In Vitro and In Vivo Evaluations of β-Lactam/β-Lactamase Mono- and Combined Therapies against Carbapenem-Nonsusceptible Enterobacteriaceae in Taiwan

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bacterial Isolate Collection
2.2. Antimicrobial Susceptibility Testing
2.3. β-. Lactamase and Carbapenemase Gene Detection
2.4. In Vivo Caenorhabditis elegans Study
2.5. Statistical Analyses
3. Results
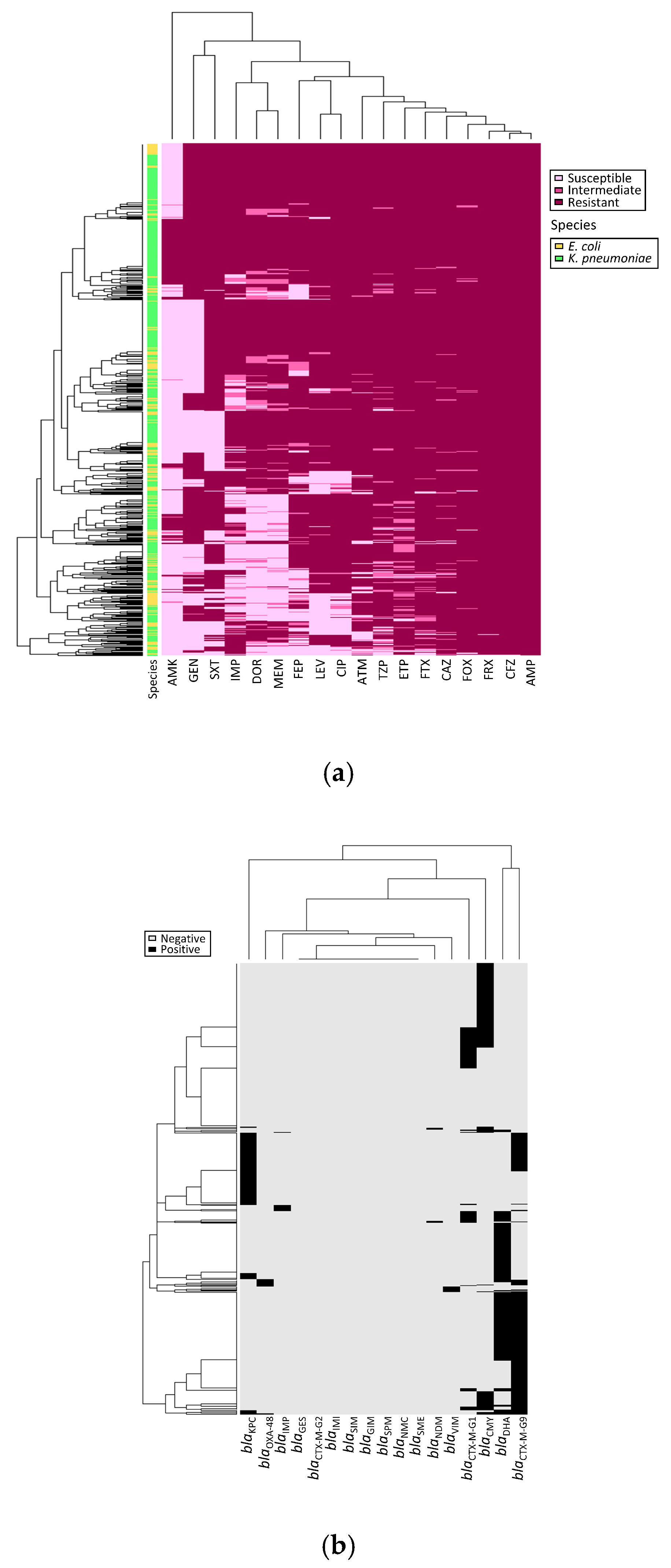
3.1. Enterobacteriaceae Isolates
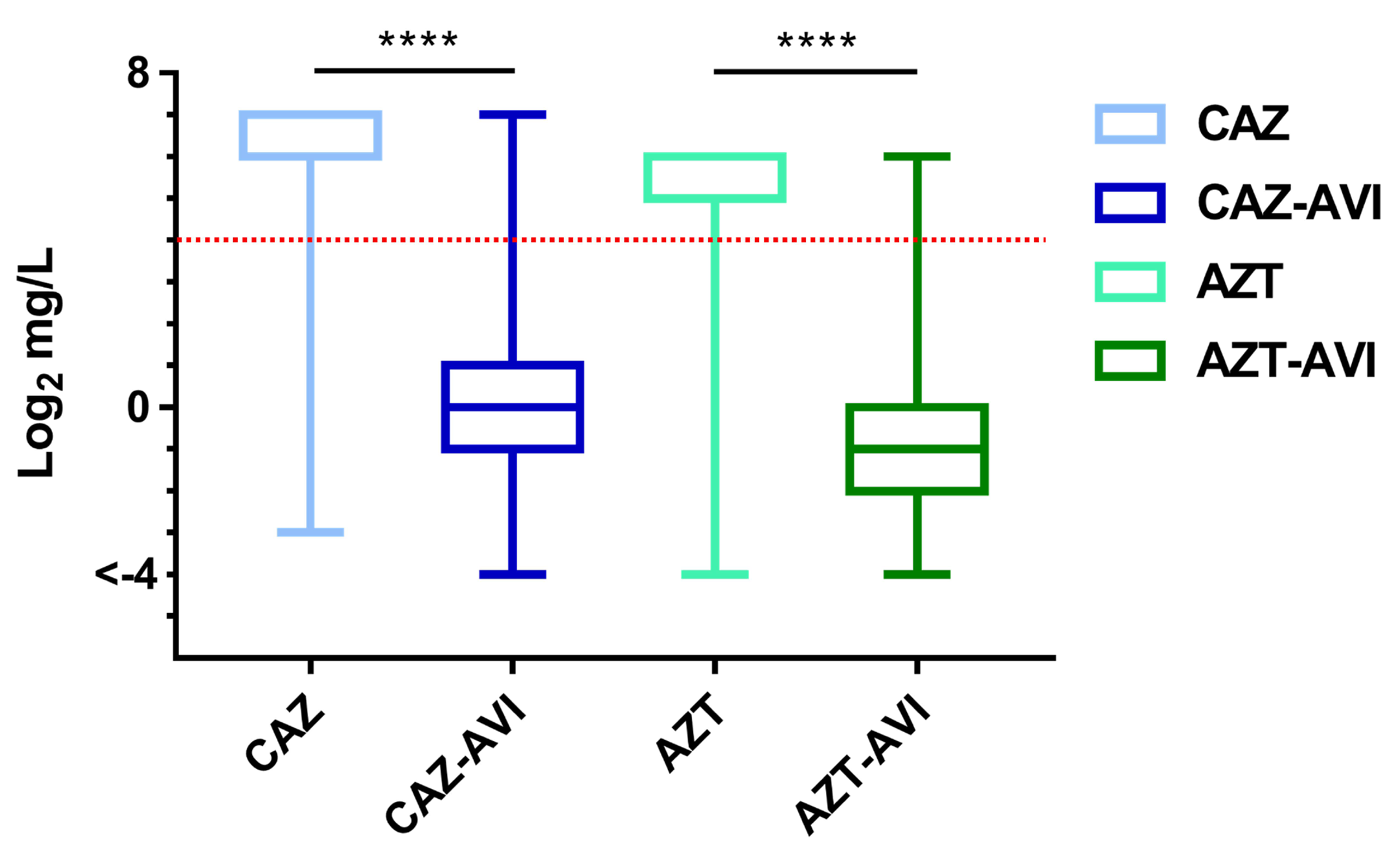
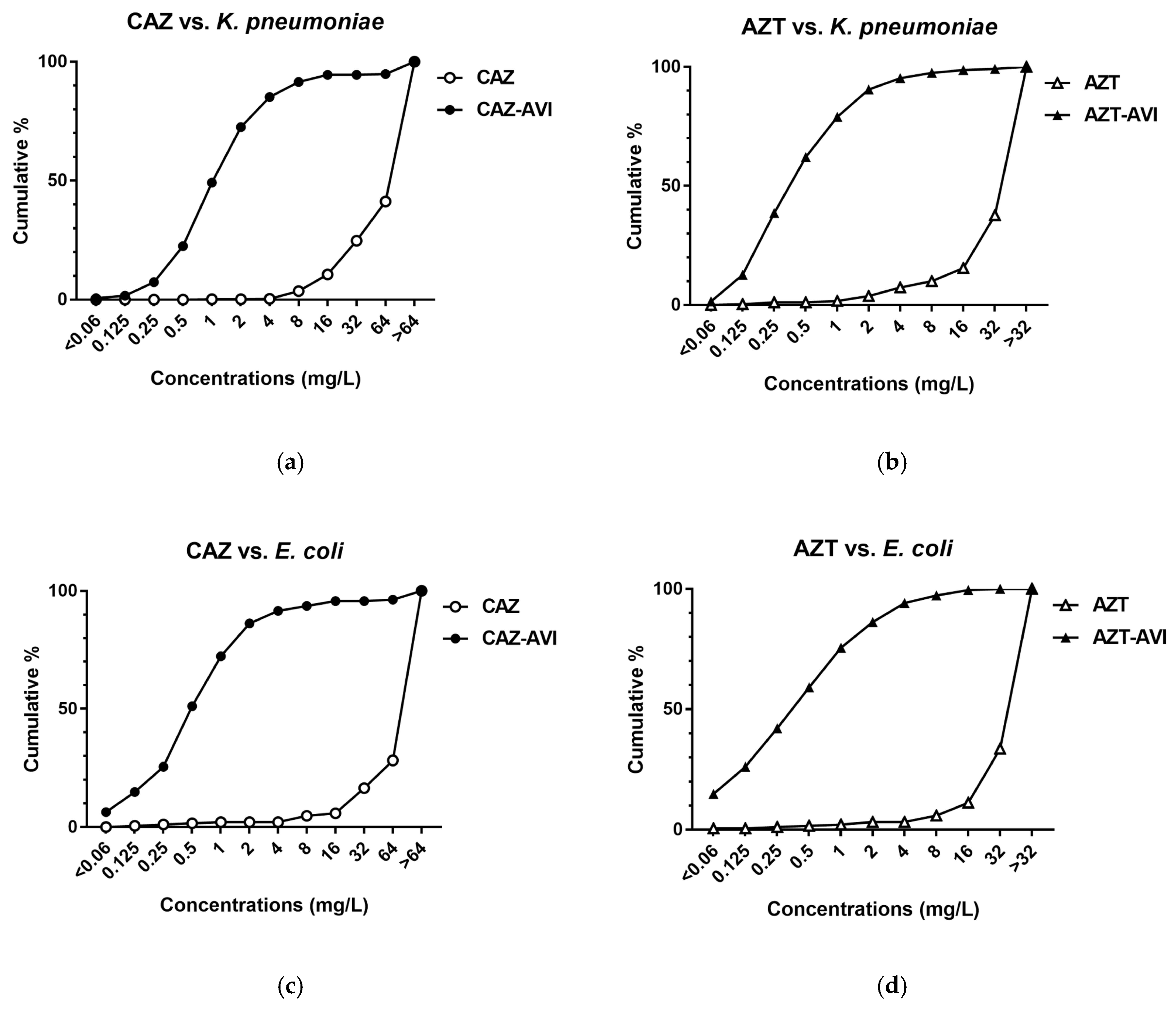
3.2. In Vitro β-lactam with β-lactamase Inhibitor Activity
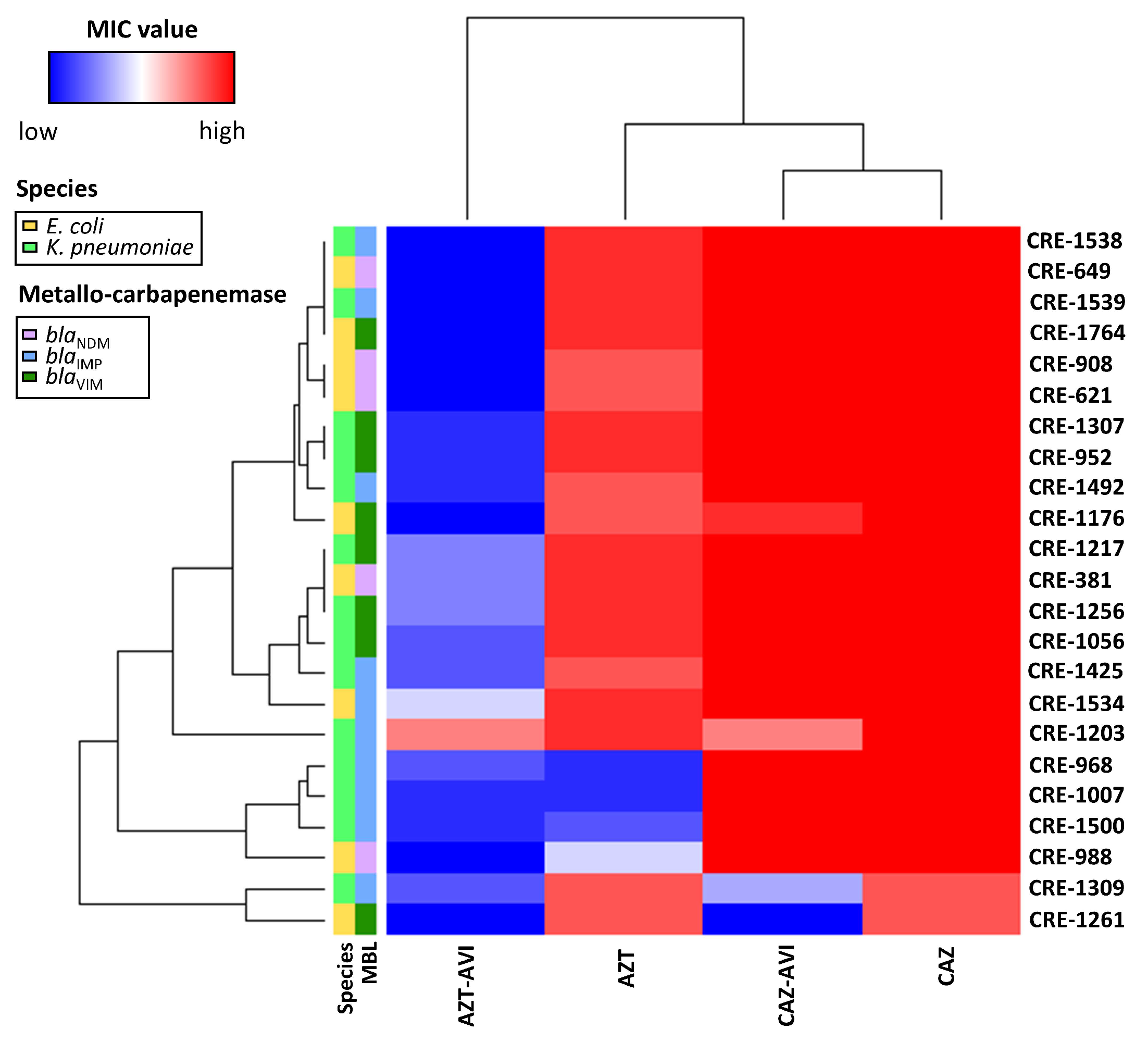
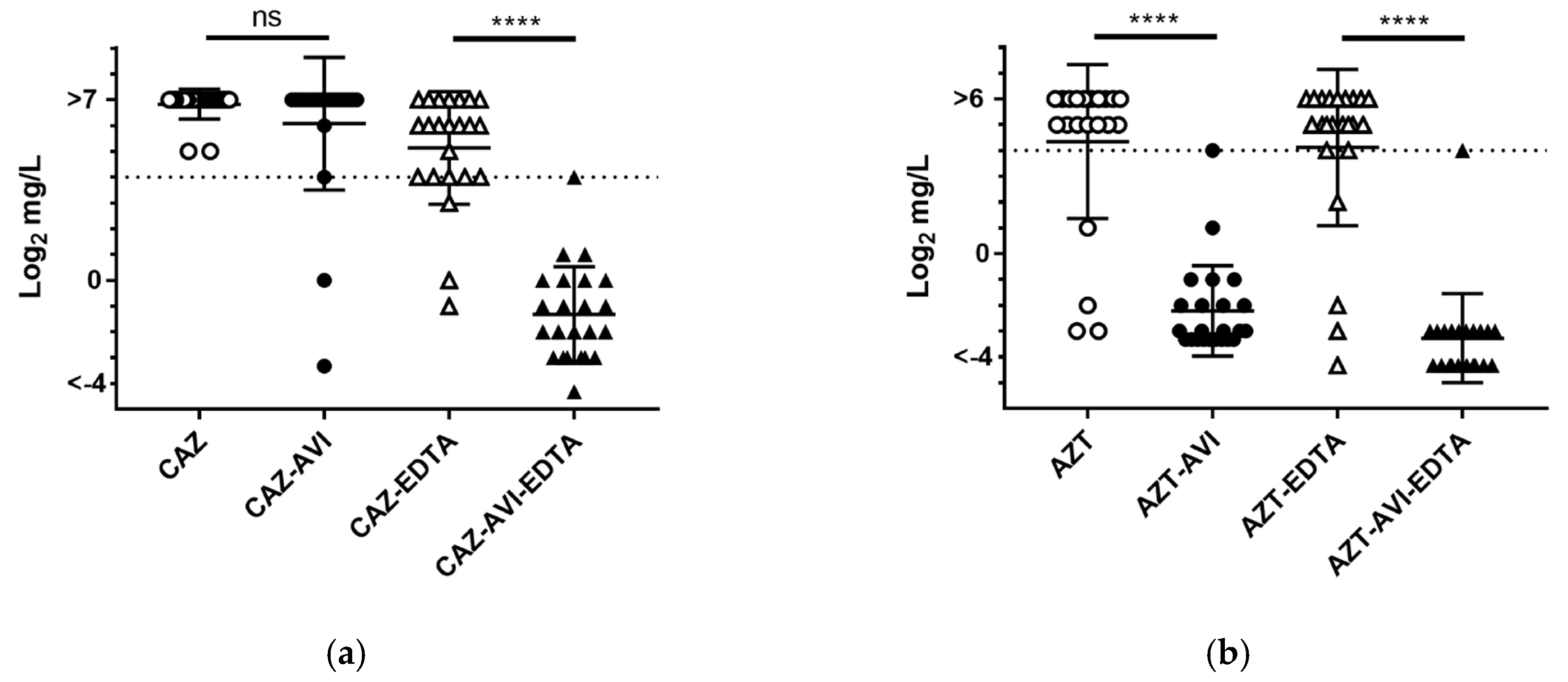
3.3. Combination Therapy Efficacy Against Metallo-Carbapenemase Producers
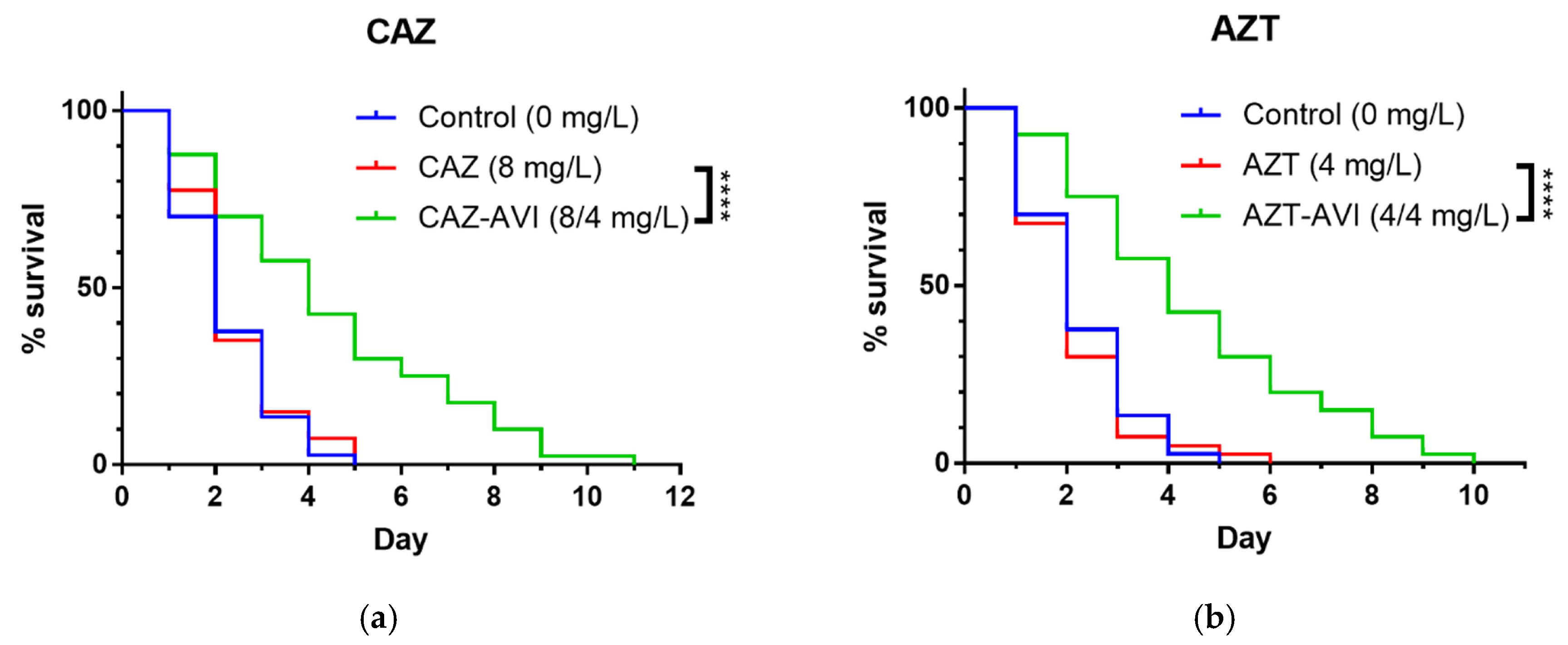
3.4. In Vivo C. Elegans Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bartsch, S.M.; McKinnell, J.A.; Mueller, L.E.; Miller, L.G.; Gohil, S.K.; Huang, S.S.; Lee, B.Y. Potential economic burden of carbapenem-resistant Enterobacteriaceae (CRE) in the United States. Clin. Microbiol. Infect. 2017, 23, 48.e9–48.e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codjoe, F.S.; Donkor, E.S. Carbapenem resistance: A review. Med. Sci. 2017, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordmann, P.; Poirel, L. Epidemiology and diagnostics of carbapenem resistance in Gram-negative bacteria. Clin. Infect. Dis. 2019, 69, S521–S528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jean, S.S.; Lu, M.C.; Shi, Z.Y.; Tseng, S.H.; Wu, T.S.; Lu, P.L.; Shao, P.L.; Ko, W.C.; Wang, F.D.; Hsueh, P.R. In vitro activity of ceftazidime-avibactam, ceftolozane-tazobactam, and other comparable agents against clinically important Gram-negative bacilli: Results from the 2017 surveillance of multicenter antimicrobial resistance in Taiwan (SMART). Infect. Drug Resist. 2018, 11, 1983–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tehrani, K.; Martin, N.I. Beta-lactam/beta-lactamase inhibitor combinations: An update. MedChemComm 2018, 9, 1439–1456. [Google Scholar] [CrossRef]
- Poulakou, G.; Lagou, S.; Karageorgopoulos, D.E.; Dimopoulos, G. New treatments of multidrug-resistant Gram-negative ventilator-associated pneumonia. Ann. Transl. Med. 2018, 6, 423. [Google Scholar] [CrossRef]
- Hackel, M.A.; Tsuji, M.; Yamano, Y.; Echols, R.; Karlowsky, J.A.; Sahm, D.F. In vitro activity of the siderophore cephalosporin, cefiderocol, against a recent collection of clinically relevant Gram-negative bacilli from North America and Europe, including carbapenem-nonsusceptible isolates (sidero-wt-2014 study). Antimicrob. Agents Chemother. 2017, 61, e00093-17. [Google Scholar] [CrossRef] [Green Version]
- Kazmierczak, K.M.; Tsuji, M.; Wise, M.G.; Hackel, M.; Yamano, Y.; Echols, R.; Sahm, D.F. In vitro activity of cefiderocol, a siderophore cephalosporin, against a recent collection of clinically relevant carbapenem-non-susceptible Gram-negative bacilli, including serine carbapenemase- and metallo-beta-lactamase-producing isolates (SIDERO-WT-2014 study). Int. Arab. J. Antimicrob. Agents 2019, 53, 177–184. [Google Scholar]
- Chang, Y.T.; Siu, L.K.; Wang, J.T.; Wu, T.L.; Chen, Y.H.; Chuang, Y.C.; Lin, J.C.; Lu, P.L. Resistance mechanisms and molecular epidemiology of carbapenem-nonsusceptible Escherichia coli in Taiwan, 2012–2015. Infect. Drug Resist. 2019, 12, 2113–2123. [Google Scholar] [CrossRef] [Green Version]
- Chiu, S.K.; Ma, L.; Chan, M.C.; Lin, Y.T.; Fung, C.P.; Wu, T.L.; Chuang, Y.C.; Lu, P.L.; Wang, J.T.; Lin, J.C.; et al. Carbapenem nonsusceptible Klebsiella pneumoniae in Taiwan: Dissemination and increasing resistance of carbapenemase producers during 2012–2015. Sci. Rep. 2018, 8, 8468. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Ninth Informational Supplement; Document M100-S29 CLSI; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- Jain, A.; Hopkins, K.L.; Turton, J.; Doumith, M.; Hill, R.; Loy, R.; Meunier, D.; Pike, R.; Livermore, D.M.; Woodford, N. NDM carbapenemases in the United Kingdom: An analysis of the first 250 cases. J. Antimicrob. Chemother. 2014, 69, 1777–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, S.P.; Wang, J.T.; Liang, C.Y.; Lee, P.S.; Chen, Y.C.; Lu, P.L. First report of blaImp-8 in Raoultella planticola. Antimicrob. Agents Chemother. 2014, 58, 593–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.H.; Chu, C.; Liu, J.W.; Chen, Y.S.; Chiu, C.J.; Su, L.H. Collateral damage of flomoxef therapy: In vivo development of porin deficiency and acquisition of blaDHA-1 leading to ertapenem resistance in a clinical isolate of Klebsiella pneumoniae producing CTX-M-3 and SHV-5 beta-lactamases. J. Antimicrob. Chemother. 2007, 60, 410–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.Y.; Wang, S.F.; Lin, J.E.; Griffith, B.T.S.; Lian, S.H.; Hong, Z.D.; Lin, L.; Lu, P.L.; Tseng, S.P. Contributions of insertion sequences conferring colistin resistance in Klebsiella pneumoniae. Int. J. Antimicrob. Agents 2020, 55, 105894. [Google Scholar] [CrossRef]
- Carbapenem-Resistant Enterobacteriaceae, Second Update. Available online: www.ecdc.europa.eu/en/publications-data/carbapenem-resistant-enterobacteriaceae-second-update#no-link (accessed on 11 November 2020).
- Ramsamy, Y.; Mlisana, K.P.; Allam, M.; Amoako, D.G.; Abia, A.L.K.; Ismail, A.; Singh, R.; Kisten, T.; Han, K.S.; Muckart, D.J.J.; et al. Genomic analysis of carbapenemase-producing extensively drug-resistant Klebsiella pneumoniae isolates reveals the horizontal spread of p18-43_01 plasmid encoding blaNDM-1 in South Africa. Microorganisms 2020, 8, 137. [Google Scholar] [CrossRef] [Green Version]
- Pons, M.J.; Mari-Almirall, M.; Ymana, B.; Moya-Salazar, J.; Munoz, L.; Saune, S.; Salazar-Hernandez, R.; Vila, J.; Roca, I. Spread of ST348 Klebsiella pneumoniae producing NDM-1 in a peruvian hospital. Microorganisms 2020, 8, 1392. [Google Scholar] [CrossRef]
- Karlowsky, J.A.; Kazmierczak, K.M.; de Jonge, B.L.M.; Hackel, M.A.; Sahm, D.F.; Bradford, P.A. In vitro activity of aztreonam-avibactam against Enterobacteriaceae and Pseudomonas aeruginosa isolated by clinical laboratories in 40 countries from 2012 to 2015. Antimicrob. Agents Chemother. 2017, 61, e00472-17. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Hu, F.; Xu, X.; Liu, Y.; Wu, W.; Zhu, D.; Wang, H. High prevalence of KPC-2-type carbapenemase coupled with CTX-M-type extended-spectrum beta-lactamases in carbapenem-resistant Klebsiella pneumoniae in a teaching hospital in China. Antimicrob. Agents Chemother. 2011, 55, 2493–2494. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Chen, D.; Xu, G.; Huang, W.; Wang, X. Molecular epidemiology and drug resistant mechanism in carbapenem-resistant Klebsiella pneumoniae isolated from pediatric patients in Shanghai, China. PLoS ONE 2018, 13, e0194000. [Google Scholar] [CrossRef]
- Ball, M.; Boyd, A.; Ensor, G.J.; Evans, M.; Golden, M.; Linke, S.R.; Milne, D.; Murphy, R.; Telford, A.; Kalyan, Y.; et al. Development of a manufacturing route to avibactam, a β-lactamase inhibitor. Org. Process. Res. Dev. 2016, 20, 1799–1805. [Google Scholar] [CrossRef]
- Bassetti, M.; Peghin, M.; Vena, A.; Giacobbe, D.R. Treatment of infections due to MDR Gram-negative bacteria. Front. Med. 2019, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Biedenbach, D.J.; Kazmierczak, K.; Bouchillon, S.K.; Sahm, D.F.; Bradford, P.A. In vitro activity of aztreonam-avibactam against a global collection of Gram-negative pathogens from 2012 and 2013. Antimicrob. Agents Chemother. 2015, 59, 4239–4248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasoo, S.; Cunningham, S.A.; Cole, N.C.; Kohner, P.C.; Menon, S.R.; Krause, K.M.; Harris, K.A.; De, P.P.; Koh, T.H.; Patel, R. In vitro activities of ceftazidime-avibactam, aztreonam-avibactam, and a panel of older and contemporary antimicrobial agents against carbapenemase-producing Gram-negative bacilli. Antimicrob. Agents Chemother. 2015, 59, 7842–7846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blizzard, T.A.; Chen, H.; Kim, S.; Wu, J.; Bodner, R.; Gude, C.; Imbriglio, J.; Young, K.; Park, Y.W.; Ogawa, A.; et al. Discovery of MK-7655, a beta-lactamase inhibitor for combination with Primaxin®. Bioorg. Med. Chem. Lett. 2014, 24, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.G.; Lawson, C.D.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Lagace-Wiens, P.R.; Denisuik, A.; Rubinstein, E.; Gin, A.S.; Hoban, D.J.; et al. Ceftazidime-avibactam: A novel cephalosporin/beta-lactamase inhibitor combination. Drugs 2013, 73, 159–177. [Google Scholar] [CrossRef] [Green Version]
- Livermore, D.M.; Warner, M.; Mushtaq, S. Activity of MK-7655 combined with imipenem against Enterobacteriaceae and Pseudomonas aeruginosa. J. Antimicrob. Chemother. 2013, 68, 2286–2290. [Google Scholar] [CrossRef] [Green Version]
- Wright, H.; Bonomo, R.A.; Paterson, D.L. New agents for the treatment of infections with Gram-negative bacteria: Restoring the miracle or false dawn? Clin. Microbiol. Infect. 2017, 23, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Guo, Y.; Li, J.; Zhang, Y.; Yang, Y.; Dong, D.; Zhu, D.; He, P.; Hu, F. In vitro and in vivo bactericidal activity of ceftazidime-avibactam against carbapenemase-producing Klebsiella pneumoniae. Antimicrob. Resist. Infect. Control 2018, 7, 142. [Google Scholar] [CrossRef]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; De Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Powles, M.A.; Galgoci, A.; Misura, A.; Colwell, L.; Dingley, K.H.; Tang, W.; Wu, J.; Blizzard, T.; Motyl, M.; Young, K. In vivo efficacy of relebactam (MK-7655) in combination with imipenem-cilastatin in murine infection models. Antimicrob. Agents Chemother. 2018, 62, e02577-17. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bacterium | Group | MIC | Antimicrobial Agent and p Value a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CAZ | CAZ-AVI | Mean log2 MIC Change (95% CI) | pb | AZT | AZT-AVI | Mean log2 MIC Change (95% CI) | pb | |||
| Klebsiella pneumoniae | Total (n = 472) | Range | 1 ~ >64 | <0.06 ~ >64 | −5.3 (−5.5, −5.2) | <0.0001 | 0.125 ~ >32 | <0.06 ~ >32 | −6.0 (−6.1, −5.8) | <0.0001 |
| MIC50 | >64 | 2 | >32 | 0.5 | ||||||
| MIC90 | >64 | 8 | >32 | 2 | ||||||
| % susceptible | 0.4% (2/472) | 91.5% (432/472) | 7.4% (35/472) | 95.3% (450/472) | ||||||
| Class A carbapenemase (n = 121) | Range | 8 ~ >64 | 0.25 ~ >64 | −5.2 (−5.4, −5.0) | <0.0001 | 16 ~ >32 | 0.125 ~ 8 | −6.3 (−6.5, −6.2) | <0.0001 | |
| MIC50 | >64 | 2 | >32 | 1 | ||||||
| MIC90 | >64 | 8 | >32 | 2 | ||||||
| % susceptible | 0% (0/121) | 95.0% (115/121) | 0% (0/121) | 99.2% (120/121) | ||||||
| Class B carbapenemase (n = 14) | Range | 32 ~ >64 | 1 ~ >64 | −0.6 (−1.4, 0.3) | 0.1788 | 0.125 ~ >32 | <0.06 ~ >32 | −6.0 (−8.2, −3.8) | <0.0001 | |
| MIC50 | >64 | >64 | >32 | 0.125 | ||||||
| MIC90 | >64 | >64 | >32 | 0.5 | ||||||
| % susceptible | 0% (0/14) | 7.1% (1/14) | 21.4% (3/14) | 92.9% (13/14) | ||||||
| Class D carbapenemase (n = 10) | Range | 8 ~ 64 | 0.25 ~ 2 | −4.8 (−5.7, −3.9) | <0.0001 | 1 ~ >32 | 0.125 ~ 2 | −6.0 (−7.2, −4.8) | <0.0001 | |
| MIC50 | 16 | 1 | 32 | 0.25 | ||||||
| MIC90 | 64 | 2 | >32 | 2 | ||||||
| % susceptible | 0% (0/10) | 100% (10/10) | 10% (1/10) | 100% (10/10) | ||||||
| Non-carbapenemase producer (n = 329) | Range | 1 ~ >64 | <0.06 ~ >64 | −5.6 (−5.8, −5.4) | <0.0001 | 0.25 ~ >32 | <0.06 ~ >32 | −5.8 (−6.0, −5.6) | <0.0001 | |
| MIC50 | >64 | 1 | >32 | 0.5 | ||||||
| MIC90 | >64 | 8 | >32 | 4 | ||||||
| % susceptible | 0.6% (2/329) | 93.6% (308/329) | 9.4% (31/329) | 93.9% (309/329) | ||||||
| Escherichia coli | Total (n = 188) | Range | 0.125 ~ >64 | <0.06 ~ >64 | −6.6 (−7.0, −6.3) | <0.0001 | <0.06 ~ >32 | <0.06 ~ 32 | −6.3 (−6.6, −6.0) | <0.0001 |
| MIC50 | >64 | 0.5 | >32 | 0.5 | ||||||
| MIC90 | >64 | 4 | >32 | 4 | ||||||
| % susceptible | 2.1% (4/188) | 93.6% (176/188) | 3.2% (6/188) | 94.1% (177/188) | ||||||
| Class A carbapenemase (n = 3) | Range | 8 ~ 32 | 0.125 ~ 2 | −5.3 (−8.2, −2.5) | 0.0153 | 32 ~ >32 | <0.06 ~ 0.125 | −9.0 (−9.2, −8.9) | <0.0001 | |
| MIC50 | 8 | 0.125 | 32 | <0.06 | ||||||
| MIC90 | 32 | 2 | >32 | 0.125 | ||||||
| % susceptible | 0% (0/3) | 100% (3/3) | 0% (0/3) | 100% (3/3) | ||||||
| Class B carbapenemase (n = 9) | Range | 32 ~ >64 | <0.06 ~ >64 | −1.1 (−3.4, 1.2) | 0.2953 | 2 ~ >32 | <0.06 ~ 2 | −8.1 (−9.6, −6.6) | <0.0001 | |
| MIC50 | >64 | >64 | 32 | <0.125 | ||||||
| MIC90 | >64 | >64 | >32 | 2 | ||||||
| % susceptible | 0% (0/9) | 11.1% (1/9) | 11.1% (1/9) | 100% (9/9) | ||||||
| Class D carbapenemase (n = 2) | Range | >64 | 0.25 ~ 4 | − | − | >32 | 0.125 ~ 4 | − | − | |
| MIC50 | >64 | 0.25 | >32 | 0.125 | ||||||
| MIC90 | >64 | 4 | >32 | 4 | ||||||
| % susceptible | 0% (0/2) | 100% (2/2) | 0% (0/2) | 100% (2/2) | ||||||
| Non-carbapenemase producer (n = 174) | Range | 0.125 ~ >64 | <0.06 ~ 16 | −6.9 (−7.2, −6.7) | <0.0001 | <0.06 ~ >32 | <0.06 ~ 32 | −6.2 (−6.5, 5.9) | <0.0001 | |
| MIC50 | >64 | 0.5 | >32 | 0.5 | ||||||
| MIC90 | >64 | 2 | >32 | 4 | ||||||
| % susceptible | 2.3% (4/174) | 97.7% (170/174) | 2.9% (5/174) | 93.7% (163/174) | ||||||
| Treatment | Median Survival Time (Days) | p Value | Hazard Ratio | ||
|---|---|---|---|---|---|
| Ratio | Lower 95% | Upper 95% | |||
| untreated control | 2 | − | − | − | − |
| ceftazidime | 2 | − | 1 | − | − |
| ceftazidime–avibactam | 4 | <0.0001 | 0.472 | 0.295 | 0.756 |
| aztreonam | 2 | − | 1 | − | − |
| aztreonam–avibactam | 4 | <0.0001 | 0.420 | 0.260 | 0.679 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.-Y.; Hsieh, Y.-J.; Kao, L.-T.; Liu, G.-H.; Lian, S.-H.; Wang, L.-C.; Lin, I.-L.; Lin, Y.-T.; Wang, S.-F.; Tseng, S.-P.; et al. In Vitro and In Vivo Evaluations of β-Lactam/β-Lactamase Mono- and Combined Therapies against Carbapenem-Nonsusceptible Enterobacteriaceae in Taiwan. Microorganisms 2020, 8, 1981. https://doi.org/10.3390/microorganisms8121981
Yang T-Y, Hsieh Y-J, Kao L-T, Liu G-H, Lian S-H, Wang L-C, Lin I-L, Lin Y-T, Wang S-F, Tseng S-P, et al. In Vitro and In Vivo Evaluations of β-Lactam/β-Lactamase Mono- and Combined Therapies against Carbapenem-Nonsusceptible Enterobacteriaceae in Taiwan. Microorganisms. 2020; 8(12):1981. https://doi.org/10.3390/microorganisms8121981
Chicago/Turabian StyleYang, Tsung-Ying, Ya-Ju Hsieh, Li-Ting Kao, Guan-Hong Liu, Shao-Hsuan Lian, Liang-Chun Wang, I-Ling Lin, Yu-Tzu Lin, Sheng-Fan Wang, Sung-Pin Tseng, and et al. 2020. "In Vitro and In Vivo Evaluations of β-Lactam/β-Lactamase Mono- and Combined Therapies against Carbapenem-Nonsusceptible Enterobacteriaceae in Taiwan" Microorganisms 8, no. 12: 1981. https://doi.org/10.3390/microorganisms8121981