Nutritional Intake Influences Zinc Levels in Preterm Newborns: An Observational Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Zinc Levels Measurement
2.3. Data Collection
2.4. Nutritional Protocol
2.5. Ethics
2.6. Statistical Analysis
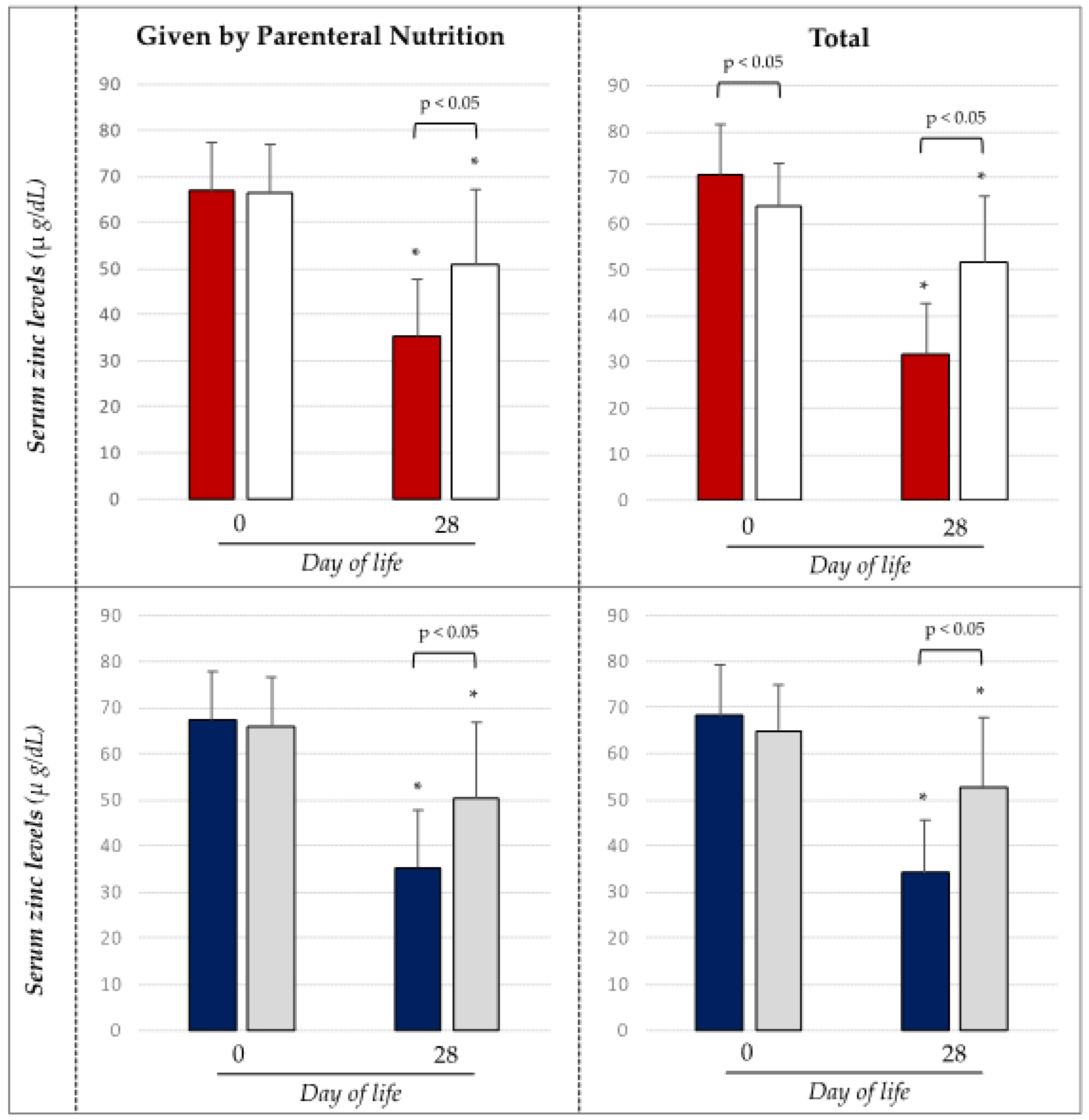
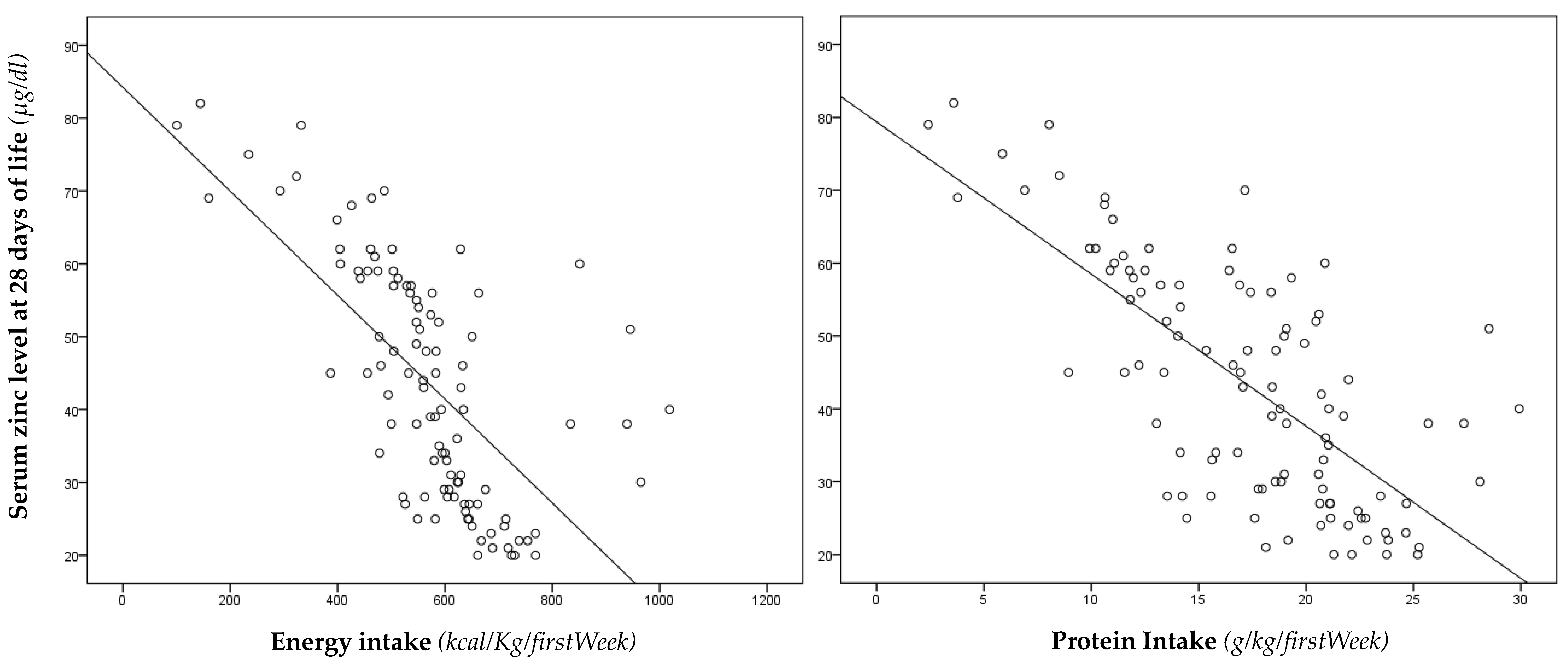
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- King, J.C. Zinc: An essential but elusive nutrient. Am. J. Clin. Nutr. 2011, 94, 679S–684S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrin, G.; Berni Canani, R.; Di Chiara, M.; Pietravalle, A.; Aleandri, V.; Conte, F.; De Curtis, M. Zinc in Early Life: A Key Element in the Fetus and Preterm Neonate. Nutrients 2015, 7, 10427–10446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallee, B.L.; Auld, D.S. Zinc coordination, function, and structure of zinc enzymes and other proteins. Biochemistry 1990, 29, 5647–5659. [Google Scholar] [CrossRef] [PubMed]
- Hambide, K.M.; Krebs, N.F. Zinc in the Fetus and Neonate; Elsevier: Saybders, PA, USA, 2004; Volume Fetal Neonatal Physiology. [Google Scholar]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clin. Nutr. 2018, 37, 2309–2314. [Google Scholar] [CrossRef] [PubMed]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; Sainz de Pipaon, M.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonsante, F.; Iacobelli, S.; Latorre, G.; Rigo, J.; De Felice, C.; Robillard, P.Y.; Gouyon, J.B. Initial Amino Acid Intake Influences Phosphorus and Calcium Homeostasis in Preterm Infants—It Is Time to Change the Composition of the Early Parenteral Nutrition. PLoS ONE 2013, 8, e72880. [Google Scholar] [CrossRef]
- Gagliardi, L.; Rusconi, F.; Bellu, R.; Zanini, R.; De Curtis, M. The Italian Neonatal Network Association of Maternal Hypertension and Chorioamnionitis with Preterm Outcomes. Pediatrics 2014, 134, e154–e161. [Google Scholar] [CrossRef]
- Terrin, G.; Passariello, A.; Manguso, F.; Salvia, G.; Rapacciuolo, L.; Messina, F.; Raimondi, F.; Canani, R.B. Serum Calprotectin: An Antimicrobial Peptide as a New Marker for the Diagnosis of Sepsis in Very Low Birth Weight Newborns. Clin. Dev. Immunol. 2011, 2011, 1–6. [Google Scholar] [CrossRef]
- Neu, J.; Walker, W.A. Necrotizing Enterocolitis. N. Engl. J. Med. 2011, 364, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Naeem, A.; Ahmed, I.; Silveyra, P. Bronchopulmonary Dysplasia: An Update on Experimental Therapeutics. Eur. Med. J. Chelmsf. Engl. 2019, 4, 20–29. [Google Scholar]
- Whitelaw, A. Intraventricular haemorrhage and posthaemorrhagic hydrocephalus: Pathogenesis, prevention and future interventions. Semin. Neonatol. 2001, 6, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, C.L. Retinopathy of Prematurity. Semin. Ophthalmol. 2008, 23, 318–323. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Committee on Fetus and Newborn Hospital Discharge of the High-Risk Neonate. Pediatrics 2008, 122, 1119–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.L.; Engstrom, J.L.; Meier, P.P.; Jegier, B.J.; Kimura, R.E. Calculating postnatal growth velocity in very low birth weight (VLBW) premature infants. J. Perinatol. 2009, 29, 618–622. [Google Scholar] [CrossRef] [Green Version]
- Terrin, G.; Passariello, A.; Canani, R.B.; Manguso, F.; Paludetto, R.; Cascioli, C. Minimal enteral feeding reduces the risk of sepsis in feed-intolerant very low birth weight newborns. Acta Paediatr. 2009, 98, 31–35. [Google Scholar] [CrossRef]
- Lin, P.W.; Stoll, B.J. Necrotising enterocolitis. Lancet 2006, 368, 1271–1283. [Google Scholar] [CrossRef]
- Hunter, C.J.; Upperman, J.S.; Ford, H.R.; Camerini, V. Understanding the Susceptibility of the Premature Infant to Necrotizing Enterocolitis (NEC). Pediatr. Res. 2008, 63, 117–123. [Google Scholar] [CrossRef]
- Elstgeest, L.E.; Martens, S.E.; Lopriore, E.; Walther, F.J.; te Pas, A.B. Does Parenteral Nutrition Influence Electrolyte and Fluid Balance in Preterm Infants in the First Days after Birth? PLoS ONE 2010, 5, e9033. [Google Scholar] [CrossRef] [Green Version]
- Iacobelli, S.; Bonsante, F.; Gouyon, J.B. Fluid and electrolyte intake during the first week of life in preterm infants receiving parenteral nutrition according current guidelines. Minerva Pediatr. 2010, 62, 203–204. [Google Scholar]
- Mizumoto, H.; Mikami, M.; Oda, H.; Hata, D. Refeeding syndrome in a small-for-dates micro-preemie receiving early parenteral nutrition: Refeeding syndrome in a SGA micro-preemie. Pediatr. Int. 2012, 54, 715–717. [Google Scholar] [CrossRef]
- Marinella, M.A. Refeeding Syndrome: Implications for the Inpatient Rehabilitation Unit. Am. J. Phys. Med. Rehabil. 2004, 83, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Hanas, J.S.; Hazuda, D.J.; Bogenhagen, D.F.; Wu, F.Y.; Wu, C.W. Xenopus transcription factor A requires zinc for binding to the 5 S RNA gene. J. Biol. Chem. 1983, 258, 14120–14125. [Google Scholar] [PubMed]
- Miller, J.; McLachlan, A.D.; Klug, A. Repetitive zinc-binding domains in the protein transcription factor IIIA from Xenopus oocytes. EMBO J. 1985, 4, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Shang, Z.; Liao, Y.D.; Wu, F.Y.; Wu, C.W. Zinc release from Xenopus transcription factor IIIA induced by chemical modifications. Biochemistry 1989, 28, 9790–9795. [Google Scholar] [CrossRef]
- Fukada, T.; Yamasaki, S.; Nishida, K.; Murakami, M.; Hirano, T. Zinc homeostasis and signaling in health and diseases: Zinc signaling. J. Biol. Inorg. Chem. JBIC Publ. Soc. Biol. Inorg. Chem. 2011, 16, 1123–1134. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, R.S. The Role of Zinc in Growth and Cell Proliferation. J. Nutr. 2000, 130, 1500S–1508S. [Google Scholar] [CrossRef] [Green Version]
- Shaw, J.C.L. Trace Elements in the Fetus and Young Infant. Am. J. Dis. Child. 1979, 133, 1260–1268. [Google Scholar] [CrossRef]
- Gibson, R.S.; De Wolfe, M.S. Changes in serum zinc concentrations of some Canadian full term and low birthweight infants from birth to six months. Acta Paediatr. Scand. 1981, 70, 497–500. [Google Scholar] [CrossRef]
- Tyrala, E.E.; Manser, J.I.; Brodsky, N.L.; Tran, N. Serum zinc concentrations in growing premature infants. Acta Paediatr. Scand. 1983, 72, 695–698. [Google Scholar] [CrossRef]
- McMaster, D.; Lappin, T.R.J.; Halliday, H.L.; Patterson, C.C. Serum Copper and Zinc Levels in the Preterm Infant. Neonatology 1983, 44, 108–113. [Google Scholar] [CrossRef]
- Hemalatha, P.; Bhaskaram, P.; Kumar, P.A.; Khan, M.M.; Islam, M.A. Zinc status of breastfed and formula-fed infants of different gestational ages. J. Trop. Pediatr. 1997, 43, 52–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, E.; Doyle, L.W. Zinc in Extremely Low-birthweight or Very Preterm Infants. NeoReviews 2007, 8, e165–e172. [Google Scholar] [CrossRef]
- Picciano, M.F.; Guthrie, H.A. Copper, iron, and zinc contents of mature human milk. Am. J. Clin. Nutr. 1976, 29, 242–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walravens, P.A.; Chakar, A.; Mokni, R.; Lemonnier, D.; Denise, J. Zinc supplements in breastfed infants. Lancet 1992, 340, 683–685. [Google Scholar] [CrossRef]
- Castillo-Durán, C.; Rodríguez, A.; Venegas, G.; Alvarez, P.; Icaza, G. Zinc supplementation and growth of infants born small for gestational age. J. Pediatr. 1995, 127, 206–211. [Google Scholar] [CrossRef]
- Schanler, R.J.; Shulman, R.J.; Prestridge, L.L. Parenteral nutrient needs of very low birth weight infants. J. Pediatr. 1994, 125, 961–968. [Google Scholar] [CrossRef]
- Terrin, G.; Berni Canani, R.; Passariello, A.; Messina, F.; Conti, M.G.; Caoci, S.; Smaldore, A.; Bertino, E.; De Curtis, M. Zinc supplementation reduces morbidity and mortality in very-low-birth-weight preterm neonates: A hospital-based randomized, placebo-controlled trial in an industrialized country. Am. J. Clin. Nutr. 2013, 98, 1468–1474. [Google Scholar] [CrossRef]
- Passariello, A.; Terrin, G.; Cecere, G.; Micillo, M.; Marco, G.; Di Costanzo, M.; Cosenza, L.; Leone, L.; Nocerino, R.; Berni Canani, R. Randomised clinical trial: Efficacy of a new synbiotic formulation containing Lactobacillus paracasei B21060 plus arabinogalactan and xilooligosaccharides in children with acute diarrhoea. Aliment. Pharmacol. Ther. 2012, 35, 782–788. [Google Scholar] [CrossRef]
- Sjöström, E.S.; Öhlund, I.; Ahlsson, F.; Domellöf, M. Intakes of Micronutrients Are Associated with Early Growth in Extremely Preterm Infants. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 885–892. [Google Scholar] [CrossRef]
- Kojima, C.; Shoji, H.; Ikeda, N.; Kitamura, T.; Hisata, K.; Shimizu, T. Association of zinc and copper with clinical parameters in the preterm newborn. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2017, 59, 1165–1168. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. 103 | |
|---|---|
| Antenatal steroids a, No. (%) | 58 (56.3) |
| Gestational age, weeks | 31.5 ± 2.8 |
| Birth weight, g | 1634 ± 561 |
| Length at birth, cm | 44.5 ± 37.1 |
| Head circumference at birth, cm | 29.1 ± 2.8 |
| Cesarean section, No. (%) | 89 (86.4) |
| Male sex, No. (%) | 57 (55.3) |
| Twins, No. (%) | 29 (28.2) |
| 1-min Apgar score | 6 ± 2 |
| 5-min Apgar score | 8 ± 1 |
| pH at birth | 7.2 ± 0.5 |
| Base excess on cord blood, mmol/L | −5.0 ± 4.8 |
| CRIB II score b | 3.0 ± 3.6 |
| Exclusively breast milk at 28 days of life, No (%) | 9 (8.7) |
| Morbidity overall, No (%) | 28 (27.2) |
| NEC, No (%) | 2 (1.9) |
| IVH, No (%) | 5 (4.9) |
| PLV, No (%) | 1 (1.0) |
| Sepsis proven by positive cultures, No (%) | 5 (4.9) |
| ROP, No. (%) | 15 (14.6) |
| BPD, No. (%) | 6 (5.8) |
| Anaemia of prematurity, No. (%) | 19 (18.4) |
| PDA, No (%) | 16 (15.5) |
| Mortality, No (%) | 2 (1.9) |
| Body Birth Weight < 1500 g | Body Birth Weight ≥ 1500 g | p | |
|---|---|---|---|
| (No. 41) | (No. 62) | ||
| Zinc at birth, µg/dL | 66.6 ± 10.3 * | 66.6 ± 10.8 * | 0.983 |
| Zinc at 28 days of life, µg/dL | 37.5 ± 13.5 | 47.2 ± 17.1 | 0.003 |
| Decrease in Zinc ** | 0.4 ± 0.2 | 0.3 ± 0.3 | 0.005 |
| Parenteral Nutrition Energy Intake, kcal/Kg/day | 526.8 ± 103.8 | 151.1 ± 232.7 | <0.001 |
| Total Energy Intake, kcal/Kg/day | 631.1 ± 135.3 | 533.4 ± 151.4 | 0.001 |
| Parenteral Nutrition Protein intake, g/Kg/day | 18.7 ± 3.9 | 4.9 ± 7.7 | <0.001 |
| Total Protein intake, g/Kg/day | 21.2 ± 3.6 | 14.5 ± 5.0 | <0.001 |
| Growth Velocity #, g/Kg/day | 11.5 ± 2.8 | 4.0 ± 7.3 | < 0.001 |
| Decrease in Zinc ** in Newborns Receiving High Intake in the First Week of Life | Decrease in Zinc ** in Newborns Receiving Low Intake in the First Week of Life | p | |
|---|---|---|---|
| Calculated on Energy intake through Parenteral Nutrition | 0.4 ± 0.2 | 0.2 ± 0.2 | <0.001 |
| Calculated on Total Energy intake | 0.5 ± 0.2 | 0.2 ± 0.2 | <0.001 |
| Calculated on Protein intake through Parenteral Nutrition | 0.5 ± 0.2 | 0.2 ± 0.2 | <0.001 |
| Calculated on Total Protein intake | 0.5 ± 0.2 | 0.2 ± 0.2 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terrin, G.; Boscarino, G.; Di Chiara, M.; Iacobelli, S.; Faccioli, F.; Greco, C.; Onestà, E.; Sabatini, G.; Pietravalle, A.; Oliva, S.; et al. Nutritional Intake Influences Zinc Levels in Preterm Newborns: An Observational Study. Nutrients 2020, 12, 529. https://doi.org/10.3390/nu12020529
Terrin G, Boscarino G, Di Chiara M, Iacobelli S, Faccioli F, Greco C, Onestà E, Sabatini G, Pietravalle A, Oliva S, et al. Nutritional Intake Influences Zinc Levels in Preterm Newborns: An Observational Study. Nutrients. 2020; 12(2):529. https://doi.org/10.3390/nu12020529
Chicago/Turabian StyleTerrin, Gianluca, Giovanni Boscarino, Maria Di Chiara, Silvia Iacobelli, Francesca Faccioli, Carla Greco, Elisa Onestà, Giulia Sabatini, Andrea Pietravalle, Salvatore Oliva, and et al. 2020. "Nutritional Intake Influences Zinc Levels in Preterm Newborns: An Observational Study" Nutrients 12, no. 2: 529. https://doi.org/10.3390/nu12020529