Rationale and Protocol of the Multimodality Evaluation of Antibody-Mediated Injury in Heart Transplantation (LEONE-HT) Observational Cross-Sectional Study

 , , , , , , and
, , , , , , and
Abstract
:1. Strengths and Limitations of This Study
- -
- The appearance of anti-HLA antibodies is known to be related to poorer outcomes, suggesting that anti-HLA antibodies induce chronic graft damage beyond acute rejection.
- -
- The LEONE-HT project aimed to describe the structural damage inflicted on the myocardium by anti-HLA antibodies and test the performance of different diagnostic techniques to identify and grade antibody-mediated injuries in HTs.
- -
- Patients underwent a complex multimodal assessment, including state-of-the-art histopathologic, physiologic and imaging techniques.
- -
- Our study limitations were inherent to the observational approach as the selection of non-exposed patients was the most complex part of the study.
- -
- This pilot study aimed to define antibody-mediated damage in HT thoroughly and set the basis for future dedicated studies in the field.
2. Introduction
3. Methods and Analysis
3.1. Study Hypotheses and Objectives
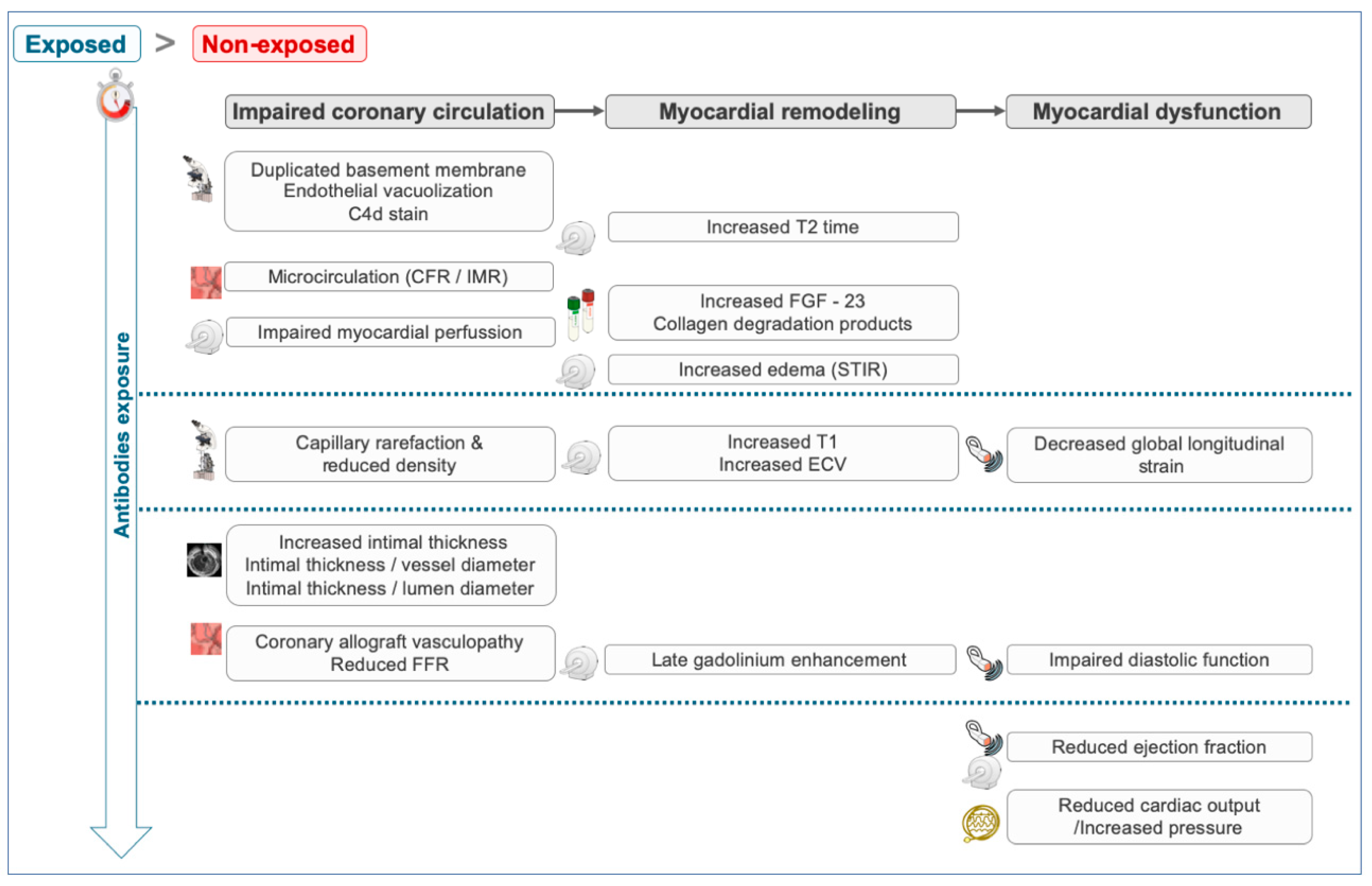
- Endothelial cell vacuolization, subendothelial widening and duplicated basal membranes [12].
- An impaired myocardial perfusion evaluated with cardiac magnetic resonance (CMR)-based quantitative perfusion sequences and with invasive parameters (a pressure guidewire) of microvascular damage (coronary flow reserve and an index of microvascular resistance) [13].
- Increased T2 recovery times in CMR T2 mapping sequences due to intracellular edemas and increased native T1 recovery times and calculated extracellular volume as a sign of myocardial fibrosis [16].
- Subclinical parameters of a myocardial dysfunction (reduced global longitudinal strain in transthoracic echocardiography) [17].
- Signs of coronary allograft vasculopathy in patients with long-term exposure, including a reduced fractional flow reserve (guidewire pressure) and increased intimal thickness (intravascular ultrasound (IVUS)) [18].
- Diastolic and systolic dysfunctions in patients with an established chronic rejection.
- Primary objective: To determine whether, in HT patients, a structural graft injury is modified or accelerated in patients exposed to anti-HLA antibodies compared with non-exposed contemporary HT patients through a thorough evaluation with TEM, OM and IHC techniques.
- Secondary objectives:
- ○
- An assessment of the predictive performance of different diagnostic tools (CMR, transthoracic echocardiography, serum markers of fibrosis, intracoronary pressure guidewire and IVUS) to detect tissue damage using TEM, OM and IHC techniques as the combined reference standard.
- ○
- An estimation of the risk of adverse outcomes as a function of time from anti-HLA antibody positivity.
3.2. Study Population
3.3. Sample Size Estimation
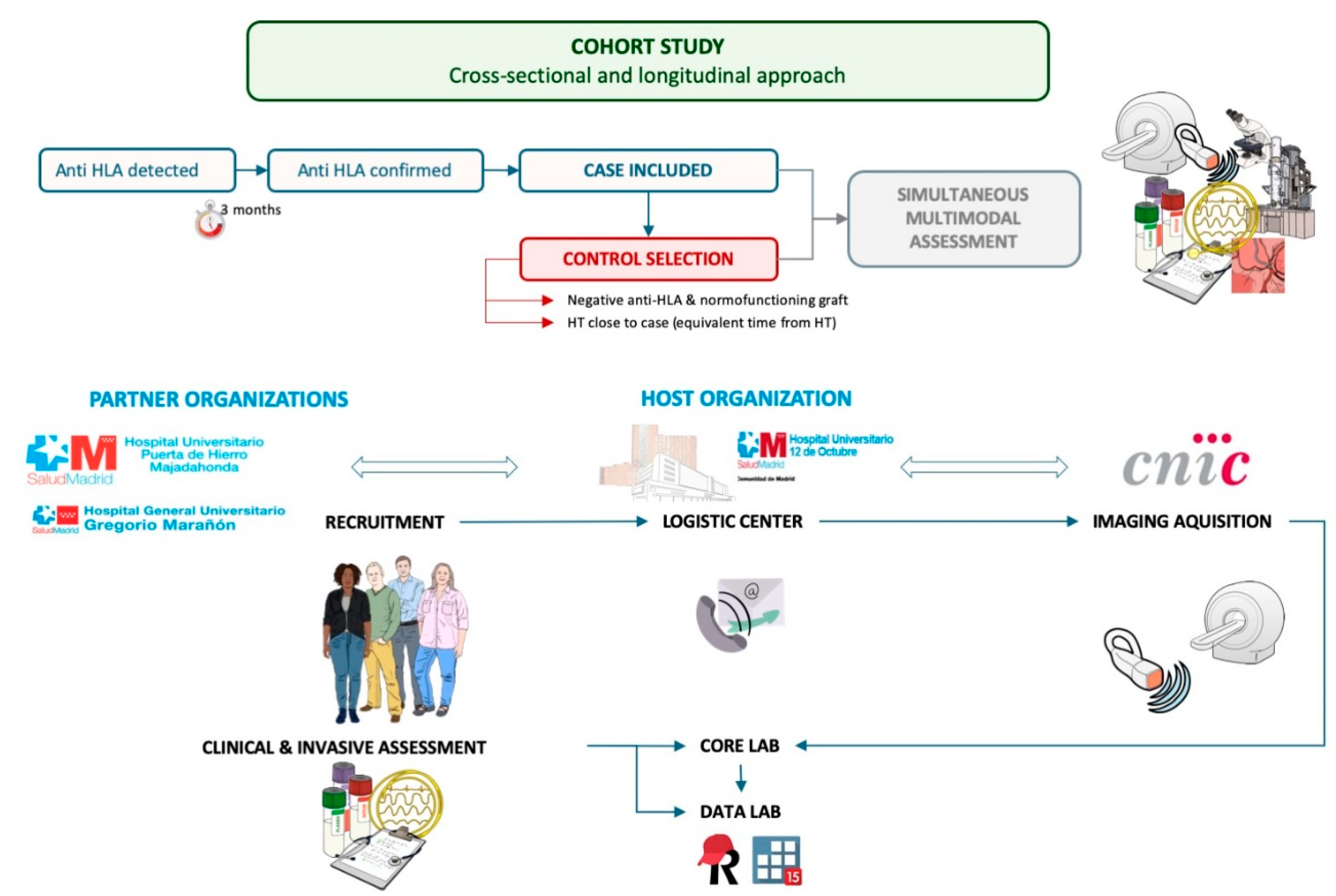
3.4. Study Design
3.5. Assessment Variables
- Primary outcomes: individual and combined structural graft injury outcomes based on the presence of microvascular inflammation, intimal or transmural arteritis or thrombotic microangiopathy (OM); linear C4d staining (%) (IHC); and endothelial edema and vacuolization (semi-quantitative score), subendothelial widening (pm) and basal membrane duplication (TEM).
- For the secondary objectives:
- ○
- Microvascular damage assessment: Index of microcirculatory resistance and coronary flow reserve (pressure guidewire), a CMR-based quantitative perfusion assessment (mL/min/100 g of tissue) and the capillary density (capillaries/mm2) (OM).
- ○
- CMR T2 mapping (ms) to detect intracellular edemas (endothelial vacuolization).
- ○
- CMR T1 mapping (ms) and CMR extracellular volume quantification (%) as well as TTE-based global longitudinal strain (%) to identify myocardial remodeling and fibrosis.
- ○
- Fibroblast growth factor 23 (R.U./mL), procollagen type 1 carboxy-terminal propeptide (µg/L) and collagen type 1 C-terminal telopeptide (µg/L) as the serum markers of fibrosis and remodeling.
- ○
- FFR (coronary physiology) and IVUS-based intimal thickness (mm) as early markers of coronary allograft vasculopathy.
- ○
- Rate of antibody-mediated rejection, anti-HLA antibody seroconversion, heart failure and death.
3.6. Data Collection and Statistical Analysis
3.7. Patients and Public Involvement
4. Ethics and Dissemination
4.1. Ethical Considerations
4.2. Dissemination
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Goldfarb, S.; Hayes, D.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Stehlik, J.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-fifth Adult Heart Transplantation Report-2018; Focus Theme: Multiorgan Transplantation. J. Heart Lung Transplant. 2018, 37, 1155–1168. [Google Scholar] [CrossRef] [PubMed]
- López-Sainz, Á.; Barge-Caballero, E.; Barge-Caballero, G.; Couto-Mallón, D.; Paniagua-Martin, M.J.; Seoane-Quiroga, L.; Iglesias-Gil, C.; Herrera-Noreña, J.M.; Cuenca-Castillo, J.J.; Vázquez-Rodríguez, J.M.; et al. Late graft failure in heart transplant recipients: Incidence, risk factors and clinical outcomes. Eur. J. Heart 2018, 20, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Toquet, C.; Rouvier, P.; Beuscart, T.; Bories, M.C.; Varnous, S.; Guillemain, R.; Pattier, S.; Suberbielle, C.; Leprince, P.; et al. Late Failing Heart Allografts: Pathology of Cardiac Allograft Vasculopathy and Association with Antibody-Mediated Rejection. Am. J. Transplant. 2016, 16, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Banner, N.R.; Hamour, I.M.; Ozawa, M.; Goh, A.; Robinson, D.; Terasaki, P.I.; Rose, M.L. De novo donor HLA-specific antibodies after heart transplantation are an independent predictor of poor patient survival. Am. J. Transplant. 2011, 11, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; Colvin, M.; Potena, L.; Dragun, D.; Crespo-Leiro, M.G.; Delgado, J.F.; Olymbios, M.; Parameshwar, J.; Patel, J.; Reed, E.; et al. The management of antibodies in heart transplantation: An ISHLT consensus document. J. Heart Lung Transplant. 2018, 37, 537–547. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2010, 29, 914–956. [Google Scholar] [CrossRef]
- Terasaki, P.I. Humoral theory of transplantation. Am. J. Transplant. 2003, 3, 665–673. [Google Scholar] [CrossRef]
- Tambur, A.R.; Pamboukian, S.V.; Costanzo, M.R.; Herrera, N.D.; Dunlap, S.; Montpetit, M.; Heroux, A. The presence of HLA-directed antibodies after heart transplantation is associated with poor allograft outcome. Transplantation 2005, 80, 1019–1025. [Google Scholar] [CrossRef]
- Loupy, A.; Haas, M.; Roufosse, C.; Naesens, M.; Adam, B.; Afrouzian, M.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Becker, J.U.; et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell- and antibody-mediated rejection. Am. J. Transplant. 2020, 20, 2318–2331. [Google Scholar] [CrossRef]
- Berry, G.J.; Burke, M.M.; Andersen, C.; Bruneval, P.; Fedrigo, M.; Fishbein, M.C.; Goddard, M.; Hammond, E.H.; Leone, O.; Marboe, C.; et al. The 2013 International Society for Heart and Lung Transplantation Working Formulation for the standardization of nomenclature in the pathologic diagnosis of antibody-mediated rejection in heart transplantation. J. Heart Lung Transplant. 2013, 32, 1147–1162. [Google Scholar] [CrossRef] [PubMed]
- Afzali, B.; Chapman, E.; Racapé, M.; Adam, B.; Bruneval, P.; Gil, F.; Kim, D.; Hidalgo, L.; Campbell, P.; Sis, B.; et al. Molecular Assessment of Microcirculation Injury in Formalin-Fixed Human Cardiac Allograft Biopsies with Antibody-Mediated Rejection. Am. J. Transplant. 2017, 17, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.M.; Khush, K.; Luikart, H.; Okada, K.; Lim, H.S.; Kobayashi, Y.; Honda, Y.; Yeung, A.C.; Valantine, H.; Fearon, W.F. Invasive Assessment of Coronary Physiology Predicts Late Mortality After Heart Transplantation. Circulation 2016, 133, 1945–1950. [Google Scholar] [CrossRef] [PubMed]
- López, B.; González, A.; Ravassa, S.; Beaumont, J.; Moreno, M.U.; San José, G.; Querejeta, R.; Díez, J. Circulating Biomarkers of Myocardial Fibrosis: The Need for a Reappraisal. J. Am. Coll. Cardiol. 2015, 65, 2449–2456. [Google Scholar] [CrossRef]
- Vázquez-Sánchez, S.; Poveda, J.; Navarro-García, J.A.; González-Lafuente, L.; Rodríguez-Sánchez, E.; Ruilope, L.M.; Ruiz-Hurtado, G. An Overview of FGF-23 as a Novel Candidate Biomarker of Cardiovascular Risk. Front. Physiol. 2021, 12, 632260. [Google Scholar] [CrossRef]
- Dolan, R.S.; Rahsepar, A.A.; Blaisdell, J.; Suwa, K.; Ghafourian, K.; Wilcox, J.E.; Khan, S.S.; Vorovich, E.E.; Rich, J.D.; Anderson, A.S.; et al. Multiparametric Cardiac Magnetic Resonance Imaging Can Detect Acute Cardiac Allograft Rejection After Heart Transplantation. JACC Cardiovasc. Imaging 2019, 12, 1632–1641. [Google Scholar] [CrossRef]
- Mingo-Santos, S.; Moñivas-Palomero, V.; Garcia-Lunar, I.; Mitroi, C.D.; Goirigolzarri-Artaza, J.; Rivero, B.; Oteo, J.F.; Castedo, E.; González-Mirelis, J.; Cavero, M.A.; et al. Usefulness of Two-Dimensional Strain Parameters to Diagnose Acute Rejection after Heart Transplantation. J. Am. Soc. Echocardiogr. 2015, 28, 1149–1156. [Google Scholar] [CrossRef]
- Kobashigawa, J.A.; Tobis, J.M.; Starling, R.C.; Tuzcu, E.M.; Smith, A.L.; Valantine, H.A.; Yeung, A.C.; Mehra, M.R.; Anzai, H.; Oeser, B.T.; et al. Multicenter intravascular ultrasound validation study among heart transplant recipients: Outcomes after five years. J. Am. Coll. Cardiol. 2005, 45, 1532–1537. [Google Scholar] [CrossRef]
- Wavamunno, M.D.; O’Connell, P.J.; Vitalone, M.; Fung, C.L.; Allen, R.D.; Chapman, J.R.; Nankivell, B.J. Transplant glomerulopathy: Ultrastructural abnormalities occur early in longitudinal analysis of protocol biopsies. Am. J. Transplant. 2007, 7, 2757–2768. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| For Exposed Patients | Recipient of a second HT Multiple organ transplantation Unknown immunological history Recipients sensitized with anti-HLA antibodies against donor HLA before HT CMR contrast not administered with GFR < 30 mL/min/1.73 m2 Patients with implantable cardiac devices who did not undergo a CMR study |
| |
| For Non-Exposed Patients | |
| Recipient of a first HT Negative anti-HLA antibodies HT contemporary to the index case |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuche, J.; de la Cruz Bertolo, J.; Marco Clement, I.; Sánchez, V.S.; Sarnago Cebada, F.; Mancebo, E.; Enguita, A.B.; Alonso-Riaño, M.; Ruiz-Hurtado, G.; López-Azor, J.C.; et al. Rationale and Protocol of the Multimodality Evaluation of Antibody-Mediated Injury in Heart Transplantation (LEONE-HT) Observational Cross-Sectional Study. Methods Protoc. 2022, 5, 75. https://doi.org/10.3390/mps5050075
Nuche J, de la Cruz Bertolo J, Marco Clement I, Sánchez VS, Sarnago Cebada F, Mancebo E, Enguita AB, Alonso-Riaño M, Ruiz-Hurtado G, López-Azor JC, et al. Rationale and Protocol of the Multimodality Evaluation of Antibody-Mediated Injury in Heart Transplantation (LEONE-HT) Observational Cross-Sectional Study. Methods and Protocols. 2022; 5(5):75. https://doi.org/10.3390/mps5050075
Chicago/Turabian StyleNuche, Jorge, Javier de la Cruz Bertolo, Irene Marco Clement, Violeta Sánchez Sánchez, Fernando Sarnago Cebada, Esther Mancebo, Ana Belén Enguita, Marina Alonso-Riaño, Gema Ruiz-Hurtado, Juan Carlos López-Azor, and et al. 2022. "Rationale and Protocol of the Multimodality Evaluation of Antibody-Mediated Injury in Heart Transplantation (LEONE-HT) Observational Cross-Sectional Study" Methods and Protocols 5, no. 5: 75. https://doi.org/10.3390/mps5050075