Melanocortin-4 Receptor and Lipocalin 2 Gene Variants in Spanish Children with Abdominal Obesity: Effects on BMI-SDS after a Lifestyle Intervention

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Design
2.3. Anthropometric, Clinical and Biochemical Measurements
2.4. Physical Activity
2.5. Children Eating Behavior Questionnaire (CEBQ)
2.6. DNA Extraction
2.7. Mutation Screen
2.8. Statistical Analysis
3. Results
3.1. Description of Identified Variants
3.2. Phenotypic Description of Mutation Carriers
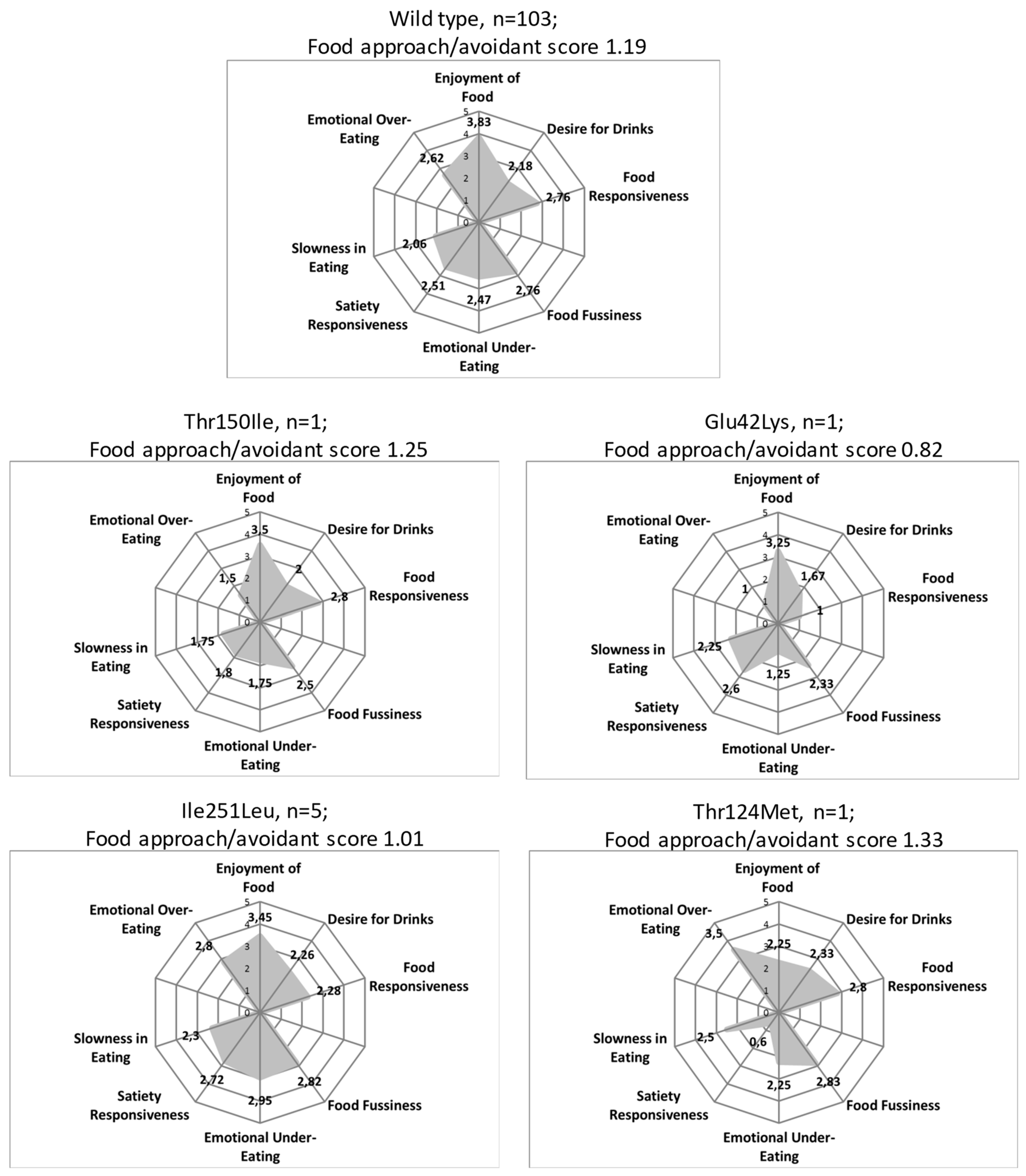
3.3. Children Eating Behavior
3.4. Change in BMI-SDS and Mutations in MC4R and LCN2 After 8-Week and 1-Year of Follow Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 June 2018).
- Loos, R.J.F. The genetic epidemiology of melanocortin 4 receptor variants. Eur. J. Pharmacol. 2011, 660, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Razquin, C.; Marti, A.; Martinez, J.A. Evidences on three relevant obesogenes: MC4R, FTO and PPARγ. Approaches for personalized nutrition. Mol. Nutr. Food Res. 2011, 55, 136–149. [Google Scholar] [CrossRef]
- Koochakpoor, G.; Hosseini-Esfahani, F.; Daneshpour, M.S.; Hosseini, S.A.; Mirmiran, P. Effect of interactions of polymorphisms in the Melanocortin-4 receptor gene with dietary factors on the risk of obesity and Type 2 diabetes: A systematic review. Diabet. Med. 2016, 33, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.; Bonnefond, A.; Manzoor, J.; Shabir, F.; Ayesha, H.; Philippe, J.; Durand, E.; Crouch, H.; Sand, O.; Ali, M.; et al. Genetic variants in LEP, LEPR, and MC4R explain 30% of severe obesity in children from a consanguineous population. Obesity 2015, 23, 1687–1695. [Google Scholar] [CrossRef] [PubMed]
- Zlatohlavek, L.; Hubacek, J.A.; Vrablik, M.; Pejsova, H.; Lanska, V.; Ceska, R. The Impact of Physical Activity and Dietary Measures on the Biochemical and Anthropometric Parameters in Obese Children. Is There Any Genetic Predisposition? Cent. Eur. J. Public Health 2015, 23. [Google Scholar] [CrossRef]
- Hinney, A.; Volckmar, A.-L.; Knoll, N. Chapter Five - Melanocortin-4 Receptor in Energy Homeostasis and Obesity Pathogenesis. In G Protein-Coupled Receptors in Energy Homeostasis and Obesity Pathogenesis, 1st ed.; Elsevier Inc.: New York, NY, USA, 2013; Volume 114, pp. 147–191. [Google Scholar]
- Collet, T.H.; Dubern, B.; Mokrosinski, J.; Connors, H.; Keogh, J.M.; Mendes de Oliveira, E.; Henning, E.; Poitou-Bernert, C.; Oppert, J.-M.; Tounian, P.; et al. Evaluation of a melanocortin-4 receptor (MC4R) agonist (Setmelanotide) in MC4R deficiency. Mol. Metab. 2017, 6, 1321–1329. [Google Scholar] [CrossRef]
- Lubrano-Berthelier, C.; Dubern, B.; Lacorte, J.M.; Picard, F.; Shapiro, A.; Zhang, S.; Bertrais, S.; Hercberg, S.; Basdevant, A.; Clément, K.; et al. Melanocortin 4 receptor mutations in a large cohort of severely obese adults: Prevalence, functional classification, genotype-phenotype relationship, and lack of association with binge eating. J. Clin. Endocrinol. Metab. 2006, 91, 1811–1818. [Google Scholar] [CrossRef]
- Catalán, V.; Gómez-Ambrosi, J.; Rodríguez, A.; Ramírez, B.; Valentí, V.; Moncada, R.; Silva, C.; Salvador, J.; Frühbeck, G. Peripheral mononuclear blood cells contribute to the obesity-associated inflammatory state independently of glycemic status: involvement of the novel proinflammatory adipokines chemerin, chitinase-3-like protein 1, lipocalin-2 and osteopontin. Genes Nutr. 2015, 10. [Google Scholar] [CrossRef]
- Elkhidir, A.E.; Eltaher, H.B.; Mohamed, A.O. Association of lipocalin-2 level, glycemic status and obesity in type 2 diabetes mellitus. BMC Res. Notes 2017, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Foncea, R.; Deis, J.A.; Guo, H.; Bernlohr, D.A.; Chen, X. Lipocalin 2 expression and secretion is highly regulated by metabolic stress, cytokines, and nutrients in adipocytes. PLoS ONE 2014, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mosialou, I.; Shikhel, S.; Liu, J.M.; Maurizi, A.; Luo, N.; He, Z.; Huang, Y.R.; Zong, H.H.; Friedman, R.A.; Barasch, J. MC4R-dependent suppression of appetite by bone-derived lipocalin 2. Nature 2017, 543, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Serra Majem, L.; Aranceta Bartrina, J.; Ribas Barba, L.; Pérez Rodrigo, C.; García Closas, R. Estudio enKid: objetivos y metodología. Crecimiento y desarrollo. Estudio enKid; Masson S.A.: Barcelona, Spain, 2000; Volume 4. [Google Scholar]
- Ojeda-Rodríguez, A.; Zazpe, I.; Morell-Azanza, L.; Chueca, M.J.; Azcona-Sanjulian, M.C.; Marti, A. Improved diet quality and nutrient adequacy in children and adolescents with abdominal obesity after a lifestyle intervention. Nutrients 2018, 10, 1500. [Google Scholar] [CrossRef]
- Aranceta Batrina, J.; Arija Val, V.; Maíz Aldalur, E.; de Victoria Muñoz, E.M.; Ortega Anta, R.M.; Pérez Rodrigo, C.; Quiles Izquierdo, J.; Rodríguez Martín, A.; Román Viñas, B.; Salvador i Castell, G.; et al. Guías alimentarias para la población española (SENC, diciembre 2016); la nueva pirámide de la alimentación saludable. Nutr. Hosp. 2015, 31, 1–145. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Morell-Azanza, L.; García-Calzón, S.; Rendo-Urteaga, T.; Martin-Calvo, N.; Chueca, M.; Martínez, J.A.; Azcona-Sanjulián, M.C.; Marti, A. Serum oxidized low-density lipoprotein levels are related to cardiometabolic risk and decreased after a weight loss treatment in obese children and adolescents. Pediatr. Diabetes 2017, 18, 18. [Google Scholar] [CrossRef]
- Sobradillo, B.; Aguirre, A.; Uresti, U.; Bilbao, A.; Fernández-Ramos, C.; Lizarraga, A.; Lorenzo, H.; Madariag, L.; Rica, I.; Ruiz, I.; et al. Curvas y tablas de Crecimiento. Estudios Longitudinal y Transversal. Bilbao: Fundación Faustino Orbegozo Eizaguirre. 2004. Available online: https://www.fundacionorbegozo.com/wp-content/uploads/pdf/estudios_2004.pdf (accessed on 20 January 2015).
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans—A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation 2005, 111, 697–716. [Google Scholar] [CrossRef]
- Morell-Azanza, L.; Ojeda-Rodríguez, A.; Ochotorena-Elicegui, A.; Martín-Calvo, N.; Chueca, M.; Marti, A.; Azcona-San Julian, C. Changes in objectively measured physical activity after a multidisciplinary lifestyle intervention in children with abdominal obesity: A randomized control trial. BMC Pediatr. 2019, 6–13. [Google Scholar] [CrossRef]
- Konstabel, K.; Veidebaum, T.; Verbestel, V.; Moreno, L.A.; Bammann, K.; Tornaritis, M.; Eiben, G.; Molnár, D.; Siani, A.; Sprengeler, O.; et al. Objectively measured physical activity in European children: The IDEFICS study. Int. J. Obes. 2014, 38, S135–S143. [Google Scholar] [CrossRef]
- González, A.; Martínez, J.L.S.; Santos-Martínez, J.L. Adaptación y aplicación del cuestionario de conducta de alimentación infantil CEBQ. Fundam Nutr y Dietética Bases Metod y Apl. 2011, pp. 339–344. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=6364656 (accessed on 2 March 2017).
- MutationTaster. Available online: www.mutationtaster.org (accessed on 5 April 2017).
- Xiang, Z.; Pogozheva, I.D.; Sorenson, N.B.; Wilczynski, A.M.; Holder, J.R.; Litherland, S.A.; Millard, W.J.; Mosberg, H.I.; Haskell-Luevano, C. Peptide and small molecules rescue the functional activity and agonist potency of dysfunctional human melanocortin-4 receptor polymorphisms. Biochemistry 2007, 46, 8273–8287. [Google Scholar] [CrossRef] [PubMed]
- Calton, M.A.; Ersoy, B.A.; Zhang, S.; Kane, J.P.; Malloy, M.J.; Pullinger, C.R.; Bromberg, Y.; Pennacchio, L.A.; Dent, R.; McPherson, R.; et al. Association of functionally significant Melanocortin-4 but not Melanocortin-3 receptor mutations with severe adult obesity in a large North American case-control study. Hum. Mol. Genet. 2009, 18, 1140–1147. [Google Scholar] [CrossRef]
- Thearle, M.S.; Muller, Y.L.; Hanson, R.L.; Mullins, M.; AbdusSamad, M.; Tran, J.; Knowler, W.C.; Bogardus, C.; Krakoff, J.; Baier, L.J. Greater impact of melanocortin-4 receptor deficiency on rates of growth and risk of type 2 diabetes during childhood compared with adulthood in Pima Indians. Diabetes 2012, 61, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Nowacka-Woszuk, J.; Cieslak, J.; Skowronska, B.; Majewska, K.A.; Stankiewicz, W.; Fichna, P.; Switonski, M. Missense mutations and polymorphisms of the MC4R gene in Polish obese children and adolescents in relation to the relative body mass index. J. Appl. Genet. 2011, 52, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Bonnefond, A.; Keller, R.; Meyre, D.; Stutzmann, F.; Thuillier, D.; Stefanov, D.G.; Froguel, P.; Horber, F.F.; Kral, J.G. Eating Behavior, Low-Frequency Functional Mutations in the Melanocortin-4 Receptor (MC4R) Gene, and Outcomes of Bariatric Operations: A 6-Year Prospective Study. Diabetes Care 2016, 39, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Rovite, V.; Petrovska, R.; Vaivade, I.; Kalnina, I.; Fridmanis, D.; Zaharenko, L.; Peculis, R.; Pirags, V.; Schioth, H.B.; Klovins, J. The role of common and rare MC4R variants and FTO polymorphisms in extreme form of obesity. Mol. Biol. Rep. 2014, 41, 1491–1500. [Google Scholar] [CrossRef]
- Melchior, C.; Schulz, A.; Windholz, J.; Kiess, W.; Schneberg, T.; Krner, A. Clinical and functional relevance of melanocortin-4 receptor variants in obese german children. Horm. Res. Paediatr. 2012, 78, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Koester-Weber, T.; Valtuena, J.; Breidenassel, C.; Beghin, L.; Plada, M.; Moreno, S.; Huybrechts, I.; Palacios, G.; Gomez-Martinez, S.; Albers, U.; et al. Valores de referencia para leptina, Cortisol, Insulina y glucosa entre los adolescentes europeos y su asociaciÓn con adiposidad: Estudio helena. Nutr. Hosp. 2014, 30, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Hainerova, I.; Larsen, L.H.; Holst, B.; Finkova, M. Melanocortin 4 Receptor Mutations in Obese Czech Children: Studies of Prevalence, Phenotype Development, Weight Reduction Response, and Functional Analysis. J. Clin. Endocrinol. Metab. 2007, 92, 3689–3696. [Google Scholar] [CrossRef]
- Hinney, A.; Bettecken, T.; Tarnow, P.; Brumm, H.; Reichwald, K.; Lichtner, P.; Scherag, A.; Nguyen, T.T.; Schlumberger, P.; Rief, W.; et al. Prevalence, spectrum, and functional characterization of melanocortin-4 receptor gene mutations in a representative population-based sample and obese adults from Germany. J. Clin. Endocrinol. Metab. 2006, 91, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Miraglia del Giudice, E.; Cirillo, G.; Nigro, V.; Santoro, N.; D’Urso, L.; Raimondo, P.; Cozzolino, D.; Scafato, D.; Perrone, L. Low frequency of melanocortin-4 receptor (MC4R) mutations in a Mediterranean population with early-onset obesity. Int. J. Obes. 2002, 26, 647–651. [Google Scholar] [CrossRef]
- Stutzmann, F.; Tan, K.; Vatin, V.; Dina, C.; Jouret, B.; Tichet, J.; Balkau, B.; Potoczna, N.; Horber, F.; O’Rahilly, S.; et al. Prevalence of melanocortin-4 receptor deficiency in europeans and their age-dependent penetrance in multigenerational pedigrees. Diabetes 2008, 57, 2511–2518. [Google Scholar] [CrossRef]
- Demiralp, D.O.; Berberoǧlu, M.; Akar, N. Melanocortin-4 receptor polymorphisms in Turkish pediatric obese patients. Clin. Appl. Thromb. 2011, 17, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Valladares, M.; Domínguez-Vásquez, P.; Obregón, A.M.; Weisstaub, G.; Burrows, R.; Maiz, A.; Santos, J.L. Melanocortin-4 receptor gene variants in Chilean families: Association with childhood obesity and eating behavior. Nutr. Neurosci. 2010, 13, 71–78. [Google Scholar] [CrossRef]
- Reinehr, T.; Hebebrand, J.; Friedel, S.; Toschke, A.M.; Brumm, H.; Biebermann, H.; Hinney, A. Lifestyle Intervention in Obese Children With Variations in the Melanocortin 4 Receptor Gene. Obesity 2009, 17, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Young, E.H.; Wareham, N.J.; Farooqi, S.; Hinney, A.; Hebebrand, J.; Scherag, A.; O’rahilly, S.; Barroso, I.; Sandhu, M.S. The V103I polymorphism of the MC4R gene and obesity: Population based studies and meta-analysis of 29 563 individuals. Int. J. Obes. 2007, 31, 1437–1441. [Google Scholar] [CrossRef] [PubMed]
- Stutzmann, F.; Vatin, V.; Cauchi, S.; Morandi, A.; Jouret, B.; Landt, O.; Tounian, P.; Levy-Marchal, C.; Buzzetti, R.; Pinelli, L.; et al. Non-synonymous polymorphisms in melanocortin-4 receptor protect against obesity: The two facets of a Janus obesity gene. Hum. Mol. Genet. 2007, 16, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Ma, J.; Zhang, S.; Hinney, A.; Hebebrand, J.; Wang, Y.; Wang, H.J. Association of the MC4R V103I polymorphism with obesity: A chinese case-control study and meta-analysis in 55,195 individuals. Obesity 2010, 18, 573–579. [Google Scholar] [CrossRef]
- Ochoa, M.C.; Razquin, C.; Azcona, C.; García-Fuentes, M.; Martínez, J.A. Val103Ile and Ile251Leu polymorphisms in MC4R gene in Spanish children and adolescents. Rev. Española Obes. 2005, 3, 250–272. [Google Scholar]
- Ochoa, M.C.; Azcona, C.; Biebermann, H.; Brumm, H.; Razquin, C.; Wermter, A.K.; Martínez, J.A.; Hebebrand, J.; Hinney, A.; Moreno-Aliaga, M.J.; et al. A novel mutation Thr162Arg of the melanocortin 4 receptor gene in a Spanish children and adolescent population. Clin. Endocrinol. (Oxf). 2007, 66, 652–658. [Google Scholar] [CrossRef]
- Marti, A.; Corbala, M.S.; Forga, L.; Martinez, J.A.; Hinney, A.; Hebebrand, J. A novel nonsense mutation in the melanocortin-4 receptor associated with obesity in a Spanish population. Int. J. Obes. 2003, 27, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.E.; de Melo, M.E.; Fujiwara, C.T.H.; Pioltine, M.B.; Matioli, S.R.; Santos, A.; Cercato, C.; Halpern, A.; Mancini, M.C. Associations between a common variant near the MC4R gene and serum triglyceride levels in an obese pediatric cohort. Endocrine 2015, 49, 653–658. [Google Scholar] [CrossRef]
- Ashcroft, J.; Semmler, C.; Carnell, S.; van Jaarsveld, C.H.M.; Wardle, J. Continuity and stability of eating behaviour traits in children. Eur. J. Clin. Nutr. 2008, 62, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.L.; Amador, P.; Valladares, M.; Albala, C.; Martinez, J.A.; Marti, A. Obesity and eating behaviour in a three-generation Chilean family with carriers of the Thrl50Ile mutation in the melanocortin-4 receptor gene. J. Physiol. Biochem. 2008, 64, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Zlatohlavek, L.; Vrablik, M.; Motykova, E.; Ceska, R.; Vasickova, L.; Dlouha, D.; Hubacek, J.A. FTO and MC4R gene variants determine BMI changes in children after intensive lifestyle intervention. Clin. Biochem. 2013, 46, 313–316. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Gene Subject | N° of Subjects | Aminoacid Exchange | rs Number | In-silico Prediction* | Function | Reference of Functional Analysis |
|---|---|---|---|---|---|---|
| MC4R | ||||||
| Mutations | ||||||
| Glu42Lys | 1 | p.Glu42Lys | rs776051881 | Disease causing | Not known | - |
| Thr150Ile | 1 | p.Thr150Ile | rs766665118 | Disease causing | Reduced | [9,25] |
| Arg305Gln | 1 | p.Arg305Gln | rs775382722 | Disease causing | Reduced | [26] |
| Polymorphisms | ||||||
| Ile251Leu | 5 | p.Ile251Leu | rs52820871 | Disease causing | Like wild type | [27,28,29,30,31] |
| LCN2 | ||||||
| Mutations | ||||||
| Thr124Met | 1 | p.Thr124Met | rs79993583 | Probably harmless | - | - |
| MC4R Mutations | LCN2 Mutation | |||||
|---|---|---|---|---|---|---|
| Wt Population | Glu42Lys | Thr150Ile | Arg305Gln+Ile251Leu | Ile251Leu | Thr124Met | |
| N | 103 | 1 | 1 | 1 | 5 | 1 |
| Age (years) | 11.32 (2.46) | 14 | 8 | 12 | 9 (1) | 15 |
| Sex (Male/Female) | 39/64 | Female | Male | Female | 2/3 | Male |
| Tanner (I/II/III/IV/V) | 31/17/18/6/24 | V | I | II | 4/-/1/-/- | V |
| Height (cm) | 151.23 (12.72) | 168 | 137.8 | 151 | 137.3 (13.86) | 175.9 |
| Weight (Kg) | 66.71 (18.77) | 97 | 49.1 | 67.2 | 49.94 (17.87) | 112.9 |
| BMI (Kg/m2) | 28.55 (4.51) | 34.4 | 25.85 | 29.5 | 25.64 (3.53) | 36.5 |
| BMI-SDS | 2.92 (1.10) | 4.04 | 3.5 | 2.91 | 2.69 (1.05) | 4.01 |
| WHR | 0.88 (0.06) | 0.90 | 0.89 | 0.93 | 0.86 (0.04) | 0.82 |
| % fat mass | 37.22 (6.33) | 40.8 | 32.1 | 43.2 | 33.98 (9.28) | 38.7 |
| Acantosis nigricans (+/-) | 43/52 | + | - | - | 0/5 | + |
| Glucose (mg/dL) | 89.04 (6.58) | 85 | 88 | 78 | 88.25 (6.84) | 87 |
| Insulin (μu/mL) | 17.92 (13.29) | 20.2 | 7 | 13.5 | 11.87 (6.43) | 11.4 |
| HOMA-IR | 4.03 (3.17) | 4.23 | 1.52 | 2.6 | 2.66 (1.68) | 2.44 |
| Total Colesterol (mg/dL) | 162.65 (24.97) | 116 | 162 | 157 | 198.75 (14.88)* | 160 |
| HDL-colesterol (mg/dL) | 46.70 (9.96) | 42 | 53 | 46 | 56.75 (12.25) | 41 |
| LDL-colesterol (mg/dL) | 97.67 (21.15) | 64 | 96 | 97 | 125.75 (16.82)* | 99 |
| Triglycerides (mg/dL) | 94.48 (44.73) | 49 | 64 | 68 | 81.25 ( 41.65) | 98 |
| Leptin (ng/mL) | 36.41 (18.60) | 90.8 | 14 | NA | 33.52 (13.11) | 8.1 |
| MVPA (min/day) | 44.88 (23.69) | 37.5 | 50.65 | 30.93 | 44.55 (18.37) | 120.92 |
| CEBQ ratio | 1.22 (0.42) | 0.82 | 1.25 | NA | 1.01 (0.12) | 0.85 |
| ΔBMI-SDS | |||||
|---|---|---|---|---|---|
| 8 Week | 1 Year | ||||
| Mutation Carriers | Non Carriers | Mutation Carriers | Non Carriers | ||
| Usual Care Group | n = 27 −0.44 (0.66)*** | n = 22 −0.47 (0.52)*** | |||
| MC4R: Glu42Lys | − 0.51 | Drop out | |||
| MC4R: Thr150Ile | −0.67 | −0.90 | |||
| Intensive Care group | n = 68 −0.51 (0.38)*** | n = 56 −0.60 (0.72)*** | |||
| MC4R: Arg305Gln + Ile251Leu | −0.13 | −0.81 | |||
| MC4R: Ile251Leu | Mean (n = 5) | −0.74 (0.41)** | −1.02 (1.21) | ||
| Carrier 1 | −0.95 | −1.47 | |||
| Carrier 2 | −0.10 | 0.07 | |||
| Carrier 3 | −0.56 | 0.38 | |||
| Carrier 4 | −1.14 | −1.56 | |||
| Carrier 5 | −0.97 | −2.53 | |||
| LCN2: Thr124Met | −0.59 | Drop out | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morell-Azanza, L.; Ojeda-Rodríguez, A.; Giuranna, J.; Azcona-SanJulián, M.C.; Hebebrand, J.; Marti, A.; Hinney, A. Melanocortin-4 Receptor and Lipocalin 2 Gene Variants in Spanish Children with Abdominal Obesity: Effects on BMI-SDS after a Lifestyle Intervention. Nutrients 2019, 11, 960. https://doi.org/10.3390/nu11050960
Morell-Azanza L, Ojeda-Rodríguez A, Giuranna J, Azcona-SanJulián MC, Hebebrand J, Marti A, Hinney A. Melanocortin-4 Receptor and Lipocalin 2 Gene Variants in Spanish Children with Abdominal Obesity: Effects on BMI-SDS after a Lifestyle Intervention. Nutrients. 2019; 11(5):960. https://doi.org/10.3390/nu11050960
Chicago/Turabian StyleMorell-Azanza, Lydia, Ana Ojeda-Rodríguez, Johanna Giuranna, Mª Cristina Azcona-SanJulián, Johannes Hebebrand, Amelia Marti, and Anke Hinney. 2019. "Melanocortin-4 Receptor and Lipocalin 2 Gene Variants in Spanish Children with Abdominal Obesity: Effects on BMI-SDS after a Lifestyle Intervention" Nutrients 11, no. 5: 960. https://doi.org/10.3390/nu11050960