Does Vitamin D Deficiency Affect the Immunogenic Responses to Influenza Vaccination? A Systematic Review and Meta-Analysis

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
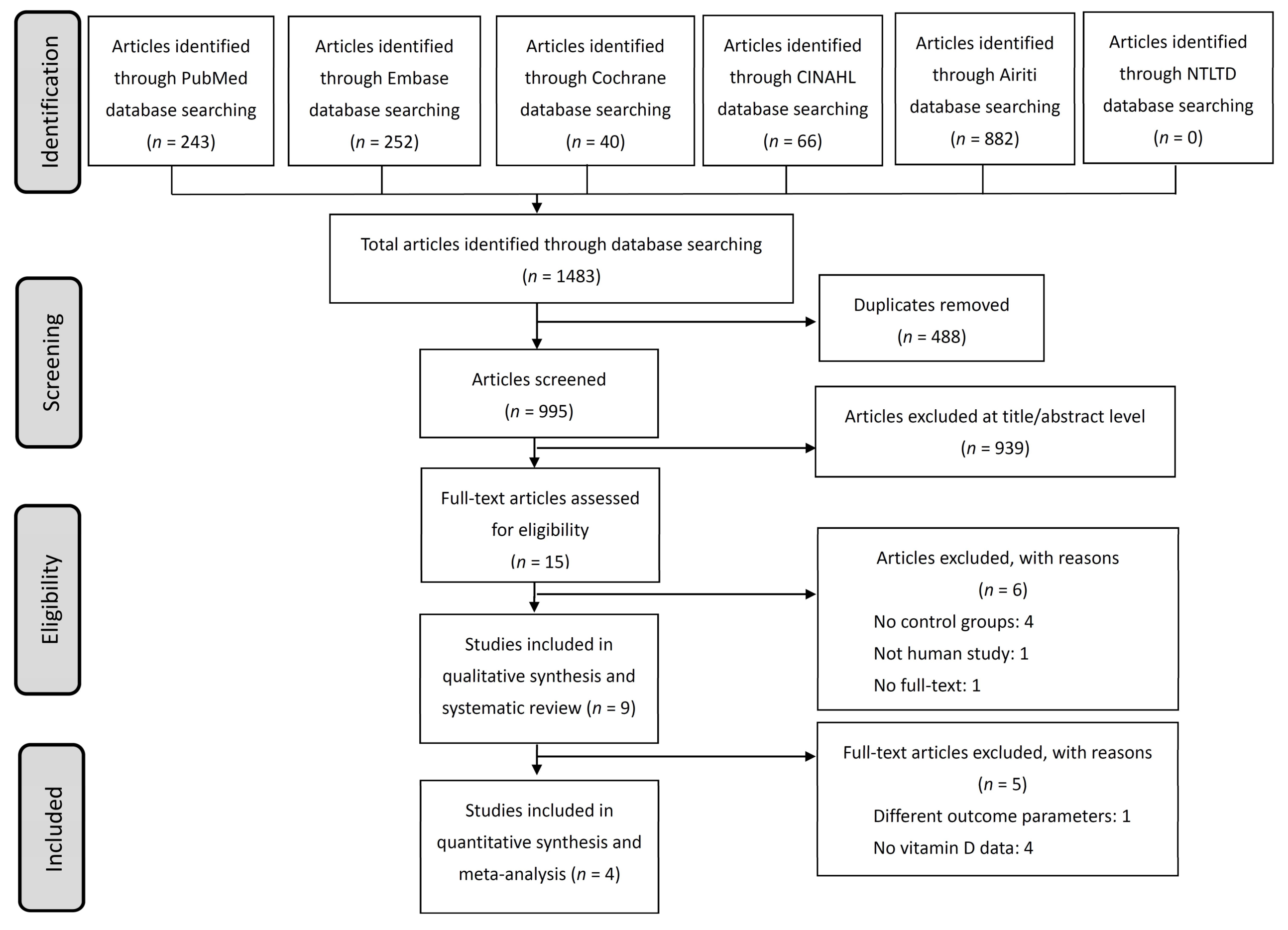
2.1. Study Design and Study Selection
2.2. Data Extraction and Quality Assessment
2.3. Data Synthesis and Analysis
3. Results
3.1. Description of Studies and Quality Assessment
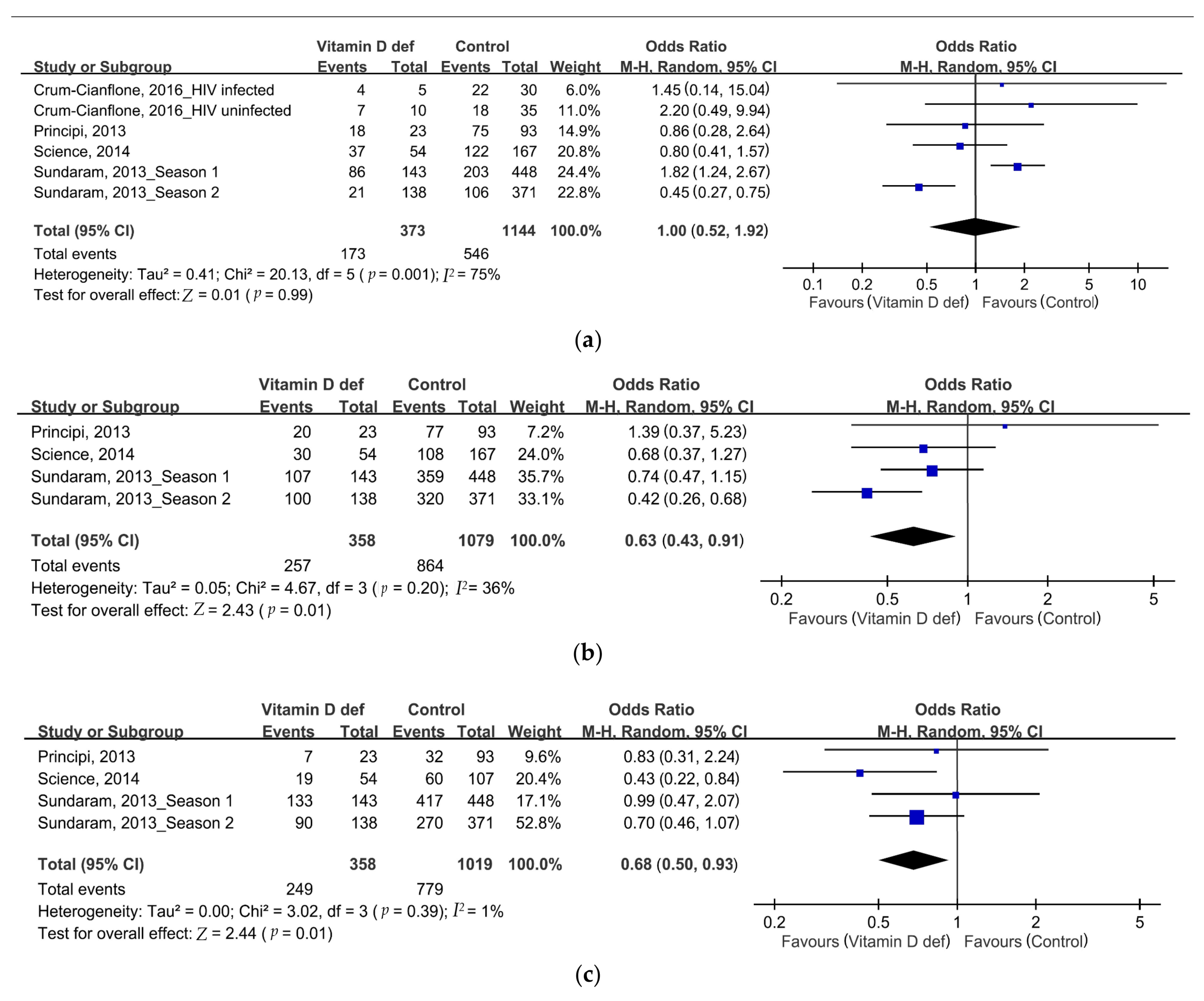
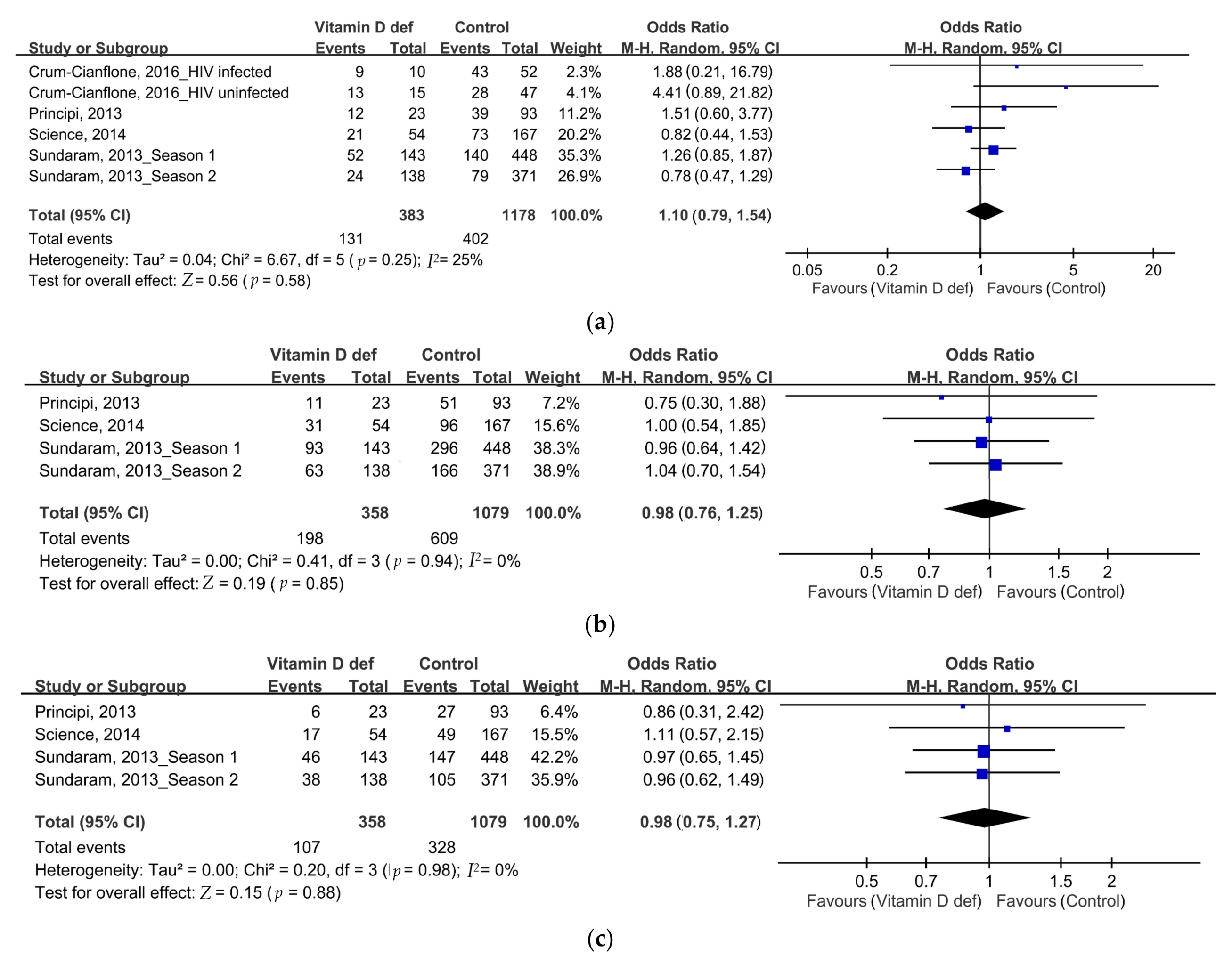
3.2. Data Synthesis and Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jordan, R.E.; Hawker, J.I. Influenza in elderly people in care homes. BMJ 2006, 333, 1229–1230. [Google Scholar] [CrossRef] [PubMed]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- DiazGranados, C.A.; Dunning, A.J.; Kimmel, M.; Kirby, D.; Treanor, J.; Collins, A.; Pollak, R.; Christoff, J.; Earl, J.; Landolfi, V.; et al. Efficacy of high-dose versus standard-dose influenza vaccine in older adults. N. Engl. J. Med. 2014, 371, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Pae, M.; Meydani, S.N.; Wu, D. The role of nutrition in enhancing immunity in aging. Aging Dis. 2012, 3, 91–129. [Google Scholar] [PubMed]
- Talbot, H.K.; Keitel, W.; Cate, T.R.; Treanor, J.; Campbell, J.; Brady, R.C.; Graham, I.; Dekker, C.L.; Ho, D.; Winokur, P.; et al. Immunogenicity, safety and consistency of new trivalent inactivated influenza vaccine. Vaccine 2008, 26, 4057–4061. [Google Scholar] [CrossRef] [PubMed]
- Del Porto, F.; Lagana, B.; Biselli, R.; Donatelli, I.; Campitelli, L.; Nisini, R.; Cardelli, P.; Rossi, F.; D’Amelio, R. Influenza vaccine administration in patients with systemic lupus erythematosus and rheumatoid arthritis. Safety and immunogenicity. Vaccine 2006, 24, 3217–3223. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- McNally, J.D.; Nama, N.; O’Hearn, K.; Sampson, M.; Amrein, K.; Iliriani, K.; McIntyre, L.; Fergusson, D.; Menon, K. Vitamin D deficiency in critically ill children: A systematic review and meta-analysis. Crit. Care 2017, 21. [Google Scholar] [CrossRef] [PubMed]
- An, L.; Sun, M.H.; Chen, F.; Li, J.R. Vitamin D levels in systemic sclerosis patients: A meta-analysis. Drug Des. Dev. Ther. 2017, 11, 3119–3125. [Google Scholar] [CrossRef] [PubMed]
- Man, L.; Zhang, Z.; Zhang, M.; Zhang, Y.; Li, J.; Zheng, N.; Cao, Y.; Chi, M.; Chao, Y.; Huang, Q.; et al. Association between vitamin D deficiency and insufficiency and the risk of childhood asthma: Evidence from a meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 5699–5706. [Google Scholar] [PubMed]
- Chowdhury, R.; Kunutsor, S.; Vitezova, A.; Oliver-Williams, C.; Chowdhury, S.; Kiefte-de-Jong, J.C.; Khan, H.; Baena, C.P.; Prabhakaran, D.; Hoshen, M.B.; et al. Vitamin D and risk of cause specific death: Systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferder, M.; Inserra, F.; Manucha, W.; Ferder, L. The world pandemic of vitamin D deficiency could possibly be explained by cellular inflammatory response activity induced by the renin-angiotensin system. Am. J. Physiol. Cell Physiol. 2013, 304, C1027–C1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira, J.S.R.; de Paula, T.P.; Sperb, L.F.; Miller, M.E.P.; Azevedo, M.J.; Viana, L.V. Association of plasma vitamin D status with lifestyle patterns and ambulatory blood pressure monitoring parameters in patients with type 2 diabetes and hypertension. Diabetes Res. Clin. Pract. 2018, 139, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.E.; Powell, J.T. Vitamin D and cardiovascular disease. Circ. Res. 2014, 114, 379–393. [Google Scholar] [CrossRef] [PubMed]
- McNally, J.D.; Menon, K.; Chakraborty, P.; Fisher, L.; Williams, K.A.; Al-Dirbashi, O.Y.; Doherty, D.R. The association of vitamin D status with pediatric critical illness. Pediatrics 2012, 130, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.M.; Looker, A.C.; Chang, S.-C.; Graubard, B.I. Prospective study of serum vitamin D and cancer mortality in the United States. J. Natl. Cancer Inst. 2007, 99, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Chiang, K.C.; Chen, T.C. The anti-cancer actions of vitamin D. Anticancer Agents Med. Chem. 2013, 13, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Cannell, J.J.; Vieth, R.; Umhau, J.C.; Holick, M.F.; Grant, W.B.; Madronich, S.; Garland, C.F.; Giovannucci, E. Epidemic influenza and vitamin D. Epidemiol. Infect. 2006, 134, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Pojsupap, S.; Iliriani, K.; Sampaio, T.Z.; O’Hearn, K.; Kovesi, T.; Menon, K.; McNally, J.D. Efficacy of high-dose vitamin D in pediatric asthma: A systematic review and meta-analysis. J. Asthma 2015, 52, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.A., Jr.; Ganmaa, D.; Sidbury, R.; Erdenedelger, K.; Radnaakhand, N.; Khandsuren, B. Randomized trial of vitamin D supplementation for winter-related atopic dermatitis in children. J. Allergy Clin. Immunol. 2014, 134, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.E.; Leung, M.; Mesfin, E.; Qamar, H.; Watterworth, J.; Papp, E. Vitamin D supplementation during pregnancy: State of the evidence from a systematic review of randomised trials. BMJ 2017. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Fang, V.J.; Perera, R.A.; Kam, A.M.; Ng, S.; Chan, Y.H.; Chan, K.H.; Ip, D.K.; Peiris, J.M.; Cowling, B.J. Serum 25-hydroxyvitamin D was not associated with influenza virus infection in children and adults in Hong Kong, 2009–2010. J. Nutr. 2016, 146, 2506–2512. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Forrest, K.Y.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J. Clin. Endocrinol. Metab. 2012, 97, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- De Jong, J.C.; Palache, A.M.; Beyer, W.E.; Rimmelzwaan, G.F.; Boon, A.C.; Osterhaus, A.D. Haemagglutination-inhibiting antibody to influenza virus. Dev. Biol. 2003, 115, 63–73. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.J.; Martin, J.M.; Cole, K.S.; Zimmerman, R.K.; Susick, M.; Moehling, K.K.; Levine, M.Z.; Spencer, S.; Flannery, B.; Nowalk, M.P. Are children’s vitamin D levels and BMI associated with antibody titers produced in response to 2014-2015 influenza vaccine? Hum. Vaccines Immunother. 2017, 13, 1661–1665. [Google Scholar] [CrossRef] [PubMed]
- Sadarangani, S.P.; Ovsyannikova, I.G.; Goergen, K.; Grill, D.E.; Poland, G.A. Vitamin D, leptin and impact on immune response to seasonal influenza A/H1N1 vaccine in older persons. Hum. Vaccin Immunother. 2016, 12, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Crum-Cianflone, N.F.; Won, S.; Lee, R.; Lalani, T.; Ganesan, A.; Burgess, T.; Agan, B.K. Vitamin D levels and influenza vaccine immunogenicity among HIV-infected and HIV-uninfected adults. Vaccine 2016, 34, 5040–5046. [Google Scholar] [CrossRef] [PubMed]
- Science, M.; Maguire, J.L.; Russell, M.L.; Smieja, M.; Walter, S.D.; Loeb, M. Serum 25-hydroxyvitamin D level and influenza vaccine immunogenicity in children and adolescents. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, M.E.; Talbot, H.K.; Zhu, Y.; Griffin, M.R.; Spencer, S.; Shay, D.K.; Coleman, L.A. Vitamin D is not associated with serologic response to influenza vaccine in adults over 50 years old. Vaccine 2013, 31, 2057–2061. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Marchisio, P.; Terranova, L.; Zampiero, A.; Baggi, E.; Daleno, C.; Tirelli, S.; Pelucchi, C.; Esposito, S. Impact of vitamin D administration on immunogenicity of trivalent inactivated influenza vaccine in previously unvaccinated children. Hum. Vaccines Immunother. 2013, 9, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Thorne, A. Vitamin D supplementation does not increase immunogenicity of seasonal influenza vaccine in HIV-infected adults. HIV Clin. Trials 2011, 12, 275–276. [Google Scholar] [CrossRef] [PubMed]
- Chadha, M.K.; Fakih, M.; Muindi, J.; Tian, L.; Mashtare, T.; Johnson, C.S.; Trump, D. Effect of 25-hydroxyvitamin D status on serological response to influenza vaccine in prostate cancer patients. Prostate 2011, 71, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Kriesel, J.D.; Spruance, J. Calcitriol (1,25-dihydroxy-vitamin D3) coadministered with influenza vaccine does not enhance humoral immunity in human volunteers. Vaccine 1999, 17, 1883–1888. [Google Scholar] [CrossRef]
- Puig-Barbera, J.; Mira-Iglesias, A.; Tortajada-Girbes, M.; Lopez-Labrador, F.X.; Librero-Lopez, J.; Diez-Domingo, J.; Carballido-Fernandez, M.; Carratala-Munuera, C.; Correcher-Medina, P.; Gil-Guillen, V.; et al. Waning protection of influenza vaccination during four influenza seasons, 2011/2012 to 2014/2015. Vaccine 2017, 43, 5799–5807. [Google Scholar] [CrossRef] [PubMed]
- Bellei, N.C.J.; Carraro, E.; Castelo, A.; Granato, C.F.H. Risk factors for poor immune response to influenza vaccination in elderly people. Braz. J. Infect. Dis. 2006, 10, 269–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzoli, L.; Ioannidis, J.P.; Flacco, M.E.; de Vito, C.; Villari, P. Effectiveness and harms of seasonal and pandemic influenza vaccines in children, adults and elderly: A critical review and re-analysis of 15 meta-analyses. Hum. Vaccines Immunother. 2012, 8, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, A.; Sprenger, M. Low effectiveness undermines promotion of seasonal influenza vaccine. Lancet Infect. Dis. 2013, 13, 7–9. [Google Scholar] [CrossRef]
- Haq, K.; McElhaney, J.E. Immunosenescence: Influenza vaccination and the elderly. Curr. Opin. Immunol. 2014, 29, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, R.; Pozzi, T.; Montomoli, E.; Fragapane, E.; Senatore, F.; Minutello, M.; Podda, A. Increased immunogenicity of the MF59-adjuvanted influenza vaccine compared to a conventional subunit vaccine in elderly subjects. Eur. J. Epidemiol. 2001, 17, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.L.; Shih, P.C.; Liu, S.J.; Lin, C.H.; Liu, J.M.; Lei, W.T.; Lin, C.Y. The influence of prebiotic or probiotic supplementation on antibody titers after influenza vaccination: A systematic review and meta-analysis of randomized controlled trials. Drug Des. Dev. Ther. 2018, 12, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Lei, W.T.; Shih, P.C.; Liu, S.J.; Lin, C.Y.; Yeh, T.L. Effect of probiotics and prebiotics on immune response to influenza vaccination in adults: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2017, 9, 1175. [Google Scholar] [CrossRef] [PubMed]
- Langer-Gould, A.; Lucas, R.; Xiang, A.H.; Chen, L.H.; Wu, J.; Gonzalez, E.; Haraszti, S.; Smith, J.B.; Quach, H.; Barcellos, L.F. MS Sunshine Study: Sun exposure but not vitamin D is associated with multiple sclersosis risk in Blacks and Hispanics. Nutrients 2018, 10, 268. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.M.; Gorman, S.; Black, L.; Neale, R.E. Clinical, research, and public health implications of poor measurement of vitamin D status. J. AOAC Intl. 2017, 100, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the institute of medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; So, T.-Y.; Thackray, J. A review on vitamin D deficiency treatment in pediatric patients. J. Pediatr. Pharmacol. Ther. 2013, 18, 277–291. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Studies Author, Year | Country | Participants (M%:F%) | Age (y/o) Mean (SD) | Vit D cutoff 25-OH D level (ng/ml) | VDD Patients (%) | Supplement of Vit D | Type of Vaccine | Components of Vaccine | Measured Outcomes | Associated with VDD |
|---|---|---|---|---|---|---|---|---|---|---|
| Lin, 2017 [33] | USA | 135 children (46%:54%) | NR | 20 | 61 (45%) | No | LAIV (83) TIV (52) | A/California/7/2009 (H1N1); A/Texas/50/2012 (H3N2); B/Massachusetts/2/2012 | Antibody titers | Weakly negative |
| Sadarangani, 2016 [34] | USA | 159 elders (61.6%:38.4%) | 59.5 (median) | 25 | 8 (5%) | No | TIV | A/California/7/2009 (H1N1); A/Perth/16/2009 (H3N2); B/Brisbane/60/2008 | Antibody titers | Weakly positive |
| Crum-Cianflone, 2016 * [35] | USA | 64 HIV-infected (93.8%:6.2%); 64 HIV-uninfected (89.1%:10.9%) | 35; 34.5 | 20 | 16 (25%); 11 (17.2%) | No | Monovalent inactivated vaccine | A/California/7/2009(H1N1) | Seroconversion Antibody titers | No |
| Science, 2014 * [36] | Canada | 221 children (48%:52%) | 9.16 | 25 | 2 (0.9%) | No | TIV | A/Brisbane/59/2007 (H1N1); A/Brisbane/10/2007 (H3N2); B/Florida/4/2006. | Antibody titers Seroprotection | No |
| Sundaram, 2013, Season 1 * [37] | USA | 591 adults (39%:61%) | 64 ± 10 years | 25 | 143 (29%) | No | TIV | A/Brisbane/59/2007 (H1N1); A/Brisbane/10/2007 (H3N2); B/Florida/4/2006 | Seroprotection | Negative |
| Sundaram, 2013, Season 2 * [37] | USA | 509 adults (38%:62%) | 66 ± 10 | 25 | 138 (27%) | No | TIV | A/Brisbane/59/2007-like (H1N1), A/Brisbane/10/2007-like (H3N2), B/Brisbane/60/2008-like; A/California/7/2009 (H1N1) | Seroprotection | No |
| Principi, 2013 * [38] | Italy | 116 AOM children (52.6%:47.4%) | 3 ± 1 | 20 | 23 (19.8%) | Yes | TIV | A/California/7/2009(H1N1); A/Perth/16/2009(H3N2); B/Brisbane/60/2008 | Seroprotection Seroconversion Antibody titers | No |
| Cooper, 2011 [39] | Canada | 298 HIV-infected adults (90%:10%) | NR | Not measured | Not measured | Yes | TIV | A/Brisbane (H1N1); A/Uruguay (H3N2); B/Florida | Seroprotection Seroconversion | No |
| Chadha, 2011 [40] | USA | 35 Prostate cancer patients (100%:0%) | 68 | Median | 9 (26%) | Partial | TIV | A/New Caledonia/20/99 (H1N1); A/Wisconsin/67/2005 (H3N2); and B/Malaysia/2506/2004 | Antibody titers Seroprotection | Positive |
| Kriesel, 1999 [41] | USA | 175 healthy volunteers (52.6%:47.4%) | 32 | Not measured | Not measured | Yes | TIV | A/Wuhan/359/95(H3N2); A/Singapore/6/1986(H1N1); B/Beijing/184/93 | Antibody titers Seroprotection | No |
| Study Population | Seroprotection Rate | Seroconversion Rate | ||||
|---|---|---|---|---|---|---|
| A/H1N1 | A/H3N2 | B strain | A/H1N1 | A/H3N2 | B Strain | |
| Vitamin D def | 46.40% | 71.80% | 69.60% | 34.20% | 55.30% | 29.90% |
| Control | 47.70% | 80.10% | 76.40% | 34.10% | 56.40% | 30.40% |
| Odds ratio | 1 (0.52–1.92) | 0.63 (0.43–0.91) | 0.68 (0.5–0.93) | 1.1 (0.79–1.54) | 0.98 (0.76–1.25) | 0.98 (0.75–1.27) |
| p | 0.99 | 0.01 | 0.01 | 0.58 | 0.19 | 0.88 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.-D.; Lin, C.-H.; Lei, W.-T.; Chang, H.-Y.; Lee, H.-C.; Yeung, C.-Y.; Chiu, N.-C.; Chi, H.; Liu, J.-M.; Hsu, R.-J.; et al. Does Vitamin D Deficiency Affect the Immunogenic Responses to Influenza Vaccination? A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 409. https://doi.org/10.3390/nu10040409
Lee M-D, Lin C-H, Lei W-T, Chang H-Y, Lee H-C, Yeung C-Y, Chiu N-C, Chi H, Liu J-M, Hsu R-J, et al. Does Vitamin D Deficiency Affect the Immunogenic Responses to Influenza Vaccination? A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(4):409. https://doi.org/10.3390/nu10040409
Chicago/Turabian StyleLee, Ming-Dar, Chao-Hsu Lin, Wei-Te Lei, Hung-Yang Chang, Hung-Chang Lee, Chun-Yan Yeung, Nan-Chang Chiu, Hsin Chi, Jui-Ming Liu, Ren-Jun Hsu, and et al. 2018. "Does Vitamin D Deficiency Affect the Immunogenic Responses to Influenza Vaccination? A Systematic Review and Meta-Analysis" Nutrients 10, no. 4: 409. https://doi.org/10.3390/nu10040409