
The Main Bacterial Communities Identified in the Sites Affected by Periimplantitis: A Systematic Review

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Collection
3. Results
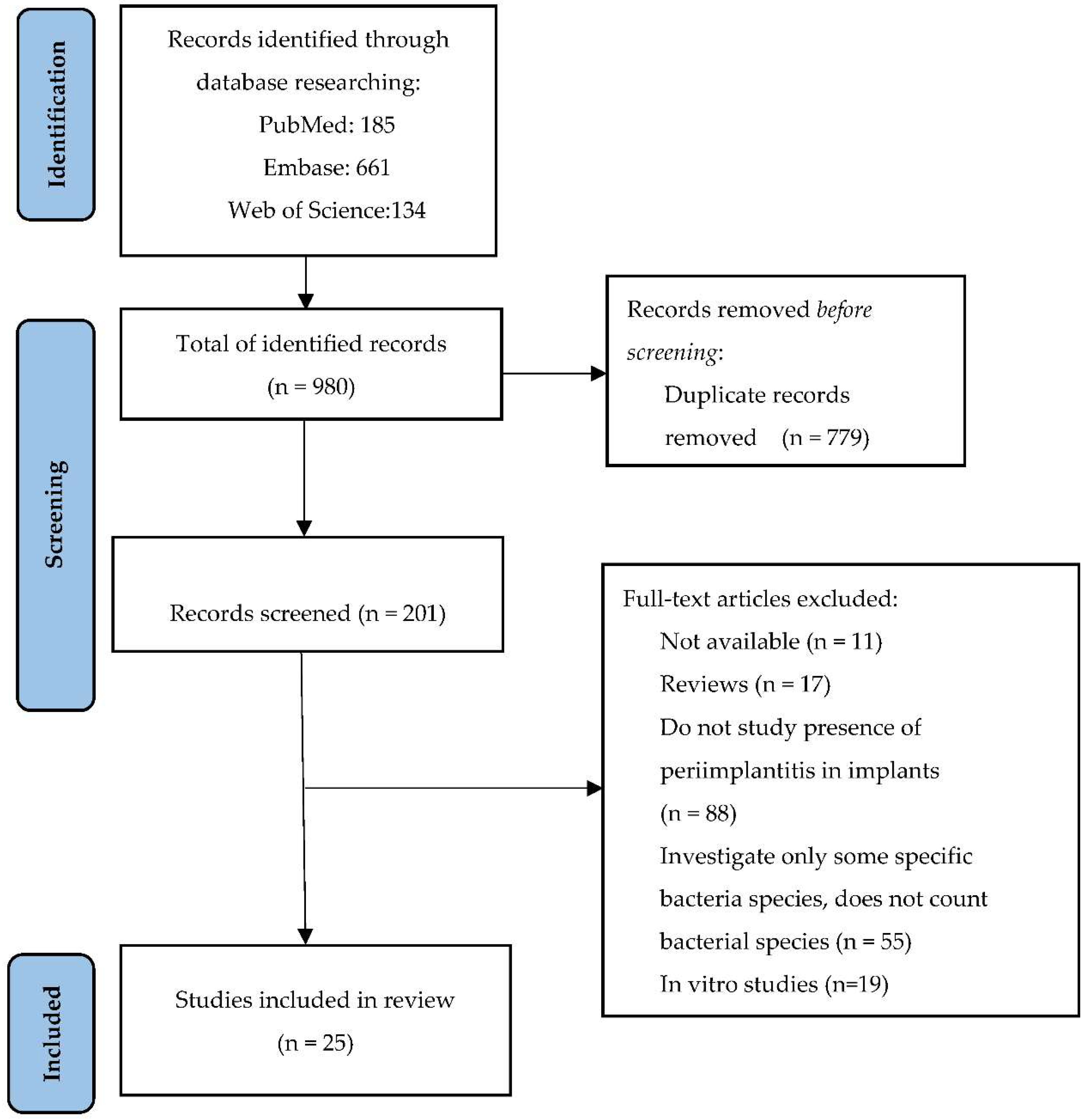
3.1. Bibliographic Documentation and Selection of Articles
3.2. Clinical and Microbiological Characteristics of the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Apratim, A.; Eachempati, P.; Krishnappa Salian, K.K.; Singh, V.; Chhabra, S.; Shah, S. Zirconia in dental implantology: A review. J. Int. Soc. Prev. Community Dent. 2015, 5, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saini, M.; Singh, Y.; Arora, P.; Arora, V.; Jain, K. Implant biomaterials: A comprehensive review. World J. Clin. Cases 2015, 16, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia dental implants: Where are we now, and where are we heading? Periodontol. 2000 2017, 73, 241–258. [Google Scholar] [CrossRef] [PubMed]
- Hanawa, T. Zirconia versus titanium in dentistry: A review. Dent. Mater. J. 2020, 31, 24–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pjetursson, B.E.; Valente, N.A.; Strasding, M.; Zwahlen, M.; Liu, S.; Sailer, I. A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic single crowns. Clin. Oral Implant. Res. 2018, 29, 199–214. [Google Scholar] [CrossRef] [Green Version]
- Sailer, I.; Strasding, M.; Valente, N.A.; Zwahlen, M.; Liu, S.; Pjetursson, B.E. A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic multiple-unit fixed dental prostheses. Clin. Oral Implant. Res. 2018, 29, 184–198. [Google Scholar] [CrossRef] [Green Version]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and Microbial Biofilm Profiles of Periimplantitis: A Systematic Review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and periimplantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Zhou, J.; Sun, X.; Li, X.; Zhou, Y. Diversity analysis of subgingival microbial bacteria in periimplantitis in Uygur population. Medicine 2018, 97, e9774. [Google Scholar] [CrossRef]
- Belibasakis, G.N.; Manoil, D. Microbial Community-Driven Etiopathogenesis of Periimplantitis. J. Dent. Res. 2021, 100, 21–28. [Google Scholar] [CrossRef]
- Sadid-Zadeh, R.; Willis, J.; Forgo, G.; Haraszthy, V. Comparative Analysis of Biofilm Formation on Materials Used for the Fabrication of Implant-Supported Prostheses. Braz. Dent. J. 2020, 31, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Persson, G.R.; Renvert, S. Cluster of bacteria associated with periimplantitis. Clin. Implant Dent. Relat. Res. 2014, 16, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J.M. Definition, etiology, prevention and treatment of periimplantitis—A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadkhodazadeh, M.; Amid, R.; Moscowchi, A. Does COVID-19 Affect Periodontal and Peri-Implant Diseases? J. Long-Term Eff. Med. Implant. 2020, 30, 1–2. [Google Scholar] [CrossRef]
- Sorsa, T.; Sahni, V.; Buduneli, N.; Gupta, S.; Räisänen, I.T.; Golub, L.M.; Lee, H.M.; Pätilä, T.; Bostanci, N.; Meurman, J.; et al. Active matrix metalloproteinase-8 (aMMP-8) point-of-care test (POCT) in the COVID-19 pandemic. Expert Rev. Proteom. 2021, 18, 707–717. [Google Scholar] [CrossRef]
- Mancini, L.; Americo, L.M.; Pizzolante, T.; Donati, R.; Marchetti, E. Impact of COVID-19 on Periodontitis and Peri-Implantitis: A Narrative Review. Front. Oral Health 2022, 3, 822–824. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune-Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rakašević, D.; Lazić, Z.; Rakonjac, B.; Soldatović, I.; Janković, S.; Magić, M.; Aleksić, Z. Efficiency of photodynamic therapy in the treatment of periimplantitis—A three-month randomized controlled clinical trial. Srp. Arh. Celok. Lek. 2016, 144, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Neilands, J.; Wickström, C.; Kinnby, B.; Davies, J.R.; Hall, J.; Friberg, B.; Svensäter, G. Bacterial profiles and proteolytic activity in periimplantitis versus healthy sites. Anaerobe 2015, 35, 28–34. [Google Scholar] [CrossRef]
- Soriano-Lerma, A.; Magán-Fernández, A.; Gijón, J.; Sánchez-Fernández, E.; Soriano, M.; García-Salcedo, J.A.; Mesa, F. Short-term effects of hyaluronic acid on the subgingival microbiome in periimplantitis: A randomized controlled clinical trial. J. Periodontol. 2020, 91, 734–745. [Google Scholar] [CrossRef]
- Arısan, V.; Karabuda, Z.C.; Arıcı, S.V.; Topçuoğlu, N.; Külekçi, G. A randomized clinical trial of an adjunct diode laser application for the nonsurgical treatment of periimplantitis. Photomed. Laser Surg. 2015, 33, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tada, H.; Masaki, C.; Tsuka, S.; Mukaibo, T.; Kondo, Y.; Hosokawa, R. The effects of Lactobacillus reuteri probiotics combined with azithromycin on periimplantitis: A randomized placebo-controlled study. J. Prosthodont. Res. 2018, 62, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Isehed, C.; Holmlund, A.; Renvert, S.; Svenson, B.; Johansson, I.; Lundberg, P. Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerative treatment of periimplantitis. A randomized controlled trial. J. Clin. Periodontol. 2016, 43, 863–873. [Google Scholar] [CrossRef]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennström, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Periimplantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef]
- Pranno, N.; Cristalli, M.P.; Mengoni, F.; Sauzullo, I.; Annibali, S.; Polimeni, A.; La Monaca, G. Comparison of the effects of air-powder abrasion, chemical decontamination, or their combination in open-flap surface decontamination of implants failed for periimplantitis: An ex vivo study. Clin. Oral Investig. 2021, 25, 2667–2676. [Google Scholar] [CrossRef] [PubMed]
- Wawrzyk, A.; Łobacz, M.; Adamczuk, A.; Sofińska-Chmiel, W.; Rahnama, M. The Efficacy of a Diode Laser on Titanium Implants for the Reduction of Microorganisms That Cause Periimplantitis. Materials 2021, 14, 7215. [Google Scholar] [CrossRef]
- Ciobanu, L.; Bancescu, G.; Didilescu, A.C.; Băncescu, A.A. Investigation of antibiotic susceptibility of the bacterial isolates and local flora changes after complex therapy in chronic periodontitis and periimplantitis. Farmacia 2018, 66, 1064–1069. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Muzafferiy, F.; Anderson, A.C.; Wölber, J.P.; Ratka-Krüger, P.; Fretwurst, T.; Nelson, K.; Vach, K.; Hellwig, E. Shift of microbial composition of periimplantitis-associated oral biofilm as revealed by 16S rRNA gene cloning. J. Med. Microbiol. 2018, 67, 332–340. [Google Scholar] [CrossRef]
- Zheng, H.; Xu, L.; Wang, Z.; Li, L.; Zhang, J.; Zhang, Q.; Chen, T.; Lin, J.; Chen, F. Subgingival microbiome in patients with healthy and ailing dental implants. Sci. Rep. 2015, 5, 10948. [Google Scholar] [CrossRef]
- Wang, H.; Liu, Y.; Li, W.; Li, W.; Xu, H.; Niu, G.; Wang, Z. Microbiota in Gingival Crevicular Fluid Before and After Mechanical Debridement with Antimicrobial Photodynamic Therapy in Periimplantitis. Front. Cell. Infect. Microbiol. 2022, 11, 1357. [Google Scholar] [CrossRef] [PubMed]
- Korsch, M.; Marten, S.M.; Stoll, D.; Prechtl, C.; Dötsch, A. Microbiological findings in early and late implant loss: An observational clinical case-controlled study. BMC Oral Health 2021, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Ghensi, P.; Manghi, P.; Zolfo, M.; Armanini, F.; Pasolli, E.; Bolzan, M.; Bertelle, A.; Dell’Acqua, F.; Dellasega, E.; Waldner, R.; et al. Strong oral plaque microbiome signatures for dental implant diseases identified by strain-resolution metagenomics. NPJ Biofilms Microbiomes 2020, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, E.S.; Feres, M.; Figueiredo, L.C.; Shibli, J.A.; Ramiro, F.S.; Faveri, M. Microbiological diversity of periimplantitis biofilm by Sanger sequencing. Clin. Oral Implant. Res. 2014, 25, 1192–1199. [Google Scholar] [CrossRef]
- Tamura, N.; Ochi, M.; Miyakawa, H.; Nakazawa, F. Analysis of bacterial flora associated with periimplantitis using obligate anaerobic culture technique and 16S rDNA gene sequence. Int. J. Oral Maxillofac. Implant. 2013, 28, 1521–1529. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Tong, Z.; Zhang, Y.; Si, M.; He, F. Microbial profiles of peri-implant mucositis and periimplantitis: Submucosal microbial dysbiosis correlates with disease severity. Clin. Oral Implant. Res. 2022, 33, 172–183. [Google Scholar] [CrossRef]
- Sanz-Martin, I.; Doolittle-Hall, J.; Teles, R.P.; Patel, M.; Belibasakis, G.N.; Hämmerle, C.; Jung, R.E.; Teles, F. Exploring the microbiome of healthy and diseased peri-implant sites using Illumina sequencing. J. Clin. Periodontol. 2017, 44, 1274–1284. [Google Scholar] [CrossRef]
- Yu, X.L.; Chan, Y.; Zhuang, L.; Lai, H.C.; Lang, N.P.; Keung Leung, W.; Watt, R.M. Intra-oral single-site comparisons of periodontal and peri-implant microbiota in health and disease. Clin. Oral Implant. Res. 2019, 30, 760–776. [Google Scholar] [CrossRef]
- Yeh, H.C.; Lu, J.J.; Chang, S.C.; Ge, M.C. Identification of microbiota in periimplantitis pockets by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Sci. Rep. 2019, 9, 774. [Google Scholar] [CrossRef]
- Maruyama, N.; Maruyama, F.; Takeuchi, Y.; Aikawa, C.; Izumi, Y.; Nakagawa, I. Intraindividual variation in core microbiota in periimplantitis and periodontitis. Sci. Rep. 2014, 4, 6602. [Google Scholar] [CrossRef] [Green Version]
- Kröger, A.; Hülsmann, C.; Fickl, S.; Spinell, T.; Hüttig, F.; Kaufmann, F.; Heimbach, A.; Hoffmann, P.; Enkling, N.; Renvert, S.; et al. The severity of human periimplantitis lesions correlates with the level of submucosal microbial dysbiosis. J. Clin. Periodontol. 2018, 45, 1498–1509. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch Losos, M.; Tugwell, P.; Ga, S.W.; Zello, G.A.; Petersen, J.A. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; The Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014. [Google Scholar]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef]
- Scarano, A.; Nardi, G.; Murmura, G.; Rapani, M.; Mortellaro, C. Evaluation of the Removal Bacteria on Failed Titanium Implants After Irradiation with Erbium-Doped Yttrium Aluminium Garnet Laser. J. Craniofac. Surg. 2016, 27, 1202–1204. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Resnik, R. Misch’s Avoiding Complications in Oral Implantology, 1st ed.; Elsevier: Maryland Heights, MO, USA, 2017; pp. 771–826. [Google Scholar]
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Article Title | Authors | Year of Publication | Study Design | Study Samples | Population Characteristics | Bacterial Isolation Technique | Isolated Bacteria |
|---|---|---|---|---|---|---|---|
| Diversity analysis of subgingival microbial bacteria in periimplantitis in Uygur population | Gao et al. [9] | 2018 | Observational Study | 40 samples of gingival crevicular fluid divided into two groups: healthy implants (Control group) and periimplantitis (Case group) | Uygur patients who had treatment with dental implants from 2013 to 2016 | DNA extraction, PCR amplification and 16S rRNA gene sequencing | Prevotella, Streptococcus, Acinetobacter, Fusobacterium, Neisseria, Porphyromonas, Treponema, Leptothrix, Capnocytophaga |
| Efficiency of photodynamic therapy in the treatment of periimplantitis—A three-month randomized controlled clinical trial | Rakašević et al. [19] | 2016 | Randomized controlled clinical trial | Samples from 52 periimplantitis sites divided into two groups (Study group and Control group) | Patients with periimplantitis who presented in two dental clinics in Belgrade between January 2014 until February 2015 | Bacterial culture for the diagnosis of aerobic and anaerobic pathogens | Veillonella spp., Prevotella intermedia, Peptostreptococcus spp., Peptostreptococcus asaccharolyticus, Porphyromonas gingivalis, Fusobacterium nucleatum, Actinomyces odontolyticus |
| Bacterial profiles and proteolytic activity in periimplantitis versus healthy sites | Neilands et al. [20] | 2015 | Non-randomized, controlled, clinical study | 50 samples (25 from healthy subjects, 25 from periimplantitis sites) | Patients with dental implants treatment in the past, attending maintenance appointments in a dental clinic in Sweden | Bacterial culture on Brucella agar | Porphyromonas/Prevotella, Fusobacterium, Tannerella, Streptococcus oralis, Streptococcus mitis, Streptococcus anginosus, Streptococcus constellatus, Streptococcus intermedius |
| Short-term effects of hyaluronic acid on the subgingival microbiome in periimplantitis: A randomized controlled clinical trial | Soriano-Lerma et al. [21] | 2020 | Randomized controlled trial | 108 samples divided into 3 groups (Test group, Control group 1, Control group 2) | Patients diagnosticated with periimplantitis in a private dental office in Spain | DNA isolation, PCR amplification and 16S rRNA gene sequencing | Fusobacterium, Prevotella, Porphyromonas, Ralstonia, Sphingomonas, Streptococcus, Treponema, Propionibacterium, Alloprevotella, Veillonella, Lactobacillus, Haemophilus, Staphylococcus, Campylobacter, Tannerella |
| A randomized clinical trial of an adjunct diode laser application for the nonsurgical treatment of periimplantitis | Arısan et al. [22] | 2015 | Randomized clinical trial | Samples collected from 24 implants affected by periimplantitis at baseline and 1 month after intervention | 10 patients diagnosticated with periimplantitis who went to the department clinic in Istanbul University between February 2010 and May 2013 | DNA extraction, PCR amplification and hybridization procedures | Actinomyces odontolyticus, Actinomyces viscosus, Aggregatibacteractinomycetemcomitans, Campylobacter concisus, Campylobacter gracilis, Campylobacterrectus/showae, Capnocytophaga gingivalis/sputigena/ochracea, Eikenella corrodens, Eubacterium nodatum, Fusobacterium nucleatum, Peptostreptococcus micros, Porphyromonas gingivalis, Prevotella intermedia, Prevotellanigrescens, Streptococcus constellatus group, Streptococcusgordonii group, Streptococcus mitis group, Tannerella forsythia (Bacteroides forsythus; Tannerella forsythensis), Treponema denticola, and Veillonella parvula. |
| The effects of Lactobacillus reuteri probiotics combined with azithromycin on periimplantitis: A randomized placebo-controlled study | Tada et al. [23] | 2017 | Randomized placebo-controlled study | Samples collected from periimplantitis sites at baseline and 4, 12, and 24 weeks after allocated treatment | 30 patients diagnosticated with periimplantitis from 7 different institutions including Kyushu Dental University Hospital, Japan, divided into 2 groups, placebo and probiotics | DNA isolation, PCR amplification and 16S rRNA gene sequencing | Treponema denticola, Fusobacterium nucleatum, Peptostreptococcus micros, Streptococcus constellatus, Prevotella nigrescens, Tannerella forsythia, Campylobacter gracilis. Prevotella intermedia, Campylobacter rectus, Porphyromonas gingivalis, Veillonella parvula, Streptococcus gordonii, Capnocytophaga, Streptococcus mitis |
| Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerativetreatment of periimplantitis. A randomized controlled trial | Isehed et al. [24] | 2016 | Randomized controlled trial | Samples collected from the deepest pocket of the each implant at baseline, 2 weeks, 3, 6, and 12 months after surgery treatment | 29 patients diagnosticated with periimplantitis from a periodontology clinic in Sweden | DNA extraction with Gen Elute Bacterial Geno-mic DNA kit (Sigma Aldrich, St. Louis, MO, USA), bacterial characterization by the HOMIM microarray | Fusobacteria (cluster probe), Parvimonas micra, Porphyromonas sp., Eubacterium nodatum, Porphyromonas gingivalis, Ochrobactrum anthropi, Tannerella forsythia and Campylobacter concisus/Campylobacter rectus. |
| Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Periimplantitis: A Randomized Controlled Clinical Trial | Carcuac et al. [25] | 2016 | Randomized Controlled Clinical Trial | Samples collected from periimplantitis sites at baseline, 3, 6 and 12 months after surgery | 100 patients with severe periimplantitis who were referred to 2 clinics specialized in periodontics in Sweden | Culture and checkerboard DNA-DNA hybridization analyses | Fusobacterium nucleatum, Prevotella intermedia/Prevotella nigrescens, Campylobacter rectus, Porphyromonas gingivalis, Tannerella forsythia, Porphyromonas endodontalis, Parvimonas micra |
| Comparison of the effects of air-powder abrasion, chemical decontamination, or their combination in open-flap surface decontamination of implants failed for periimplantitis: an ex vivo study | Pranno et al. [26] | 2021 | Single-blind, randomized, controlled, ex vivo study | 80 samples collected from the retrieved implants | 20 patients from Oral Surgery Unit University of Rome with minimum 4 implants affected by periimplantitis which need to be explanted | Bacterial culture techniques: for aerobic bacteria—Columbia sheep blood agar plates and for anaerobic—Schaedler sheep blood agar | Staphylococcus aureus, Streptococcus mitis/oralis, Staphylococcus epidermidis and Streptococcus salivarius. Enterococcus faecalis, Candida albicans, Pseudomonas aeruginosa and Neisseria flavescens |
| The Efficacy of a Diode Laser on Titanium Implants for the Reduction of Microorganisms That Cause Periimplantitis | Wawrzyk et al. [27] | 2021 | Clinical study | Samples collected from saliva, the surfaces of the crowns and dental implants components | 3 patients with advanced periimplantitis | Bacterial culture technique of anaerobic using Schaedler horse blood agar | Staphylococcus aureus, Streptococcus constellatus, Streptococcus oralis, Streptococcus pneumoniae, Rothia mucilaginosa, and Rothia aeria, and the following Gram-negative bacteria: Haemophilus parainfluenzae, Klebsiella pneumoniae, Klebsiella oxytoca, and Veilonella parvula. Candida guilliermondii, Actinomyces odontolyticus |
| Investigation of antibiotic susceptibility of the bacterial isolates and local flora changes after complex therapy in chronic periodontitis and periimplantitis | Ciobanu et al. [28] | 2018 | Clinical study | Samples collected from sites with periimplantitis before and after therapy | Patients diagnosticated with chronic periimplantitis | Culture examination | Capnocytophaga spp., Prevotella oralis, S. intermedius, S. gordonii, Veillonella spp. |
| Shift of microbial composition of periimplantitis-associated oral biofilm as revealed by 16S rRNA gene cloning | Al-Ahmad et al. [29] | 2018 | Cross-sectional study | Samples collected from the deepest sites of periimplantitis and from the periimplantar healthy sulcus | 10 patients with at least one implant affected by periimplantitis and one healthy implant | DNA extraction and PCR amplification of 16S rRNA genes | Streptococcus spp., Prevotella spp., Fusobacterium spp., Eubacterium spp., Porphyromonas gingivalis, Treponema spp., Campylobacter spp., Filifactor alocis, Abitrophia defectiva, Alloprevotella tannarae, Neisseria spp., Parvimonas micra, Selenomonas spp., Capnocytophaga spp., Atopobium spp., Peptostreptococcus spp., Tannerella forsythia, Scadovia wiggisiae, Bacteroidetes bacterium, Eikenella Corodens, Fretibacterium fastidiosum, Johnsonella ignava, Synergistales bacterium, Dialister invisus, Raoultella sp. |
| Subgingival microbiome in patients with healthy and ailing dental implants | Zheng et al. [30] | 2015 | Clinical study | Samples collected from periimplantar sulcus and pockets | 10 patients with healthy implants, 8 patients with perimucositis and 6 with periimplantitis | Microbial DNA extraction, 16S rRNA gene library preparation, and pyrosequencing | Leptotrichia hofstadii, Eubacterium infirmum, Kingella denitrificans, Actinomycescardiffensis, Eubacterium minutum, Treponema lecithinolyticum, and Gemella sanguinis were higher in PI sites Streptococcus, Leptotrichia, Actinomyces, Capnocytophaga, Prevotella, Fusobacterium, Neisseria |
| Microbiota in Gingival Crevicular Fluid Before and After Mechanical Debridement With Antimicrobial Photodynamic Therapy in Periimplantitis | Wang et al. [31] | 2022 | Clinical study | 61 samples collected from all the implants: before treatment and 7, 14, 30, 60 and 180 days after treatment | 9 patients presented at Department of Stomatology in Beijing Hospital with 14 implants affected by periimplantitis | Bacterial 16S rRNA was amplified and sequenced using an Illumina MiSeq platform | Bacteroidetes, Proteobacteria, Firmicutes, Fusobacteria, Spirochaetes, Synergistetes, and Actinobacteria Prevotella, Neisseria, Fusobacterium, Porphyromonas, Treponema, Streptococcus, Haemophilus, Capnocytophaga, Leptotrichia, and Fretibacterium |
| Microbiological findings in early and late implant loss: an observational clinical case-controlled study | Korsch et al. [32] | 2021 | Observational clinical case–control study | Samples collected from implants affected by severe periimplantitis without any chance of preservation and from healthy implants as controls | 48 patients with 53 implants were introduced in the study | DNA extraction, PCR amplification and 16S rRNA gene sequencing | Treponema sp., Streptococcus, Fretibacterium, Anaerovoracaceae uncl, Desulfobulbus sp., Pseudoramibacter alactolyticus, Dialister pneumosintes, Streptococcus sanguinis, Shewanella sp., Pantoea sp., Haemophilus sp., Haemophilus parainfluenzae, Pseudomonas sp., Lautropia mirabilis, Actinomyces naeslundii |
| Strong oral plaque microbiome signatures for dental implant diseases identified by strain-resolution metagenomics | Ghensi et al. [33] | 2020 | Clinical study | Samples collected from each implant and from contralateral healthy implant or tooth for every patient included in the study | 80 patients enrolled in the study: 28 with healthy implants, 28 with mucositis and 24 with periimplantitis | DNA extraction | P. gingivalis, T. forsythia, Treponema denticola, P. endodontalis, F. fastidiosum, Filifactor alocis, Desulfobulbus spp., T. lecithinolyticum |
| Cluster of bacteria associated with periimplantitis | Persson et al. [12] | 2014 | Retrospective clinical study | Samples collected at one implant with periimplantitis in each of 166 patients and from 47 healthy implants | 166 patients with periimplantitis and 47 patients with healthy dental implants | Checkerboard DNA–DNA hybridization | Actinomyces odontolyticus, A. actinomycetemcomitans (a), Campylobacter gracilis, Campylobacter rectus, Campylobacter showae, Helicobacter pylori, Haemophilus influenzae, Leptothrichia buccalis, P. intermedia, Propionybacterium acnes, Porphyromonas endodontalis, P. gingivalis, Staph. aureus, Staph. anaerobius, Streptococcus intermedius, Streptococcus mitis, T. forsythia, T. denticola, and Treponema socranskii. |
| Microbiological diversity of periimplantitis biofilm by Sanger sequencing | da Silva et al. [34] | 2014 | Clinical study | Samples collected from the deepest pocket depth in the test group and from mesial site of healthy implants | 20 individuals, 10 with healthy implants and 10 with at least one implant with periimplantitis, both groups with minimum 10 periodontally healthy teeth | Extraction of DNA, PCR amplification of universal 16S rRNA | Fusobacterium nucleatum, Campylobacter gracilis, Dialister invisus, Streptococcus sp., Eubacterium infirmum, Filifactor alocis and Mitsuokella sp., Parvimonas micra and Prevotella intermedia |
| Analysis of bacterial flora associated with periimplantitis using obligate anaerobic culture technique and 16S rDNA gene sequence | Tamura et al. [35] | 2013 | Clinical study | Samples collected from the deepest sites of the both groups, test and control | 30 patients, 15 diagnosticated with periimplantitis, 15 with healthy implants | Culture technique and 16S rDNA gene sequence | Streptococcus, Eubacterium, Prevotella, Actinomyces, Fusobacterium, Eubacterium nodatum, Prevotella intermedia, Fusobacterium nucleatum, Filifactor alocis, E brachy, Parascardovia denticolenns, Parvimonas micra |
| Microbial profiles of peri-implant mucositis and periimplantitis: submucosal microbial dysbiosis correlates with disease severity | Shi et al. [36] | 2022 | Cross-sectional study | Samples collected from 64 patients, 27 with perimucositis and 37 with periimplantitis | Patients with periimplantitis or perimucositis presented in Dep. Of Oral Implantology in Zhejiang University School of Medicine, China | DNA extraction, PCR amplification and 16S rRNA gene sequencing | Porphyromonas, Fusobacterium, Treponema and Prevotella, Campylobacter, Filifactor, Alloprevotella |
| Exploring the microbiome of healthy and diseased peri-implant sites using Illumina sequencing | Sanz-Martin et al. [37] | 2017 | Clinical study | Sample collection from 32 healthy implants and from 35 implants affected by periimplantitis | Patients with healthy implants and with periimplantitis presented in center of Dental Medicine at the University of Zürich | Bacterial nucleic acids isolation, sample DNA analyzed by sequencing the 16S rRNA gene V3-V4 hypervariable region | Porphyromonas (phylum Bacteroidetes), Treponema (phylum Spirochetes), Filifactor (phylum Firmicutes), Fretibacterium (phylum Synergistetes) and Tannerella (phylum Bacteroidetes) |
| Intra-oral single-site comparisons of periodontal and peri-implant microbiota in health and disease | Yu et al. [38] | 2019 | Clinical study | Samples collected from 4 sites for each patient: Healthy implant, healthy tooth, periimplantitis site and periodontitis site | 18 Chinese partial dentate patients with both periimplantitis and periodontitis | DNA extraction, PCR amplification | Bacteroidetes and Prevotella taxa (including P. denticola, P. multiformis and P. fusca). |
| Identification of microbiota in periimplantitis pockets by matrix assisted laser desorption/ionization time-of-flight mass spectrometry | Yeh et al. [39] | 2019 | Clinical study | Samples collected from periimplantitis pockets | 12 patients with periimplantitis | Culture examination | Neisseria flavescen, Streptococcus constellatus, Slackia exigua, Streptococcus intermedius, Fusobacteriumnucleatum, Gemella morbillorum and Gram-positive anaerobic Bacillus |
| Intraindividual variation in core microbiota in periimplantitis and periodontitis | Maruyama et al. [40] | 2014 | Clinical study | Samples collected from the deepest pockets in periimplantitis sites and in periodontitis sites | 20 Patients with both periimplantitis and periodontitis | DNA extraction and PCR amplification of 16S rRNA genes | Olsenella, Sphingomonas, Peptostreptococcus, unclassified Neisseriaceae, genus Desulfomicrobium, Actinomyces johnsonii, Fusobacterium nucleatum, Porphyromonas gingivalis, Streptococcus oralis, Treponema denticola, and Treponema socranskii Achromobacter xylosoxidans, Actinomyces massiliensis, and Porphyromonas sp. |
| The severity of human periimplantitislesions correlates with the level of submucosal microbial dysbiosis | Kröger et al. [41] | 2018 | Cohort study or case–control study | Samples collected from all 45 implants affected by periimplantitis | 30 patients with at list one implant with periimplantitis | DNA extraction and PCR amplification of 16S rRNA genes | Eubacteriaceae, Fretibacterium sp., Fretibacterium fastidiosum, Peptostreptococcaceae, Alloprevotella sp., Fastidiosipila sanguinis, Filifactor alocis, Peptostreptococcaceae, Bacteriodetes bacterium, Treponema parvum, Clostridiales bacterium, and Orobacterium, Granulicatella elegans, Rothia aeria, Corynebacterium durum, Veillonella dispar, Acinetobacter |
| Study | Selection | Comparability | Outcome | NOS Score |
|---|---|---|---|---|
| Case–control studies | ||||
| Gao et al. [9] | *** | * | *** | 7 |
| Rakašević et al. [19] | *** | ** | *** | 8 |
| Neilands et al. [20] | *** | * | *** | 7 |
| Soriano-Lerma et al. [21] | *** | * | ** | 6 |
| Arısan et al. [22] | *** | ** | *** | 8 |
| Tada et al. [23] | *** | ** | *** | 8 |
| Isehed et al. [24] | *** | ** | ** | 7 |
| Carcuac et al. [25] | *** | ** | ** | 7 |
| Pranno et al. [26] | *** | * | *** | 7 |
| Wawrzyk et al. [27] | ** | * | *** | 6 |
| Ciobanu et al. [28] | * | * | *** | 5 |
| Al-Ahmad et al. [29] | ** | * | *** | 6 |
| Zheng et al. [30] | ** | * | *** | 6 |
| Korsch et al. [32] | ** | * | *** | 6 |
| Persson et al. [12] | *** | * | *** | 7 |
| da Silva et al. [34] | *** | * | *** | 7 |
| Tamura et al. [35] | *** | * | *** | 7 |
| Shi et al. [36] | *** | * | *** | 7 |
| Sanz-Martin et al. [37] | *** | * | ** | 6 |
| Yeh et al. [39] | ** | * | 3 | |
| Maruyama et al. [40] | *** | * | *** | 7 |
| Kröger et al. [41] | ** | * | * | 4 |
| Cohort studies | ||||
| Wang et al. [31] | *** | * | *** | 7 |
| Ghensi et al. [33] | **** | * | *** | 8 |
| Yu et al. [38] | **** | * | *** | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iușan, S.A.L.; Lucaciu, O.P.; Petrescu, N.B.; Mirică, I.C.; Toc, D.-A.; Albu, S.; Costache, C. The Main Bacterial Communities Identified in the Sites Affected by Periimplantitis: A Systematic Review. Microorganisms 2022, 10, 1232. https://doi.org/10.3390/microorganisms10061232
Iușan SAL, Lucaciu OP, Petrescu NB, Mirică IC, Toc D-A, Albu S, Costache C. The Main Bacterial Communities Identified in the Sites Affected by Periimplantitis: A Systematic Review. Microorganisms. 2022; 10(6):1232. https://doi.org/10.3390/microorganisms10061232
Chicago/Turabian StyleIușan, Simina Angela Lăcrimioara, Ondine Patricia Lucaciu, Nausica Bianca Petrescu, Ioana Codruța Mirică, Dan-Alexandru Toc, Silviu Albu, and Carmen Costache. 2022. "The Main Bacterial Communities Identified in the Sites Affected by Periimplantitis: A Systematic Review" Microorganisms 10, no. 6: 1232. https://doi.org/10.3390/microorganisms10061232