
Patient Co-Creation Initiatives in the Ambulatory Care Setting during COVID-19: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
[(“ambulatory care” OR “outpatient care” OR “outpatient services” OR “urgent care” OR “clinic visit*”) AND (“cocreation” OR co-creation” OR “collaborative” OR “collaboration” OR “shared creation” OR “participation” OR “participative”)]
2.1. Inclusion Process
2.2. Exclusion Process
3. Results
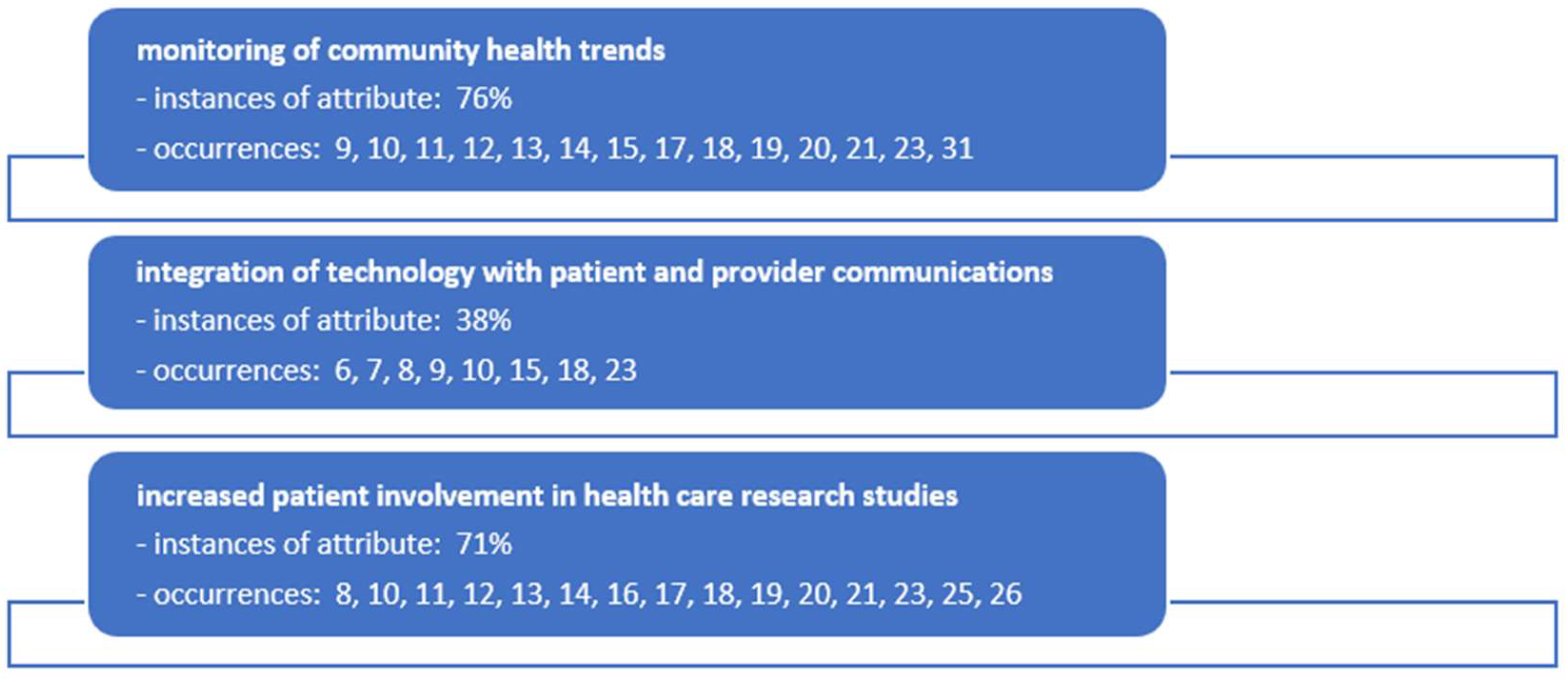
4. Discussion
4.1. Monitoring of Community Health Trends
4.2. Integrating Technology in Patient/Provider Communications
4.3. Patient Involvement in Healthcare Research Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhalla, G. Collaboration and Co-Creation: New Platforms for Marketing and Innovation; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Toni, M. The Digital Healthcare Revolution: Towards Patient Centricity with Digitization, Service Innovation and Value Co-Creation; Mattia, G., Ed.; Palgrave Macmillan: London, UK, 2022. [Google Scholar]
- Fusco, F.; Marsilio, M.; Guglielmetti, C. Co-creation in healthcare: Framing the outcomes and their determinants. J. Serv. Manag. 2023, 34, 1–26. [Google Scholar] [CrossRef]
- Mathialagan, R.; Kuthambalayan, T.S. Sustainable value co-creation in healthcare systems in the context of reduced ease of access. J. Clean. Prod. 2023, 422, 5263. [Google Scholar] [CrossRef]
- Needham, C.; Wheaton, N.; Wong Shee, A.; McNamara, K.; Malakellis, M.; Murray, M.; Alston, L.; Peeters, A.; Ugalde, A.; Huggins, C.; et al. Enhancing healthcare at home for older people in rural and regional Australia: A protocol for co-creation to design and implement system change. PLoS ONE 2023, 18, e0290386. [Google Scholar] [CrossRef] [PubMed]
- Poot, C.C.; Meijer, E.; Bruil, A.; Venema, M.; Vegt, N.J.H.; Donkel, N.; van Noort, V.; Chavannes, N.H.; Roest, A.A.W. How to use participatory design to develop an eHealth intervention to reduce preprocedural stress and anxiety among children visiting the hospital: The Hospital Hero app multi-study and pilot report. Front. Pediatr. 2023, 11, 1132639. [Google Scholar] [CrossRef] [PubMed]
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 5: Co-creative qualitative approaches for emerging themes in primary care research: Experience-based co-design, user-centred design and community-based participatory research. Eur. J. Gen. Pract. 2022, 28, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.; Wouters, E.; van Olmen, J.; Ketis, Z.K.; Chhim, S.; Chham, S.; Buffel, V.; Danhieux, K.; Stojnic, N.; Zavrnik, C.; et al. Process evaluation of the scale-up of integrated diabetes and hypertension care in Belgium, Cambodia and Slovenia (the SCUBY Project): A study protocol. BMJ Open 2022, 12, e062151. [Google Scholar] [CrossRef] [PubMed]
- Samper-Pardo, M.; Leon-Herrera, S.; Olivan-Blazquez, B.; Benede-Azagra, B.; Magallon-Botaya, R.; Gomez-Soria, I.; Calatayud, E.; Aguilar-Latorre, A.; Mendez-Lopez, F.; Perez-Palomares, S.; et al. Development and Validation of a Mobile Application as an Adjuvant Treatment for People Diagnosed with Long COVID-19: Protocol for a Co-Creation Study of a Health Asset and an Analysis of Its Effectiveness and Cost-Effectiveness. Int. J. Environ. Res. Public Health 2023, 20, 462. [Google Scholar] [CrossRef] [PubMed]
- Enam, A.; Dreyer, H.C.; De Boer, L. Impact of distance monitoring service in managing healthcare demand: A case study through the lens of cocreation. BMC Health Serv. Res. 2022, 22, 802. [Google Scholar] [CrossRef]
- Marshall-McKenna, R.; Kotronoulas, G.; Kokoroskos, E.; Granados, A.G.; Papachristou, P.; Papachristou, N.; Collantes, G.; Petridis, G.; Billis, A.; Bamidis, P.D. A multinational investigation of healthcare needs, preferences, and expectations in supportive cancer care: Co-creating the LifeChamps digital platform. J. Cancer Surviv. Res. Pract. 2023, 17, 1094–1110. [Google Scholar] [CrossRef]
- Sha, Y.; Li, C.; Xiong, Y.; Hazra, A.; Lio, J.; Jiang, I.; Huang, H.; Kerman, J.; Molina, J.; Li, L.; et al. Co-creation using crowdsourcing to promote PrEP adherence in China: Study protocol for a stepped-wedge randomized controlled trial. BMC Public Health 2022, 22, 1697. [Google Scholar] [CrossRef]
- Wormdahl, I.; Hatling, T.; Husum, T.L.; Kjus, S.H.H.; Rugkåsa, J.; Brodersen, D.; Christensen, S.D.; Nyborg, P.S.; Skolseng, T.B.; Ødegård, E.I.; et al. The ReCoN intervention: A co-created comprehensive intervention for primary mental health care aiming to prevent involuntary admissions. BMC Health Serv. Res. 2022, 22, 931. [Google Scholar] [CrossRef] [PubMed]
- Muller, S.H.A.; Kalkman, S.; van Thiel, G.J.M.W.; Mostert, M.; van Delden, J.J.M. The social license for data-intensive health research: Towards co-creation, public value and trust. BMC Med. Ethics 2021, 22, 110. [Google Scholar] [CrossRef]
- van Rooijen, M.; van Dijk-de Vries, A.; Lenzen, S.; Dalemans, R.; Moser, A.; Beurskens, A. How to foster successful implementation of a patient reported experience measurement in the disability sector: An example of developing strategies in co-creation. Res. Involv. Engagem. 2021, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Hussey, A.J.; Sibbald, S.L.; Ferrone, M.; Hergott, A.; McKelvie, R.; Faulds, C.; Roberts, Z.; Scarffe, A.D.; Meyer, M.J.; Vollbrecht, S.; et al. Confronting complexity and supporting transformation through health systems mapping: A case study. BMC Health Serv. Res. 2021, 21, 1146. [Google Scholar] [CrossRef] [PubMed]
- van Weel Baumgarten, E.; Benson, J.; Hoshi, G.; Hurle, C.; Mendive, J.; Dowrick, C.; Kassai, R. Co-creation and collaboration: A promising approach towards successful implementation. Experience from an integrated communication and mental health skills training programme for Japanese General Practice. Patient Educ. Couns. 2021, 104, 2386–2392. [Google Scholar] [CrossRef] [PubMed]
- Kovach, K.A.; Peterson, R.; Bharati, R.; Istas, K.; Monroe, M. Co-creating opportunities to incorporate cessation for electronic nicotine delivery systems in family medicine—A qualitative program evaluation. BMC Fam. Pract. 2021, 22, 169. [Google Scholar] [CrossRef] [PubMed]
- Froeling, F.; Gignac, F.; Hoek, G.; Vermeulen, R.; Nieuwenhuijsen, M.; Ficorilli, A.; De Marchi, B.; Biggeri, A.; Kocman, D.; Robinson, J.A.; et al. Narrative review of citizen science in environmental epidemiology: Setting the stage for co-created research projects in environmental epidemiology. Environ. Int. 2021, 152, 106470. [Google Scholar] [CrossRef]
- Lazo-Porras, M.; Perez-Leon, S.; Cardenas, M.K.; Pesantes, M.A.; Miranda, J.J.; Suggs, L.S.; Chappuis, F.; Perel, P.; Beran, D. Lessons learned about co-creation: Developing a complex intervention in rural Peru. Glob. Health Action 2020, 13, 1754016. [Google Scholar] [CrossRef]
- van der Boog, P.J.M.; van Dijk, S.; Navis, G.J.; Humalda, J.K.; Klaassen, G.; Meuleman, Y.; Verschuur, L.C.; Straathof, E.J.M.; Blanson Henkemans, O.A.; Bos, W.J.W.; et al. A Self-management Approach for Dietary Sodium Restriction in Patients With CKD: A Randomized Controlled Trial. Am. J. Kidney Dis. 2020, 75, 847–856. [Google Scholar]
- Nilsen, E.R.; Stendal, K.; Gullslett, M.K. Implementation of eHealth Technology in Community Health Care: The complexity of stakeholder involvement. BMC Health Serv. Res. 2020, 20, 395. [Google Scholar] [CrossRef]
- Verloo, H.; Lorette, A.; Gomes da Rocha, C.; Rosselet Amoussou, J.; Gillès de Pélichy, E.; Matos Queiros, A.; Mendez Rubio, M.; von Gunten, A. A Comprehensive Scoping Review Protocol of Using Living Labs to Explore Needs and Solutions for Older Adults with Dementia. Smart Homecare Technol. TeleHealth 2020, 7, 19–27. [Google Scholar] [CrossRef]
- Pel-Littel, R.E.; van Weert, J.C.M.; Minkman, M.M.; Reimer, W.J.M.S.O.; van de Pol, M.H.; Buurman, B.M. The development of the evidence-based SDMMCC intervention to improve shared decision making in geriatric outpatients: The DICO study. BMC Med. Inform. Decis. Mak. 2020, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.; Horseman, Z.; Fawcett, T.; Hockley, J.; Rhynas, S. Care home nursing: Co-creating curricular content with student nurses. Nurse Educ. Today 2020, 84, 104233. [Google Scholar] [CrossRef] [PubMed]
- Andfossen, N.B. Co-production between long-term care units and voluntary organisations in Norwegian municipalities: A theoretical discussion and empirical analysis. Prim. Health Care Res. Dev. 2020, 21, e33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Article Assignment | Reviewer 1 | Reviewer 2 | Reviewer 3 | Reviewer 4 | Reviewer 5 | Reviewer 6 | Reviewer 7 | Reviewer 8 | Reviewer 9 |
|---|---|---|---|---|---|---|---|---|---|
| Articles 1–10 | X | X | X | X | X | X | |||
| Articles 11–21 | X | X | X | X | X | X | X | X |
| Reference Number and Authors(s)/Year | Article Title | Journal/Publication | Participant/Population and Location | Purpose/Method | Co-Creation Outcome/Observation |
|---|---|---|---|---|---|
| [6] Poot et al., 2023 | How to use participatory design to develop an eHealth intervention to reduce preprocedural stress and anxiety among children visiting the hospital: The Hospital Hero app multi-study and pilot report | Frontiers in Pediatrics |
|
|
|
| [7] Moser and Korstjens, 2022 | Series: Practical guidance to qualitative research. Part 5: Co-creative qualitative approaches for emerging themes in primary care research: Experience-based co-design, user-centered design and community-based participatory research | The European Journal of General Practice |
|
|
|
| [8] Martens et al., 2022 | Practical guidance to qualitative research. Part 5: Co-creative qualitative approaches for emerging themes in primary care research: Experience-based co-design, user-centered design and community-based participatory research | BMJ Open |
|
|
|
| [9] Samper-Pardo et al., 2023 | Development and Validation of a Mobile Application as an Adjuvant Treatment for People Diagnosed with Long COVID-19: Protocol for a Co-Creation Study of a Health Asset and an Analysis of Its Effectiveness and Cost-Effectiveness | International Journal of Environmental Mental Research and Public Health |
|
|
|
| [10] Enam et al., 2022 | Impact of distance monitoring service in managing healthcare demand: a case study through the lens of cocreation | BMC Health Services Research |
|
|
|
| [11] Marshall-McKenna et al., 2023 | A multinational investigation of healthcare needs, preferences, and expectations in supportive cancer care: co-creating the LifeChamps digital platform | Journal of Cancer Survivorship: Research and Practice |
|
|
|
| [12] Sha et al., 2022 | Co-creation using crowdsourcing to promote PrEP adherence in China: study protocol for a stepped-wedge randomized controlled trial | BMC Public Health |
|
|
|
| [13] Wormdahl et al., 2022 | The ReCoN intervention: a co-created comprehensive intervention for primary mental health care aiming to prevent in-voluntary admissions | BMC Health Services Research |
|
|
|
| [14] Muller et al., 2021 | The social license for data-intensive health research: towards co-creation, public value and trust | BMC Medical Ethics |
|
|
|
| [15] van Rooijen et al., 2021 | How to foster successful implementation of a patient reported experience measurement in the disability sector: an example of developing strategies in co-creation | Research Involvement and Engagement |
|
|
|
| [16] Hussey et al., 2021 | Confronting complexity and supporting transformation through health systems mapping: a case study | BMC Health Services Research |
|
|
|
| [17] van Weel Baumgarten et al., 2021 | Co-creation and collaboration: a promising approach towards successful implementation. Experience from an integrated communication and mental health skills training programme for Japanese General Practice | Patient Education and Counseling |
|
|
|
| [18] Kovach et al., 2021 | Co-creating opportunities to incorporate cessation for electronic nicotine delivery systems in family medicine—a qualitative program evaluation | BMC Family Practice |
|
|
|
| [19] Froeling et al., 2021 | Narrative review of citizen science in environmental epidemiology: Setting the stage for co-created research projects in environmental epidemiology | Environment International |
|
|
|
| [20] Lazo-Porras et al., 2020 | Lessons learned about co-creation: developing a complex intervention in rural Peru | Global Health Action |
|
|
|
| [21] van der Boog et al., 2020 | A Self-management Approach for Dietary Sodium Restriction in Patients With CKD: A Randomized Controlled Trial | American Journal of Kidney Diseases |
|
|
|
| [22] Nilsen et al., 2020 | Implementation of eHealth Technology in Community Health Care: the complexity of stakeholder involvement | BMC Health Services Research |
|
|
|
| [23] Verloo et al., 2020 | A Comprehensive Scoping Review Protocol of Using Living Labs to Explore Needs and Solutions for Older Adults with Dementia. Smart Homecare | Technology and TeleHealth |
|
|
|
| [24] Pel-Littel et al., 2020 | The development of the evidence based SDMMCC intervention to improve shared decision making in geriatric outpatients: the DICO study | BMC Medical Informatics and Decision Making |
|
|
|
| [25] Watson et al., 2020 | Care home nursing: Co-creating curricular content with student nurses | Nurse Education Today |
|
|
|
| [26] Andfossen, 2020 | Co-production between long-term care units and voluntary organizations in Norwegian municipalities: A theoretical discussion and empirical analysis | Primary Health Care Research and Development |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lieneck, C.; Pacheco, G.; Cole, M.; Hipp, L.; Leal, G.; Matamoros, K.; Rojas-Trejo, B.; Stepp, N.; Torres, C. Patient Co-Creation Initiatives in the Ambulatory Care Setting during COVID-19: A Systematic Review. Medicina 2024, 60, 111. https://doi.org/10.3390/medicina60010111
Lieneck C, Pacheco G, Cole M, Hipp L, Leal G, Matamoros K, Rojas-Trejo B, Stepp N, Torres C. Patient Co-Creation Initiatives in the Ambulatory Care Setting during COVID-19: A Systematic Review. Medicina. 2024; 60(1):111. https://doi.org/10.3390/medicina60010111
Chicago/Turabian StyleLieneck, Cristian, Gerardo Pacheco, Mallory Cole, Liberty Hipp, Gabbie Leal, Kevin Matamoros, Brianna Rojas-Trejo, Nysa Stepp, and Christian Torres. 2024. "Patient Co-Creation Initiatives in the Ambulatory Care Setting during COVID-19: A Systematic Review" Medicina 60, no. 1: 111. https://doi.org/10.3390/medicina60010111