Description of Child and Adolescent Beverage and Anthropometric Measures According to Adolescent Beverage Patterns

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Participants
2.3. Beverage Intakes
2.4. Anthropometric Measures
2.5. Statistical Analyses
3. Results
3.1. Demographics
3.2. Beverage Intakes
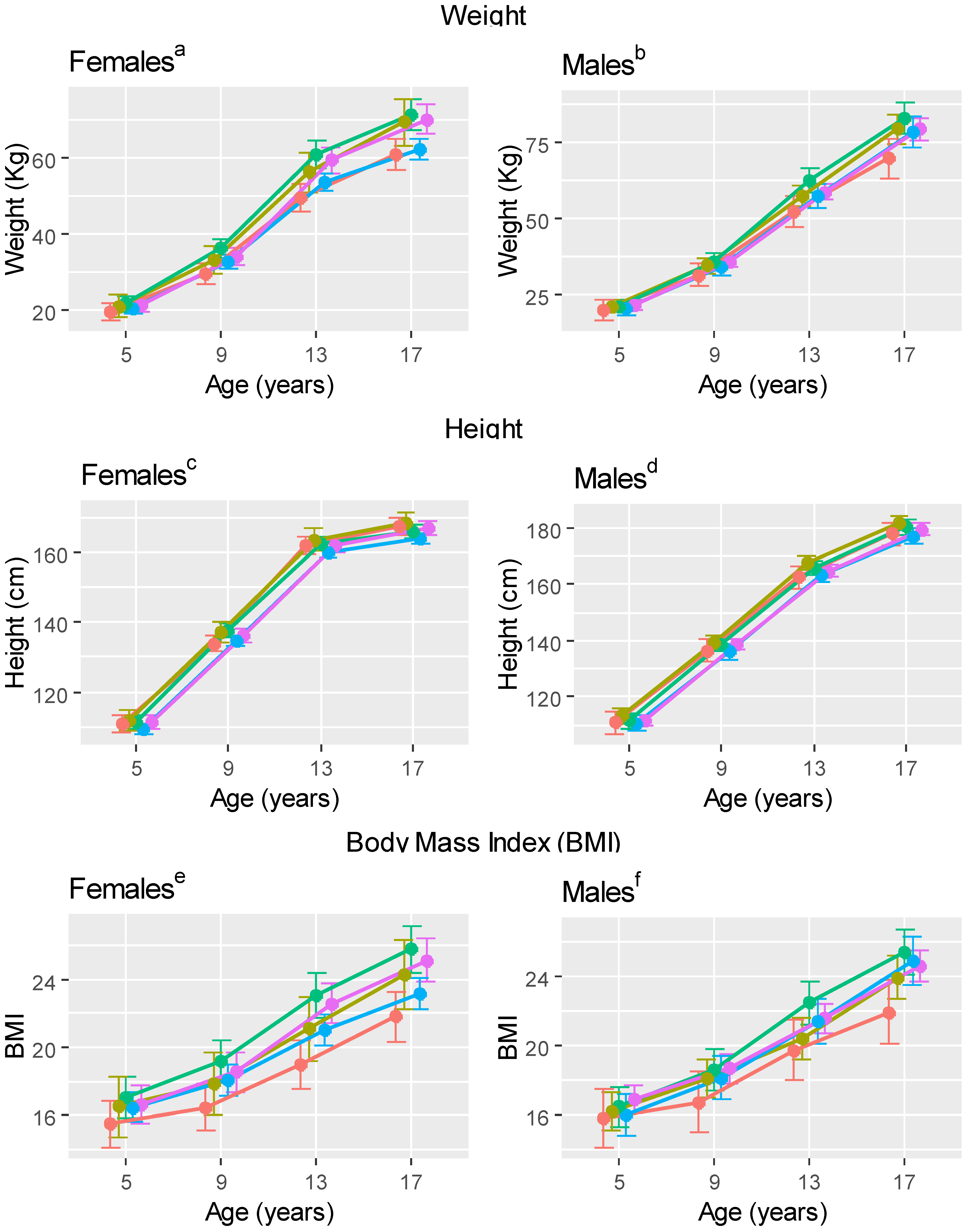
3.3. Anthropometrics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cespedes, E.M.; Hu, F.B.; Redline, S.; Rosner, B.; Gillman, M.W.; Rifas-Shiman, S.L.; Taveras, E.M. Chronic insufficient sleep and diet quality: Contributions to childhood obesity. Obesity 2016, 24, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Grasgruber, P.; Cacek, J.; Kalina, T.; Sebera, M. The role of nutrition and genetics as key determinants of the positive height trend. Econ. Hum. Biol. 2014, 15, 81–100. [Google Scholar] [CrossRef] [PubMed]
- Sudfeld, C.R.; McCoy, D.C.; Danaei, G.; Fink, G.; Ezzati, M.; Andrews, K.G.; Fawzi, W.W. Linear growth and child development in low- and middle-income countries: A meta-analyses. J. Pediatr. 2015, 135, e1266–e1275. [Google Scholar] [CrossRef] [PubMed]
- Afeiche, M.; Peterson, K.E.; Sanchez, B.N.; Schnaas, L.; Cantonwine, D.; Ettinger, A.S.; Solano-González, M.; Hernández-Avila, M.; Hu, H.; Téllez-Rojo, M.M. Windows of lead exposure sensitivity, attained height and body mass index at 48 months. J. Pediatr. 2010, 160, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Della Torre, S.B. Sugar-sweetened beverages and obesity among children and adolescents: A review of systematic literature reviews. Child. Obes. 2015, 11, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; Thompson, D.; Affenito, S.G.; Franko, D.L.; Obarzanek, E.; Barton, B.A.; Crawford, P.B. Correlates of beverage intake in adolescent girls: The National Heart, Lung, and Blood Institute Growth and Health Study. J. Pediatr. 2006, 148, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, A. Protein and micronutrient intakes are associated with child growth and morbidity from infancy to adulthood in the Philippines. J. Nutr. 2016, 146, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. J. Am. Med. Assoc. 2016, 315, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Fryar, C.C.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in obesity and severe obesity prevalence in U.S. youth and adults by sex and age, 2007–2008 to 2015–2016 (Research Letter). JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of obesity and severe obesity in U.S. children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed]
- Going, S.B.; Lohman, T.G.; Cussler, E.C.; Williams, D.P.; Morrison, J.A.; Horn, P.S. Percent body fat and chronic disease risk factor in U.S. children and youth. Am. J. Prev. Med. 2011, 41, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Messiah, S.E.; Vidot, D.C.; Gurnurkar, S.; Alhezayen, R.; Natale, R.A.; Arheart, K.L. Obesity is significantly associated with cardiovascular disease risk factors in 2- to 9- year olds. J. Clin. Hypertens. (Greenwich) 2014, 16, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Rippe, J.M.; Angelopoulos, T.J. Relationship between added sugars consumption and chronic disease risk factors: Current understanding. Nutrients 2016, 8, 697. [Google Scholar] [CrossRef] [PubMed]
- Marshall, T.A.; Van Buren, J.M.; Warren, J.J.; Cavanaugh, J.J.; Levy, S.M. Beverage consumption patterns at age 13–17 are associated with weight, height, and BMI at age 17. J. Acad. Nutr. Diet. 2017, 117, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Overweight and Obesity. U.S. Department of Health and Human Services. Available online: https://www.cdc.gov/growthcharts/clinical_charts.htm (accessed on 1 May 2018).
- Marshall, T.A.; Eichenberger Gilmore, J.M.; Broffitt, B.; Levy, S.M.; Stumbo, P.H. Relative validity of a beverage frequency questionnaire in children ages 6 months through 5 years using 3-day food and beverage diaries. J. Am. Diet. Assoc. 2003, 103, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Marshall, T.A.; Eichenberger Gilmore, J.M.; Broffitt, B.; Stumbo, P.H.; Levy, S.M. Relative validity of the Iowa Fluoride Study targeted nutrient semi-quantitative questionnaire and the Block Kids’ Food Questionnaire for estimating beverage, calcium and vitamin D intakes by children. J. Am. Diet. Assoc. 2008, 108, 465–472. [Google Scholar] [CrossRef] [PubMed]
- The R Project for Statistical Computing. R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016; Available online: http://www.R-project.org/ (accessed on 1 May 2018).
- Ward, J. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Prentice, A.; Schoenmakers, I.; Laskey, M.A.; De Bono, S.; Ginty, F.; Goldberg, G.R. Symposium on “nutrition and health in children and adolescents” Session 1: Nutrition and growth and development. Proc. Nutr. Soc. 2006, 65, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, M.; Brantsaeter, A.L.; Haugen, M.; Meltzer, H.M.; Nystad, W.; Andersen, L.F. Changes and tracking of fruit, vegetables and sugar-sweetened beverages intake from 18 months to 7 years in the Norwegian mother and child cohort study. BMC. Public Health 2013, 13, 793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantoral, A.; Tellez-Rojo, M.M.; Ettinger, A.S.; Hu, H.; Hernandez-Avila, M.; Peterson, K. Early introduction and cumulative consumption of sugar-sweetened beverages during the pre-school period and risk of obesity at 8–14 year of age. Pediatr. Obes. 2015, 11, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Li, R.; Birch, L. Mothers’ child-feeding practices are associated with children’s sugar-sweetened beverage intake. J. Nutr. 2015, 145, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyman, M.B.; Abrams, S.A. Fruit juice in infants, children and adolescents: Current recommendations. J. Pediatr. 2017, 139, e20170967. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L., III; Quann, E.E. National trends in beverage consumption in children from birth to 5 years: Analyses of NHANES across three decades. Nutr. J. 2012, 11, 92. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among children age 4–13y in the United States: Analyses of 2005–2010 NHANES data. Nutr. J. 2013, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Sonneville, K.R.; Long, M.W.; Rifas-Shiman, S.L.; Kleinman, K.; Gillman, W.M.; Taveras, E.M. Juice and water intake in infancy and later beverage intake and adiposity: Could juice be a gateway drink? Obesity 2015, 23, 170–176. [Google Scholar] [CrossRef] [PubMed]
- ChooseMyPlate. United States Department of Agriculture. Available online: http://www.choosemyplate.gov/ (accessed on 1 May 2018).
- Maillot, M.; Rehm, C.C.; Vieux, F.; Rose, C.M.; Drewnowski, A. Beverage consumption patterns among 4–19 y old children in 2009–14 NHANES show that the milk and 100% juice pattern is associated with better diets. Nutr. J. 2018, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Williams, S.M.; Jones, I.E.; Goulding, A. Children who avoid drinking cow milk have low dietary calcium intakes and poor bone health. Am. J. Clin. Nutr. 2001, 76, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Okada, T. Effect of cow milk consumption on longitudinal height gain in children. Am. J. Clin. Nutr. 2004, 80, 1088–1090. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Rangan, A.; Olsen, N.J.; Anderson, L.B.; Wedderkopp, N.; Kristensen, P.; Heitmann, B.L. Sugar-sweetened beverages consumption in relation to changes in body fatness over 6 and 12 years among 9-year-old children: The European Youth Heart Study. Eur. J. Clin. Nutr. 2014, 68, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Shamah-Levy, T.; Garcia-Chavez, C.G.; Rodriguez-Ramirez, S. Association between plain water and sugar-sweetened beverages ad total energy intake among Mexican school-age children. Nutrients 2016, 8, 710. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Beverage Category | Sex | Ages(years) | Finding | |
|---|---|---|---|---|
| Higher Mean Values | Lower Mean Values | |||
| Water/SFB * | Female | 5–8.5 | Water/SFB cluster | All other clusters |
| 9–12.5 | ||||
| 13–17 | ||||
| Male | 5–8.5 | Water/SFB cluster | All other clusters | |
| 9–12.5 | ||||
| 13–17 | ||||
| Milk | Female | 2–4.7 | Milk cluster | All other clusters |
| 5–8.5 | ||||
| 9–12.5 | ||||
| 13–17 | ||||
| Female | 9–12.5 | Juice cluster | Water/SFB cluster SSB † cluster Neutral cluster | |
| 13–17 | ||||
| Male | 5–8.5 | Milk clusterJuice cluster | Water/SFB cluster SSB cluster Neutral cluster | |
| 9–12.5 | ||||
| 13–17 | ||||
| 100% Juice | Female | 9–12.5 | Juice cluster | All other clusters |
| 13–17 | ||||
| Male | 2–4.7 | Juice cluster | All other clusters | |
| 5–8.5 | ||||
| 9–12.5 | ||||
| 13–17 | ||||
| Male | 2–4.7 | SSB cluster | Milk cluster Water/SFB cluster Neutral cluster | |
| 5–8.5 | ||||
| 13–17 | ||||
| SSBs * | Female | 9–12.5 | SSB cluster | All other clusters |
| 13–17 | ||||
| Male | 2–4.7 | SSB cluster | All other clusters | |
| 5–8.5 | ||||
| 9–12.5 | ||||
| 13–17 | ||||
| Variable | Sex | Age (year) | Finding | |
|---|---|---|---|---|
| Higher Mean Values | Lower Mean Values | |||
| Weight | Females | 13 | Milk cluster Water/SFB * cluster SSB * cluster | Juice cluster Neutral cluster |
| 17 | ||||
| Males | 13 | All other clusters | Juice cluster | |
| 17 | ||||
| Height | Females | 13 | All other clusters | Neutral cluster |
| 17 | ||||
| Males | 13 | Milk cluster Water/SFB cluster SSB cluster | Neutral cluster | |
| 17 | ||||
| Body Mass Index | Females | 9 | Water/SFB cluster | All other clusters |
| 13 | ||||
| 17 | ||||
| 5 | All other clusters | Juice cluster | ||
| 9 | ||||
| 13 | ||||
| 17 | ||||
| Males | 9 | All other clusters | Juice cluster | |
| 13 | ||||
| 17 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marshall, T.A.; Curtis, A.M.; Cavanaugh, J.E.; VanBuren, J.M.; Warren, J.J.; Levy, S.M. Description of Child and Adolescent Beverage and Anthropometric Measures According to Adolescent Beverage Patterns. Nutrients 2018, 10, 958. https://doi.org/10.3390/nu10080958
Marshall TA, Curtis AM, Cavanaugh JE, VanBuren JM, Warren JJ, Levy SM. Description of Child and Adolescent Beverage and Anthropometric Measures According to Adolescent Beverage Patterns. Nutrients. 2018; 10(8):958. https://doi.org/10.3390/nu10080958
Chicago/Turabian StyleMarshall, Teresa A., Alexandra M. Curtis, Joseph E. Cavanaugh, John M. VanBuren, John J. Warren, and Steven M. Levy. 2018. "Description of Child and Adolescent Beverage and Anthropometric Measures According to Adolescent Beverage Patterns" Nutrients 10, no. 8: 958. https://doi.org/10.3390/nu10080958