
Evaluation of the Road to Birth Software to Support Obstetric Problem-Based Learning Education with a Cohort of Pre-Clinical Medical Students

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
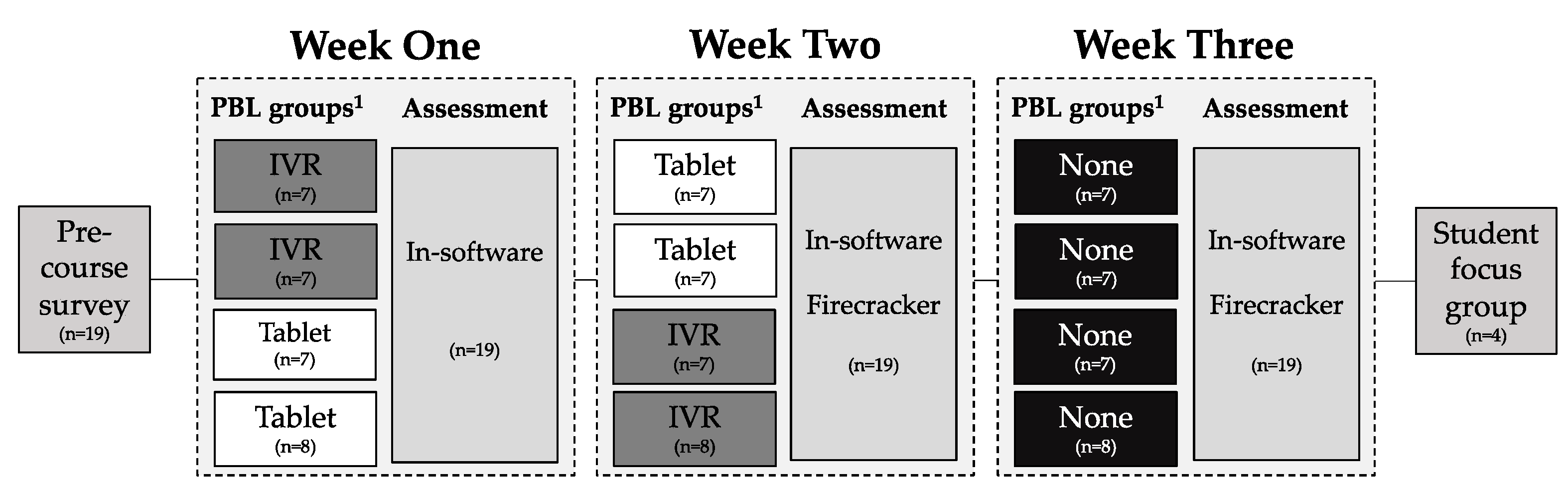
2.1. Study Design
2.2. Setting and Participants
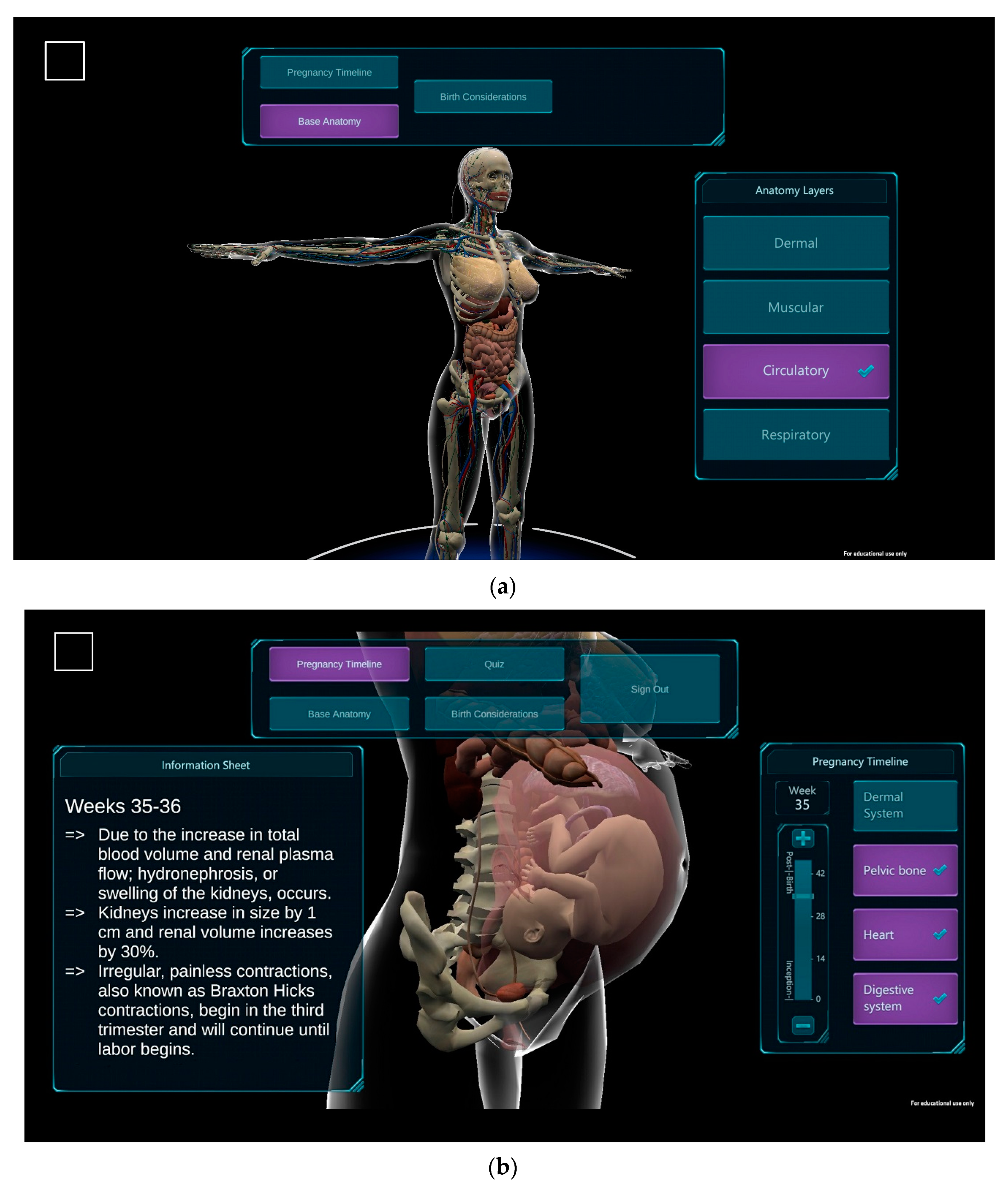
2.3. Road to Birth (RtB) Software
- Apple (Cupertino, CA, USA) smartphone/tablet (SpT) applications;
- Android (Mountain View, CA, USA) SpT applications;
- and in IVR using a HMD.
2.4. Curriculum Integration
2.5. Data Collection and Analysis
3. Results
3.1. Quantitative Findings
3.2. Qualitative Findings
- Students want a usable, professional-grade product.
- The use of technology should be optimized for its purpose.
- Students prefer content suitable for multiple uses.
Themes and Sub-Themes
4. Discussion
- The ability to use the software in remote learning environments;
- The ability to use the software as a patient education resource.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. College of Medicine Road to Birth Student Focus Group Interview Protocol
- Did you have any experience with similar mobile technologies prior to undertaking this course?
- Have you and/or are you using any program similar to the Road to Birth (RtB)?
- What were your expectations prior to using the content?
- What did you view as advantages of using the virtual reality (VR) version of RtB? Disadvantages?
- What did you view as advantages of using the tablet version of RtB? Disadvantages?
- Do you feel that they added to or hindered education during the session?
- What factors influenced you to take your assessment in the format you selected (VR or tablet)?
- How can the software be improved?
- If only one version of the software could be used in a course, which version do you think should be selected? Why?
- Do you see yourself using RtB in the clinic and if so, how?
References
- Bergman, E.M.; van der Vleuten, C.P.; Scherpbier, A.J. Why don’t they know enough about anatomy? A narrative review. Med. Teach. 2011, 33, 403–409. [Google Scholar] [CrossRef] [PubMed]
- McMenamin, P.; McLachlan, J.; Wilson, A.; McBride, J.; Pickering, J.; Evans, D.; Winkelmann, A. Do we really need cadavers anymore to learn anatomy in undergraduate medicine? Med. Teach. 2018, 40, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Bergman, E.M. Teaching and learning anatomy in a PBL curriculum. In Teaching Anatomy: A Practical Guide; Chan, L.K., Pawlina, W., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 143–152. [Google Scholar]
- Iwanaga, J.; Loukas, M.; Dumont, A.S.; Tubbs, R.S. A review of anatomy education during and after the COVID-19 pandemic: Revisiting traditional and modern methods to achieve future innovation. Clin. Anat. 2021, 34, 108–114. [Google Scholar] [CrossRef]
- Gloy, K.; Weyhe, P.; Nerenz, E.; Kaluschke, M.; Uslar, V.; Zachmann, G.; Weyhe, D. Immersive Anatomy Atlas: Learning factual medical knowledge in a virtual reality environment. Anat. Sci. Educ. 2021, 15, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Chytas, D.; Salmas, M.; Skandalakis, G.P.; Troupis, T.G. Can immersive virtual reality function as a suitable alternative to conventional anatomy education methods? Anat. Sci. Educ. 2021, 14, 693–694. [Google Scholar] [CrossRef] [PubMed]
- Kurul, R.; Ögün, M.N.; Neriman Narin, A.; Avci, Ş.; Yazgan, B. An alternative method for anatomy training: Immersive virtual reality. Anat. Sci. Educ. 2020, 13, 648–656. [Google Scholar] [CrossRef]
- Nelson, L.; Sadler, L.; Surtees, G. Bringing problem based learning to life using virtual reality. Nurse Educ. Pract. 2005, 5, 103–108. [Google Scholar] [CrossRef]
- Tudor Car, L.; Kyaw, B.M.; Dunleavy, G.; Smart, N.A.; Semwal, M.; Rotgans, J.I.; Low-Beer, N.; Campbell, J. Digital Problem-Based Learning in Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12945. [Google Scholar] [CrossRef]
- Cavicchia, M.L.; Cusumano, A.M.; Bottino, D.V. Problem-based learning implementation in a health sciences blended-learning program in Argentina. Int. J. Med. Educ. 2018, 9, 45–47. [Google Scholar] [CrossRef]
- Alverson, D.C.; Saiki, S.M., Jr.; Kalishman, S.; Lindberg, M.; Mennin, S.; Mines, J.; Serna, L.; Summers, K.; Jacobs, J.; Lozanoff, S.; et al. Medical students learn over distance using virtual reality simulation. Simul. Healthc. 2008, 3, 10–15. [Google Scholar] [CrossRef]
- Sugand, K.; Abrahams, P.; Khurana, A. The anatomy of anatomy: A review for its modernization. Anat. Sci. Educ. 2010, 3, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Kumar Ghosh, S.; Kumar, A. Building professionalism in human dissection room as a component of hidden curriculum delivery: A systematic review of good practices. Anat. Sci. Educ. 2019, 12, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Fealy, S.; Jones, D.; Hutton, A.; Graham, K.; McNeill, L.; Sweet, L.; Hazelton, M. The integration of immersive virtual reality in tertiary nursing and midwifery education: A scoping review. Nurse Educ. Today 2019, 79, 14–19. [Google Scholar] [CrossRef]
- Barmaki, R.; Yu, K.; Pearlman, R.; Shingles, R.; Bork, F.; Osgood, G.M.; Navab, N. Enhancement of Anatomical Education Using Augmented Reality: An Empirical Study of Body Painting. Anat. Sci. Educ. 2019, 12, 599–609. [Google Scholar] [CrossRef]
- Stepan, K.; Zeiger, J.; Hanchuk, S.; Del Signore, A.; Shrivastava, R.; Govindaraj, S.; Iloreta, A. Immersive virtual reality as a teaching tool for neuroanatomy. Int. Forum Allergy Rhinol. 2017, 7, 1006–1013. [Google Scholar] [CrossRef]
- Jones, D.; Siang See, Z.; Billinghurst, M.; Goodman, L.; Fealy, S. Extended reality for midwifery learning: Mixed reality and virtual reality demonstration. In Proceedings of the VRCAI ‘19: The 17th International Conference on Virtual Reality Continuum and its Applications in Industry, New York, NY, USA, 14 November 2019. [Google Scholar]
- Peters, M.; Laeng, B.; Latham, K.; Jackson, M.; Zaiyouna, R.; Richardson, C. A redrawn Vandenberg and Kuse mental rotations test: Different versions and factors that affect performance. Brain Cogn. 1995, 28, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.S.; Suh, A. The role of spatial ability in learning with virtual reality: A literature review. In Proceedings of the 54th Hawaii International Conference on System Sciences, Honolulu, HI, USA, 5 January 2021. [Google Scholar]
- Jones, D.; Hazelton, M.; Evans, D.J.R.; Pento, V.; Siang See, Z.; Van Leugenhaege, L.; Fealy, S. The Road to Birth: Using digital technology to visualise pregnancy anatomy. In Digital Anatomy: Applications of Virtual, Mixed and Augmented Reality; Uhl, J.F., Jorge, J., Lopes, D.S., Campos, P.F., Eds.; Springer: Cham, Switzerland, 2021; pp. 325–342. [Google Scholar] [CrossRef]
- Fealy, S.; Irwin, P.; Zeynep, T.; See, Z.; Jones, D. Enhancing nursing simulation education: A case for XR innovation. Virtual Worlds 2023, 2, 218–230. [Google Scholar] [CrossRef]
- See, Z.S.; Ledger, S.; Goodman, L.L.; Matthews, B.; Jones, D.; Fealy, S.; Ooi, W.H.; Amin, M. Playable experiences through technologies: Opportunities and challenges for teaching simulation learning and extended reality solution creation. J. Inf. Technol. Educ. Innov. Pract. 2023, 22, 67–90. [Google Scholar]
- Radianti, J.; Majchrzak, T.; Fromm, J.; Wohlgenannt, I. A systematic review of immersive virtual reality applications for higher education: Design elements, lessons learned, and research agenda. Comput. Educ. J. 2020, 147, 103778. [Google Scholar] [CrossRef]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description—The poor cousin of health research? BMC Med. Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef]
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Roberts, K.; Dowell, A.; Nie, J.-B. Attempting rigour and replicability in thematic analysis of qualitative research data; a case study of codebook development. BMC Med. Res. Methodol. 2019, 19, 66. [Google Scholar] [CrossRef] [PubMed]
- Bartikian, M.; Ferreira, A.; Gonçalves-Ferreira, A.; Neto, L.L. 3D printing anatomical models of head bones. Surg. Radiol. Anat. 2019, 41, 1205–1209. [Google Scholar] [CrossRef]
- Jaffar, A.A. YouTube: An emerging tool in anatomy education. Anat. Sci. Educ. 2012, 5, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Weyhe, D.; Uslar, V.; Weyhe, F.; Kaluschke, M.; Zachmann, G. Immersive anatomy atlas-empirical study investigating the usability of a virtual reality environment as a learning tool for anatomy. Front. Surg. 2018, 5, 73. [Google Scholar] [CrossRef]
- Kim, J.W.; Myung, S.J.; Yoon, H.B.; Moon, S.H.; Ryu, H.; Yim, J.J. How medical education survives and evolves during COVID-19: Our experience and future direction. PLoS ONE 2020, 15, e0243958. [Google Scholar] [CrossRef]
- Shahrvini, B.; Baxter, S.L.; Coffey, C.S.; MacDonald, B.V.; Lander, L. Pre-clinical remote undergraduate medical education during the COVID-19 pandemic: A survey study. BMC Med. Educ. 2021, 21, 13. [Google Scholar] [CrossRef]
- Acquavita, S.P.; Krummel, D.A.; Talks, A.; Cobb, A.; McClure, E. Assessing the digital divide among low-income perinatal women: Opportunities for provision of health information and counseling. Telemed. J. E Health 2019, 25, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Fealy, S.; Chan, S.; Wynne, O.; Eileen, D.; Ebert, L.; Ho, R.; Zhang, M.; Jones, D. The Support for New Mums Project: A protocol for a pilot randomised controlled trial designed to test a postnatal psychoeducation smartphone application. J. Adv. Nurs. 2019, 75, 1–13. [Google Scholar] [CrossRef]
- Tang, K.; Gerling, K.; Chen, W.; Geurts, L. Information and communication systems to tackle barriers to breastfeeding: Systematic search and review. J. Med. Internet Res. 2019, 21, e13947. [Google Scholar] [CrossRef]
- Connaghan, R.; Poyade, M.; Rea, P.M. Evaluation of child-friendly augmented reality tool for patient-centered education in radiology and bone reconstruction. Adv. Exp. Med. Biol. 2019, 1171, 105–126. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.P.; Crouch, E. Digital information technology use and patient preferences for Internet-based health education modalities: Cross-sectional survey study of middle-aged and older adults with chronic health conditions. JMIR Aging 2019, 2, e12243. [Google Scholar] [CrossRef]
- Conard, S. Best practices in digital health literacy. Int. J. Cardiol. 2019, 292, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Pandrangi, V.C.; Gaston, B.; Appelbaum, N.P.; Albuquerque, F.C., Jr.; Levy, M.M.; Larson, R.A. The application of virtual reality in patient education. Ann. Vasc. Surg. 2019, 59, 184–189. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C.; McCann, M.; Brady, A.M. Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 5, Cd011425. [Google Scholar] [CrossRef]
- Cahn, A.; Akirov, A.; Raz, I. Digital health technology and diabetes management. J. Diabetes 2018, 10, 10–17. [Google Scholar] [CrossRef]
- Nandi, P.L.; Chan, J.N.; Chan, C.P.; Chan, P.; Chan, L.P. Undergraduate medical education: Comparison of problem-based learning and conventional teaching. Hong Kong Med. J. 2000, 6, 301–306. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency of Use n (%) | ||||
|---|---|---|---|---|
| How often Do You Use Each of the Following? | Never | Monthly | Weekly | Daily |
| Non-portable game consoles | 16 (84%) | 3 (16%) | 0 | 0 |
| Portable game consoles | 14 (74%) | 3 (16%) | 1 (5%) | 1 (5%) |
| Use of virtual/augmented reality | 19 (100%) | 0 | 0 | 0 |
| Course content on Compass | 3 (16%) | 1 (5%) | 11 (58%) | 3 (16%) |
| Online discussion forums | 11 (58%) | 31.6% | 1 (5%) | 1 (5%) |
| Firecracker | 0 | 3 (16%) | 14 (74%) | 2 (11%) |
| Video conferencing | 11 (58%) | 3 (16%) | 5 (26%) | 0 |
| Question banks | 0 | 1 (5%) | 10 (53%) | 8 (42%) |
| Smartphone/tablet apps | 10.5% | 5 (26%) | 21.1% | 8 (42%) |
| Podcasts | 47.4% | 5 (26%) | 3 (16%) | 2 (11%) |
| Internet websites | 1 (5%) | 0 | 2 (11%) | 16 (84%) |
| Google/Google Scholar | 0 | 0 | 6 (32%) | 13 (68%) |
| Wikipedia | 1 (5%) | 2 (11%) | 10 (53%) | 6 (32%) |
| Text messaging | 5 (26%) | 2 (11%) | 1 (5%) | 11 (58%) |
| Social media | 8 (42%) | 2 (11%) | 2 (11%) | 7 (37%) |
| YouTube | 2 (11%) | 2 (11%) | 10 (53%) | 5 (26%) |
| Median (% Correct) | Interquartile Range | |
|---|---|---|
| Road to Birth in-software week one quiz | 87 | 17 |
| Road to Birth in-software week two quiz | 79 | 21 |
| Road to Birth in-software week three quiz | 86 | 14 |
| Firecracker week two quiz | 75 | 15 |
| Firecracker week three quiz | 89 | 11 |
| Main Themes | Sub-Themes | Representative Quotes |
|---|---|---|
| 1. Students want a usable, professional-grade product | Design of product (artwork, text) | “I was kind of disappointed in the quality of the software.” “I think…there could be… more detail in some… of the changes.” |
| Utility of product (usability, convenience) | “Being able to zoom in and spin… the model around [on the smartphone] was almost pointless just because the screen was so small. I can’t see any detail.” “I found my primary use … for it was actually it was a convenient pocket resource to have since I did have it on my phone.” | |
| 2. The use of technology should be optimized for its purpose | IVR for educational use should build on its interactive nature | “Where you get an advantage in VR over just looking at pictures in a textbook.” “My experiences with VR for educational purposes, I’m not convinced that it’s… really that great. It can be useful for some people, but I think for some people… it doesn’t really add very much.” “If you’re going to use this platform to quiz us, at least use a 3D model and be like, here is this placenta previa or not previa? Where is this? What is it?” “I don’t think that most people in this school have even given or even tried the 3D anatomy for normal anatomy. Yet they complained about anatomy, and… no one came over there to do it. I invited people to come out. But everyone’s automatically like ‘VR? No thanks.’” |
| IVR provides an enjoyable learning experience | “[I was] the one who actually used it in the PBL session. I had a blast. I thought it was… lots of fun. I was crawling on the floor trying to get better viewpoints for them.” “I think VR is cool and I’d love to see it… used in education more.” | |
| 3. Students prefer content suitable for multiple purposes | Desire for a product that teaches pathology and physiology | “I… liked [the previas] … I would say those… plus the breech, were probably the best parts of the [software].” |
| Road to Birth as a tool to teach others | “I think it’ll be very beneficial when it comes to showing someone who doesn’t understand… a lot of information.” “I was talking about pregnancy changes with someone who was not in… the field of medicine… What I was able to do is I was actually [able] to pull it out and scroll to 32 weeks cause the individual was approximately 32 weeks, and actually physically showed them what that looked like internally and explained how somebody’s symptoms that they’re experiencing were a result of those changes in the organs.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hutchcraft, M.L.; Wallon, R.C.; Fealy, S.M.; Jones, D.; Galvez, R. Evaluation of the Road to Birth Software to Support Obstetric Problem-Based Learning Education with a Cohort of Pre-Clinical Medical Students. Multimodal Technol. Interact. 2023, 7, 84. https://doi.org/10.3390/mti7080084
Hutchcraft ML, Wallon RC, Fealy SM, Jones D, Galvez R. Evaluation of the Road to Birth Software to Support Obstetric Problem-Based Learning Education with a Cohort of Pre-Clinical Medical Students. Multimodal Technologies and Interaction. 2023; 7(8):84. https://doi.org/10.3390/mti7080084
Chicago/Turabian StyleHutchcraft, Megan L., Robert C. Wallon, Shanna M. Fealy, Donovan Jones, and Roberto Galvez. 2023. "Evaluation of the Road to Birth Software to Support Obstetric Problem-Based Learning Education with a Cohort of Pre-Clinical Medical Students" Multimodal Technologies and Interaction 7, no. 8: 84. https://doi.org/10.3390/mti7080084