
Clinicopathological and Radiological Features of Cats Presented with Infectious Respiratory Disease Signs: A Focus on Rhodococcus equi and Klebsiella pneumoniae
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Bacterial Culture and Confirmation
2.3. Diagnostic Imaging
2.4. Histopathology
3. Results
3.1. Signalment and History
3.2. Clinical Findings
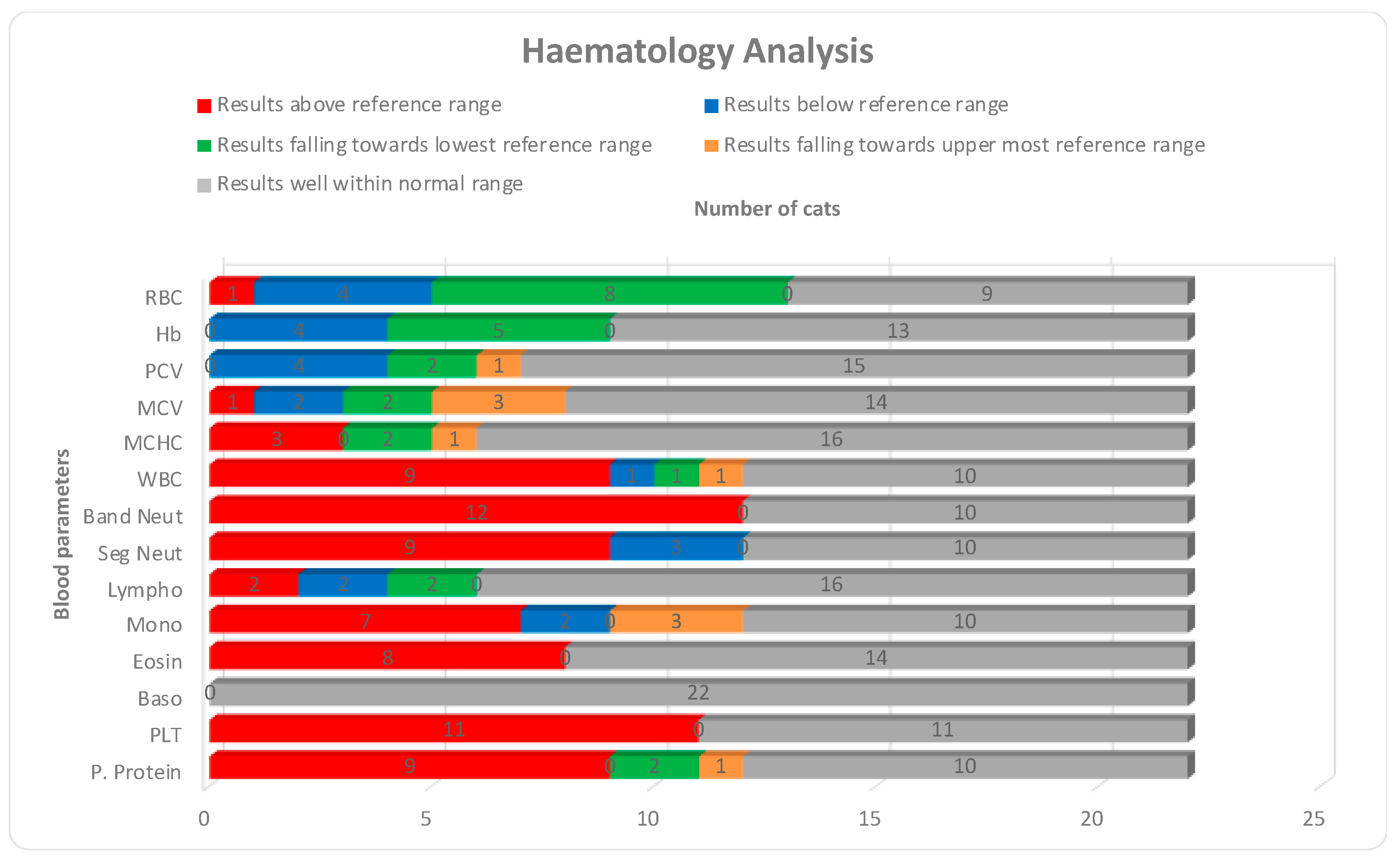
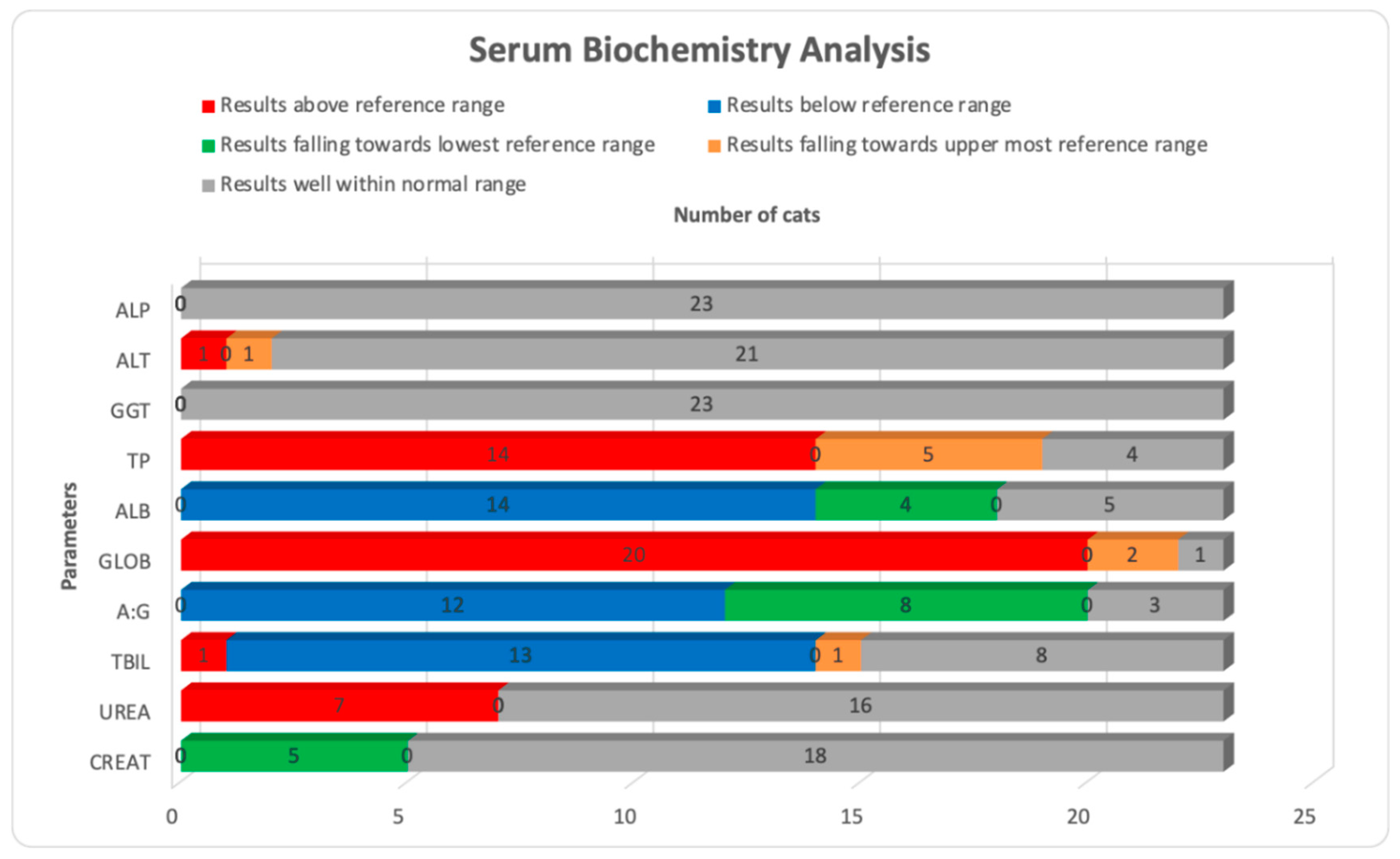
3.3. Hematological and Serum Biochemistry Results
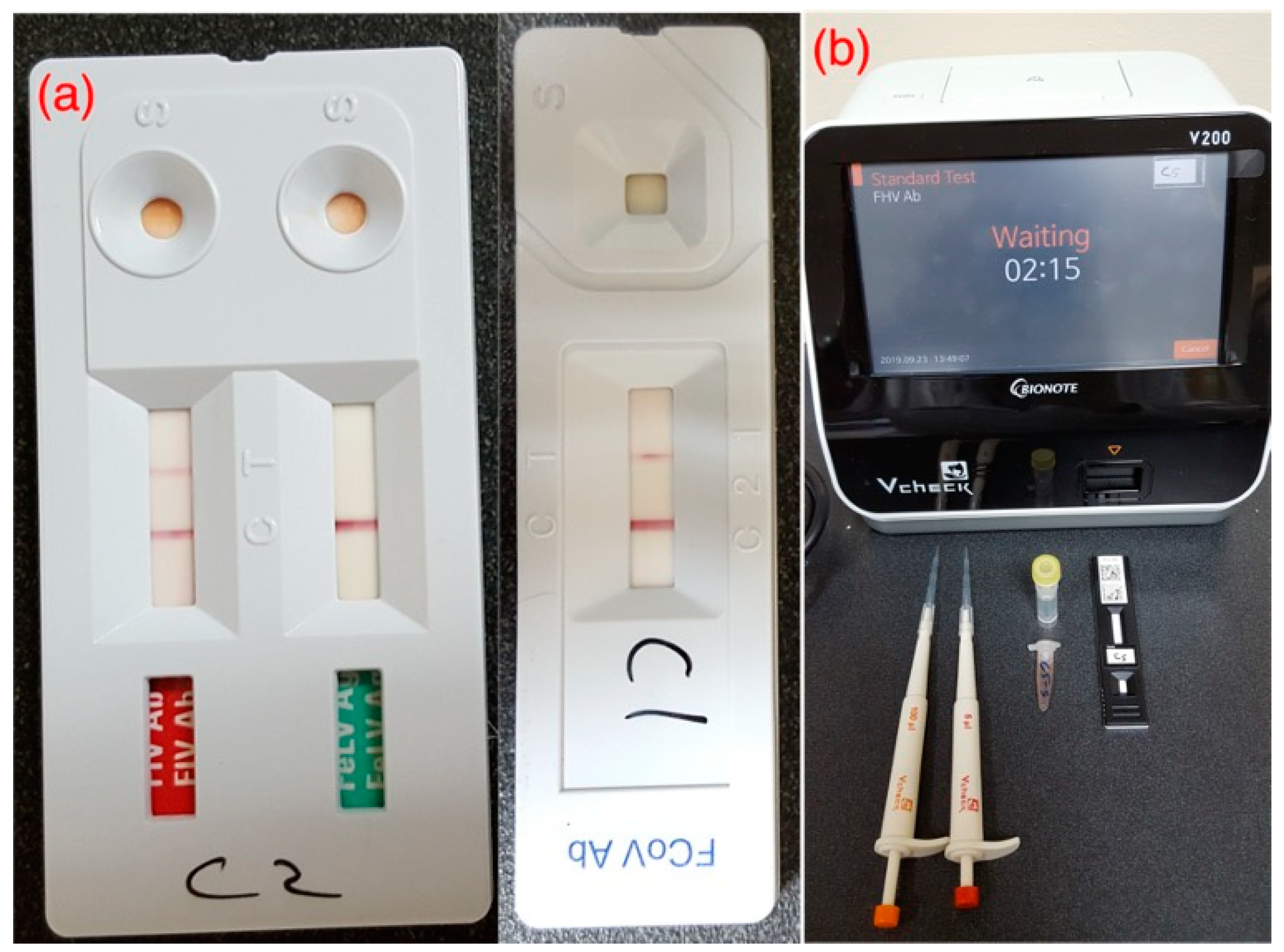
3.4. Lungworm and Viral Screening Results
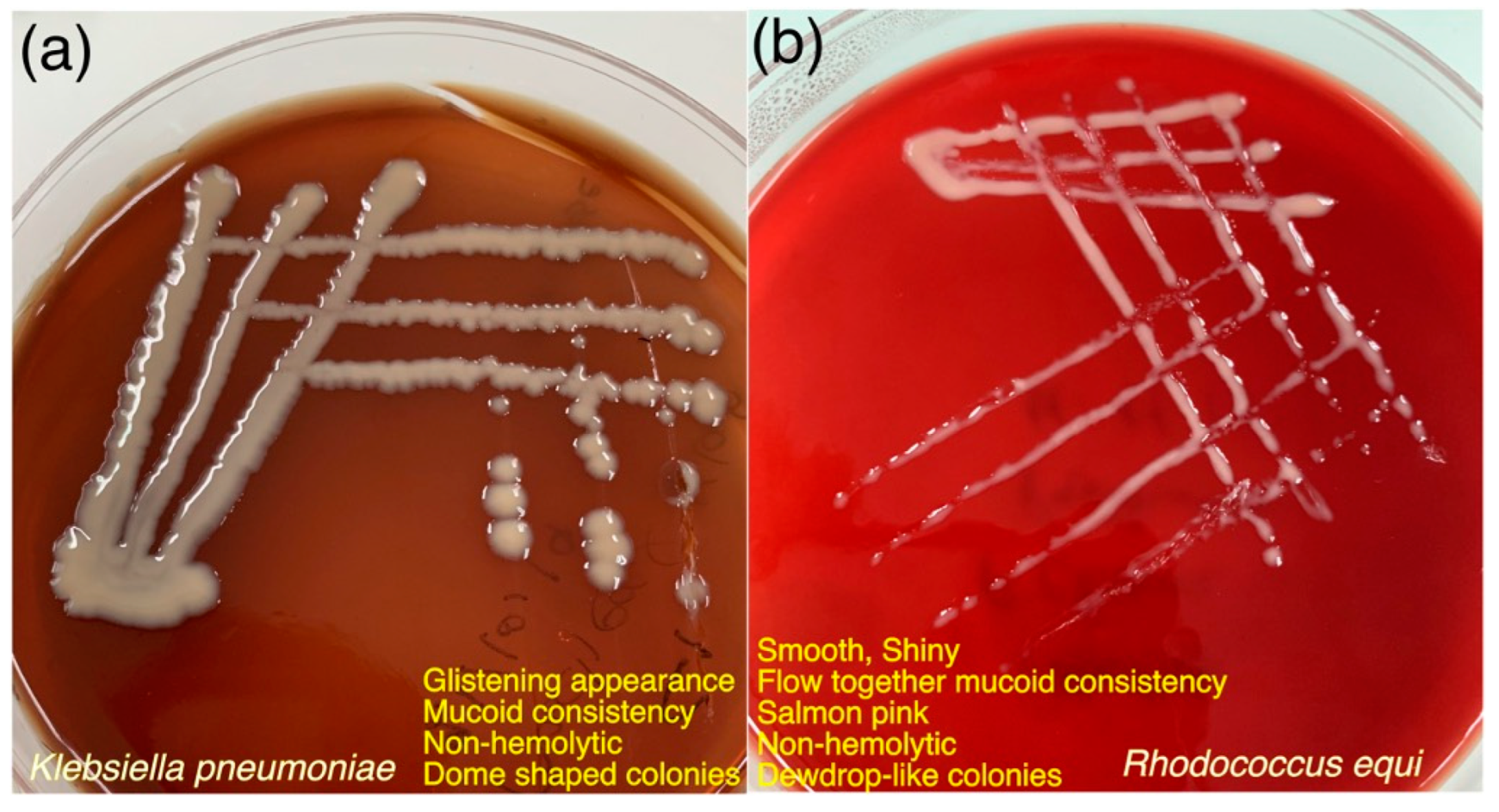
3.5. Bacterial Culture and Confirmation Results
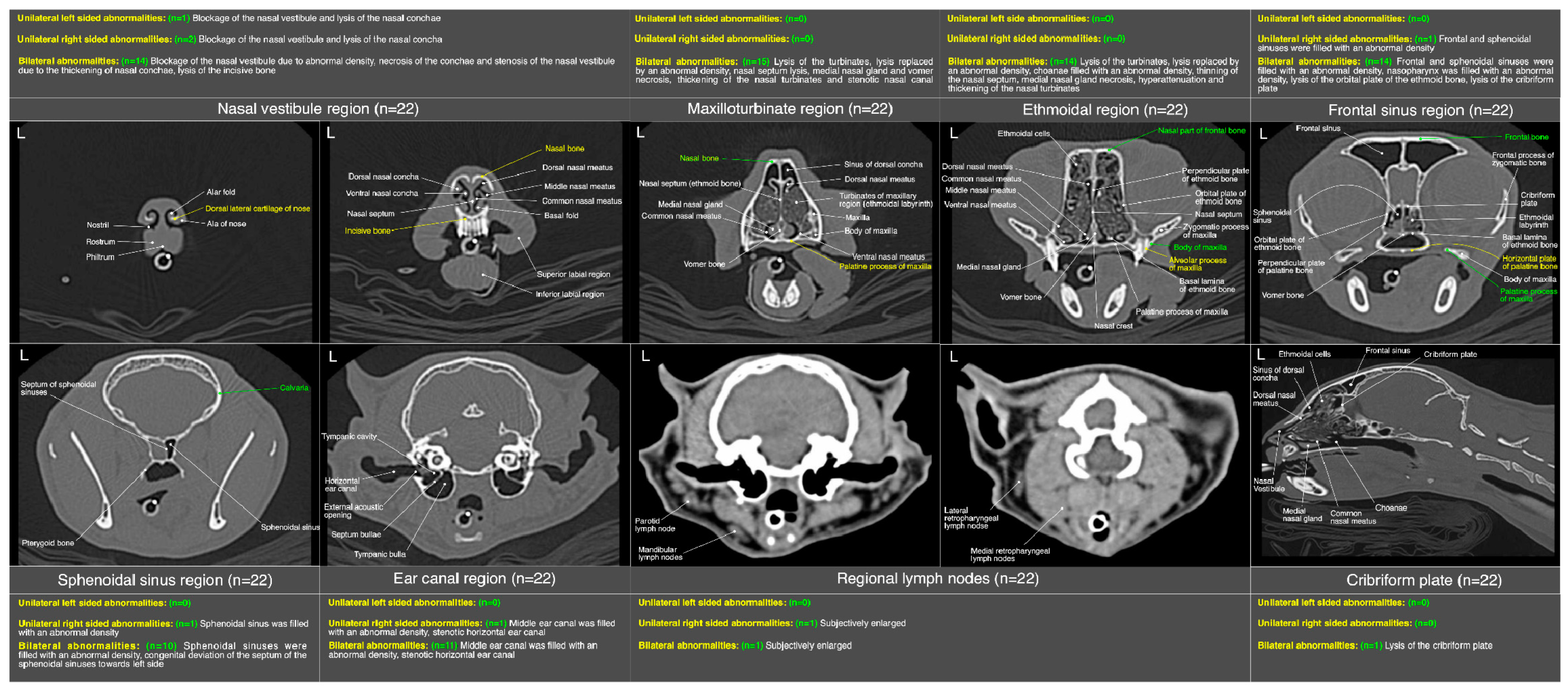
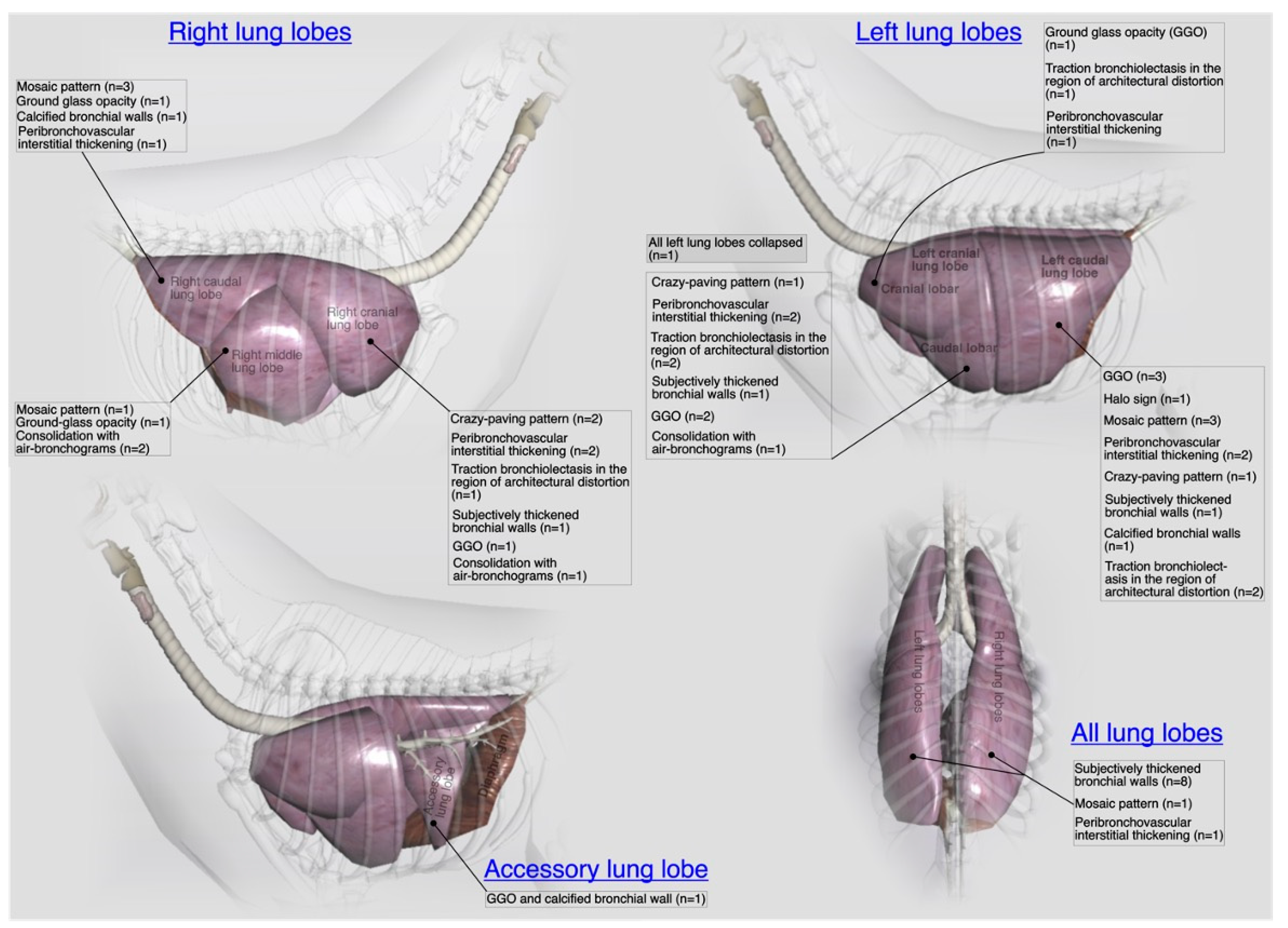
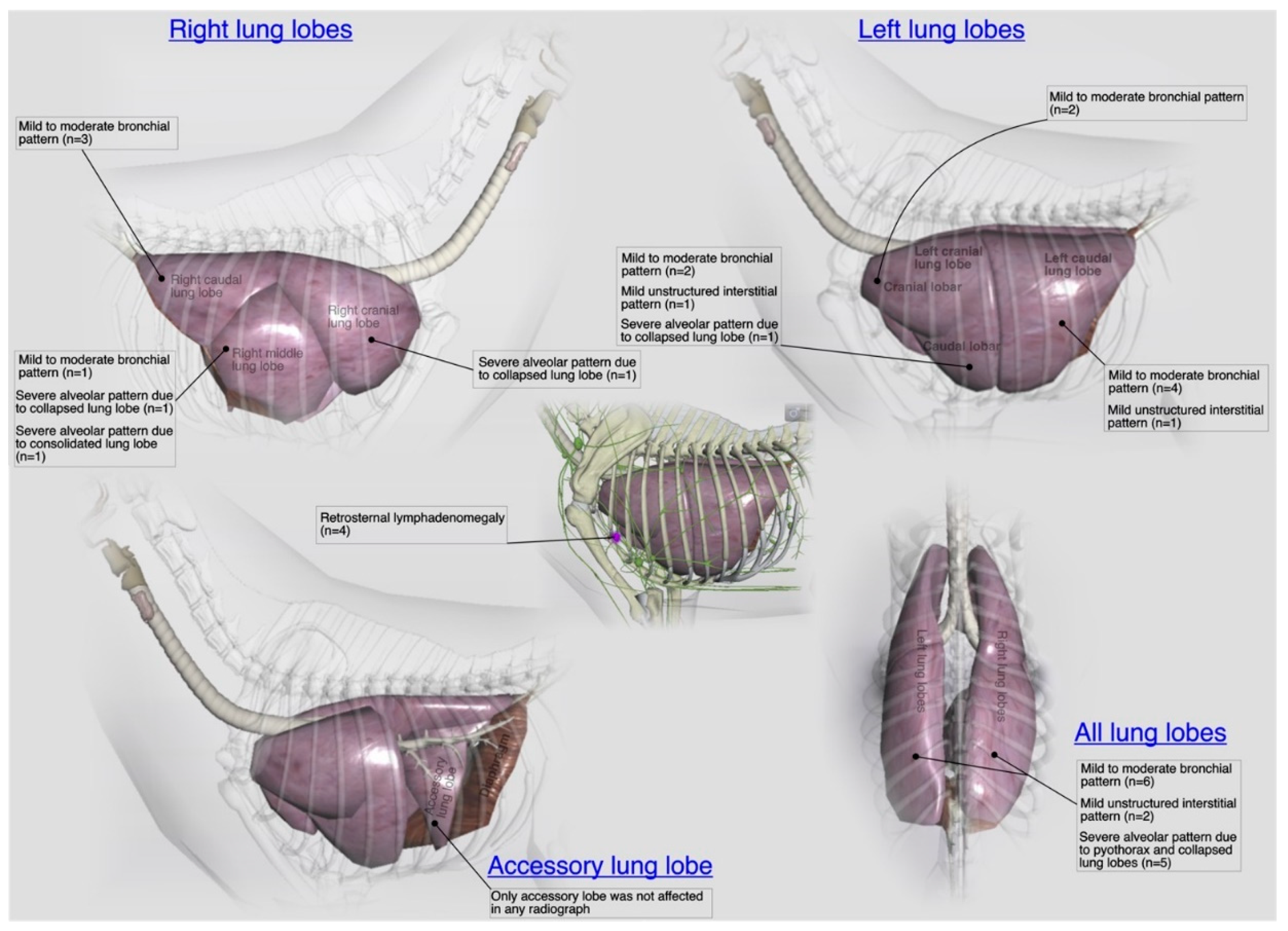
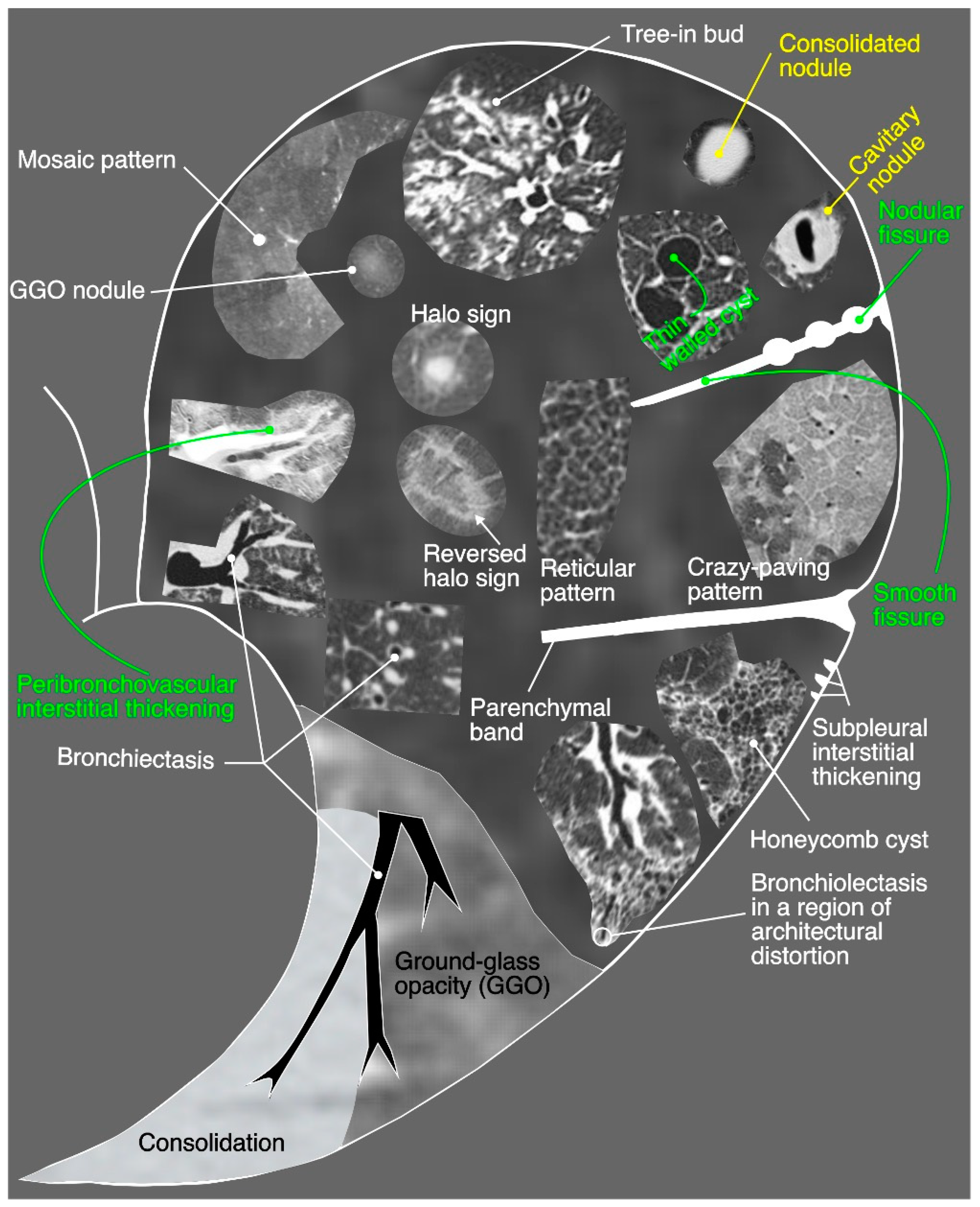
3.6. Radiological Findings
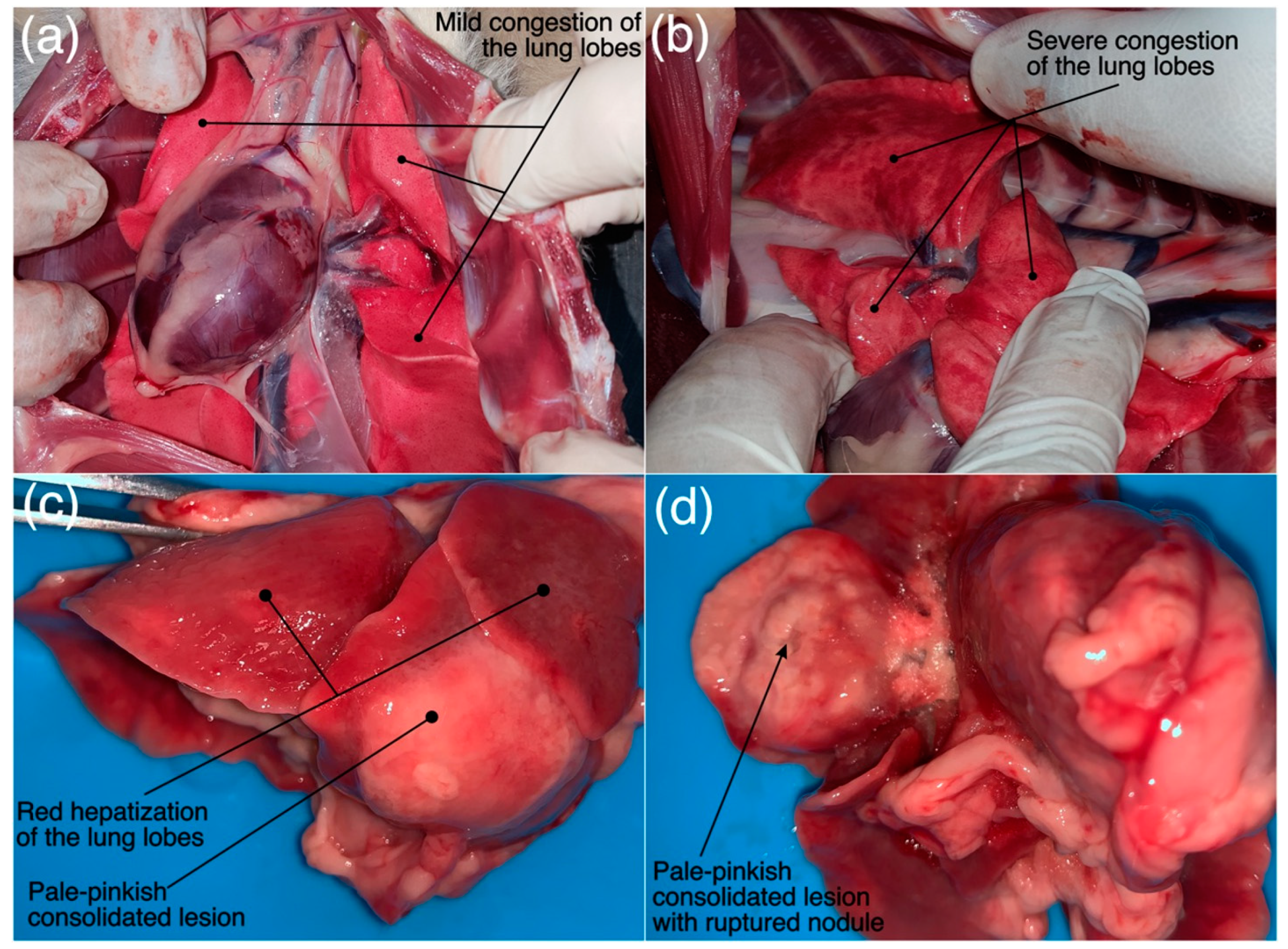
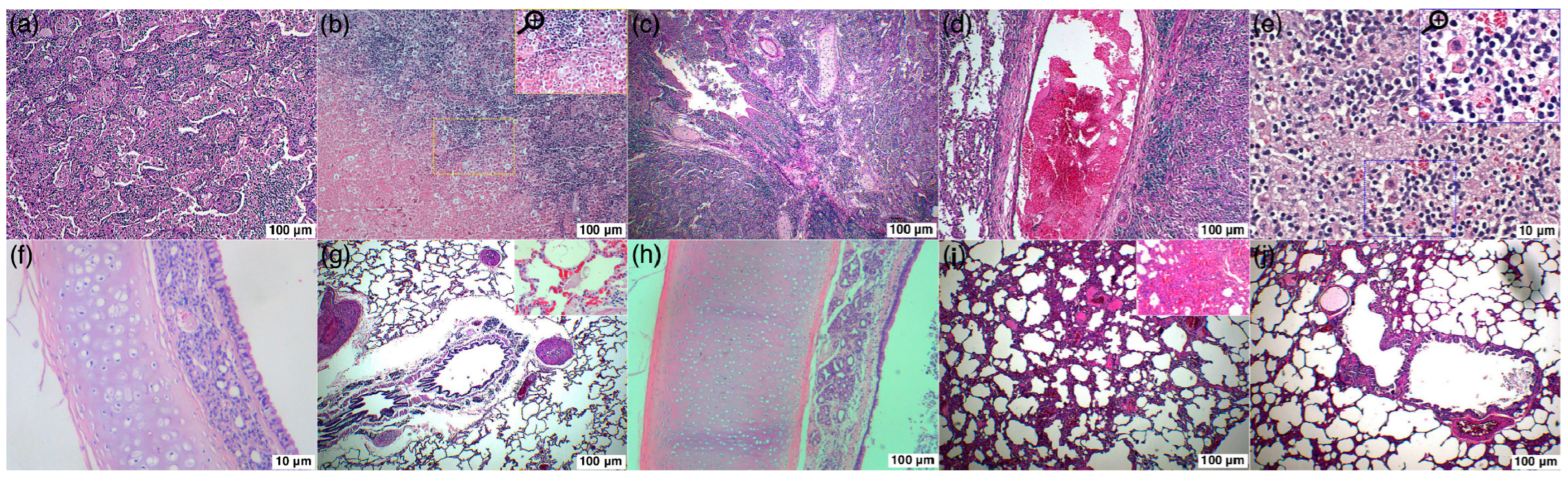
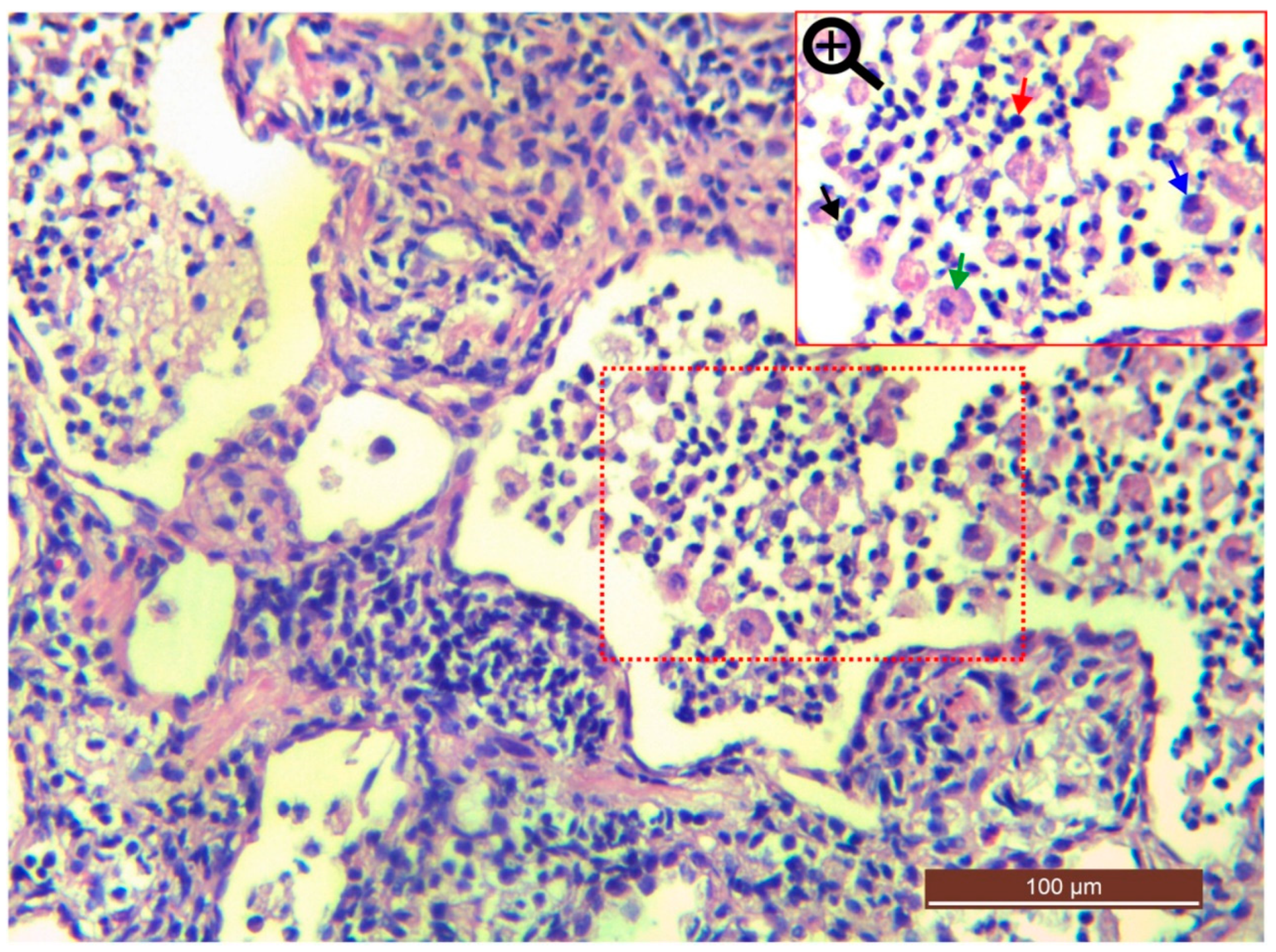
3.7. Pathological Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharp, C.R. Feline rhinitis & upper respiratory disease. Today’s Vet. Pract. 2012, pp. 14–20. Available online: https://todaysveterinarypractice.com/respiratory-medicine/feline-rhinitis-upper-respiratory-disease/ (accessed on 16 February 2020).
- Foster, S.F.; Martin, P. Lower Respiratory Tract Infections in Cats. J. Feline Med. Surg. 2011, 13, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Aslam, M.W.; Lau, S.F.; Chin, C.S.L.; Ahmad, N.I.; Rahman, N.-A.; Kuppusamy, K.; Omar, S.; Radzi, R. Clinicopathological and radiographic features in 40 cats diagnosed with pulmonary and cutaneous Rhodococcus equi infection (2012–2018). J. Feline Med. Surg. 2019, 22, 774–790. [Google Scholar] [CrossRef] [PubMed]
- Low, Y.-M.; Yap, P.S.-X.; Abdul Jabar, K.; Ponnampalavanar, S.; Karunakaran, R.; Velayuthan, R.; Chong, C.-W.; Abu Bakar, S.; Md Yusof, M.Y.; Teh, C.S.-J. The emergence of carbapenem resistant Klebsiella pneumoniae in Malaysia: Correlation between microbiological trends with host characteristics and clinical factors. Antimicrob. Resist. Infect. Control 2017, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Gan, H.M.; Eng, W.W.H.; Dhanoa, A. First genomic insights into carbapenem-resistant Klebsiella pneumoniae from Malaysia. J. Glob. Antimicrob. Resist. 2020, 20, 153–159. [Google Scholar] [CrossRef]
- Aslam, M.W.; Lau, S.F. A review on Rhodococcus equi: Horse, cat and human. J. Vet. Malays. 2019, 31, 1–12. [Google Scholar]
- Foster, S.F.; Martin, P.; Allan, G.S.; Barrs, V.R.; Malik, R. Lower respiratory tract infections in cats: 21 cases (1995–2000). J. Feline Med. Surg. 2004, 6, 167–180. [Google Scholar] [CrossRef]
- Gunew, M. Rhodococcus equi infection in cats. Aust. Vet. Pract. 2002, 32, 2–5. [Google Scholar]
- Passamonti, F.; Lepri, E.; Coppola, G.; Sforna, M.; Proietti, P.C.; Chiodetti, I.; Coletti, M.; Marenzoni, M.L. Pulmonary rhodococcosis in a cat. J. Feline Med. Surg. 2011, 13, 283–285. [Google Scholar] [CrossRef]
- Fairley, R.A.; Fairley, N.M. Fairley Rhodococcus equi infection of cats. Vet. Dermatol. 1999, 10, 43–46. [Google Scholar] [CrossRef]
- Falsone, L.; Brianti, E.; Gaglio, G.; Napoli, E.; Anile, S.; Mallia, E.; Giannelli, A.; Poglayen, G.; Giannetto, S.; Otranto, D. The European wildcats (Felis silvestris silvestris) as reservoir hosts of Troglostrongylus brevior (Strongylida: Crenosomatidae) lungworms. Vet. Parasitol. 2014, 205, 193–198. [Google Scholar] [CrossRef]
- Taubert, A.; Pantchev, N.; Vrhovec, M.G.; Bauer, C.; Hermosilla, C. Lungworm infections (Angiostrongylus vasorum, Crenosoma vulpis, Aelurostrongylus abstrusus) in dogs and cats in Germany and Denmark in 2003–2007. Vet. Parasitol. 2009, 159, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Tayebeh, F.; Amani, J.; Nazarian, S.; Moradyar, M.; Mirhosseini, S.A. Molecular Diagnosis of Clinically Isolated Klebsiella pneumoniae Strains by PCR-ELISA. J. Appl. Biotechnol. Rep. 2016, 3, 501–505. [Google Scholar]
- Ladrón, N.; Fernández, M.; Agüero, J.; González Zörn, B.; Vázquez-Boland, J.A.; Navas, J. Rapid identification of Rhodococcus equi by a PCR assay targeting the choE gene. J. Clin. Microbiol. 2003, 41, 3241–3245. [Google Scholar] [CrossRef] [PubMed]
- Schoenborn, W.C.; Wisner, E.R.; Kass, P.P.; Dale, M. Retrospective assessment of computed tomographic imaging of feline sinonasal disease in 62 cats. Vet. Radiol. Ultrasound 2003, 44, 185–195. [Google Scholar] [CrossRef]
- Masseau, I.; Reinero, C.R. Thoracic computed tomographic interpretation for clinicians to aid in the diagnosis of dogs and cats with respiratory disease. Vet. J. 2019, 253, 105388. [Google Scholar] [CrossRef]
- Vosugh, D.; Nazem, M.N. Radiological evaluation of caudal vena cava in domestic short hair cats with regard to right heart failure diagnosis. Bulg. J. Vet. Med. 2019, 22, 220–226. [Google Scholar] [CrossRef]
- Fernandez, M.; Manzanilla, E.G.; Lloret, A.; León, M.; Thibault, J.-C. Prevalence of feline herpesvirus-1, feline calicivirus, Chlamydophila felis and Mycoplasma felis DNA and associated risk factors in cats in Spain with upper respiratory tract disease, conjunctivitis and/or gingivostomatitis. J. Feline Med. Surg. 2017, 19, 461–469. [Google Scholar] [CrossRef]
- Schulz, B.S.; Wolf, G.; Hartmann, K. Bacteriological and antibiotic sensitivity test results in 271 cats with respiratory tract infections. Vet. Rec. 2006, 158, 269–270. [Google Scholar] [CrossRef]
- Bannasch, M.J.; Foley, J.E. Epidemiologic evaluation of multiple respiratory pathogens in cats in animal shelters. J. Feline Med. Surg. 2005, 7, 109–119. [Google Scholar] [CrossRef]
- Dinnage, J.D.; Scarlett, J.M.; Richards, J.R. Descriptive epidemiology of feline upper respiratory tract disease in an animal shelter. J. Feline Med. Surg. 2009, 11, 816–825. [Google Scholar] [CrossRef]
- Wong, W.T.; Kelman, M.; Ward, M.P. Surveillance of upper respiratory tract disease in owned cats in Australia, 2009–2012. Prev. Vet. Med. 2013, 112, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Zicola, A.; Saegerman, C.; Quatpers, D.; Viandier, J.; Thiry, E. Feline herpesvirus 1 and feline calicivirus infections in a heterogeneous cat population of a rescue shelter. J. Feline Med. Surg. 2009, 11, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Henzel, A.; Brum, M.C.S.; Lautert, C.; Martins, M.; Lovato, L.T.; Weiblen, R. Isolation and identification of feline calicivirus and feline herpesvirus in Southern Brazil. Brazilian J. Microbiol. 2012, 43, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Gourkow, N.; Lawson, J.H.; Hamon, S.C.; Phillips, C.J.C. Descriptive epidemiology of upper respiratory disease and associated risk factors in cats in an animal shelter in coastal western Canada. Can. Vet. J. 2013, 54, 132–138. [Google Scholar] [PubMed]
- Dawson, S.; Willoughby, K. Feline infectious upper respiratory tract disease—an update. Pract. 1999, 21, 232–237. [Google Scholar] [CrossRef]
- Rasmussen, T.T.; Kirkeby, L.P.; Poulsen, K.; Reinholdt, J.; Kilian, M. Resident aerobic microbiota of the adult human nasal cavity. APMIS 2000, 108, 663–675. [Google Scholar] [CrossRef]
- Henderson, S.M.; Bradley, K.; Day, M.J.; Tasker, S.; Caney, S.M.A.; Moore, A.H.; Gruffydd-Jones, T.J. Investigation of nasal disease in the cat—A retrospective study of 77 cases. J. Feline Med. Surg. 2004, 6, 245–257. [Google Scholar] [CrossRef]
- Cohn, L.A. Feline Respiratory Disease Complex. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 1273–1289. [Google Scholar] [CrossRef]
- Barrs, V.R.; Allan, G.S.; Martin, P.; Beatty, J.A.; Malik, R. Feline pyothorax: A retrospective study of 27 cases in Australia. J. Feline Med. Surg. 2005, 7, 211–222. [Google Scholar] [CrossRef]
- Allison, R.W.; Meinkoth, J.H.; Rizzi, T.E. Abnormalities of the Standard Biochemical Profile. In Small Animal Medical Diagnosis; Lorenz, M.D., Neer, T.M., DeMars, P.L., Eds.; Wiley-Blackwell: New York, NY, USA, 2009; ISBN 9780813813387. [Google Scholar]
- Piek, C.J. The interpretation of automated haematology analyser data in practice. Eur. J. Companion Anim. Pract. 2010, 20, 177–185. [Google Scholar]
- Macdonald, E.S.; Norris, C.R.; Berghaus, R.B.; Griffey, S.M. Clinicopathologic and radiographic features and etiologic agents in cats with histologically confirmed infectious pneumonia: 39 cases (1991–2000). J. Am. Vet. Med. Assoc. 2003, 223, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Bart, M.; Guscetti, F.; Zurbriggen, A.; Pospischil, A.; Schiller, I. Feline Infectious Pneumonia: A Short Literature Review and a Retrospective Immunohistological Study on the Involvement of Chlamydia spp. and Distemper Virus. Vet. J. 2000, 159, 220–230. [Google Scholar] [CrossRef] [PubMed]
- McGrotty, Y.; Knottenbelt, C. Significance of plasma protein abnormalities in dogs and cats. Practice 2002, 24, 512–517. [Google Scholar] [CrossRef]
- DuFort, R.M. Abnormal Laboratory Findings. In Textbook of Veterinary Internal Medicine; Ettinger, S.J., Feldman, E.C., Eds.; Saunders Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Reference values for haematology and haemostasis. In BSAVA Manual of Canine and Feline Haematology and Transfusion Medicine; Day, M.J.; Kohn, B. (Eds.) British Small Animal Veterinary Association: Gloucestershire, UK, 2018; p. 324. [Google Scholar]
- Nur Anis, A.; Zulkifli, S.; Syamimmi, N.; Shuhada, N.; Norazura, A.H.; Azian, N.; Samad, A.A. Verminous pneumonia in an Asian palm civet. In Proceedings of the 14th Proceedings of the Seminar on Veterinary Sciences, Selangor, Malaysia, 19–20 October 2019; Jurnal Veterinary Malaysia: Bangi, Selangor, Malaysia, 2019; p. 105. [Google Scholar]
- Syammimi, A.H.N.; Nurshuhada, A.; Anis, A.N.; Norazura, S.; Zulkifli, Z.S.; Syamsyul, A. Metastrongylus spp. infection in wild boar (Sus scrofa) in Malaysia. In Proceedings of the 14th Seminar on Veterinary Sciences, Serdang, Malaysia, 19–20 October 2019; Jurnal Veterinary Malaysia: Bangi, Malaysia, 2019; p. 88. [Google Scholar]
- Mohamaddiah, N.A.; Khor, K.H.; Arshad, S.S.; Kamal, F.M. Serological prevalence and haematological profile of feline immunodeficiency virus (FIV) in semi-roamer and outdoor cats. J. Vet. Malays. 2014, 26, 20–26. [Google Scholar]
- Ling, C.H.; Watanabe, M.; Zeenathul, N.A.; Rani, P.A.M.A. Detection of Feline Herpesvirus and Feline Calicivirus in Cats with Feline Upper Respiratory Tract Disease presented to University Veterinary Hospital, Universiti Putra Malaysia. In Proceedings of the 9th Seminar on Veterinary Sciences, Serdang, Malaysia, 24–28 February 2014; Faculty of Veterinary Medicine, UPM: Selangor, Malaysia, 2014; p. 178. [Google Scholar]
- Sharif, S.; Arshad, S.S.; Hair-Bejo, M.; Omar, A.R.; Zeenathul, N.A.; Hafidz, M.A. Prevalence of feline coronavirus in two cat populations in Malaysia. J. Feline Med. Surg. 2009, 11, 1031–1034. [Google Scholar] [CrossRef]
- Scherk, M. Snots and Snuffles: Rational Approach to Chronic Feline Upper Respiratory Syndromes. J. Feline Med. Surg. 2010, 12, 548–557. [Google Scholar] [CrossRef]
- Quimby, J.; Lappin, M.R. Update on feline upper respiratory diseases: Introduction and diagnostics. Compend. Contin. Educ. Vet. 2009, 31, 554–564. [Google Scholar]
- Lee-Fowler, T. Feline respiratory disease: What is the role of Mycoplasma species? J. Feline Med. Surg. 2014, 16, 563–571. [Google Scholar] [CrossRef]
- Shon, A.S.; Bajwa, R.P.S.; Russo, T.A. Hypervirulent (hypermucoviscous) Klebsiella pneumoniae. Virulence 2013, 4, 107–118. [Google Scholar] [CrossRef]
- Reed, N. Chronic Rhinitis in the Cat. Vet. Clin. N. Am. Small Anim. Pract. 2014, 44, 33–50. [Google Scholar] [CrossRef]
- Dear, J.D. Bacterial pneumonia in dogs and cats. Vet. Clin. N. Am.-Small Anim. Pract. 2014, 44, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Tromblee, T.C.; Jones, J.C.; Etue, A.E.; Dru Forrester, S. Association between clinical characteristics, computed tomography characteristics, and histologic diagnosis for cats with sinonasal disease. Vet. Radiol. Ultrasound 2006, 47, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.M.; Abbott, G.F.; Greene, R.E.; Shepard, J.-A.O.; Vummidi, D.; Digumarthy, S.R. Imaging Pulmonary Infection: Classic Signs and Patterns. Am. J. Roentgenol. 2014, 202, 479–492. [Google Scholar] [CrossRef]
- Garg, M.; Prabhakar, N.; Gulati, A.; Agarwal, R.; Dhooria, S. Spectrum of imaging findings in pulmonary infections. Part 1: Bacterial and viral. Pol. J. Radiol. 2019, 84, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Nambu, A. Imaging of community-acquired pneumonia: Roles of imaging examinations, imaging diagnosis of specific pathogens and discrimination from noninfectious diseases. World J. Radiol. 2014, 6, 779. [Google Scholar] [CrossRef]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
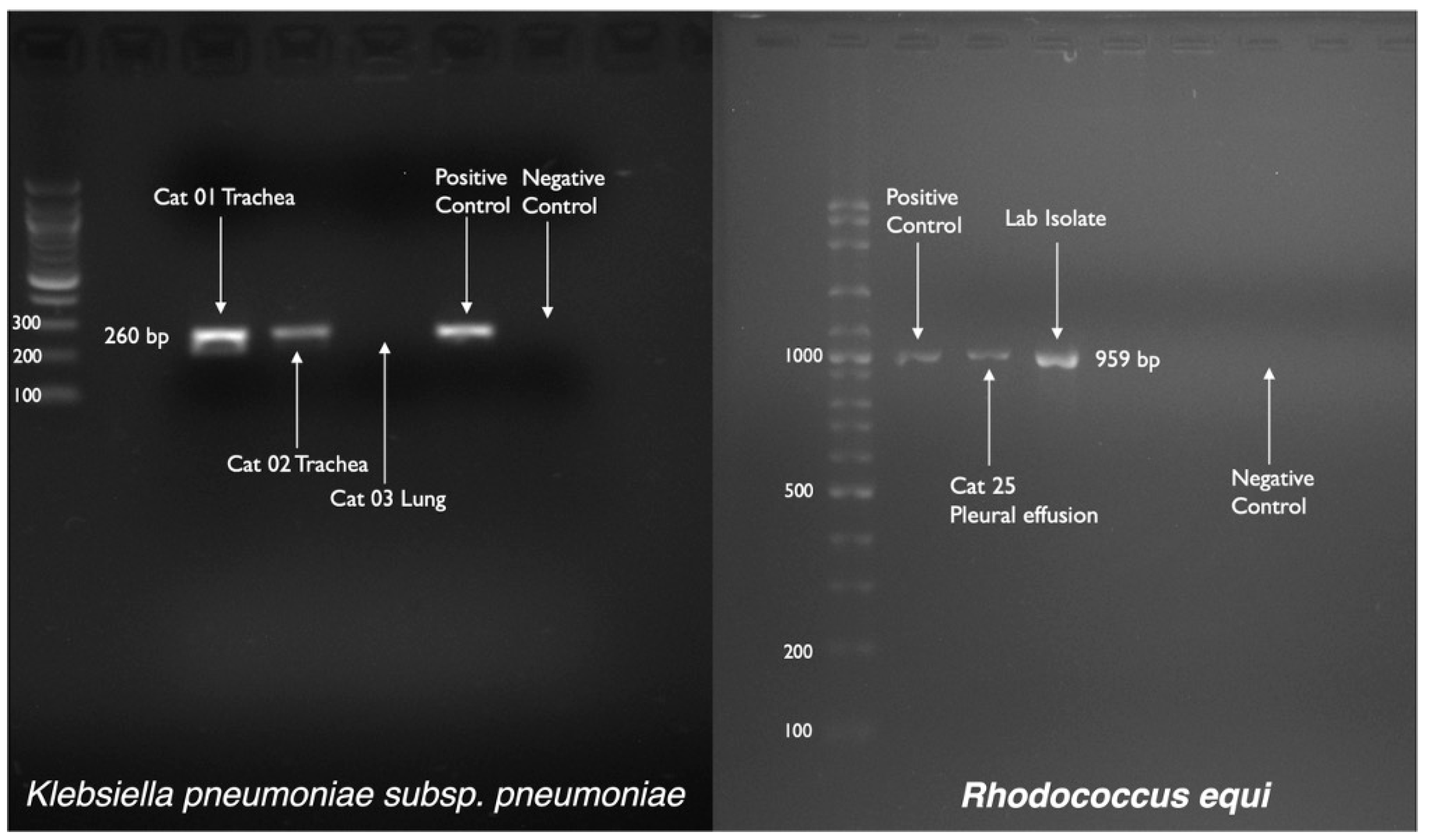
| Oligonucleotide | Sequence | Nucleotide Position | Expected Product Size | Reference |
|---|---|---|---|---|
| Klebsiella pneumoniae (16S rDNA gene) | ||||
| KP16F | GCAAGTCGAGCGGTAGCACAG | 50-70 | 260 bp | [13] |
| KP16R | CAGTGTGGCTGGTCATCCTCTC | 279-309 | ||
| Rhodococcus equi (choE gene) | ||||
| COX-F | GTCAACAACATCGACCAGGCG | 1221-1241 | 959 bp | [14] |
| COX-R | CGAGCCGTCCACGACGTACAG | 2160-2180 | ||
| Cycling Conditions | Reaction Mixture | Analysis |
|---|---|---|
| Klebsiella pneumoniae | ||
| 95 °C for 3 min [95 °C for 45 s, 58 °C for 45 s, 72 °C for 1 min] × 28 72 °C for 5 min | 25 µL | 1.5% gel 100 V for 30 min |
| Rhodococcus equi | ||
| 95 °C for 5 min [95 °C for 1 min, 57 °C for 1 min, 72 °C for 1 min] × 30 72 °C for 10 min | 25 µL | 1.5% gel 80 V for 90 min |
| Parameters for Shelters’ Cats (n = 22) | n (%) |
|---|---|
| Lethargy | 17 (77) |
| Low body condition score (BCS) (≤2.5) | 16 (73) |
| Dehydration (>5%) | 14 (63) |
| Stertorous respiratory sound | 14 (63) |
| Sneezing | 12 (55) |
| Serous nasal discharge | 12 (55) |
| Unilateral or bilateral epiphora | 11 (50) |
| Mucoid or mucopurulent nasal discharge | 10 (45) |
| Oral ulceration | 08 (36) |
| Encrustation of eyelids and/or external nares | 08 (36) |
| Tachypnea | 08 (36) |
| Fever | 07 (32) |
| Conjunctivitis | 06 (27) |
| Orthopnea | 05 (23) |
| Dyspnea | 03 (14) |
| Coughing | 02 (09) |
| Mandibular lymphadenomegaly | 01 (05) |
| Parameters for privately owned pyothorax cats (n =12) | |
| Respiratory distress | 12 (100) |
| Abnormal respiratory sound such as crackles/absent lung sound | 12 (100) |
| Anorexia/Hyporexia | 12 (100) |
| Sample ID | RBC (×1012/L) | Hb (g/L) | PCV (L/L) | MCV (fL) | MCHC (g/L) | WBC (×109/L) | Band N (×109/L) | Neut (×109/L) | Lymp (×109/L) | Mono (×109/L) | Eosin (×109/L) | Baso (×109/L) | PLT (×109/L) | P. Protein (g/L) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref. Range | 05–10 | 80–150 | 0.24–0.45 | 39–55 | 300–360 | 5.5–19.5 | <0.30 | 2.5–12.5 | 1.5–7.0 | 0.20–0.80 | 0.1–1.5 | Rare | 300–700 | 60–80 |
| Cat 01 | 6.73 | 93 | 0.30 | 45 | 310 | 18.37 | 0.55 | 15.61 | 0.37 | 1.84 | 0.00 | 0.00 | 123 | 98 |
| Cat 02 | 11.12 | 133 | 0.44 | 40 | 302 | 9.12 | 0.27 | 7.02 | 1.09 | 0.73 | 0.00 | 0.00 | 264 | 112 |
| Cat 03 | 4.80 | 82 | 0.26 | 54 | 661 | 8.33 | 0.08 | 3.00 | 4.25 | 0.42 | 0.58 | 0.00 | 335 | 70 |
| Cat 04 | 6.72 | 111 | 0.34 | 51 | 456 | 10.48 | 0.10 | 7.44 | 2.31 | 0.52 | 0.10 | 0.00 | 217 | 86 |
| Cat 05 | 4.94 | 73 | 0.23 | 47 | 317 | 16.96 | 0.34 | 10.68 | 4.41 | 0.51 | 1.02 | 0.00 | 248 | 92 |
| Cat 06 | 7.06 | 104 | 0.32 | 45 | 325 | 21.06 | 0.42 | 15.37 | 2.53 | 0.63 | 2.11 | 0.00 | 408 | 72 |
| Cat 07 | 5.15 | 96 | 0.30 | 58 | 320 | 15.61 | 0.16 | 10.77 | 3.43 | 0.47 | 0.78 | 0.00 | 334 | 94 |
| Cat 08 | 5.98 | 94 | 0.31 | 52 | 303 | 21.48 | 0.43 | 14.61 | 3.01 | 0.86 | 2.58 | 0.00 | 401 | 78 |
| Cat 09 | 6.29 | 103 | 0.31 | 49 | 332 | 20.14 | 0.40 | 13.49 | 4.03 | 0.60 | 1.61 | 0.00 | 388 | 64 |
| Cat 10 | 5.31 | 87 | 0.28 | 53 | 311 | 29.32 | 0.88 | 18.18 | 4.69 | 1.47 | 4.10 | 0.00 | 269 | 74 |
| Cat 11 | 5.86 | 104 | 0.31 | 53 | 335 | 23.22 | 0.46 | 16.95 | 1.86 | 1.16 | 2.79 | 0.00 | 225 | 70 |
| Cat 12 | 5.82 | 91 | 0.28 | 48 | 325 | 22.50 | 0.45 | 14.40 | 4.50 | 1.35 | 1.80 | 0.00 | 84 | 70 |
| Cat 13 | 5.63 | 85 | 0.27 | 48 | 315 | 0.52 | TFC | TFC | TFC | TFC | TFC | TFC | 160 | 68 |
| Cat 14 | 5.92 | 86 | 0.27 | 46 | 319 | 5.95 | 0.06 | 2.14 | 3.33 | 0.18 | 0.24 | 0.00 | 320 | 62 |
| Cat 15 | 4.09 | 67 | 0.21 | 51 | 319 | 26.06 | 0.52 | 12.51 | 3.13 | 0.52 | 9.38 | 0.00 | 245 | 72 |
| Cat 19 | 5.46 | 87 | 0.26 | 48 | 335 | 12.78 | 0.13 | 7.03 | 3.83 | 0.26 | 1.53 | 0.00 | 506 | 68 |
| Cat 20 | 7.76 | 111 | 0.33 | 43 | 336 | 14.02 | 0.14 | 10.66 | 1.68 | 1.12 | 0.42 | 0.00 | 190 | 100 |
| Cat 21 | 8.45 | 116 | 0.35 | 41 | 331 | 12.32 | 0.12 | 7.39 | 3.94 | 0.74 | 0.12 | 0.00 | 203 | 86 |
| Cat 22 | 7.58 | 123 | 0.38 | 50 | 324 | 21.66 | 0.43 | 15.60 | 3.90 | 1.52 | 0.22 | 0.00 | 390 | 82 |
| Cat 24 | 4.64 | 63 | 0.17 | 36.2 | 375 | 9.39 | susp | 0.85 | 7.69 | 0.71 | 0.08 | -- | 332 | -- |
| Cat 25 | 6.61 | 78 | 0.23 | 34.9 | 338 | 22.21 | susp | 6.22 | 14.68 | 0.60 | 0.63 | 0.08 | 472 | -- |
| Cat 26 | 7.16 | 100 | 0.28 | 39 | 357 | 10.70 | 0.11 | 7.38 | 2.35 | 0.32 | 0.54 | -- | 391 | 110 |
| Sample ID | ALP (U/L) | ALT (U/L) | GGT (U/L) | TP (Serum) (g/L) | ALB (g/L) | GLOB (g/L) | A:G (Unit) | TBIL (µmol/L) | Urea (mmol/L) | Creat (µmol/L) | Na+ (mmol/L) | K+ (mmol/L) | Cl− (mmol/L) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref. Range | <80 | 10–90 | <6.0 | 55–75 | 25–40 | 25–45 | 0.5–1.4 | 1.7–17 | 3–10 | 60–193 | 146–156 | 3.9–5.5 | 110–132 |
| Cat 01 | 7 | 26 | <2 | 82.4 | 25.7 | 56.7 | 0.5 | 16.4 | 35.2 | 159 | – | – | – |
| Cat 02 | 6 | 71 | <2 | 101.8 | 31.9 | 69.9 | 0.5 | 47.2 | 31.3 | 118 | – | – | – |
| Cat 03 | 13 | 36 | 4 | 68.6 | 23.6 | 45.0 | 0.5 | 2.3 | 10.2 | 126 | – | – | – |
| Cat 04 | 14 | 64 | <2 | 98.0 | 24.6 | 73.4 | 0.3 | 1.5 | 8.1 | 100 | – | – | – |
| Cat 05 | 20 | 36 | <2 | 78.8 | 29.4 | 49.4 | 0.6 | 1.2 | 11.0 | 104 | – | – | – |
| Cat 06 | 15 | 38 | <2 | 96.2 | 22.4 | 73.8 | 0.3 | 1.1 | 8.0 | 115 | – | – | – |
| Cat 07 | 7 | 48 | <2 | 85.3 | 24.5 | 60.8 | 0.4 | 0.9 | 7.6 | 116 | – | – | – |
| Cat 08 | 19 | 63 | <2 | 72.3 | 31.5 | 40.8 | 0.8 | 1.3 | 8.3 | 101 | – | – | – |
| Cat 09 | 12 | 39 | <2 | 75.4 | 21.4 | 54.0 | 0.4 | 1.6 | 6.8 | 88 | – | – | – |
| Cat 10 | 7 | 26 | <2 | 82.4 | 25.7 | 56.7 | 0.5 | 16.4 | 35.2 | 159 | – | – | – |
| Cat 11 | 14 | 37 | 4 | 75.1 | 22.0 | 53.1 | 0.4 | 1.2 | 6.4 | 115 | – | – | – |
| Cat 12 | 10 | 36 | <2 | 74.5 | 23.3 | 51.2 | 0.5 | 1.3 | 6.6 | 90 | – | – | – |
| Cat 13 | 24 | 27 | <2 | 73.7 | 28.0 | 45.7 | 0.6 | 1.9 | 5.9 | 80 | – | – | – |
| Cat 14 | 15 | 51 | <2 | 69.4 | 24.5 | 44.9 | 0.5 | 1.5 | 9.3 | 107 | – | – | – |
| Cat 15 | 14 | 90 | <2 | 74.6 | 22.6 | 52.0 | 0.4 | 1.3 | 9.3 | 72 | – | – | – |
| Cat 16 | 2 | 107 | <2 | 93.7 | 24.2 | 69.5 | 0.3 | 4.2 | 24.5 | 72 | – | – | – |
| Cat 17 | 19 | 51 | 3 | 73.1 | 25.7 | 47.4 | 0.5 | 1.3 | 7.7 | 87 | – | – | – |
| Cat 18 | 9 | 47 | <2 | 73.6 | 21.5 | 52.1 | 0.4 | 0.8 | 7.6 | 60 | – | – | – |
| Cat 19 | 8 | 54 | 3 | 72.4 | 20.6 | 51.8 | 0.4 | 1.2 | 7.8 | 75 | – | – | – |
| Cat 20 | 14 | 50 | 5 | 104.7 | 24 | 80.7 | 0.3 | 2.2 | 11.8 | 129 | – | – | – |
| Cat 21 | 3 | 41 | <2 | 86.3 | 28.5 | 57.8 | 0.5 | 2.1 | 7.1 | 71 | – | – | – |
| Cat 22 | 4 | 82 | <2 | 83.7 | 25.7 | 58 | 0.4 | 2.3 | 8 | 80 | – | – | – |
| Cat 26 | 12 | 51 | – | 96.8 | 23.1 | 73.7 | 0.3 | – | 6.0 | 60 | 150 | 5.3 | 112 |
| Patient ID | FIV Antibody | FeLV Antigen | FCoV Antibody | FCV Antibody | FHV Antibody |
|---|---|---|---|---|---|
| Cat 01 | Negative | Negative | Positive | High titer (5), VN 1:128 | Negative(0), VN ≤ 1:2 |
| Cat 02 | Positive | Negative | Positive | High titer (6), VN ≥ 256 | Medium titer (3), VN 1:16 |
| Cat 03 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Negative(0), VN ≤ 1:2 |
| Cat 04 | Positive | Negative | Positive | High titer (6), VN ≥ 256 | Low titer (1), VN 1:4 |
| Cat 05 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Medium titer (3), VN 1:16 |
| Cat 06 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Low titer (1), VN 1:4 |
| Cat 07 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Low titer (2), VN 1:8 |
| Cat 08 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Medium titer (3), VN 1:16 |
| Cat 09 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Low titer (1), VN 1:4 |
| Cat 10 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Medium titer (3), VN 1:16 |
| Cat 11 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | High titer (5), VN 1:64 |
| Cat 12 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | High titer (5), VN 1:64 |
| Cat 13 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Negative(0), VN ≤ 1:2 |
| Cat 14 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Medium titer (3), VN 1:16 |
| Cat 15 | Positive | Negative | Positive | High titer (6), VN ≥ 256 | High titer (5), VN 1:64 |
| Cat 16 | Positive | Negative | Positive | High titer (6), VN ≥ 256 | High titer (6), VN ≥ 1:128 |
| Cat 17 | Negative | Negative | Positive | High titer (5), VN 1:128 | Negative(0), VN ≤ 1:2 |
| Cat 18 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Low titer (2), VN 1:8 |
| Cat 19 | Negative | Positive | Positive | High titer (6), VN ≥ 256 | High titer (4), VN 1:32 |
| Cat 20 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Medium titer (3), VN 1:16 |
| Cat 21 | Negative | Negative | Positive | High titer (5), VN 1:128 | High titer (5), VN 1:64 |
| Cat 22 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | Low titer (2), VN 1:8 |
| Cat 23 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | High titer (5), VN 1:64 |
| Cat 24 | Negative | Negative | Positive | High titer (6), VN ≥ 256 | High titer (6), VN ≥ 1:128 |
| Cat 25 | Negative | Negative | Positive | High titer (4), VN 1:64 | Negative(0), VN ≤ 1:2 |
| Cat 26 | Negative | Negative | Positive | Negative(0), VN ≤ 1:4 | Low titer (1), VN 1:4 |
| Cat 27 | Negative | Negative | Positive | High titer (5), VN 1:128 | Negative(0), VN ≤ 1:2 |
| Patient ID | Growth on Blood Agar | Growth on MacConkey Agar | Biochemical Confirmation for K. pneumoniae and R. equi | PCR Confirmation for K. pneumoniae and R. equi | ||||
|---|---|---|---|---|---|---|---|---|
| URT Swab | LRT Swab | URT Swab | LRT Swab | URT Sample | LRT Sample | URT Sample | LRT Sample | |
| Cat 01 | + | – | + | – | + (KP) | – | + (KP) | – |
| Cat 02 | + | – | + | – | + (KP) | – | + (KP) | – |
| Cat 03 | – | – | – | + | – | + (K.sp) | – | – |
| Cat 04 | – | – | – | – | – | – | – | – |
| Cat 05 | – | – | – | – | – | – | – | – |
| Cat 06 | – | – | – | – | – | – | – | – |
| Cat 07 | + | + | – | + | – | – | – | – |
| Cat 08 | + | – | – | – | – | – | – | – |
| Cat 09 | – | – | – | – | – | – | – | – |
| Cat 10 | – | – | – | – | – | – | – | – |
| Cat 11 | + | – | + | – | – | – | – | – |
| Cat 12 | + | – | – | – | – | – | – | – |
| Cat 13 | – | – | – | – | – | – | – | – |
| Cat 14 | + | – | – | – | – | – | – | – |
| Cat 15 | + | + | + | – | – | – | – | – |
| Cat 16 | – | – | – | – | – | – | – | – |
| Cat 17 | – | – | – | – | – | – | – | – |
| Cat 18 | + | + | + | + | – | – | – | – |
| Cat 19 | + | – | – | – | – | – | – | – |
| Cat 20 | + | – | – | – | – | – | – | – |
| Cat 21 | + | + | – | – | – | – | – | – |
| Cat 22 | – | – | – | – | – | – | – | – |
| Cat 23 | + | – | – | – | – | – | – | – |
| Cat 24 | + | + | + | – | – | – | – | – |
| Cat 25 | – | + | – | – | – | + (RE) | – | + (RE) |
| Cat 26 | + | + | – | – | – | – | – | – |
| Cat 27 | + | + | – | – | – | – | – | – |
| Cat 28 | + | + | – | – | – | – | – | – |
| Cat 29 | + | – | – | – | – | – | – | – |
| Cat 30 | – | + | – | + | – | – | – | – |
| Cat 31 | – | + | – | – | – | – | – | – |
| Cat 32 | + | + | – | – | – | – | – | – |
| Cat 33 | + | – | – | – | – | – | – | – |
| Cat 34 | + | + | + | – | – | – | – | – |
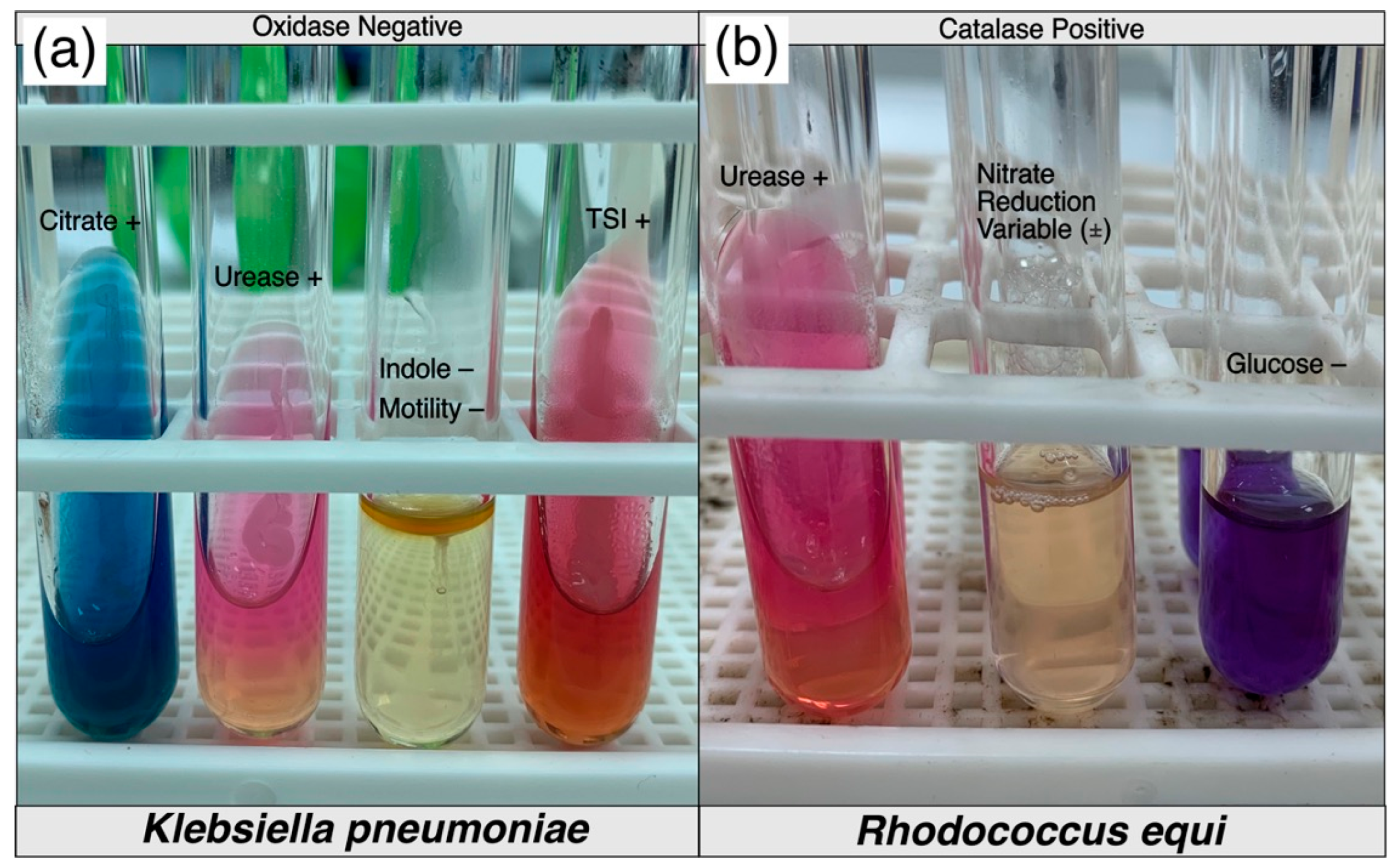
| Triple Sugar Iron | SIM | Citrate | Urease | Oxidase | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Slant | Butt | Gas | H2S | Sulphide | Indole | Motility | ||||
| Cat 01 Trachea | Alkaline | Acid | + | – | – | – | – | + | + | – |
| Cat 02 Trachea | Acid | Acid | + | – | – | – | – | + | + | – |
| Cat 03 Lungs | Acid | Acid | + | – | – | – | – | + | + | – |
| Catalase | Urease | Glucose | Nitrate reduction | |||||||
| Cat 25 Lungs | Positive | Positive | Negative | Variable | ||||||
| Parameters | N (%) |
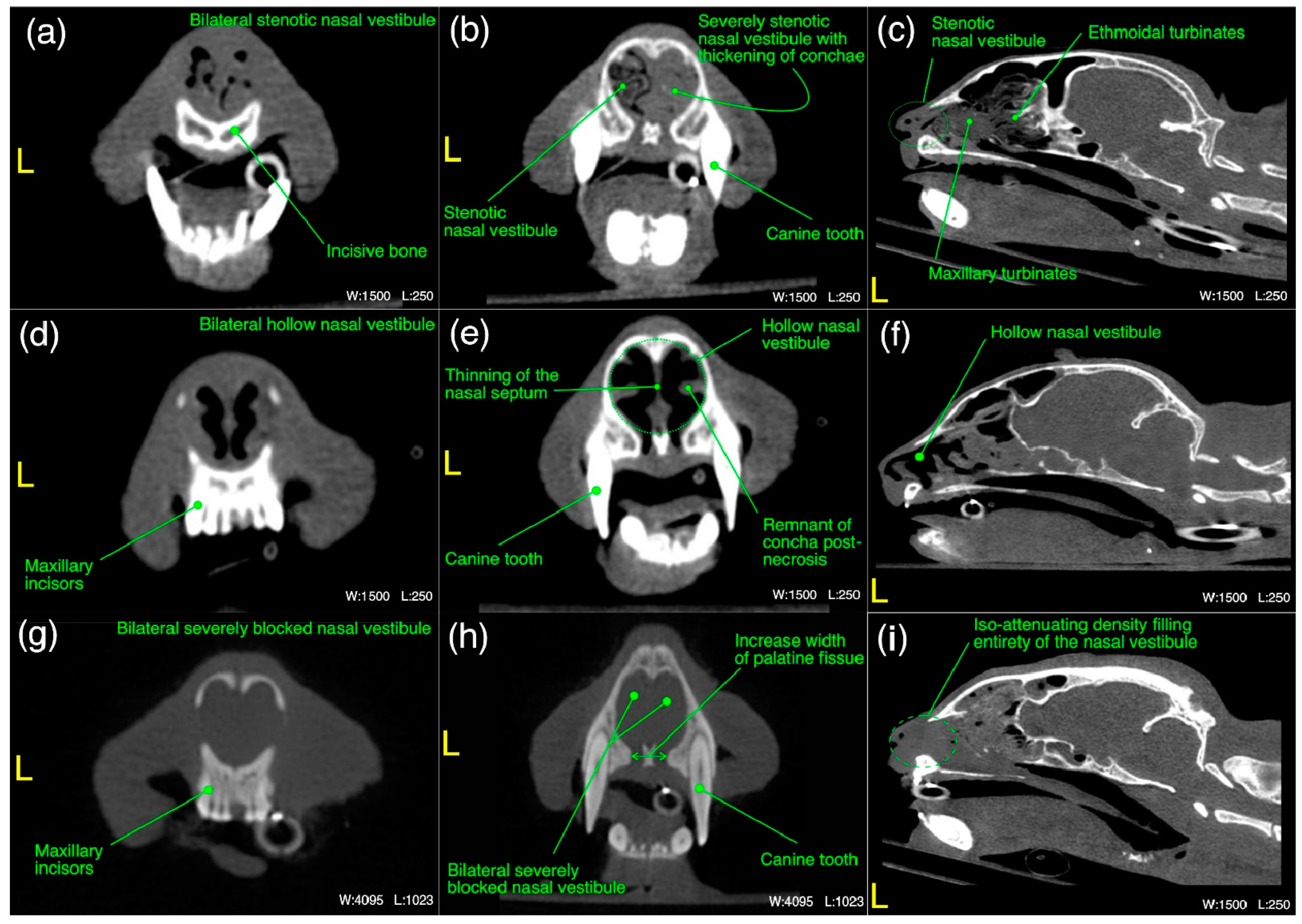
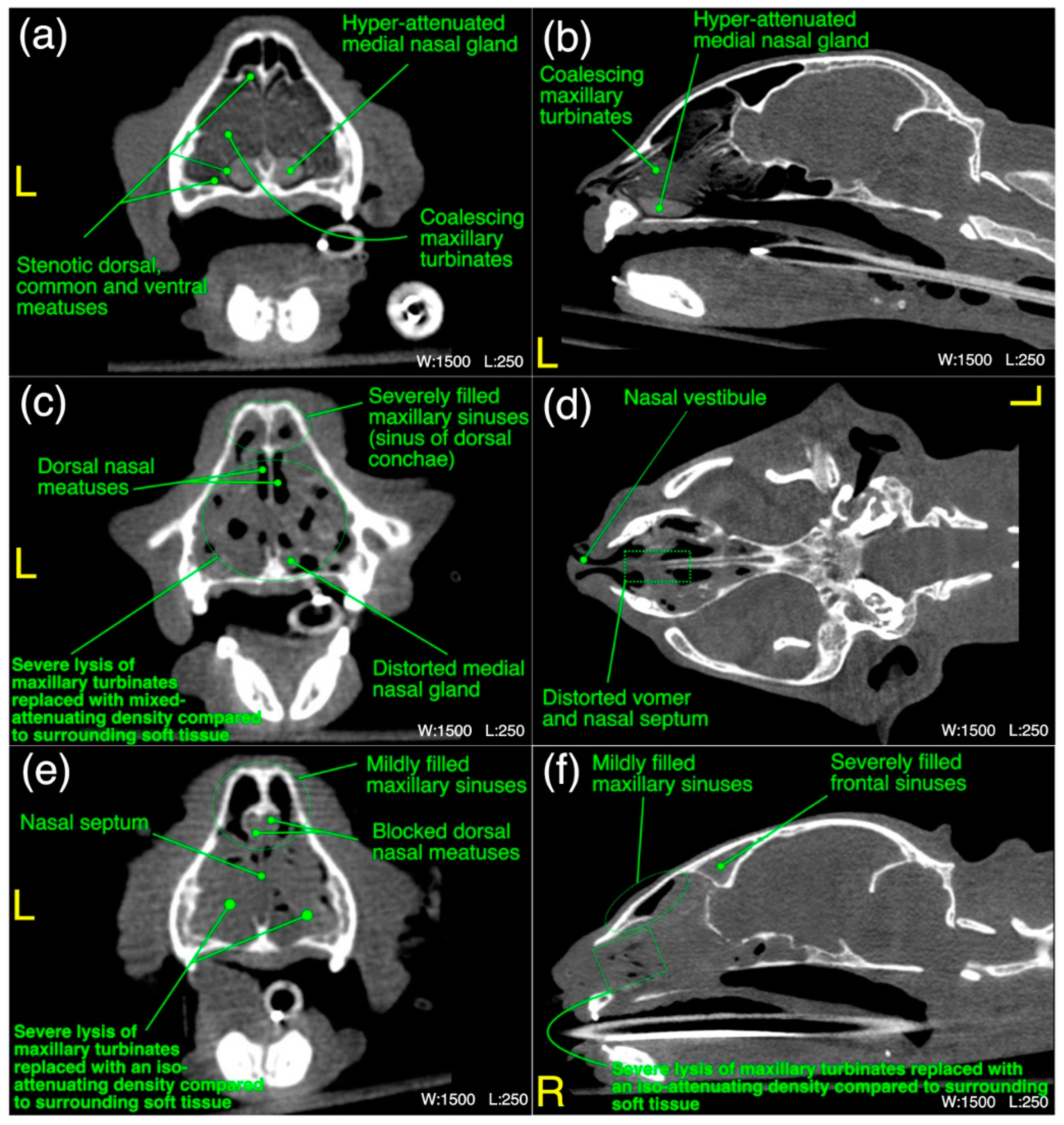
| Nasal vestibule (n =22) | |
| Unilateral moderate to severe thickening of the nasal conchae | 01 (05) |
| Bilateral moderate to severe thickening of the nasal conchae | 02 (09) |
| Severe blockage of the bilateral nasal vestibule with iso-/mixed-attenuating density | 04 (18) |
| Unilateral mild to moderate blockage of the nasal vestibule with iso-attenuating density | 03 (14) |
| Unilateral severe blockage of the nasal vestibule with iso-attenuating density | 04 (18) |
| Mild lysis of the surrounding bony structures | 01 (05) |
| Unilateral/bilateral mild to moderate pathological necrosis of the nasal conchae | 05 (23) |
| Bilateral mild to moderate increase in width of palatine fissure | 02 (09) |
| Unilateral/bilateral stenotic and mildly blocked nares (nasal opening) | 03 (14) |
| Maxilloturbinate region (n =22) | |
| Moderate to severe thickening ± hyper-attenuation of maxillary turbinates | 02 (09) |
| Bilateral severe lysis of the turbinates | 07 (32) |
| Unilateral/bilateral moderate lysis of the turbinates | 05 (23) |
| Bilateral partially/unilaterally (mild to moderate) occupied nasal passage with an abnormal density at maxilloturbinate region excluding sinus of dorsal conchae | 04 (18) |
| Bilateral severely occupied nasal passage with an abnormal density at the level of maxilloturbinate region excluding sinus of dorsal conchae | 09 (41) |
| Partial (mild) lysis of nasal septum | 06 (27) |
| Unilaterally/bilateral partially (moderate to severe) filled sinus of dorsal conchae | 03 (14) |
| Bilateral severely filled sinus of dorsal conchae | 06 (27) |
| Distortion/mild to moderate necrosis of the medial nasal gland | 08 (36) |
| Distortion/mild lysis of the vomer at any point along the nasal passage of this region | 05 (23) |
| Unilateral/bilateral severely stenotic maxillary nasal passage due to the thickening of maxillary turbinates | 03 (14) |
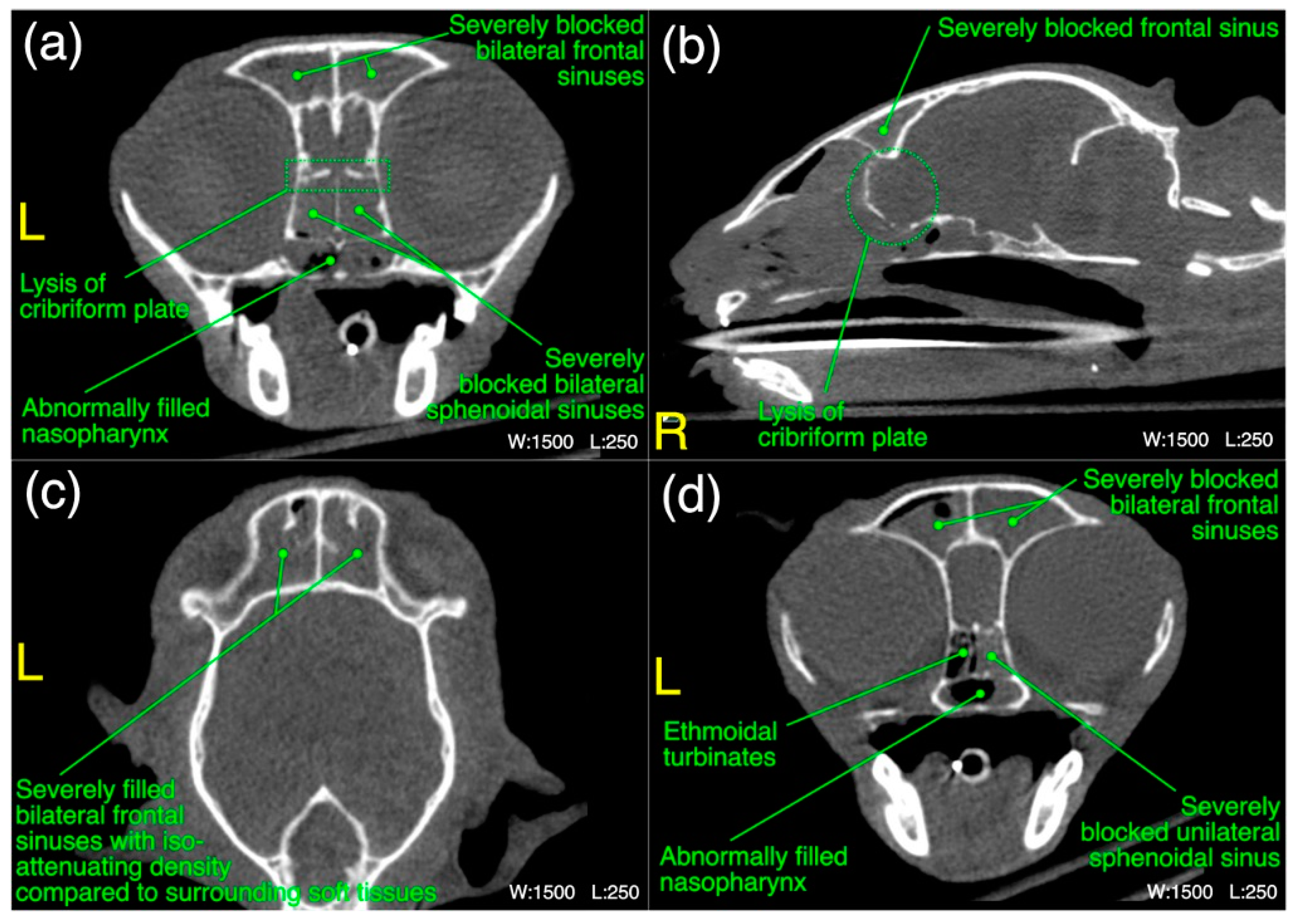
| Ethmoidal region (n =22) | |
| Bilateral moderate to severe lysis of the turbinates including basal laminae of ethmoid bone | 12 (55) |
| Bilateral moderate thickening ± hyper-attenuation of the ethmoidal turbinates including basal laminae of ethmoid bone | 04 (18) |
| Severe infiltration of abnormal space occupying density in bilateral nasal cavity of this region | 07 (32) |
| Mild to moderate infiltration of abnormal space occupying density in bilateral nasal cavity of this region | 04 (18) |
| Mild lysis of nasal septum | 02 (09) |
| Distorted/ moderate to severe necrosis of medial nasal gland | 06 (27) |
| Severe infiltration of the choanae with abnormal fluid/soft tissue density | 07 (32) |
| Mild to moderate infiltration of the choanae with abnormal fluid/soft tissue density | 03 (14) |
| Frontal sinus region (n =22) | |
| Severe infiltration of the bilateral frontal sinuses with abnormal soft tissue/fluid density | 02 (09) |
| Unilateral/mild to moderate bilateral infiltration of the frontal sinuses with abnormal soft tissue/fluid density | 10 (45) |
| Severe infiltration of the bilateral sphenoidal sinuses with abnormal soft tissue/fluid density | 05 (23) |
| Unilateral/mild to moderate bilateral infiltration of the sphenoidal sinuses with abnormal soft tissue/fluid density | 07 (32) |
| Mild lysis of the cribriform plate | 01 (5) |
| Mild to moderate infiltration of the nasopharynx with abnormal soft tissue/fluid density | 02 (09) |
| Mild to moderate lysis of the surrounding bony structures | 01 (05) |
| Neck region (n =22) | |
| Subcutaneous emphysema in fascial planes of the neck region | 02 (09) |
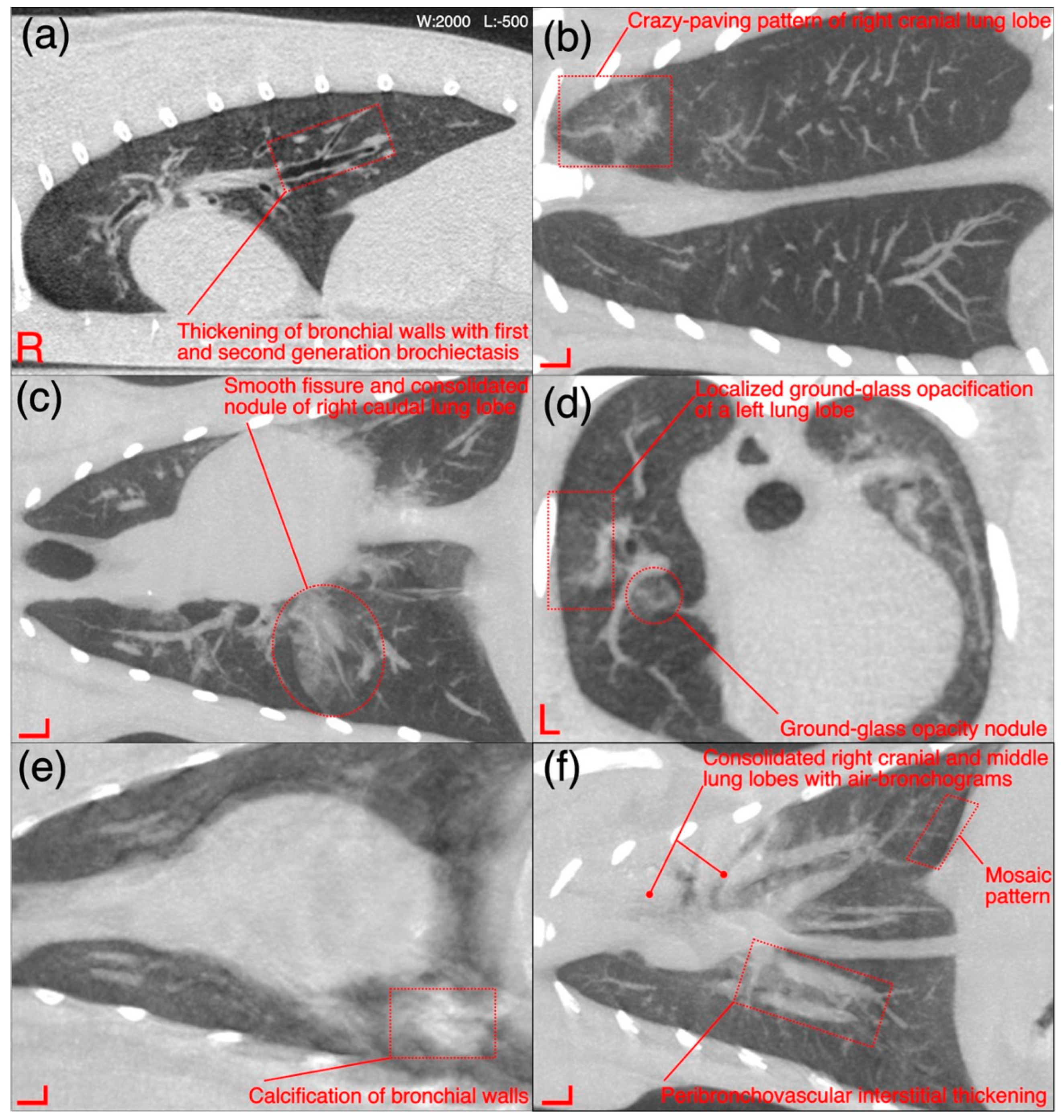
| Thoracic region (n =22) | |
| Mild thickening of the first/second/third generation bronchial walls | 08 (36) |
| Calcification of bronchial wall in any lung lobe(s) | 01 (05) |
| Mild mosaic pattern in any lung lobe | 04 (18) |
| Mild crazy-paving pattern | 02 (09) |
| Mild to moderate peribronchovascular interstitial thickening | 04 (18) |
| Ground glass opacification pattern in any lung lobe | 05 (23) |
| Halo sign in any lung lobe(s) | 01 (05) |
| Mild traction bronchiolectasis in any lung lobe(s) | 02 (09) |
| Consolidation of any lung lobe(s) | 02 (09) |
| Any collapsed lung lobe(s) | 01 (05) |
| Pneumomediastinum | 01 (05) |
| Megaesophagus | 01 (05) |
| Congenital pectus excavatum | 01 (05) |
| Congenital loss of unilateral diaphragmatic outline resulting into diaphragmatic hernia | 01 (05) |
| Additional findings from CT scans of skull, neck and thorax (n =22) | |
| Severe infiltration of the bilateral middle ear canal (tympanic bulla and tympanic cavity) with an abnormal soft tissue/fluid density | 08 (36) |
| Severe infiltration of the unilateral middle ear canal (tympanic bulla and tympanic cavity) with an abnormal soft tissue/fluid density | 01 (05) |
| Moderate infiltration of the bilateral middle ear canal (tympanic bulla and tympanic cavity) with an abnormal soft tissue/fluid density | 03 (14) |
| Subjectively enlarged mandibular lymph node(s) | 02 (09) |
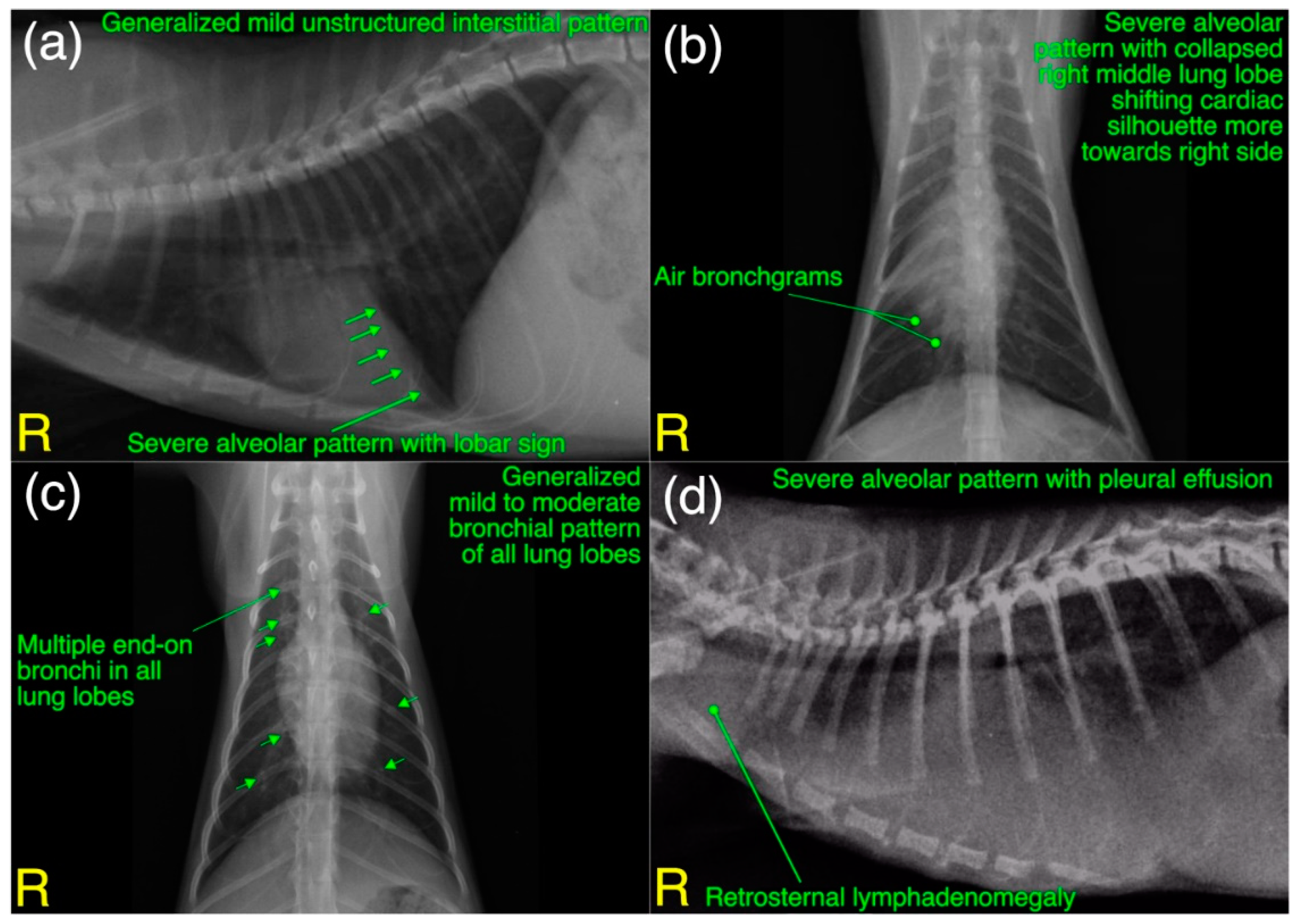
| Radiographic findings [(n =27) 22 shelter cats +5 privately owned cats] | |
| Mild to moderate bronchial pattern in any lung lobe(s) | 13 (48) |
| Generalized mild to moderate unstructured interstitial pattern in any lung lobe(s) | 03 (14) |
| Severe alveolar pattern with air bronchograms in any lung lobe(s) | 07 (26) ** |
| Mild vascular pattern including disturbance in caudal vena cava to descending aorta ratio (normal = 0.77 ± 0.2 for DSH cats) # | 06 (22) |
| Moderate to severe pleural effusion | 05 (19) |
| Cavitary lesion/pneumatocele in any lung lobe(s) | 02 (07) |
| Congenital pectus excavatum | 01 (04) |
| Congenital loss of unilateral diaphragmatic outline resulting into diaphragmatic hernia | 01 (04) |
| Liver silhouette beyond costochondral junction with well tapered edges | 15 (56) |
| Retrosternal lymph node enlargement | 04 (15) * |
| Deviated cardiac silhouette due to congenital malformations | 02 (07) |
| Slight to significant gas opacity in cervical and/or thoracic esophagus | 04 (15) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aslam, M.W.; Lau, S.F.; Radzi, R.; Omar, S.; Kaka, U.; Ahmed, I. Clinicopathological and Radiological Features of Cats Presented with Infectious Respiratory Disease Signs: A Focus on Rhodococcus equi and Klebsiella pneumoniae. Microorganisms 2023, 11, 737. https://doi.org/10.3390/microorganisms11030737
Aslam MW, Lau SF, Radzi R, Omar S, Kaka U, Ahmed I. Clinicopathological and Radiological Features of Cats Presented with Infectious Respiratory Disease Signs: A Focus on Rhodococcus equi and Klebsiella pneumoniae. Microorganisms. 2023; 11(3):737. https://doi.org/10.3390/microorganisms11030737
Chicago/Turabian StyleAslam, Muhammad Waseem, Seng Fong Lau, Rozanaliza Radzi, Sharina Omar, Ubedullah Kaka, and Ishtiaq Ahmed. 2023. "Clinicopathological and Radiological Features of Cats Presented with Infectious Respiratory Disease Signs: A Focus on Rhodococcus equi and Klebsiella pneumoniae" Microorganisms 11, no. 3: 737. https://doi.org/10.3390/microorganisms11030737