An Appraisal of Antidotes’ Effectiveness: Evidence of the Use of Phyto-Antidotes and Biotechnological Advancements

 , and
, and
Abstract
:1. Introduction
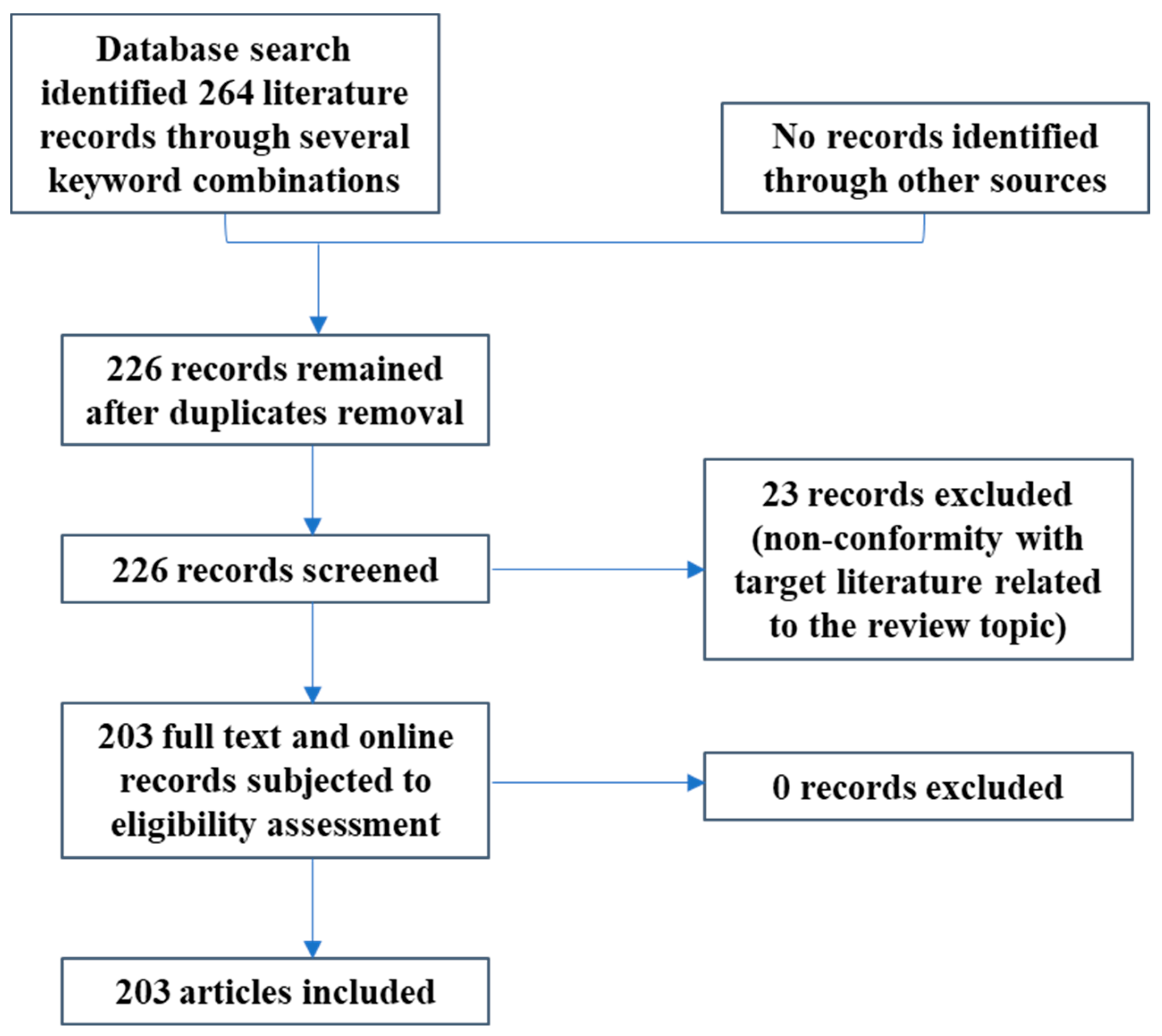
2. Materials and Methods
3. Results and Discussion
3.1. Classes of Antidotes and Mechanism(s) of Action
3.1.1. Competitive Antagonists
3.1.2. Chelating Agents
3.1.3. Acceleration of Detoxification
3.1.4. Reduced Toxicity
3.1.5. Receptor Site Blocker
3.1.6. Cyanide Binders/Sulphur Donors
3.1.7. Cardiac Drug Antidotes
3.1.8. Universal/General Antidotes
3.2. In vitro Studies on the Use of Antidotes
3.3. In vivo Studies On The Use Of Antidotes
3.4. Snake Venoms As Poisons
3.4.1. Cytotoxins
3.4.2. Hemotoxins
3.4.3. Neurotoxins
Calciseptine
Cobrotoxins
Calcicludine
Fasciculin-II
Caliotoxins
Bungarotoxins
3.5. Natural antidotes of plant origin
3.5.1. Evidence of use and effectiveness against snakebite and other animals’ poisons
3.5.2. Evidence of use and effectiveness against other toxins/poisons
4. Future Prospects And Biotechnological Advancements In Antidote Administration
5. Conclusions
Funding
Conflicts of Interest
References
- Centre for Disease Control (CDC). Injury Prevention and Control: Leading Causes of Non-Fatal Injury Reports, 2001–2012. WISQARS Non-Fatal Injury Queries. 2013. Available online: http://webappa.cdc.gov/sasweb/ncipc/nfilead2001.html (accessed on 10 December 2019).
- Buckley, N.A.; Eddleston, M.; Dawson, A.H. The need for translational research on antidotes for pesticide poisoning. Clin. Exp. Pharmacol. Physiol. 2005, 32, 999–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunnell, D.; Eddleston, M. Suicide by intentional ingestion of pesticides: A continuing tragedy in developing countries. Int. J. Epidemiol. 2003, 32, 902–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Capital Poison Centre (NCPC). Available online: www.poison.org/poison-statistics-national-data2017 (accessed on 18 December 2019).
- Sohn, C.H.; Ryoo, S.M.; Lim, K.S.; Kim, W.; Lim, H.; Oh, B.J. Kind and estimated stocking amount of antidotes for initial treatment for acute poisoning at emergency medical centers in Korea. J. Korean Med. Sci. 2014, 29, 1562–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, D.; Desel, H. Common causes of poisoning: Etiology, diagnosis and treatment. Dtsch. Arztebl. Int. 2013, 110, 690–700. [Google Scholar]
- Sgrignolli, L.R.; Mendes, G.E.F.; Carlos, C.P.; Burdmann, E.A. Acute kidney injury caused by Bothrops snake venom. Nephron Clin. Pract. 2011, 119, 131–137. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Health Observatory (GHO) Data; World Health Statistics; WHO, 2015; Available online: https://www.who.int/gho/publications/world_health_statistics/2015/en/ (accessed on 8 December 2019).
- World Health Organization (WHO). Unedited Report of the 17th Expert Committee on the Selection and Use of Essential Medicines; WHO Technical Report Series; WHO, 2009; Available online: https://www.who.int/selection_medicines/committees/expert/17/en/ (accessed on 28 November 2019).
- Nikfar, S.; Khatibi, M.; Abdollahiasl, A.; Abdollahi, M. Cost and utilization study of antidotes: An Iranian experience. Int. J. Pharmacol. 2011, 7, 46–49. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Training and Guidance—Poison Information, Prevention and Management, 2019. Available online: https://www.who.int/ipcs/publications/training_poisons/guidelines_poison_control/en/index7.html (accessed on 16 December 2019).
- Dines, A.; Dargan, P.; Nash, S. Poisoning. Hosp. Pharm. 2007, 50, 10. [Google Scholar]
- Meredith, T.J.; Jacobsen, D.; Haines, J.A.; Berger, J.C.; World Health Organization. Naloxone, Flumazenil and Dantrolene as Antidotes; No. EUR 14797 EN of the Commission of the European Communities, Dissemination of Scientific and Technical Knowledge Unit, Directorate-General Information Technologies and Industries, and Telecommunications, Luxembourg; Cambridge University Press: Cambridge, UK, 1993. [Google Scholar]
- Smollin, C.G. Toxicology: Pearls and pitfalls in the use of antidotes. Emerg. Med. Clin. 2010, 28, 149–161. [Google Scholar] [CrossRef]
- Dart, R.C.; Goldfrank, L.R.; Erstad, B.L.; Huang, D.T.; Todd, K.H.; Weitz, J.; Bebarta, V.S.; Caravati, E.M.; Henretig, F.M.; Delbridge, T.R.; et al. Expert consensus guidelines for stocking of antidotes in hospitals that provide emergency care. Ann. Emerg. Med. 2017, 71, 314–325. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.Y.; Kazzi, Z.N. Antidotes and rescue therapies. Curr. Pharm. Biotechnol. 2012, 13, 1914–1916. [Google Scholar] [CrossRef]
- Burda, A.M.; Uthaivongsakdi, K.T.; Sigg, T.; Wahl, M. Availability of pralidoxime and implications of inadequate stocking. Am. J. Health Syst. Pharm. 2004, 61, 1336–1337. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, J. Bioterrorism threat shines spotlight on drug manufacturing. Pharm. Technol. 2001, 13, 14–22. [Google Scholar]
- Mowry, J.B.; Spyker, D.A.; Brooks, D.E.; Zimmerman, A.; Schauben, J.L. 2015 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 33rd Annual Report. Clin. Toxicol. 2016, 54, 924–1109. [Google Scholar] [CrossRef]
- Mansour, A.; Al-Bizri, L.; El-Maamary, J.; Al-Helou, A.; Hamade, R.; Saliba, E.; Khammash, D.; Makhoul, K.; Matli, K.; Ghosn, N.; et al. National study on the adequacy of antidotes stocking in Lebanese hospitals providing emergency care. BMC Pharmacol. Toxicol. 2016, 17, 51. [Google Scholar] [CrossRef] [Green Version]
- Thanacoody, R.H.; Aldridge, G.; Laing, W.; Dargan, P.I.; Nash, S.; Thompson, J.P.; Vale, A.; Bateman, N.; Thomas, S. National audit of antidote stocking in acute hospitals in the UK. Emerg. Med. J. 2013, 30, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Salem, W.A.; Salameh, R.; Qureshi, I.; Al-Bukari, A.A.M.A.; Shaat, E.B.J.S.; Moinudheen, J.; Hoffman, R.J.; Aleassi, G. Appropriate utilization and stocking of antidotes in Qatar public hospitals. Asia Pac. J. Med. Toxicol. 2017, 6, 72–78. [Google Scholar]
- Gasco, L.; Rosbolt, M.B.; Bebarta, V.S. Insufficient stocking of cyanide antidotes in US hospitals that provide emergency care. J. Pharmacol. Pharmacother. 2013, 4, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Dart, R.C.; Borron, S.W.; Caravati, E.M.; Cobaugh, D.J.; Curry, S.C.; Falk, J.L.; Goldfrank, L.; Gorman, S.E.; Groft, S.; Heard, K.; et al. Expert consensus guidelines for stocking of antidotes in hospitals that provide emergency care. Ann. Emerg. Med. 2009, 54, 386–394. [Google Scholar] [CrossRef]
- Brent, J. Translational antidote research: A bedside to bench tale. Asia Pac. J. Med. Toxicol. 2015, 4, 9–12. [Google Scholar]
- Caoili, E.S. Antidotes, antibody-mediated immunity and the future of pharmaceutical product development. Hum. Vaccin. Immunother. 2013, 9, 294–299. [Google Scholar] [CrossRef] [Green Version]
- Gomes, A.; Das, R.; Sarkhel, S.; Mishra, R.; Mukherjee, S.; Bhattacharya, S.; Gomes, A. Herbs and herbal constituents active against snake bite. Indian J. Exp. Biol. 2010, 48, 865–878. [Google Scholar] [PubMed]
- Soares, A.M.; Ticli, F.K.; Marcussi, S.; Lourenco, M.V.; Januario, A.H.; Sampaio, S.V.; Giglio, J.R.; Lomonte, B.; Pereira, S. Medicinal plants with inhibitory properties against snake venoms. Curr. Med. Chem. 2005, 12, 2625–2641. [Google Scholar] [CrossRef] [PubMed]
- Pillay, V. Current views on antidotal therapy in managing cases of poisoning and overdose. J. Assoc. Physicians India 2008, 56, 881–892. [Google Scholar] [PubMed]
- Dear, J.W. Clinical Biochemistry: Metabolic and Clinical Aspects, 3rd ed.; Churchill Livingstone: London, UK, 2014. [Google Scholar]
- National Poison Information Centre (NPIC). List of Antidotes of Common Poisonings. Department of Pharmacology, AIIMS: New Delhi, India, 2017; Available online: https://www.ncpacsag.ac.in/npic.html (accessed on 10 December 2019).
- Mikirova, N.; Casciari, J.; Hunninghake, R. Efficacy of oral DMSA and intravenous EDTA in chelation of toxic metals and improvement of the number of stem/progenitor cells in circulation. Transl. Biomed. 2011, 2, 424. [Google Scholar]
- Blanusa, M.; Varnai, V.M.; Piasek, M.; Kostial, K. Chelators as antidotes of metal toxicity: Therapeutic and experimental aspects. Curr. Med. Chem. 2005, 12, 2771–2794. [Google Scholar] [CrossRef]
- Bernal, W.; Wendon, J. Acute liver failure. N. Engl. J. Med. 2013, 369, 2525–2534. [Google Scholar] [CrossRef]
- Miners, J.O.; Drew, R.; Birkett, D.J. Mechanism of action of paracetamol protective agents in mice in vivo. Biochem. Pharmacol. 1984, 33, 2995–3000. [Google Scholar] [CrossRef]
- Bateman, D.N.; Carroll, R.; Pettie, J.; Yamamoto, T.; Elamin, M.E.; Peart, L.; Dow, M.; Coyle, J.; Cranfield, K.R.; Hook, C.; et al. Effect of the UK’s revised paracetamol poisoning management guidelines on admissions, adverse reactions and costs of treatment. Br. J. Clin. Pharmacol. 2014, 78, 610–618. [Google Scholar] [CrossRef]
- Bateman, D.N.; Dear, J.W. Acetylcysteine in paracetamol poisoning: A perspective of 45 years of use. Toxicol. Res. 2019, 8, 489–498. [Google Scholar] [CrossRef]
- Bhattacharya, R. Antidotes to cyanide poisoning: Present status. Indian J. Pharmacol. 2000, 32, 94–101. [Google Scholar]
- Maduh, E.U. Mechanism of Cyanide Neurotoxicity. Ph.D. Thesis, Purdue University, West Lafayette, IN, USA, 1989. [Google Scholar]
- Baskin, S.I.; Porter, D.W.; Rockwood, G.A.; Romano, J.A., Jr.; Patel, H.C.; Kiser, R.C.; Cook, C.M.; Ternay, A.L., Jr. In vitro and in vivo comparison of sulphur donors as antidotes to acute cyanide intoxication. J. Appl. Toxicol. 1999, 19, 173–183. [Google Scholar] [CrossRef]
- Lu, G.; DeGuzman, F.R.; Hollenbach, S.J.; Karbarz, M.J.; Abe, K.; Lee, G.; Luan, P.; Hutchaleelaha, A.; Inagaki, M.; Conley, P.B.; et al. A specific antidote for reversal of anticoagulation by direct and indirect inhibitors of coagulation factor Xa. Nat. Med. 2013, 19, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Furie, B.; Bouchard, B.A.; Furie, B.C. Vitamin K-dependent biosynthesis of gammacarboxyglutamic acid. Blood. 1999, 93, 1798–1808. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, H.J.M. Prothrombin complex concentrate, a general antidote for oral anticoagulation. In Anticoagulation Therapy; Basaran, O., Biteker, M., Eds.; IntechOpen: London, UK, 2016; pp. 79–109. [Google Scholar]
- Crowther, M.; Crowther, M.A. Antidotes for novel oral anticoagulants: Current status and future potential. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1736–1745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, A.; Liu, D. Novel antidotes for target specific oral anticoagulants. Exp. Hematol. Oncol. 2015, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- Forster, V.; Leroux, J.C. Injectable Nano-Antidotes (Nanotidotes) for the Treatment of Drug Overdose and Poisoning. 2015. Available online: https://pdfs.semanticscholar.org/d7f4/b0a015774b2aa66dd22f3112053dc3e287f2.pdf (accessed on 20 November 2019).
- Lapus, R.M. Activated charcoal for pediatric poisonings: The universal antidote? Curr. Opin. Pediatr. 2007, 19, 216–222. [Google Scholar] [CrossRef]
- Worek, H.; Eyer, P.; Aurbek, N.; Szinicz, L.; Thiermann, H. Recent advances in evaluation of oxime efficacy in nerve agent poisoning by in vitro analysis. Toxicol. Appl. Pharmacol. 2007, 219, 226–234. [Google Scholar] [CrossRef]
- Trümpler, S.; Nowak, S.; Meermann, B.; Wiesmüller, G.A.; Buscher, W.; Sperling, M.; Karst, U. Detoxification of mercury species—An in vitro study with antidotes in human whole blood. Anal. Bioanal. Chem. 2009, 395, 1929–1935. [Google Scholar] [CrossRef]
- Berend, S.; Vrdoljak, A.L.; Radic, B.; Kuca, K. New bispyridinium oximes: In vitro and in vivo evaluation of their biological efficiency in soman and tabun poisoning. Chem. Biol. Interact. 2008, 175, 413–416. [Google Scholar] [CrossRef]
- Kovarik, Z.; Vrdoljak, A.; Berend, S.; Katalinic, M.; Kuca, K.; Musilek, K.; Radic, B. Evaluation of oxime K203 as antidote in tabun poisoning. Arch. Ind. Hyg. Toxicol. 2009, 60, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Fischer, A.B.; Hess, C.; Neubauer, T.; Eikmann, T. Testing of chelating agents against lead toxicity using mammalian cell cultures. Analyst 1998, 123, 55–58. [Google Scholar] [CrossRef]
- Dawson, R.M. Review of oximes available for treatment of nerve agent poisoning. J. Appl. Toxicol. 1994, 14, 317–331. [Google Scholar] [CrossRef]
- Peter, J.V.; Moran, J.L.; Graham, P. Oxime therapy and outcomes in human organophosphate poisoning: An evaluation using metanalytic techniques. Crit. Care Med. 2006, 34, 502–510. [Google Scholar] [CrossRef]
- Eddleston, M.; Szinicz, L.; Eyer, P.; Buckley, N. Oximes in acute organophosphorus pesticide poisoning: A systematic review of clinical trials. QJM Int. J. Med. 2002, 95, 275–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sit, R.K.; Kovarik, Z.; Hrvat, N.M.; Žunec, S.; Green, C.; Fokin, V.V.; Sharpless, K.B.; Radić, Z.; Taylor, P. Pharmacology, pharmacokinetics, and tissue disposition of zwitterionic hydroxyiminoacetamido alkylamines as reactivating antidotes for organophosphate exposure. J. Pharmacol. Exp. Ther. 2018, 367, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Kuča, K.; Cabal, J.; Jun, D.; Kassa, J.; Bartosova, L.; Kunesova, G.; Dohnal, V. Strategy for the development of new acetylcholinesterase reactivators–antidotes used for treatment of nerve agent poisonings. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2005, 149, 429–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worek, F.; Kirchner, T.; Szinicz, L. Effect of atropine and bispyridinium oximes on respiratory and circulatory function in guinea-pigs poisoned by sarin. Toxicology 1995, 95, 123–133. [Google Scholar] [CrossRef]
- Golderman, V.; Shavit-Stein, E.; Tamarin, I.; Rosman, Y.; Shrot, S.; Rosenberg, N.; Maggio, N.; Chapman, J.; Eisenkraft, A. The organophosphate paraoxon and its antidote obidoxime inhibit thrombin activity and affect coagulation in vitro. PLoS ONE 2016, 11, e0163787. [Google Scholar] [CrossRef] [Green Version]
- Lovrić, J.; Berend, S.; Vrdoljak, A.L.; Radić, B.; Katalinić, M.; Kovarik, Z.; Želježić, D.; Kopjar, N.; Rast, S.; Mesić, M. A conjugate of pyridine-4-aldoxime and atropine as a potential antidote against organophosphorus compounds poisoning. Acta Biochim. Pol. 2011, 58, 193–198. [Google Scholar] [CrossRef]
- Kalagatur, N.K.; Karthick, K.; Allen, J.A.; Ghosh, N.; Sivaraman, O.; Chandranayaka, S.; Gupta, V.K.; Krishna, K.; Mudili, V. Application of activated carbon derived from seed shells of Jatropha curcas for decontamination of zearalenone mycotoxin. Front. Pharmacol. 2017, 8, 760. [Google Scholar] [CrossRef] [Green Version]
- Kalaska, B.; Kaminski, K.; Sokolowska, E.; Czaplicki, D.; Kujdowicz, M.; Stalinska, K.; Bereta, J.; Szczubialka, K.; Pawlak, D.; Nowakowska, M.; et al. Nonclinical evaluation of novel cationically modified polysaccharide antidotes for unfractionated heparin. PLoS ONE 2015, 10, e0119486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szinicz, L.; Worek, F.; Thiermann, H.; Kehe, K.; Eckert, S.; Eyer, P. Development of antidotes: Problems and strategies. Toxicology 2007, 233, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Worek, F.; Reiter, G.; Eyer, P.; Szinicz, L. Reactivation kinetics of acetylcholinesterase from different species inhibited by highly toxic organophosphates. Arch. Toxicol. 2002, 76, 523–529. [Google Scholar] [PubMed]
- Ballatori, N.; Lieberman, M.W.; Wang, W. N-acetlcysteine as an antidote in methylmercury poisoning. Environ. Health Perspect. 1998, 106, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Way, J.L. Cyanide intoxication and its mechanism of antagonism. Ann. Rev. Pharmacol. Toxicol. 1984, 24, 451–481. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, B.; Vijayaraghavan, R. Promising role of α-Ketoglutarate in protecting against the lethal effects of cyanide. Hum. Exp. Toxicol. 2002, 21, 297–303. [Google Scholar] [CrossRef]
- Mikirova, N.; Casciari, J.; Hunninghake, R.; Riordan, N. EDTA chelation therapy in the treatment of toxic metals exposure. Spatula DD 2011, 1, 81–89. [Google Scholar] [CrossRef]
- Nath, A.K.; Shi, X.; Harrison, D.L.; Morningstar, J.E.; Mahon, S.; Chan, A.; Sips, P.; Lee, J.; MacRae, C.A.; Boss, G.R.; et al. Cisplatin analogs confer protection against cyanide poisoning. Cell Chem. Biol. 2017, 24, 565–575. [Google Scholar] [CrossRef] [Green Version]
- Van Helden, H.P.M.; van derWiel, H.J.; Wolthuis, O.L. Therapy of organophosphate poisoning: The marmoset as a model for man. Br. J. Pharmacol. 1983, 8, 579–589. [Google Scholar] [CrossRef]
- Maxwell, D.M.; Brecht, K.M. The role of carboxylesterase in species variation of oxime protection against soman. Neurosci. Biobehav. Rev. 1991, 15, 135–139. [Google Scholar] [CrossRef]
- Chen, C.H.; Huang, T.H.; Elzoghby, A.O.; Wang, P.W.; Chang, C.W.; Fang, J.Y. Squarticles as the nanoantidotes to sequester the overdosed antidepressant for detoxification. Int. J. Nanomed. 2017, 12, 8071–8083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhowan, B.; Lim, J.; MacLean, M.D.; Berman, A.G.; Kim, M.K.; Yang, Q.; Linnes, J.; Lee, C.H.; Goergen, C.J.; Lee, H. Simple minimally-invasive automatic antidote delivery device (A2D2) towards closed-loop reversal of opioid overdose. J. Control. Release 2019, 306, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, M.; Abel, M.; Fischer, G.W.; Itzkovich, C.J.; Eisenkraft, J.B. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiology 2006, 105, 217–218. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, G.L.; VadeBoncouer, T.; Ramaraju, G.A.; Garcia-Amaro, M.F.; Cwik, M.J. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaine-induced asystole in rats. Anesthesiology 1998, 88, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Forster, V.; Leroux, J.C. Nano-antidotes for drug overdose and poisoning. Sci. Transl. Med. 2015, 7, 290ps14. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.; Heard, K.; Foran, M.; Koyfman, A. Intravenous lipid emulsion in the emergency department: A systematic review of recent literature. J. Emerg. Med. 2015, 48, 387–397. [Google Scholar] [CrossRef]
- Kiss, L.; Bocsik, A.; Walter, F.R.; Ross, J.; Brown, D.; Mendenhall, B.A.; Crews, S.R.; Lowry, J.; Coronado, V.; Thompson, D.E.; et al. From the cover: In vitro and in vivo blood-brain barrier penetration studies with the novel cyanide antidote candidate dimethyl trisulfide in mice. Toxicol. Sci. 2017, 160, 398–407. [Google Scholar] [CrossRef]
- Yin, J.; Fung, M.; Cherwonogrodzky, J.W. Discovery of an effective ricin antidote: An old drug for a new use. In Ricin Toxin; Bentham Science: Sharjah, UAE, 2014; Chapter 10; pp. 182–196. [Google Scholar]
- Frawley, K.L.; Carpenter, T.S.; Bae, Y.; Pearce, L.L.; Peterson, J. A Comparison of potential azide antidotes in a mouse model. Chem. Res. Toxicol. 2020. [Google Scholar] [CrossRef]
- Brent, J.; Burkhart, K.; Dargan, P.; Hatten, B.; Magarbane, B.; Palmer, R.; White, J. Critical Care Toxicology—Diagnosis and Management of Critically Poisoned Patients, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Yang, L.Z.; Xia, B.; Hai-xue, Y.K. Isolation and identification of chemical constituents of alkaloids from the Datura Metel L. Acta Chin. Med. Pharmacol. 2010, 5, 35. [Google Scholar]
- Vyas, V.K.; Brahmbhatt, K.; Bhatt, H.; Parmar, U. Therapeutic potential of snake venom in cancer therapy: Current perspective. Asian Pac. J. Trop. Biomed. 2013, 3, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Marsh, N.; Williams, V. Practical application of snake venom toxins in haemostasis. Toxicon 2005, 45, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wei, L.J. ACTX-8, a cytotoxic L-amino acid oxidase isolated from Agkistrodon acutus snake venom, induces apoptosis in Hela cervical cancer cells. Life Sci. 2007, 80, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Dubovskii, P.V.; Utkin, Y.N. Cobra cytotoxins: Structural organization and antibacterial activity. Acta Nat. 2014, 6, 11–18. [Google Scholar] [CrossRef]
- Nielsen, V.G.; Frank, N.; Matika, R.W. Carbon monoxide inhibits hemotoxic activity of Elapidae venom: Potential role of heme. Biometals 2018, 31, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K. Procoagulant snake toxins: Laboratory studies, diagnosis and understanding snakebite coagulopathy. Semin. Thromb. Hemost. 2009, 35, 093–103. [Google Scholar] [CrossRef]
- Rolan, T.D. Neyrotoxic snakes of the Americas. Neurol. Clin. Pract. 2015, 5, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Joseph, R.; Pahari, S.; Hodgson, W.C.; Kini, R.M. Hypotensive agents from snake venoms. Curr. Drug Targets Cardiovasc. Haematol. Disord. 2004, 4, 437–459. [Google Scholar] [CrossRef]
- Watanabe, T.X.; Itahara, Y.; Kuroda, H.; Chen, Y.N.; Kimura, T.; Sakakibara, S. Smooth muscle relaxing and hypotensive activities of synthetic calciseptine and the homologous snake venom peptide FS2. Jpn. J. Pharmacol. 1995, 68, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.C.; Chang, C.C.; Hayashi, K.; Suzuki, T. Amino acid composition and end group analysis of cobrotoxin. Toxicon 1969, 7, 43–47. [Google Scholar] [CrossRef]
- Gilquin, B.; Lecoq, A.; Desne, F.; Guenneugues, M.; Zinn-Justin, S.; Menez, A. Conformational and structural variability supported by the BPTI fold: Solution structure of the Ca2+ channel calcicludine. Proteins Struct. Funct. Bioinform. 1999, 34, 520–532. [Google Scholar] [CrossRef]
- Rajendran, B.K.; Suresh, M.X.; Bhaskaran, S.P.; Harshitha, Y.; Gaur, U.; Kwok, H.F. Pharmacoinformatic approach to explore the antidote potential of phytochemicals on bungarotoxin from Indian Krait, Bungarus caeruleus. Comput. Struct. Biotechnol. J. 2018, 16, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Teron, R.; Borthakur, S.K. Folklore claims of some medicinal plants as antidote against poisons among the Karbis of Assam, India. Pleione 2013, 7, 346–356. [Google Scholar]
- Castaneda, I.C.H.; Pereanez, J.A.; Preciado, L.M. Synthetic inhibitors of snake venom enzymes: Thioesters derived from 2-sulfenyl ethylacetate. Pharmaceuticals 2019, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mhaskar, K.S.; Caius, J.F. Indian plant remedies in snakebites. Indian J. Med. Res. 1931, 19, 28. [Google Scholar]
- Otero, R.; Nunez, V.; Barona, J.; Saldarriaga, M.; Osorio, R.G.; Fonnegra, R.; Jiminez, S.L.; Diaz, A. Snakebites and ethnobotany in the northwest region of Colombia. Part III: Neutralization of the hemorrhagic effect of Bothrops atrox venom. J. Ethnopharmacol. 2000, 73, 233–241. [Google Scholar] [CrossRef]
- Nunez, V.; Otero, R.; Barona, J.; Saldarriaga, M.; Osorio, R.G.; Fonnegra, R.; Jiminez, S.L.; Diaz, A.; Quintana, J.C. Neutralization of the edema-forming, defibrinating and coagulant effects of Bothrops asper venom by extracts of plants used by healers in Colombia. Braz. J. Med. Biol. Res. 2004, 37, 969–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratanabanangkoon, K.; Cherdchu, C.; Chudapongse, P. Studies on the cobra neurotoxin inhibiting activity in an extract of Curcuma longa (Zingiberaceae) rhizome. Southeast Asia J. Trop. Med. Public Health 1993, 24, 178. [Google Scholar]
- Deepa, M.; Gowda, T.V. Purification and characterization of a glycoprotein inhibitor of toxic phospholipase from Withania somnifera. Arch. Biochem. Biophys. 2002, 408, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.I.; Gomes, A. Snake venom neutralization by Indian medicinal plants (Vitea negendo and Embelica officinalis) root extracts. J. Ethnopharmacol. 2003, 86, 75–80. [Google Scholar] [CrossRef]
- Alam, M.I.; Auddy, B.; Gomes, A. Isolation, purification and partial characterization of viper venom neutralizing factor from the root extract of Indian medicinal plant Hemidesmus indicus R.Br. Toxicon 1994, 32, 1551–1557. [Google Scholar] [CrossRef]
- Alam, M.I.; Gomes, A. Viper venom-induced inflammation and inhibition of free radical formation by pure compound (2-hydroxy-4-methoxy benzoic acid) isolated and purified from anantamul (Hemisdesmus indicus R.Br) root extract. Toxicon 1998, 36, 207–215. [Google Scholar] [CrossRef]
- Ode, O.J.; Asuzu, I.U. The anti-snake venom activities of the methanolic extract of the bulb of Crinum jagus (Amarylidaceae). Toxicon 2006, 48, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, D.; Mukherjee, S.; Smith, M.G.; Das, S.K. Role of sphingomyelinase in the environmental toxin induced apoptosis of pulmonary cells. In Lipids: Sphingolipid Metabolizing Enzymes; Haldar, D., Das, S.K., Eds.; Research Signpost Publishers: Trivandrum, India, 2004; pp. 117–139. [Google Scholar]
- Hung, Y.C.; Sava, V.; Hung, M.Y.; Huang, G.S. Inhibitory effects on phospholipase A2 and antivenin activity of melanin extracted from Thea sinensis Linn. Life Sci. 2004, 74, 2037–2047. [Google Scholar] [CrossRef] [PubMed]
- Vale, L.H.F.; Mendes, M.M.; Hamaguchi, A.; Soares, A.M.; Rodrigues, V.M.; Homsi-Brandeburgo, M.I. Neutralization of pharmacological and toxic activities of bothrops snake venoms by Schizolobium parahyba (Fabaceae) aqueous extract and its fractions. Basic Clin. Pharmacol. Toxicol. 2008, 103, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.I.; Gomes, A. Adjuvant effects and antiserum action potentiation by a (herbal) compound 2-hydroxy-4-methoxy benzoic acid isolated from the root extract of the Indian medicinal plant ‘sarsaparilla’ (Hemidesmus indicus R.Br.). Toxicon 1998, 36, 1423–1431. [Google Scholar] [CrossRef]
- Alam, M.I. Studies on the Anti-Snake Venom Activity of Selected Plants. Ph.D. Thesis, University of Calcutta, Calcutta, India, 1997. [Google Scholar]
- Chatterjee, I.; Chakravarty, A.K.; Gomes, A. Daboia russellii and Naja kaouthia venom neutralization by lupeol acetate isolated from the root extract of Indian sarsaparilla Hemidesmus indicus R.Br. J. Ethnopharmacol. 2006, 106, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, U.P.; Melo, J.G.; Medeiros, M.F.; Menezes, I.R.; Moura, G.J.; Asfora El-Deir, A.C.; Nóbrega Alves, R.R.; de Medeiros, P.M.; de Sousa Araújo, T.A.; Alves Ramos, M.; et al. Natural products from ethnodirected studies: Revisiting the ethnobiology of the zombie poison. Evid. Based Complement. Alternat. Med. 2012, 2012, 202508. [Google Scholar] [CrossRef]
- Singha, M.K.; Patel, D.K.; Kanungo, V.K. Medicinal plants used as antidotes in northern part of Bastar district of Chhattisgarh. J. Ecobiotechnol. 2012, 4, 58–60. [Google Scholar]
- Mahomoodally, M.F. Traditional medicines in Africa: An appraisal of ten potent African medicinal plants. Evid. Based Complement. Alternat. Med. 2013, 2013, 617459. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, R.; Dutta, A.; Chaudhuri, S.R.; Sharma, N.; Giri, A.K.; Chaudaudri, K. In vitro and in vivo reduction of sodium arsenite induced toxicity by aqueous garlic extract. Food Chem. Toxicol. 2008, 46, 740–751. [Google Scholar] [CrossRef]
- Shafaghati, N.; Hedeyati, M.; Seyed, J.H. Protective effects of curcumin against genoticity induced by 131-iodine in human cultured lymphocyte cells. Pharmacogn. Mag. 2014, 10, 106. [Google Scholar] [PubMed]
- Kumar, R.S.; Matsui, M.; Reybier, K.; Darius, H.T.; Chinain, M.; Pauillac, S.; Laurent, D. Ability of certain plant extracts traditionally used to treat ciguatera fish poisoning to inhibit nitric oxide production in RAW 264.7 macrophages. J. Ethnopharmacol. 2009, 123, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Matsui, M.; Kumar-Roine, S. hilpa, Darius, T.; Chinain, M.; Laurent, D.; Pauillac, S. Characterisation of the anti-inflammatory potential of Vitex trifolia L. (Labiatae), a multipurpose plant of the Pacific traditional medicine. J. Ethnopharmacol. 2009, 126, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Institut de Recherche Pour le Développement (IRD) Update. Ciguatera Fish Poisoning: Traditional Remedies the Source of Antidotes. Available online: https://en.ird.fr/the-media-centre/scientific-newssheets/338-ciguatera-fish-poisoning-traditional-remedies-the-source-of-antidotes (accessed on 29 November 2019).
- World Health Organisation (WHO). Fact Sheet No.134 (December 2008): Traditional Medicine. Available online: http://www.who.int/mediacentre/factsheets/2003/fs134/en/ (accessed on 10 December 2019).
- Burnett, J.C.; Ruthel, G.; Stegmann, C.M.; Panchal, R.G.; Nguyen, T.L.; Hermone, A.R.; Stafford, R.G.; Lane, D.J.; Kenny, T.A.; McGrath, C.F.; et al. Inhibition of metalloprotease botulinum serotype A from a pseudo-peptide binding mode to a small molecule that is active in primary neurons. J. Biol. Chem. 2007, 282, 5004–5014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.B.; Cai, S.; Adler, M.; Singh, B.K.; Parmar, V.S.; Singh, B.R. Natural compounds and their analogues as potent antidotes against the most poisonous bacterial toxin. Appl. Environ. Microbiol. 2018, 84, e01280-18. [Google Scholar] [CrossRef] [Green Version]
- Thyagarajan, B. Antidotes to botulinum neurotoxin. In Biological Toxins and Bioterrorism; Springer Science and Business Media: Dordrecht, The Netherlands, 2015; pp. 375–400. [Google Scholar]
- Noumi, E. Animal and plant poisons and their antidotes in Eseka and Mbalmayo regions, Centre Province, Cameroon. J. Ethnopharmacol. 2004, 93, 231–241. [Google Scholar] [CrossRef]
- Kamble, S.R.; Deokar, R.R.; Patil, S.R.; Mane, S.R. Herbal antidotes used for antivenum treatment from 32-Shirala Tahasil, Dist. Sangli (MS), India. Int. J. Innov. Res. Sci. Eng. Technol. 2015, 4. [Google Scholar] [CrossRef]
- Mors, W.B.; Nascimento, M.C.D.; Parente, J.P.; DaSilva, M.H.; Melo, P.A.; Kurtz, G.S. Neutralization of lethal and myotoxic activities of South American rattlesnake venom by extracts and constituents of the plant Eclipta prostata (Asteraceae). Toxicon 1989, 27, 1003–1009. [Google Scholar] [CrossRef]
- Rita, P.; Animesh, D.K.; Aninda, M.; Benoy, G.K.; Sandip, H. Snake bite, snake venom, antivenom and herbal antidotes—A review. Int. J. Res. Ayuverda Pharm. 2011, 2, 1060–1067. [Google Scholar]
- Ugulu, I. Traditional ethnobotanical knowledge about medicinal plants used for external therapy in Alasehir, Turkey. Int. J. Med. Aromat. Plants 2011, 1, 101–106. [Google Scholar]
- Murugan, P.S.; Ramprasath, T.; Selvam, V. Cardioprotective role of Acalypha indica extract on isoproterenol induced myocardial infarction in rats. J. Pharm. Res. 2011, 4, 2129–2132. [Google Scholar]
- Asad, M.H. Enlisting the scientifically unnoticed medicinal plants of Pakistan as a source of novel therapeutic agents showing antivenom activity. Afr. J. Pharm. Pharmacol. 2011, 5, 2292–2305. [Google Scholar]
- Sehgal, C.K.; Taneja, S.C.; Dhar, K.L.; Atal, C.K. 2′-p-hydroxybenzoyl mussaenosidic acid, a new iridoid glucoside from Vitex negundo. Phytochemistry 1982, 21, 363–366. [Google Scholar] [CrossRef]
- Sehgal, C.K.; Taneja, S.C.; Dhar, K.L.; Atal, C.K. 6′-p-hydroxybenzoyl mussaenosidic acid, an iridoid glucoside from Vitex negundo. Phytochemistry 1983, 22, 1036–1038. [Google Scholar] [CrossRef]
- Kang, J.G.; Shin, S.Y.; Kim, M.J.; Bajpai, V.; Maheshwari, D.K.; Kang, S.C. Isolation and anti-fungal activities of 2-hydroxymethyl-chroman-4-one produced by Burkholderia sp. MSSP. J. Antibiot. 2004, 57, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Chettankumar, M.; Srinivas, L. New biological activity against phospholipase A2 by tumerin, a protein from Curcuma longa L. Biol. Chem. 2009, 389, 299–303. [Google Scholar] [CrossRef]
- Murkherjee, A.K.; Doley, R.; Saikai, D. Isolation of a snake venom, phospholipase A2 (PLA2) inhibitor (AIPLAI) from leaves of Azadirachta indica (Neem): Mechanism of PLA2 inhibitor by AIPLAI in in vitro condition. Toxicon 2008, 51, 1548–1553. [Google Scholar] [CrossRef]
- Leanpolchareanchai, J.; Pithayanukul, P.; Bavovada, R.; Saparpakorn, P. Molecular docking studies and anti-enzymatic activities of Thai mango seed kernel extract against snake venoms. Molecules 2009, 14, 1404–1422. [Google Scholar] [CrossRef] [Green Version]
- DASilva, A.P.; Farina, M.; Franco, J.L.; Dafre, A.L.; Kassa, J.; Kuca, K. Temporal effects of newly developed oximes (K027, K048) on malathion-induced acetylcholinesterase inhibition and lipid peroxidation in mouse prefrontal cortex. Neurotoxicology 2008, 29, 184–189. [Google Scholar] [CrossRef]
- Batina, M.F.; Cintra, A.C.; Veronese, E.L.; Lavrador, M.A.; Giglio, J.R.; Pereira, P.S.; Dias, D.A.; Franca, S.C.; Sampaio, S.V. Inhibition of the lethal and myotoxic effects of Crolatus durissus terrificus venom by Tabernaemontana catharinensis: Identification of one of the active components. Planta Med. 2000, 66, 424–428. [Google Scholar] [CrossRef]
- Januario, A.H.; Santos, S.L.; Marcussi, S.; Mazzi, M.V.; Pietro, R.C.; Sato, D.N. Neo-clerodane diterpenoid, a new metalloprotease snake venom inhibitor from Baccharis trimera (Asteraceae): Anti-proteolytic and anti-hemmorrhagic properties. Chem. Biol. Interact. 2004, 150, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.S.; Pandey, S.C.; Srivastava, S.; Gupta, V.S.; Patro, B.; Ghosh, A.C. Chemistry and medicinal properties of Tinospora cordifolia (guduchi). Indian J. Pharmacol. 2003, 35, 83–91. [Google Scholar]
- Chanda, S.; Bhayani, D.; Desai, D. Polyphenols and flavonoids of twelve Indian medicinal plants. Bioscan 2013, 8, 595–601. [Google Scholar]
- Yusuf, N.A.; Rahim, N.S.M.; Azhar, S.Z.A.; Ghani, K.A.; Sommano, S.; Khalid, N. Adventitious root cultures of Boesenbergia rotunda as a source of Pinostrobin. Int. J. Adv. Sci. Eng. IT 2018, 8, 377–383. [Google Scholar] [CrossRef]
- Johnson, T.S.; Ravishankar, G.A.; Venkataraman, L.V. Elicitation of capsaicin production in freely suspended cells and immobilized cell cultures of Capsicum frutescens mill. Food Biotechnol. 1991, 5, 197–205. [Google Scholar] [CrossRef]
- Sharmila, S.; Kalaichelvi, K.; Dhivya, S.M. Pharmacognostical and phytochemical analysis of Cayratia pedata var. glabra—A vitaceae member. Int. J. Pharm. Sci. Res. 2018, 9, 218–226. [Google Scholar]
- Olalekan, A.J.; Ayodeji, K.E.; Bamidele, I. Nutritional and phytochemical compositions of fireweed (Crassocephalum crepidioides). J. Agric. Technol. 2013, 9, 439–449. [Google Scholar]
- Mungole, A.; Chaturvedi, A. Hibiscus sabdariffa L. a rich source of secondary metabolites. Int. J. Pharm. Sci. Rev. Res. 2011, 6, 83–87. [Google Scholar]
- Leroux, J.C. Injectable nanocarriers for biodetoxification. Nat. Nanotechnol. 2007, 2, 679–684. [Google Scholar] [CrossRef]
- Jin, S.; Sarkar, K.S.; Jin, Y.N.; Liu, Y.; Kokel, D.; Van Ham, T.J.; Roberts, L.D.; Gerszten, R.E.; MacRae, C.A.; Peterson, R.T. An in vivo zebrafish screen identifies organophosphate antidotes with diverse mechanisms of action. J. Biomol. Screen. 2013, 18, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Smith, W.J.; Wang, G.; Gaikwad, H.; Vu, V.P.; Groman, E.; Bourne, D.W.; Simberg, D. Accelerated blood clearance of antibodies by nanosized click antidotes. ACS Nano 2018, 12, 12523–12532. [Google Scholar] [CrossRef] [PubMed]
- Andrew, K.; Michael, F.; Benedict, K.; Nestor, T.; Saadyah, A. Next generation opioid antidotes: Covalent nanoparticles for the delivery of Mu opioid antagonists. In Proceedings of the American Chemical Society 257th National Meeting, Orlando, FL, USA, 31 March–4 April 2019. [Google Scholar]
- Azarov, I.; Wang, L.; Rose, J.J.; Xu, Q.; Huang, X.N.; Belanger, A.; Wang, Y.; Guo, L.; Liu, C.; Ucer, K.B.; et al. Five-coordinate H64Q neuroglobin as ligand-trap antidote for carbon monoxide poisoning. Sci. Transl. Med. 2016, 8, 368–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuddenham, E. Medicine: RNA as drug and antidote. Nature 2002, 419, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Oney, S.; Lam, R.T.; Bompiani, K.M.; Blake, C.M.; Quick, G.; Heidel, J.D.; Liu, J.Y.C.; Mack, B.C.; Davis, M.E.; Leong, K.W.; et al. Development of universal antidotes to control aptamer activity. Nat. Med. 2009, 15, 1224–1228. [Google Scholar] [CrossRef]
- Dubé, P.A.; Monast, P.O. Idarucizumab: A specific antidote for dabigatran. Bull. Inf. Toxicol. 2013, 31, 17–25. [Google Scholar]
- Long, J.B.; Zhang, Y.; Brusic, V.; Chitkushev, L.; Zhang, G. Antidote application: An educational system for treatment of common toxin overdose. In Proceedings of the 8th ACM International Conference on Bioinformatics, Computational Biology, and Health Informatics, Boston, MA, USA, 20–23 August 2017. [Google Scholar]
- Elliott, A.; Dube, P.A.; Cossette-Côté, A.; Patakfalvi, L.; Villeneuve, E.; Morris, M.; Gosselin, S. Intraosseous administration of antidotes—A systematic review. J. Clin. Toxicol. 2017, 55, 1025–1054. [Google Scholar] [CrossRef]
- Isbister, G.K.; Buckley, N.A. Therapeutics in clinical toxicology: In the absence of strong evidence how do we choose between antidotes, supportive care and masterful inactivity. Br. J. Clin. Pharmacol. 2016, 81, 408–411. [Google Scholar] [CrossRef] [Green Version]
- Buckley, N.A.; Dawson, A.H.; Juurlink, D.N.; Isbister, G.K. Who gets antidotes? Choosing the chosen few. Br. J. Clin. Pharmacol. 2016, 81, 402–407. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Antidote | Poisoning Indication(s) | Reference(s) |
|---|---|---|
| Oxygen (Hyperbaric) tetrachloride | Carbon monoxide, cyanide, hydrogen sulfide, carbon | [29,38,39] |
| Physostigmine | Central anticholinergics | [29] |
| Potassium hexacyanoferrate, Diethyldithiocarbamate | Thallium | [29] |
| Succimer (DMSA) | Lead, mercury | [29,30,32] |
| Dimercaprol | Arsenic, copper, mercury, gold | [29,32,33] |
| Pyridoxine | Isoniazid, hydrazines, ethylene glycol, gyrometrine | [29] |
| Flumazenil | Benzodiazepines | [29] |
| Oximes | Organophosphates | [16,29] |
| Zwitterionic hydroxyiminoacetamido alkylamines | Organophosphates | [29] |
| Phytomenadione (Vitamin K) | Coumarin derivatives | [30,41] |
| Dantrolene | Malignant hyperthermia, Malignant neuroleptic syndrome | [29] |
| Sodium thiosuphate | Cyanide, bromate, chlorate, iodine | [12,38,39,40] |
| Activated charcoal | For most poisons, Gastric decontamination | [9,29,47] |
| Sodium bicarbonate | Metabolic acidosis | [29] |
| Heparin | Hypercoagulability | [29] |
| Furosemide | Fluid retention | [29] |
| Lidocaine | Ventricular arrhythmias | [29] |
| Promethazine | Allergic reactions | [29] |
| Copper sulfate | Phosphorus | [29] |
| Levallorphan, Nalorphine | Opiates | [29] |
| Experimental Model | Antidote | Indication | Remark | Reference(s) |
|---|---|---|---|---|
| In vitro | DMSA | Mercury poisoning | Moderately effective | [15] |
| K203 | Tabun gas | Very effective | [17] | |
| EDTA | Lead poisoning | Moderately effective | [18] | |
| DMPS | Lead poisoning | Moderately effective | [18] | |
| DDTC | Lead poisoning | Moderately effective | [18] | |
| Vitamin B1 | Lead poisoning | Moderately effective | [18] | |
| Vitamin B2 | Lead poisoning | Ineffective | [18] | |
| Vitamin B6 | Lead poisoning | Moderately effective | [18] | |
| Vitamin B12 | Lead poisoning | Ineffective | [18] | |
| Vitamin C | Lead poisoning | Moderately effective | [18] | |
| Dex40-GTMAC3 | UFH | Very effective | [62] | |
| ATR-4-OX | Paraxon | Moderately effective | [60] | |
| Activated carbon from Jatropha curcas | Zearalenone | Moderately effective | [61] | |
| Zwitterionic aldoximes | Organo phosphate poisoning | Very effective | [56] | |
| Obidoxime | Paraxon | Very effective | [59] | |
| In vivo | NAC | Mercury poisoning | Very effective | [20] |
| SN | Cyanide poisoning | Moderately effective | [21] | |
| STS | Cyanide poisoning | Moderately effective | [21] | |
| α-KG | Cyanide poisoning | Very effective | [22] | |
| K203 + atropine | Tabun gas | Very effective | [17] | |
| HI-6 + atropine | Soman gas | Very effective | [16] | |
| Calcium EDTA | Lead/Aluminum poisoning | Very effective | [23] | |
| Sodium EDTA | Lead/Aluminum poisoning | Moderately effective | [23] | |
| Cisplatin | Cyanide poisoning | Moderately effective | [69] | |
| Anionic squarticles | Amitriptyline intoxication | Moderately effective | [72] | |
| ILE | Cardiotoxicity | Very effective | [74] | |
| Ethoin | Ricin poisoning | Moderately effective | [79] | |
| Cobalt-macrocylic compounds | Azide/Cyanide toxicity | Moderately effective | [80] |
| Poisons | Plant Used | Family | Part Used | Active Metabolite(S) | Mode of Use | Reference(s) |
|---|---|---|---|---|---|---|
| Snake venom | Bidens Pilosa | Asteraceae | Leaf | Not available | Leaf juice is applied locally | [95,119,124] |
| Desmodium adscendens | Fabaceae | Leaf | Triterpenoid aponins Phenylethylamines Indole-3-alkyl amines | Leaf juice is applied locally | [68,95,119,124] | |
| Palisota barteri | Commelinaceae | Stem | Not available | Powdered plant part is applied locally | [95,119,124] | |
| Rauvolfia vomitoria | Apocynaceae | Fruit, leaf and root bark | Not available | Powdered form of all plant parts is applied locally | [95,119,124] | |
| Allium sativum | Liliaceae | Leaf | Allicin Anthocyanine Scordinine A and B | Leaf paste is applied locally | [27,28,95,106,125,126] | |
| Eclipta prostate | Asteraceae | Whole plant | Sitosterol, Stigmasterol D-mannitol Wedelolactone | Not available | [126] | |
| Citrus limon | Rutaceae | Stem bark | 4-β-glucopyranoside d-limonene linalcol | Powder of stem bark mixed with water is administered orally | [27,28,95,106,125,126,127,128] | |
| Dioscorea alata | Dioscoreaceae | Whole plant | Not available | Paste of whole plant is applied locally | [27,28,95,106,125,126] | |
| Mirabilis jalapa | Nyctaginaceae | Root | Not available | Extract of root is taken orally | [27,28,95,106,125] | |
| Ocimum canum | Lamiaceae | Leaf | Not available | Leaf paste is applied locally | [27,28,95,106,125] | |
| Saccharum bengalense | Poaceae | Root | Not available | Root is chewed | [27,28,95,106,125] | |
| Acalypha indica | Euphorbiaceae | Root | Terpenoids Phenolic compounds Sterols | Root paste is applied locally | [27,28,95,106,129] | |
| Hemidesmus indicus | Asclepediaceae | Root | 2-hydroxy-4-methyl benzoic acid Lupeol acetate | Decoction of root is taken orally | [104,109,111] | |
| Achyranthes aspera | Amaranthaceae | Root | Not available | Root paste is taken with water | [27,28,95,106,125] | |
| Calatropis procera | Asclepidiaceae | Latex | Calotropin Calotropagenin Sterol | Plant latex is applied locally | [27,28,95,106,125,130] | |
| Vitex negundo | Verbenaceae | Leaf | 6′-p-hydroxybenzoyl mussaenosidic acid; 2′-p-hydroxybenzoyl mussaenosidic acid Protocatechuic acid; oleanolic acid; flavonoids | Leaf extract is administered orally | [27,28,95,106,125,130,131,132] | |
| Piper spp. | Piperaceae | Seeds | 4-nerolidylcatechol | Grinded seed is applied locally | [98] | |
| Datura metel | Solanaceae | Leaf and stem | Meteloidine Hyoscyamine Apoatropine Anisodamine Hyoscine Norharman | Infusion of dry leaf and stem is administered orally | [27,28,95,106,125,133] | |
| Curcuma longa | Zingiberaceae | Rhizome | Turmerin | Powder of rhizome is applied locally | [27,28,95,106,125,134] | |
| Azadirachta indica | Meliaceae | Leaf | AIPLAI | Leaf extract is administered orally | [135] | |
| Mimosa pudica | Mimosaceae | Root | 2-Hydroxymethyl- chroman-4-one D-manitolSitosterol | Root extract is administered orally | [27,28,95,106,125,133] | |
| Mangifera indica | Anacardiaceae | Stem bark | Pentagalloyl glucopyranose | Stem bark extract is administered orally | [27,28,95,106,125,136] | |
| Aristolochia spp. | Aristolochiaceae | Leaf | Aristolochic acid | Not available | [28] | |
| Hugonia mystax | Linaceae | Leaf | 2-dodecanol Benzene propanoic acid 2-methyl-1-undecanol | Leaf juice is applied locally | [94] | |
| Cordia verbenacea | Borraginaceae | Leaf | Rosmarinic acid | Not available | [28] | |
| Mikania glomerata | Asteraceae | Leaf | Coumarin | Not available | [28] | |
| Silybum marianum | Asteraceae | Root | Silymarin | Root paste is applied locally | [28] | |
| Casearia sylvestris | Salicaceae | Leaf | Ellagic acid | Not available | [137] | |
| Symplocos racemosa | Symplocaceae | Fruits | Benzolsalireposide salireposide | Not available | [28] | |
| Cynara scolymus | Asteraceae | Fruits | Cynarin | Not available | [28] | |
| Thea sinensis (Camellia sinensis) | Theaceae | Leaf | Melanin | Decoction of leaf is administered orally | [28] | |
| Vernonia condensata | Asteraceae | Leaf | Caffeic acid | Leaf paste is applied locally | [28] | |
| Phyllanthus klotzchianus | Phyllanthaceae | Whole plant | Quercetin Rutin | Whole plant extract is administered orally | [28] | |
| Ceiba pentandra | Malvaceae | Stem bark | 7-hydroxycadalene | Extract of stem bark is administered orally | [94] | |
| Sapindus saponaria | Sapindaceae | Fruits | Flavonoids | Not available | [28] | |
| Periandra mediterranea | Fabaceae | Flower | Triterpenes Sterols Periandrins | Decoction of flower is administered orally | [28] | |
| Mandevilla velutina | Apocynaceae | Leaf | Steroids | Not available | [28] | |
| Derris sericea | Fabaceae | Leaf | Derricidin | Not available | [28] | |
| Guiera senegalensis | Combretaceae | Root | Tannins | Not available | [28] | |
| Harpalyce brasiliana | Fabaceae | Leaf | Edunol | Not available | [28] | |
| Dorstenia brasiliensis | Moraceae | Whole plant | Bergapten | Decoction of whole plant is administered orally | [28] | |
| Ehretia buxifolia | Boraginaceae | Leaf | Ehretianone | Decoction of leaf is administered orally | [28] | |
| Derris urucu | Fabaceae | Leaf | 2,5-dihydroxymethyl-3,4-dihydroxypyrrolidine | Not available | [28] | |
| Bredemeyera floribunda | Polygalaceae | Root | Bredemereyosides B and D | Not available | [28] | |
| Withania somnifera | Solanaceae | Root | Indole-3-(4’-oxo) butyric acid | Powder of dry root is applied locally | [94,101] | |
| Betula alba | Betulaceae | Stem bark | Betulin Betulin acid | Decoction of stem bark is administered orally | [28] | |
| Tabernaemontana catharinensis | Apocynaceae | Stem bark | 12-methoxy-4-methyl voachalotine | Not available | [138] | |
| Pentaclethra macroloba | Fabaceae | Root | Triterpenoid saponin | Not available | [137] | |
| Baccharis trimera | Asteraceae | Leaf | Neo-clerodane diterpenoid | Leaf paste is applied locally | [139] | |
| Pimpinella anisum | Apiaceae | Leaf | Anisic acid | Not available | [105] | |
| Leucas aspera | Lamiaceae | Leaf | Nerolidol-2 | Leaf extract is administered orally | [94] | |
| Murraya paniculata | Rutaceae | Leaf | Trans-nerolidol | Leaf extract is administered orally | [94] | |
| Annona squamosal | Annonaceae | Seed | Eugenol | Seeds are crushed and applied locally | [94] | |
| Bixa Orellana | Bixaceae | Leaf | Germacren-4-ol | Leaf extract is administered orally | [94] | |
| Tinospora cordifolia | Menispermaceae | Leaf | Cordifelone Tinosporidine 3, (a,4-di hydroxy-3-methoxy-benzyl)-4-(4- hydroxy-3-methoxy-benzyl)-tetrahydrofuran | Leaf juice and garlic paste is taken orally | [94,140] | |
| Insecticide/ Pesticide poisoning | Begonia roxburghii | Begoniaceae | Whole plant | Not available | Whole plant extract is administered orally | [95] |
| Polygonum affine | Polygonaceae | Shoot | Not available | Tender shoots are chewed | [95] | |
| Polygonum microcephalum | Polygonaceae | Shoot | Not available | Tender shoots are chewed | [95] | |
| Datura poisoning | Averrhoa carambola | Oxalidaceae | Fruits | Phenols Flavonoids | Fruits are eaten | [95,141] |
| Catfish sting | Boesenbergia rotunda | Zingiberaceae | Rhizome | Pinostrobin | Paste of rhizome is applied locally | [95,142] |
| Bee sting | Capsicum frutescens | Solanaceae | Leaf | Capsaicin | Leaf paste is applied locally | [95,143] |
| Lagenaria siceraria | Cucurbitaceae | Leaf | Not available | Paste of leaf is applied locally | [95] | |
| Food poisoning | Cayratia pedate | Vitaceae | Leaf | Triterpenoids Steroids Tannins Phenols | Decoction of leaf is administered orally | [95,144] |
| Xanthium strumarium | Asteraceae | Leaf | Not available | Leaf juice is administered orally | [95] | |
| Caterpillar poisoning | Crassocephalum crepidioides | Asteraceae | Leaf | Ascorbic acid Tannin Saponin Phytate | Paste of leaf is rubbed on the body | [95,145] |
| Leech bites | Curcuma longa | Zingiberaceae | Rhizome | Curcumin | Paste of rhizome is applied locally | [95] |
| Mushroom poisoning | Rhus javanica | Anarcardiaceae | Fruits | Not available | Fruits are chewed | [95] |
| General chemical poisoning | Hibiscus sabdariffa | Malvaceae | Leaf and calyx | Triterpenoids Steroids | Decoction of leaf and calyx is administered orally | [95,146] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aruwa, C.E.; Mukaila, Y.O.; Ajao, A.A.-n.; Sabiu, S. An Appraisal of Antidotes’ Effectiveness: Evidence of the Use of Phyto-Antidotes and Biotechnological Advancements. Molecules 2020, 25, 1516. https://doi.org/10.3390/molecules25071516
Aruwa CE, Mukaila YO, Ajao AA-n, Sabiu S. An Appraisal of Antidotes’ Effectiveness: Evidence of the Use of Phyto-Antidotes and Biotechnological Advancements. Molecules. 2020; 25(7):1516. https://doi.org/10.3390/molecules25071516
Chicago/Turabian StyleAruwa, Christiana Eleojo, Yusuf Ola Mukaila, Abdulwakeel Ayokun-nun Ajao, and Saheed Sabiu. 2020. "An Appraisal of Antidotes’ Effectiveness: Evidence of the Use of Phyto-Antidotes and Biotechnological Advancements" Molecules 25, no. 7: 1516. https://doi.org/10.3390/molecules25071516