 2015, 212, 499.e1–499.e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalano, P.M.; Mele, L.; Landon, M.B.; Ramin, S.M.; Reddy, U.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. Inadequate weight gain in overweight and obese pregnant women: What is the effect on fetal growth? Am. J. Obstet. Gynecol. 2014, 211, 137.e1–137.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yee, L.M.; Cheng, Y.W.; Inturrisi, M.; Caughey, A.B. Gestational weight loss and perinatal outcomes in overweight and obese women subsequent to diagnosis of gestational diabetes mellitus. Obes. (Silver Spring) 2013, 21, E770–E774. [Google Scholar] [CrossRef]
- Yamamoto, J.M.; Kellett, J.E.; Balsells, M.; García-Patterson, A.; Hadar, E.; Solà, I.; Gich, I.; van der Beek, E.M.; Castañeda-Gutiérrez, E.; Heinonen, S.; et al. Gestational Diabetes Mellitus and Diet: A Systematic Review and Meta-analysis of Randomized Controlled Trials Examining the Impact of Modified Dietary Interventions on Maternal Glucose Control and Neonatal Birth Weight. Diabetes Care 2018, 41, 1346–1361. [Google Scholar] [CrossRef] [Green Version]
- Andreasyan, K.; Ponsonby, A.L.; Dwyer, T.; Morley, R.; Riley, M.; Dear, K.; Cochrane, J. Higher Maternal Dietary Protein Intake in Late Pregnancy Is Associated with a Lower Infant Ponderal Index at Birth. Eur. J. Clin. Nutr. 2007, 61, 498–508. [Google Scholar] [CrossRef] [Green Version]
- Food Products—Determination of the Glycaemic index (GI) and Recommendation for Food Classification. Available online: https://www.iso.org/standard/43633.html (accessed on 27 February 2020).
- Foods to Avoid in Pregnancy. Available online: https://www.nhs.uk/conditions/pregnancy-and-baby/foods-to-avoid-pregnant (accessed on 3 March 2020).
- Pregnancy. Available online: https://www.nhs.uk/common-health-questions/pregnancy/ (accessed on 4 March 2020).
- World Health Organization. Vitamin and Mineral Requirements in Human Nutrition. 2004. Available online: https://apps.who.int/iris/bitstream/handle/10665/42716/9241546123.pdf?ua=1 (accessed on 12 January 2020).
- Vitamins, Supplements and Nutrition in Pregnancy—Your Pregnancy and Baby Guide. Available online: https://www.nhs.uk/conditions/pregnancy-and-baby/vitamins-minerals-supplements-pregnant/ (accessed on 21 February 2020).
- World Health Organization. Guideline: Calcium Supplementation in Pregnant Women. 2013. Available online: https://apps.who.int/iris/bitstream/handle/10665/85120/9789241505376_eng.pdf;jsessionid=599A5A44F7B610DBBA7EC959792C678F?sequence=1 (accessed on 2 February 2020).
- Karlsson, J.; Persson, L.O.; Sjöström, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1715–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, E.; Lee, C.; Imamura, F.; Hollidge, S.E.; Westgate, K.L.; Venables, M.C.; Poliakov, I.; Rowland, M.K.; Osadchiy, T.; Bradley, J.C.; et al. Validity and reliability of an online self-report 24-h dietary recall method (Intake24): A doubly labelled water study and repeated-measures analysis. J. Nutr. Sci. 2019, 8, e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, H.; Cole, T. lmsGrowth, a Microsoft Excel Add-In to Access Growth References Based on the LMS Method (Version 2.68). 2009. Available online: http://www.healthforallchildren.co.uk/ (accessed on 2 March 2020).
- Gestation Network; Centile Calculator. Available online: https://www.gestation.net/cc/about.htm (accessed on 14 February 2020).
- The International Fetal and Newborn Growth Consortium for the 21st Century. Available online: https://intergrowth21.tghn.org/ (accessed on 23 March 2020).
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations from the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiken, C.E.M.; Hone, L.; Murphy, H.R.; Meek, C.L. Improving outcomes in gestational diabetes: Does gestational weight gain matter? Diabet. Med. 2019, 36, 167–176. [Google Scholar] [CrossRef]
- Stein, A.D.; Ravelli, A.C.; Lumey, L.H. Famine, third-trimester pregnancy weight gain, and intrauterine growth: The Dutch Famine Birth Cohort Study. Hum. Biol. 1995, 67, 135–150. [Google Scholar]
- Vandraas, K.F.; Vikanes, Å.V.; Vangen, S.; Magnus, P.; Støer, N.C.; Grjibovski, A.M. Hyperemesis gravidarum and birth outcomes-a population-based cohort study of 2.2 million births in the Norwegian Birth Registry. BJOG 2013, 120, 1654–1660. [Google Scholar] [CrossRef] [Green Version]
- Hodson, K.; Dalla Man, C.; Smith, F.E.; Barnes, A.; McParlin, C.; Cobelli, C.; Robson, S.C.; Araújo-Soares, V.; Taylor, R. Liver triacylglycerol content and gestational diabetes: Effects of moderate energy restriction. Diabetologia 2017, 60, 306–313. [Google Scholar] [CrossRef] [Green Version]
- Weaver, C.M.; Miller, J.W. Challenges in conducting clinical nutrition research. Nutr. Rev. 2017, 75, 491–499. [Google Scholar] [CrossRef]
- Mahabir, S.; Baer, D.J.; Giffen, C.; Subar, A.; Campbell, W.; Hartman, T.J.; Clevidence, B.; Albanes, D.; Taylor, P.R. Calorie intake misreporting by diet record and food frequency questionnaire compared to doubly labeled water among postmenopausal women. Eur. J. Clin. Nutr. 2006, 60, 561–565. [Google Scholar] [CrossRef]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101 (Suppl. 2), S73–S85. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Weekday | Breakfast | Lunch | Dinner | Snack Pack |
|---|---|---|---|---|
| Monday | Porridge with nuts and jam | Chilli bean wrap | Turkey roast | Boiled egg, satsuma, small cheese |
| Tuesday | Cheese and ham omelette with rosti | Mushroom stroganoff with rice | Macaroni cheese with kale | Apple, Belgian Chocolate covered rice cake, spiced seeds |
| Wednesday | Breakfast roll | Chicken schnitzel, wedges, and green beans | Venison sausage in red wine sauce with sprouts | Cottage cheese, Ryvita, satsuma |
| Thursday | Spiced omelette with Sag Aloo | Seafood lasagne | Beef madras with rice | Peperami (mini), orange, Belgian chocolate rice cake |
| Friday | Blueberry yogurt | Edamame and feta wrap | Salmon with lemon Puy lentils | Peperami (mini), pear, spiced seeds, popcorn |
| Saturday | Granola | Spiced Moroccan chicken wrap | Fish goujon, wedges, and minted peas | Small cheese, apple, Philadelphia snack light herbs, and breadsticks |
| Sunday | Cheese and mushroom omelette | Thai red chicken curry with rice | Vegetarian bean stew, rice, and halloumi | Satsuma, Belgian chocolate covered rice cake, spiced seeds |
| Weekly Veg/Salad Pack | Contains a range of vegetables and salad options including carrots, broccoli, cauliflower, baby tomatoes, cucumber, lettuce, celery, and red pepper | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusinski, L.C.; Murphy, H.R.; De Lucia Rolfe, E.; Rennie, K.L.; Oude Griep, L.M.; Hughes, D.; Taylor, R.; Meek, C.L. Dietary Intervention in Pregnant Women with Gestational Diabetes; Protocol for the DiGest Randomised Controlled Trial. Nutrients 2020, 12, 1165. https://doi.org/10.3390/nu12041165
Kusinski LC, Murphy HR, De Lucia Rolfe E, Rennie KL, Oude Griep LM, Hughes D, Taylor R, Meek CL. Dietary Intervention in Pregnant Women with Gestational Diabetes; Protocol for the DiGest Randomised Controlled Trial. Nutrients. 2020; 12(4):1165. https://doi.org/10.3390/nu12041165
Chicago/Turabian StyleKusinski, Laura C., Helen R. Murphy, Emanuella De Lucia Rolfe, Kirsten L. Rennie, Linda M. Oude Griep, Deborah Hughes, Roy Taylor, and Claire L. Meek. 2020. "Dietary Intervention in Pregnant Women with Gestational Diabetes; Protocol for the DiGest Randomised Controlled Trial" Nutrients 12, no. 4: 1165. https://doi.org/10.3390/nu12041165