Acute Kidney Injury in Patients Undergoing Cardiac Transplantation: A Meta-Analysis

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Methods
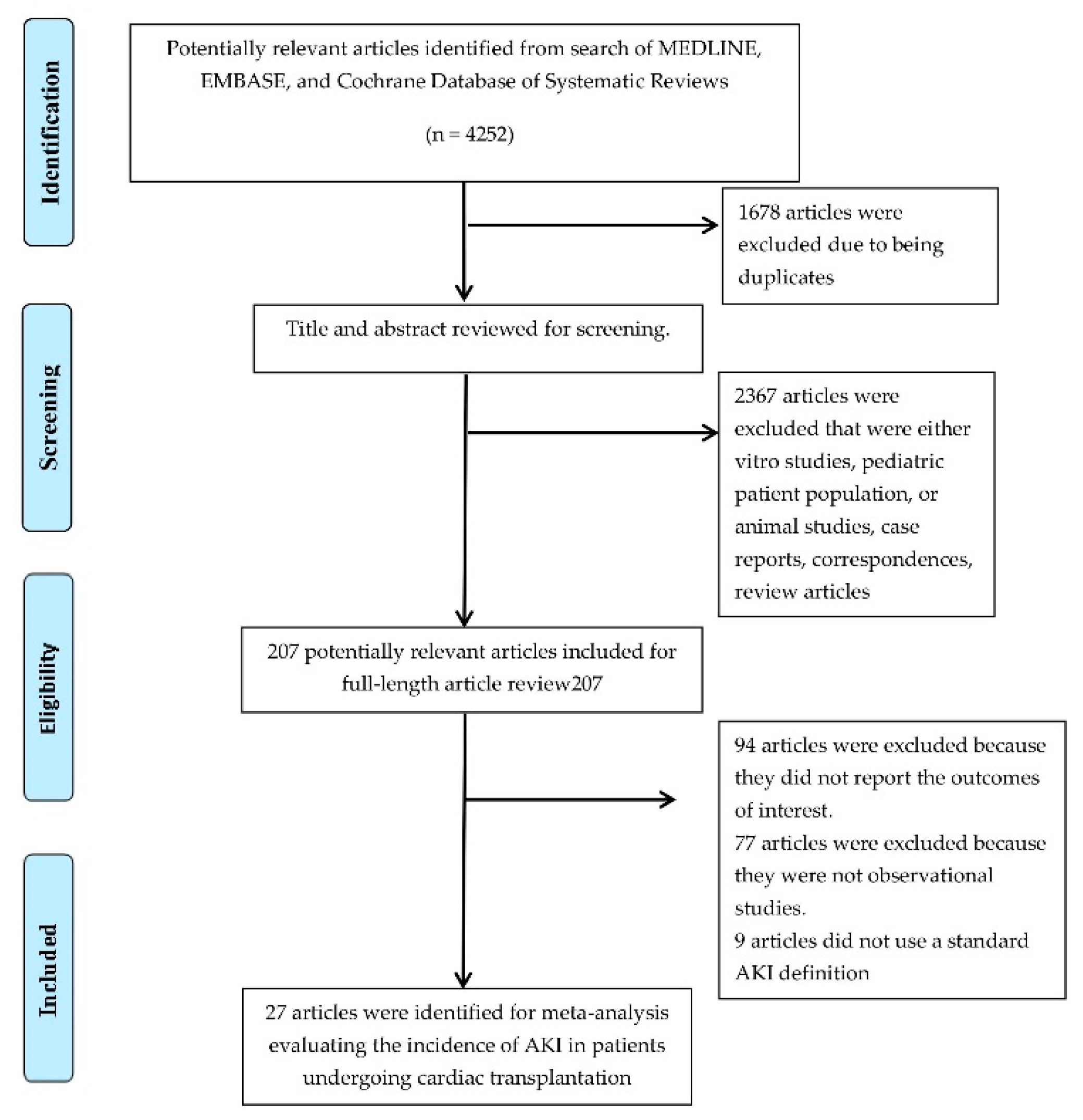
2.1. Search Strategy
2.2. Study Selection
2.3. Statistical Analysis
3. Results
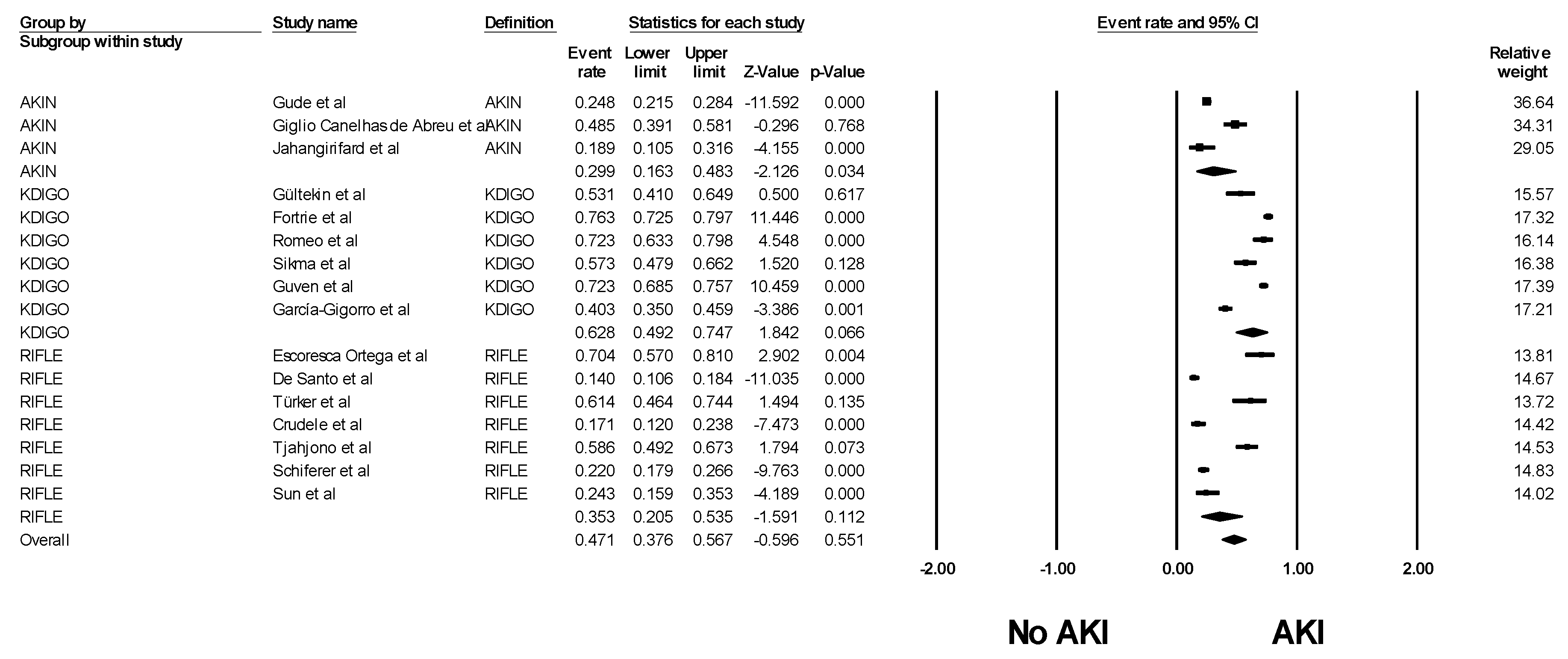
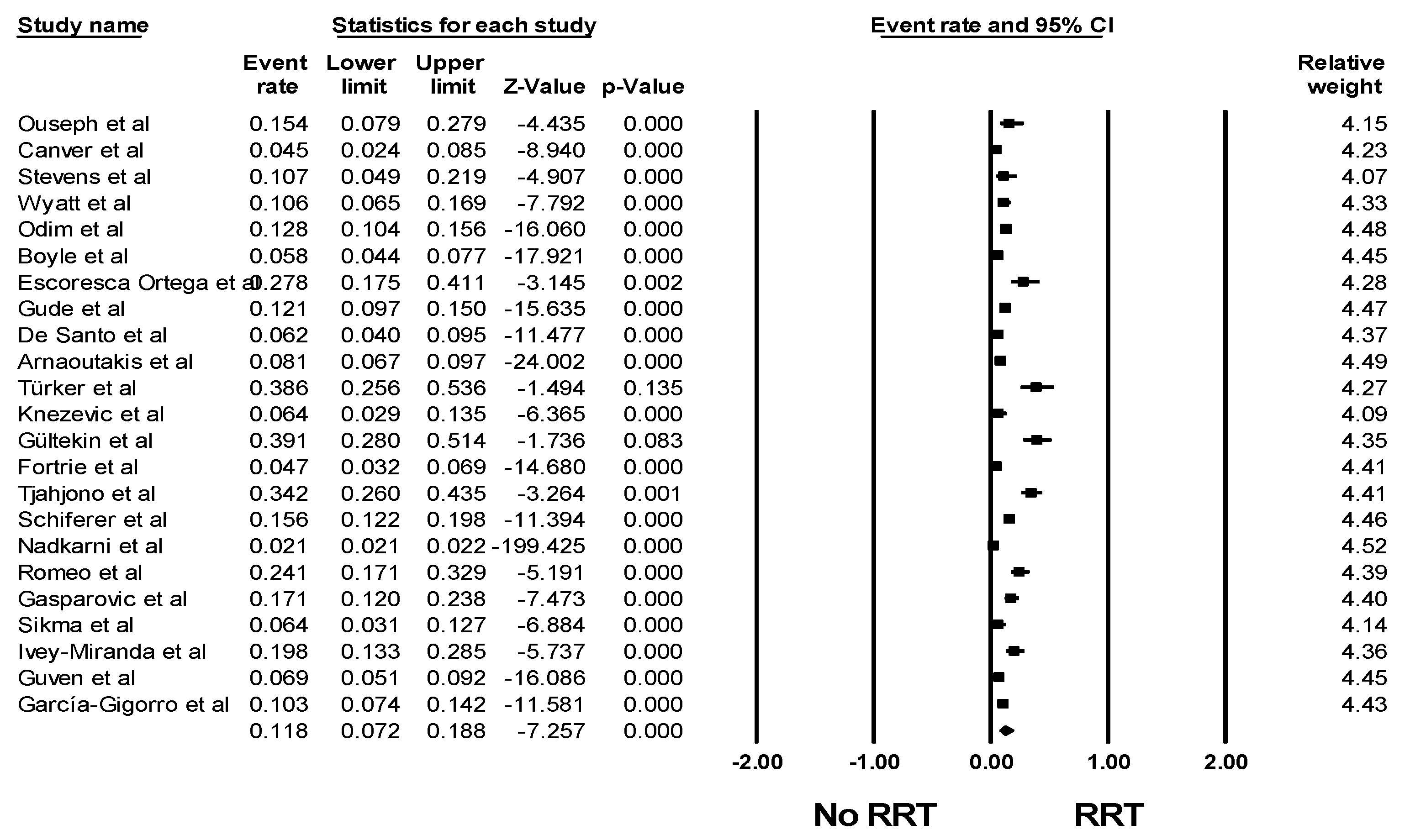
3.1. Incidence of AKI Among Patients Undergoing Cardiac Transplantation
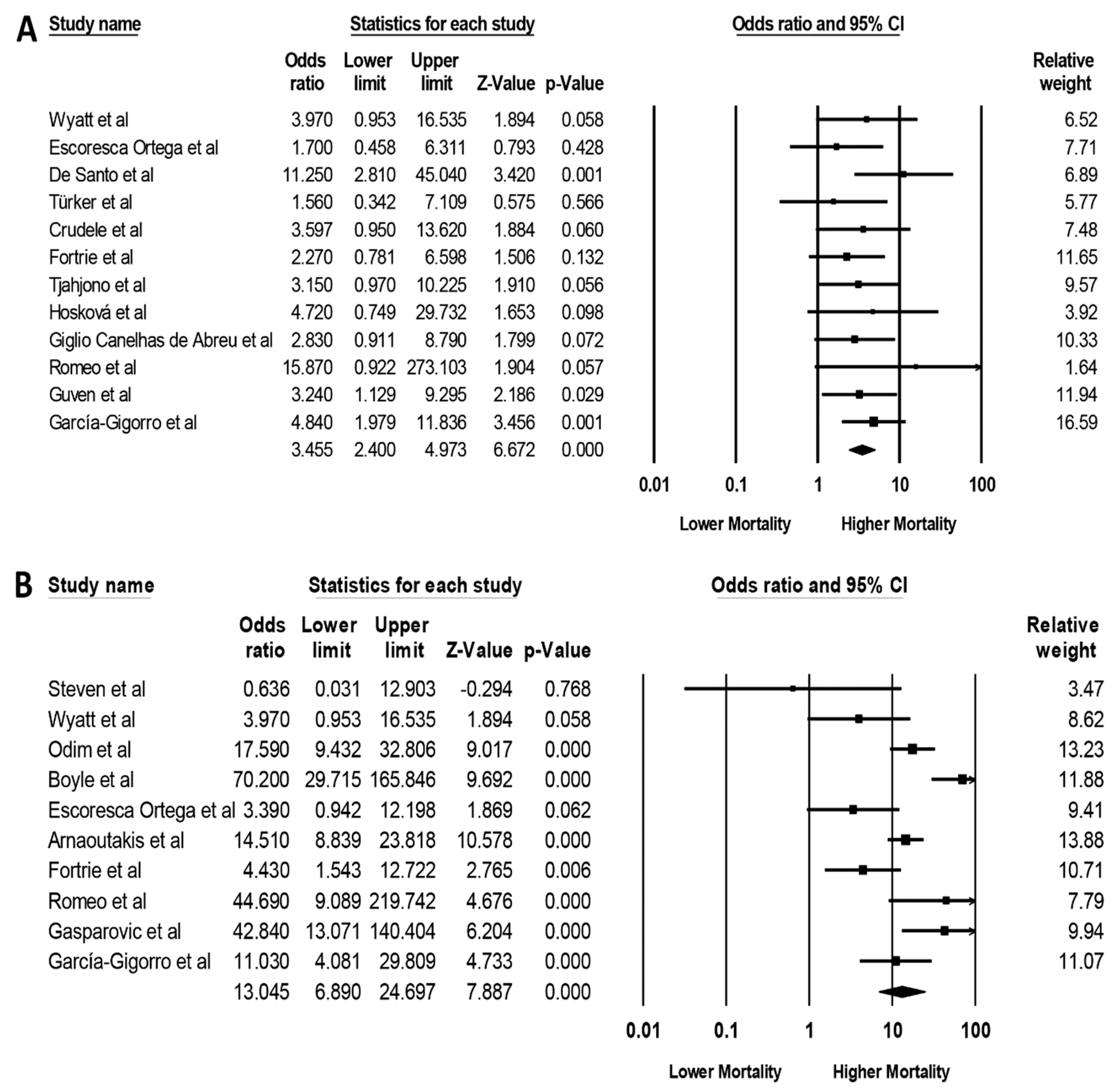
3.2. Impact of AKI on Mortality among Patients Undergoing Cardiac Transplantation
3.3. Evaluation for Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hoste, E.A.J.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerda, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Ponce, D.; Balbi, A. Acute kidney injury: Risk factors and management challenges in developing countries. Int. J. Nephrol. Renov. Dis. 2016, 9, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Burdmann, E.A.; Cerda, J.; Feehally, J.; Finkelstein, F.; Garcia-Garcia, G.; Godin, M.; Jha, V.; Lameire, N.H.; Levin, N.W.; et al. Recognition and management of acute kidney injury in the International Society of Nephrology 0by25 Global Snapshot: A multinational cross-sectional study. Lancet 2016, 387, 2017–2025. [Google Scholar] [CrossRef]
- Yang, F.; Zhang, L.; Wu, H.; Zou, H.; Du, Y. Clinical analysis of cause, treatment and prognosis in acute kidney injury patients. PLoS ONE 2014, 9, e85214. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, S.; Marks, A.; Fluck, N.; Levin, A.; McLernon, D.; Prescott, G.; Black, C. Post-discharge kidney function is associated with subsequent ten-year renal progression risk among survivors of acute kidney injury. Kidney Int. 2017, 92, 440–452. [Google Scholar] [CrossRef] [Green Version]
- Pavkov, M.E.; Harding, J.L.; Burrows, N.R. Trends in Hospitalizations for Acute Kidney Injury, United States, 2000–2014. Morb. Mortal. Wkly. Rep. 2018, 67, 289–293. [Google Scholar] [CrossRef]
- Barnard, C.N. The Operation A human cardiac transplant: An interim report of a successful operation performed at Groote Schuur Hospital, Cape Town. S. Afr. Med. J. 1967, 41, 1271–1274. [Google Scholar]
- Fortrie, G.; Manintveld, O.C.; Caliskan, K.; Bekkers, J.A.; Betjes, M.G. Acute Kidney Injury as a Complication of Cardiac Transplantation: Incidence, Risk Factors, and Impact on 1-year Mortality and Renal Function. Transplantation 2016, 100, 1740–1749. [Google Scholar] [CrossRef]
- Zijlstra, L.E.; Constantinescu, A.A.; Manintveld, O.; Birim, O.; Hesselink, D.A.; van Thiel, R.; van Domburg, R.; Balk, A.H.; Caliskan, K. Improved long-term survival in Dutch heart transplant patients despite increasing donor age: The Rotterdam experience. Transpl. Int. 2015, 28, 962–971. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar]
- John, R.; Rajasinghe, H.A.; Chen, J.M.; Weinberg, A.D.; Sinha, P.; Mancini, D.M.; Naka, Y.; Oz, M.C.; Smith, C.R.; Rose, E.A.; et al. Long-term outcomes after cardiac transplantation: An experience based on different eras of immunosuppressive therapy. Ann. Thorac. Surg. 2001, 72, 440–449. [Google Scholar] [CrossRef]
- Belayev, L.Y.; Palevsky, P.M. The link between acute kidney injury and chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2014, 23, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic kidney disease and mortality risk: A systematic review. J. Am. Soc. Nephrol. 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [PubMed]
- Hamour, I.M.; Omar, F.; Lyster, H.S.; Palmer, A.; Banner, N.R. Chronic kidney disease after heart transplantation. Nephrol. Dial. Transplant. 2009, 24, 1655–1662. [Google Scholar] [CrossRef] [Green Version]
- Ojo, A.O.; Held, P.J.; Port, F.K.; Wolfe, R.A.; Leichtman, A.B.; Young, E.W.; Arndorfer, J.; Christensen, L.; Merion, R.M. Chronic renal failure after transplantation of a nonrenal organ. N. Engl. J. Med. 2003, 349, 931–940. [Google Scholar] [CrossRef]
- Lund, L.H.; Khush, K.K.; Cherikh, W.S.; Goldfarb, S.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Chambers, D.C.; Yusen, R.D.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Heart Transplantation Report-2017; Focus Theme: Allograft ischemic time. J. Heart Lung Transpl. 2017, 36, 1037–1046. [Google Scholar] [CrossRef]
- Alam, A.; Badovinac, K.; Ivis, F.; Trpeski, L.; Cantarovich, M. The outcome of heart transplant recipients following the development of end-stage renal disease: Analysis of the Canadian Organ Replacement Register (CORR). Am. J. Transpl. 2007, 7, 461–465. [Google Scholar] [CrossRef]
- Garcia-Gigorro, R.; Renes-Carreno, E.; Corres Peiretti, M.A.; Arribas Lopez, P.; Perez Vela, J.L.; Gutierrez Rodriguez, J.; Delgado, J.F.; Cortina Romero, J.M.; Montejo Gonzalez, J.C. Incidence Risk Factors and Outcomes of Early Acute Kidney Injury After Heart Transplantation: An 18-year Experience. Transplantation 2018, 102, 1901–1908. [Google Scholar] [CrossRef]
- Romeo, F.J.; Varela, C.F.; Vulcano, N.; Pizarro, R.; Greloni, G.; Posatini, R.; Marenchino, R.; Rosa-Diez, G.J.; Belziti, C.A. Acute Kidney Injury After Cardiac Transplantation: Foe or Common Innocent Bystander? Transplant. Proc. 2018, 50, 1489–1495. [Google Scholar] [CrossRef]
- Tjahjono, R.; Connellan, M.; Granger, E. Predictors of Acute Kidney Injury in Cardiac Transplantation. Transpl. Proc. 2016, 48, 167–172. [Google Scholar] [CrossRef]
- Martinelli, S.M.; Patel, U.D.; Phillips-Bute, B.G.; Milano, C.A.; Archer, L.E.; Stafford-Smith, M.; Shaw, A.D.; Swaminathan, M. Trends in cardiac surgery-associated acute renal failure in the United States: A disproportionate increase after heart transplantation. Ren. Fail. 2009, 31, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yeom, S.Y.; Hwang, H.Y.; Choi, J.W.; Cho, H.J.; Lee, H.Y.; Huh, J.H.; Kim, K.B. Twenty-Year Experience of Heart Transplantation: Early and Long-Term Results. Korean J. Thorac. Cardiovasc. Surg. 2016, 49, 242–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoskova, L.; Franekova, J.; Malek, I.; Kautzner, J.; Szarszoi, O.; Jabor, A.; Pindak, M.; Viklicky, O.; Melenovsky, V. Comparison of Cystatin C and NGAL in Early Diagnosis of Acute Kidney Injury After Heart Transplantation. Ann. Transplant. 2016, 21, 329–345. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Section 2: AKI Definition. Kidney Int. 2012, 2, 19–36. [CrossRef] [Green Version]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury, N. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative w: Acute renal failure, definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Ouseph, R.; Brier, M.E.; Jacobs, A.A.; Erbeck, K.M. Continuous venovenous hemofiltration and hemodialysis after orthotopic heart transplantation. Am. J. Kidney Dis. 1998, 32, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Canver, C.C.; Heisey, D.M.; Nichols, R.D. Acute renal failure requiring hemodialysis immediately after heart transplantation portends a poor outcome. J. Cardiovasc. Surg. 2000, 41, 203–206. [Google Scholar]
- Stevens, L.M.; El-Hamamsy, I.; Leblanc, M.; Perrault, L.P.; Pellerin, M.; Bouchard, D.; Carrier, M. Continuous renal replacement therapy after heart transplantation. Can. J. Cardiol. 2004, 20, 619–623. [Google Scholar] [PubMed]
- Wyatt, C.M.; Arons, R.R. The burden of acute renal failure in nonrenal solid organ transplantation. Transplantation 2004, 78, 1351–1355. [Google Scholar] [CrossRef]
- Odim, J.; Wheat, J.; Laks, H.; Kobashigawa, J.; Gjertson, D.; Osugi, A.; Mukherjee, K.; Saleh, S. Peri-operative renal function and outcome after orthotopic heart transplantation. J. Heart Lung Transplant. 2006, 25, 162–166. [Google Scholar] [CrossRef]
- Boyle, J.M.; Moualla, S.; Arrigain, S.; Worley, S.; Bakri, M.H.; Starling, R.C.; Heyka, R.; Thakar, C.V. Risks and outcomes of acute kidney injury requiring dialysis after cardiac transplantation. Am. J. Kidney Dis. 2006, 48, 787–796. [Google Scholar] [CrossRef]
- Escoresca Ortega, A.M.; Ruiz de Azua Lopez, Z.; Hinojosa Perez, R.; Ferrandiz Millon, C.M.; Diaz Martin, A.; Corcia Palomo, Y.; Lage Galle, E. Kidney failure after heart transplantation. Transplant. Proc. 2010, 42, 3193–3195. [Google Scholar] [CrossRef]
- Gude, E.; Andreassen, A.K.; Arora, S.; Gullestad, L.; Grov, I.; Hartmann, A.; Leivestad, T.; Fiane, A.E.; Geiran, O.R.; Vardal, M.; et al. Acute renal failure early after heart transplantation: Risk factors and clinical consequences. Clin. Transplant. 2010, 24, E207–E213. [Google Scholar] [CrossRef]
- De Santo, L.S.; Romano, G.; Amarelli, C.; Maiello, C.; Baldascino, F.; Bancone, C.; Grimaldi, F.; Nappi, G. Implications of acute kidney injury after heart transplantation: What a surgeon should know. Eur. J. Cardio Thorac. Surg. 2011, 40, 1355–1361. [Google Scholar] [CrossRef]
- Arnaoutakis, G.J.; George, T.J.; Kilic, A.; Beaty, C.A.; Weiss, E.S.; Conte, J.V.; Shah, A.S. Risk factors for early death in patients bridged to transplant with continuous-flow left ventricular assist devices. Ann. Thorac. Surg. 2012, 93, 1549–1554. [Google Scholar] [CrossRef]
- Turker, M.; Zeyneloglu, P.; Sezgin, A.; Pirat, A.; Arslan, G. RIFLE criteria for acute kidney dysfunction following heart transplantation: Incidence and risk factors. Transpl. Proc. 2013, 45, 3534–3537. [Google Scholar] [CrossRef] [PubMed]
- Crudele, V.; Cacciatore, F.; Grimaldi, V.; Maiello, C.; Romano, G.; Amarelli, C.; Picascia, A.; Abete, P.; Napoli, C. Human leukocyte antigen-DR mismatch is associated with increased in-hospital mortality after a heart transplant. Exp. Clin. Transplant. 2013, 11, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, I.; Poglajen, G.; Hrovat, E.; Oman, A.; Pintar, T.; Wu, J.C.; Vrtovec, B.; Haddad, F. The effects of levosimendan on renal function early after heart transplantation: Results from a pilot randomized trial. Clin. Transplant. 2014, 28, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Gultekin, B.; Beyazpinar, D.S.; Ersoy, O.; Ozkan, M.; Akay, H.T.; Sezgin, A. Incidence and Outcomes of Acute Kidney Injury After Orthotopic Cardiac Transplant: A Population-Based Cohort. Exp. Clin. Transplant. 2015, 3, 26–29. [Google Scholar]
- Schiferer, A.; Zuckermann, A.; Dunkler, D.; Eskandary, F.; Bernardi, M.; Hiesmayr, M.; Lassnigg, A.; Hutschala, D. Acute Kidney Injury and Outcome After Heart Transplantation: Large Differences in Performance of Scoring Systems. Transplantation 2016, 100, 2439–2446. [Google Scholar] [CrossRef] [PubMed]
- Nadkarni, G.N.; Chauhan, K.; Patel, A.; Saha, A.; Poojary, P.; Kamat, S.; Patel, S.; Ferrandino, R.; Konstantinidis, I.; Garimella, P.S.; et al. Temporal trends of dialysis requiring acute kidney injury after orthotopic cardiac and liver transplant hospitalizations. BMC Nephrol. 2017, 18, 244. [Google Scholar] [CrossRef]
- Giglio Canelhas de Abreu, L.; Proenca Vieira, L.; Teixeira Gomes, T.; Bacal, F. Clinical and Nutritional Factors Associated With Early Mortality After Heart Transplantation. Transplant. Proc. 2017, 49, 874–877. [Google Scholar] [CrossRef]
- Sun, G.H.; Patel, V.; Moreno-Duarte, I.; Zahedi, F.; Ursprung, E.; Couper, G.; Chen, F.Y.; Welsby, I.J.; Comenzo, R.; Kao, G.; et al. Intraoperative Administration of 4-Factor Prothrombin Complex Concentrate Reduces Blood Requirements in Cardiac Transplantation. J. Cardiothorac. Vasc. Anesth. 2018, 32, 161–167. [Google Scholar] [CrossRef]
- Gasparovic, H.; Svetina, L.; Loncaric, F.; Ljubas, J.; Cikes, M.; Biocina, B.; Milicic, D. Preponderance of microbial isolates among heart transplantation recipients requiring renal replacement therapy: A propensity score-adjusted analysis. Croat. Med. J. 2018, 59, 224–231. [Google Scholar] [CrossRef]
- Sikma, M.A.; Hunault, C.C. Association of Whole Blood Tacrolimus Concentrations with Kidney Injury in Heart Transplantation Patients. Eur. J. Drug. Metab. Pharmacokinet. 2018, 43, 311–320. [Google Scholar]
- Ivey-Miranda, J.B.; Flores-Umanzor, E.; Farrero-Torres, M.; Santiago, E.; Cepas-Guillen, P.L.; Perez-Villa, F. Predictors of renal replacement therapy after heart transplantation and its impact on long-term survival. Clin. Transplant. 2018, 32, e13401. [Google Scholar] [CrossRef] [PubMed]
- Jahangirifard, A.; Ahmadi, Z.H.; Naghashzadeh, F.; Sharif-Kashani, B.; Rashid-Farokhi, F.; Afshar, A.; Yamini-Sharif, R.; Rezaei, Y. Prophylactic Fibrinogen Decreases Postoperative Bleeding but Not Acute Kidney Injury in Patients Undergoing Heart Transplantation. Clin. Appl. Thromb. Hemost. 2018, 24, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Guven, G.; Brankovic, M.; Constantinescu, A.A.; Brugts, J.J.; Hesselink, D.A.; Akin, S.; Struijs, A.; Birim, O.; Ince, C.; Manintveld, O.C.; et al. Preoperative right heart hemodynamics predict postoperative acute kidney injury after heart transplantation. Intensive Care Med. 2018, 44, 588–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alraies, M.C.; Eckman, P. Adult heart transplant: Indications and outcomes. J. Thorac. Dis. 2014, 6, 1120–1128. [Google Scholar]
- Jung, S.H.; Kim, J.J.; Choo, S.J.; Yun, T.J.; Chung, C.H.; Lee, J.W. Long-term mortality in adult orthotopic heart transplant recipients. J. Korean Med. Sci. 2011, 26, 599–603. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Story, D.; Letis, A.; Klemz, K.; Matalanis, G.; Seevanayagam, S.; Dragun, D.; Seeliger, E.; Mertens, P.R.; et al. Effect of mean arterial pressure, haemoglobin and blood transfusion during cardiopulmonary bypass on post-operative acute kidney injury. Nephrol. Dial. Transpl. 2012, 27, 153–160. [Google Scholar] [CrossRef]
- Pickering, J.W.; James, M.T.; Palmer, S.C. Acute kidney injury and prognosis after cardiopulmonary bypass: A meta-analysis of cohort studies. Am. J. Kidney Dis. 2015, 65, 283–293. [Google Scholar] [CrossRef]
- Moreira, R.; Jacinto, T.; Neves, P.; Vouga, L.; Baeta, C. Predictors of Acute Kidney Injury Associated with Cardiopulmonary Bypass. Rev. Port. Cir. Cardio Torac. Vasc. 2019, 26, 109–115. [Google Scholar]
- Neyra, J.A.; Hu, M.C.; Minhajuddin, A.; Nelson, G.E.; Ahsan, S.A.; Toto, R.D.; Jessen, M.E.; Moe, O.W.; Fox, A.A. Kidney Tubular Damage and Functional Biomarkers in Acute Kidney Injury Following Cardiac Surgery. Kidney Int. Rep. 2019, 4, 1131–1142. [Google Scholar] [CrossRef] [Green Version]
- Zhong, J.; Yang, H.C.; Fogo, A.B. A perspective on chronic kidney disease progression. Am. J. Physiol. Renal. Physiol. 2017, 312, F375–F384. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Srivali, N.; Kittanamongkolchai, W.; Harrison, A.M.; Greason, K.L.; Kashani, K.B. Persistent acute kidney injury following transcatheter aortic valve replacement. J. Card Surg. 2017, 32, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Kittanamongkolchai, W.; Sakhuja, A.; Greason, K.L.; Kashani, K.B. The association between renal recovery after acute kidney injury and long-term mortality after transcatheter aortic valve replacement. PLoS ONE 2017, 12, e0183350. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Patient Population | Number | Definition of AKI | Incidence of AKI | Mortality |
|---|---|---|---|---|---|---|---|
| Ouseph et al. [31] | 1998 | USA | Orthotopic heart transplant | 52 | RRT | RRT, 8/52 (15.4%) | 1-year mortality RRT, 5/8 (62.5%) |
| Canver et al. [32] | 2000 | USA | Orthotopic heart transplant | 199 | RRT | RRT, 9/199 (4.5%) | RRT, 4/9 (44.4%) |
| Stevens et al. [33] | 2004 | Canada | Heart transplant | 56 | CRRT | CRRT, 6/56 (10.71%) | RRT, 0/6 (0%) |
| Wyatt et al. [34] | 2004 | USA | Heart transplant in New York State | 141 | RRT | RRT, 15/141 (10.6%) | N/A |
| Odim et al. [35] | 2005 | USA | Orthotopic heart transplant | 627 | RRT | RRT, 80/627 (12.8%) | Hospital mortality RRT, 33/80 (41.3%) |
| Boyle et al. [36] | 2006 | USA | Orthotopic heart transplant | 756 | RRT | RRT, 44/756 (5.8%) | Hospital mortality RRT, 22/44 (50%) 30-day mortality RRT, 17/44 (38.6%) |
| Escoresca Ortega et al. [37] | 2010 | Spain | Heart transplant | 54 | RIFLE criteria | AKI, 38/54 (70.4%) RRT, 15/54 (27.8%) | AKI, 30/38 (78.94%) RRT, 7/15 (46.7%) |
| Gude et al. [38] | 2010 | Norway | Orthotopic heart transplant | 585 | AKIN criteria | AKI, 145/585 (24.8%) RRT, 71/585 (12.1%) | 30-day mortality RRT, 11/71 (15.5%) 90-day mortality RRT, 15/71 (21.1%) |
| De Santo et al. [39] | 2011 | Italy | Orthotopic heart transplant | 307 | RIFLE criteria | AKI, 43/307 (14.0%) CVVH, 19/307 (6.2%) | Hospital mortality AKI, 12/43 (27.9%) 1-year mortality AKI, 12/43 (27.9%) |
| Arnaoutakis et al. [40] | 2012 | USA | LVAD-bridged heart transplant from UNOS data | 1312 | RRT | RRT, 106/1312 (8.1%) | 90-day mortality RRT, 41/93 (44.1%) |
| Türker et al. [41] | 2013 | Turkey | Heart transplant | 44 | RIFLE criteria | AKI, 27/44 (61.4%) RRT, 17/44 (38.6%) | AKI, 7/26 (26.9%) |
| Crudele et al. [42] | 2013 | Italy | Heart transplant | 158 | RIFLE criteria | AKI, 27/158 (17.1%) | AKI, 9/27 (33.3%) |
| Knezevic et al. [43] | 2014 | Slovenia | Heart transplant | 94 | RRT | RRT, 6/94 (6.4%) | N/A |
| Gültekin et al. [44] | 2015 | Turkey | Orthotopic heart transplant | 64 | KDIGO criteria | AKI, 34/64 (53.1%) RRT, 25/64 (39.1%) | N/A |
| Fortrie et al. [8] | 2016 | The Netherlands | Heart transplant | 531 | KDIGO criteria | AKI, 405/531 (76.3%) RRT, 25/531 (4.7%) | Hospital mortality AKI, 28/405 (6.9%) RRT, 5/25 (20.0%) 1-year mortality AKI, 41/405 (10.12%) RRT, 7/25 (28.0%) |
| Tjahjono et al. [20] | 2016 | Australia | Orthotopic heart transplant | 111 | RIFLE criteria | AKI, 65/111 (58.6%) RRT, 38/111 (34.2%) | AKI, 15/65 (23.1%) |
| Schiferer et al. [45] | 2016 | Austria | Heart transplant | 346 | RIFLE criteria | AKI RIFLE, 76/346 (22.0%) RRT, 54/346 (15.6%) | 1-year mortality RIFLE AKI, 19/76 (25.00%) RRT, 20/54 (37.0%) |
| Nadkarni et al. [46] | 2017 | USA | Orthotopic heart transplant from the Nationwide Inpatient Sample database during 2002–2013 | 130,143 | RRT | RRT, 2776/130,143 (2.1%) | N/A |
| Giglio Canelhas de Abreu et al. [47] | 2017 | Brazil | Heart transplant | 103 | AKIN criteria | AKI, 50/103 (48.5%) | AKI, 16/50 (32%) |
| Sun et al. [48] | 2018 | USA | Patients with preexisting LVADs who underwent orthotopic heart transplantation | 74 | RIFLE criteria | AKI, 18/74 (24.3%) | N/A |
| Romeo et al. [19] | 2018 | Argentina | Heart transplant | 112 | KDIGO criteria | AKI, 81/112 (72.3%) RRT, 27/112 (24.1%) | Hospital mortality AKI, 16/81 (19.8%) RRT, 14/27 (51.9%) 1-year mortality AKI, 19/81 (23.5%) RRT, 16/27 (59.3%) |
| Gašparović et al. [49] | 2018 | Croatia | Heart transplant | 158 | RRT | RRT, 27/158 (17.1%) | 3-month mortality RRT 17/27 (63.0%) |
| Sikma et al. [50] | 2018 | The Netherlands | Heart transplant | 110 | KDIGO criteria | AKI, 63/110 (57.3%) RRT, 7/110 (6.4%) | N/A |
| Ivey-Miranda et al. [51] | 2018 | Mexico | Heart transplant | 106 | RRT | RRT, 21/106 (19.81%) | N/A |
| Jahangirifard et al. [52] | 2018 | Iran | Heart transplant | 53 | AKIN criteria | AKI, 10/53 (18.87%) | N/A |
| Guven et al. [53] | 2018 | The Netherlands | Heart transplant | 595 | KDIGO criteria | AKI, 430/595 (72.3%) RRT, 41/595 (6.9%) | Hospital mortality AKI, 32/430 (7.4%) 1-year mortality AKI, 43/430 (10.0%) RRT, 9/41 (22.0%) |
| García-Gigorro et al. [18] | 2018 | Spain | Heart transplant | 310 | KDIGO criteria | AKI, 125/310 (40.3%) RRT, 32/310 (10.3%) | Hospital mortality AKI, 20/125 (16%) RRT, 15/32 (46.9%) |
| Study | Year | OR for Mortality | Confounder Adjustment |
|---|---|---|---|
| Ouseph et al. [31] | 1998 | 1-year mortality RRT: 16.67 (2.86–97.09) | None |
| Steven et al. [33] | 2004 | 0/6 in RRT vs 5/50 (10%) in non-RRT | None |
| Wyatt et al. [34] | 2004 | Hospital mortality AKI, 3.97 (0.95–16.48) RRT, 8.96 (1.75–45.80) | Age, sex, race, DM, transplant center |
| Odim et al. [35] | 2006 | Hospital mortality RRT, 17.59 (9.43–32.80) | None |
| Boyle et al. [36] | 2006 | Hospital mortality RRT, 70.20 (29.71–165.82) | None |
| Escoresca Ortega et al. [37] | 2010 | AKI, 1.70 (0.46–6.34) RRT, 3.39 (0.94–12.17) | None |
| De Santo et al. [39] | 2011 | Hospital mortality AKI, 11.25 (2.81–45.04) 1-year mortality AKI, 4.25 (1.41–12.79) | Preoperative GFR, infection, graft failure |
| Arnaoutakis et al. [40] | 2012 | 90-day mortality RRT, 14.51 (8.84–23.82) | None |
| Türker et al. [41] | 2013 | AKI, 1.56 (0.34–7.06) | None |
| Crudele et al. [42] | 2013 | Mortality AKI, 3.597 (0.95–13.62) | Recipient age, troponin, reoperation, ischemia duration, HLA mismatch |
| Fortrie et al. [8] | 2016 | Hospital mortality AKI, 2.27 (0.78–6.59) RRT, 4.43 (1.54–12.70) 1-year mortality AKI, 2.25 (0.93–5.44) RRT, 2.75 (1.13–6.63) | Age, urgency status on waiting list, RV failure, reoperation, primary graft failure, other transplant complications |
| Tjahjono et al. [20] | 2016 | AKI, 3.15 (0.97–10.22) | None |
| Schiferer et al. [45] | 2016 | 1-year mortality RIFLE AKI, 1.86 (1.01–3.45) RRT, 3.71 (1.94–7.07) | None |
| Hošková et al. [23] | 2016 | 30-day mortality AKI, 4.72 (0.75–29.76) 1-year mortality AKI, 1.52 (0.42–5.46) | None |
| Giglio Canelhas de Abreu et al. [47] | 2017 | AKI, 2.83 (0.91–8.78) | Hemoglobin, creatinine, intubation duration, INTERMACS score |
| Romeo et al. [19] | 2018 | Hospital mortality 16/81 in AKI vs 0/31 in no AKI RRT, 44.69 (9.09–219.77) 1-year mortality AKI, 4.44 (0.97–20.36) RRT, 6.79 (2.25–20.52) | Age, diabetes, bypass time |
| Gašparović et al. [49] | 2018 | 3-month mortality RRT, 42.84 (13.07–140.39) | None |
| Guven et al. [53] | 2018 | Hospital mortality AKI, 3.24 (1.13–9.30) 1-year mortality AKI, 2.1806 (1.00–4.74) RRT, 2.82 (1.28–6.24) | None |
| García-Gigorro et al. [18] | 2018 | Hospital mortality AKI, 4.84 (1.98–11.84) RRT, 11.03 (4.08–29.8) | Acute right ventricular failure, primary graft failure |
| Risk Factors for AKI |
|---|
Preoperative risk factors
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Lertjitbanjong, P.; Hansrivijit, P.; Crisafio, A.; Mao, M.A.; Watthanasuntorn, K.; Aeddula, N.R.; Bathini, T.; Kaewput, W.; Cheungpasitporn, W. Acute Kidney Injury in Patients Undergoing Cardiac Transplantation: A Meta-Analysis. Medicines 2019, 6, 108. https://doi.org/10.3390/medicines6040108
Thongprayoon C, Lertjitbanjong P, Hansrivijit P, Crisafio A, Mao MA, Watthanasuntorn K, Aeddula NR, Bathini T, Kaewput W, Cheungpasitporn W. Acute Kidney Injury in Patients Undergoing Cardiac Transplantation: A Meta-Analysis. Medicines. 2019; 6(4):108. https://doi.org/10.3390/medicines6040108
Chicago/Turabian StyleThongprayoon, Charat, Ploypin Lertjitbanjong, Panupong Hansrivijit, Anthony Crisafio, Michael A. Mao, Kanramon Watthanasuntorn, Narothama Reddy Aeddula, Tarun Bathini, Wisit Kaewput, and Wisit Cheungpasitporn. 2019. "Acute Kidney Injury in Patients Undergoing Cardiac Transplantation: A Meta-Analysis" Medicines 6, no. 4: 108. https://doi.org/10.3390/medicines6040108