
Orthopedic Surgeons’ Accuracy When Orienting an Acetabular Cup. A Comparison with Untrained Individuals

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
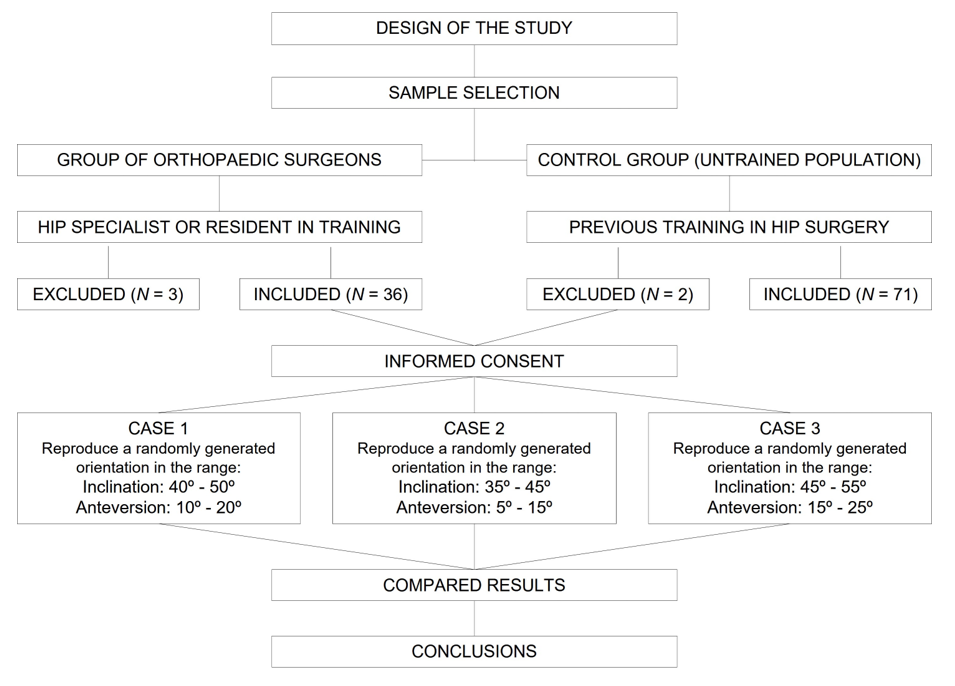
2.1. Study Design and Participants
- Orthopedic surgeons (n = 36): The subjects from this group were recruited among the participants in the 2021 National Congress of the Spanish Hip Society (SECCA). They were all specialist hip surgeons or residents in training. To facilitate a segmented analysis, participants were categorized according to their professional status (resident, specialist or head of department) and experience (number of hip surgeries performed in one year).
- Volunteers with no medical training (n = 71): Subjects were recruited among the staff of a medical device distributing company (MBA SURGICAL EMPOWERMENT, Gijón, Spain), as performed by Silberberg et al. [37]. Anybody who, on account of their position, had previous training in the field of hip surgery was excluded from participating in the study.

2.2. Measurement System
2.3. Anatomical Model and Set-Up
2.4. Procedure and Tests Carried Out
- Case 1: inclination between 40 and 50 degrees, anteversion between 10 and 20 degrees.
- Case 2: inclination between 35 and 45 degrees; anteversion between 5 and 15 degrees.
- Case 3: inclination between 45 and 55 degrees; anteversion between 15 and 25 degrees.
2.5. Measurement Error
2.6. Statistical Analysis and Software Used
3. Results
3.1. Description of the Sample
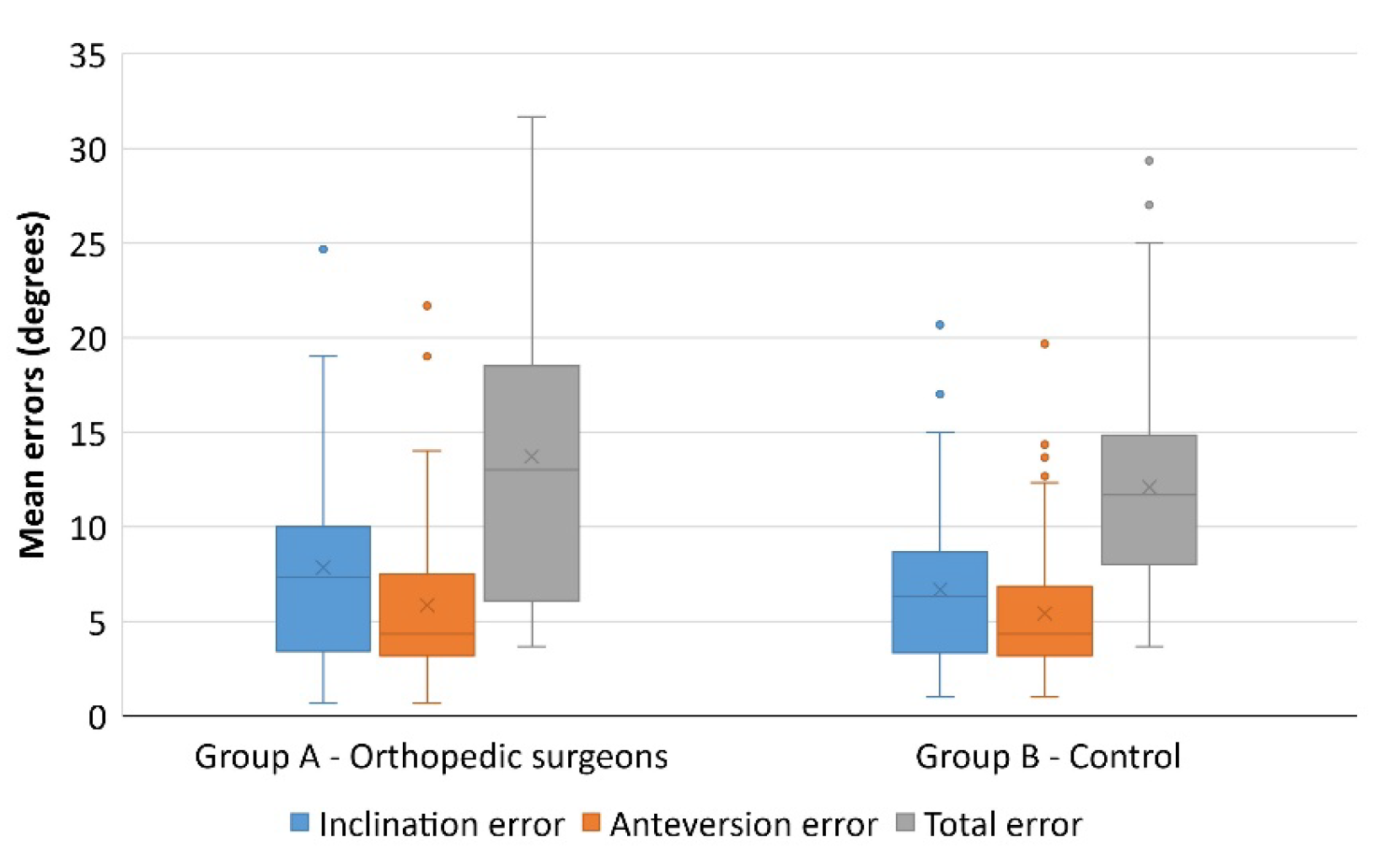
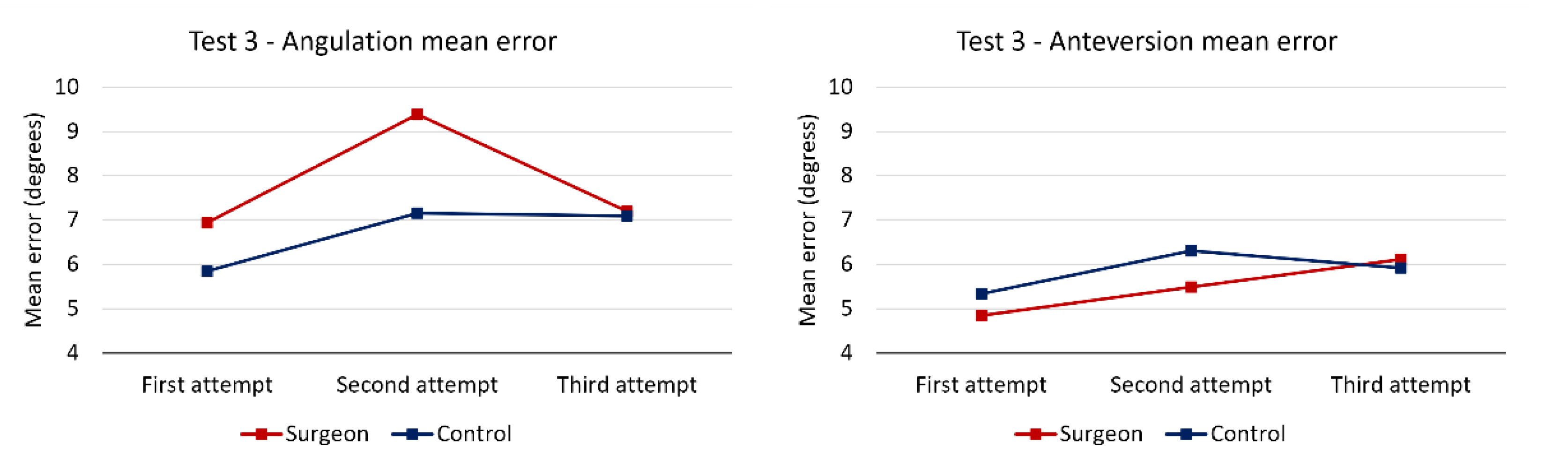
3.2. Results of the test: Positioning of the Acetabular Cup according to the Proposed Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, D.; Royle, M.; Norton, M. Metal-on-Metal Hip Resurfacing. The Effect of Cup Position and Component Size on Range of Motion to Impingement. J. Arthroplast. 2009, 24, 144–151. [Google Scholar] [CrossRef] [PubMed]
- D’lima, D.D.; Urquhart, A.G.; Buehler, K.O.; Walker, R.H.; Colwell, C.W. The Effect of the Orientation of the Acetabular and Femoral Components on the Range of Motion of the Hip at Different Head-Neck Ratios. J. Bone Jt. Surg. Am. 2000, 82, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Kummer, F.J.; Shah, S.; Iyer, S.; DiCesare, P.E. The Effect of Acetabular Cup Orientations on Limiting Hip Rotation. J. Arthroplast. 1999, 14, 509–513. [Google Scholar] [CrossRef]
- Biedermann, R.; Tonin, A.; Krismer, M.; Rachbauer, F.; Eibl, G.; Stöckl, B. Reducing the Risk of Dislocation after Total Hip Arthroplasty: The Effect of Orientation of the Acetabular Component. J. Bone Jt. Surg. Br. 2005, 87, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after Total Hip-Replacement Arthroplasties. J. Bone Jt. Surg. Am. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Kennedy, J.G.; Rogers, W.B.; Soffe, K.E.; Sullivan, R.J.; Griffen, D.G.; Sheehan, L.J. Effect of Acetabular Component Orientation on Recurrent Dislocation, Pelvic Osteolysis, Polyethylene Wear, and Component Migration. J. Arthroplast. 1998, 13, 530–534. [Google Scholar] [CrossRef]
- McCollum, D.E.; Gray, W.J. Dislocation after Total Hip Arthroplasty. Causes and Prevention. Clin. Orthop. Relat. Res. 1990, 261, 159–170. [Google Scholar] [CrossRef]
- Elkins, J.M.; Callaghan, J.J.; Brown, T.D. The 2014 Frank Stinchfield Award: The ‘Landing Zone’ for Wear and Stability in Total Hip Arthroplasty Is Smaller Than We Thought: A Computational Analysis. Clin. Orthop. Relat. Res. 2015, 473, 441–452. [Google Scholar] [CrossRef] [Green Version]
- Herrando, L.E. Inestabilidad de La Artroplastia Total de Cadera. Univ. Zaragoza 2015, 59, 287–294. [Google Scholar]
- Langton, D.J.; Joyce, T.J.; Jameson, S.S.; Lord, J.; Van Orsouw, M.; Holland, J.P.; Nargol, A.V.F.; De Smet, K.A. Adverse Reaction to Metal Debris Following Hip Resurfacing: The Influence of Component Type, Orientation and Volumetric Wear. J. Bone Jt. Surg. Br. 2011, 93, 164–171. [Google Scholar] [CrossRef]
- Patil, S.; Bergula, A.; Chen, P.C.; Colwell, C.W.; D’lima, D.D. Polyethylene Wear and Acetabular Component Orientation. J. Bone Jt. Surg. Am. 2003, 85, 56–63. [Google Scholar] [CrossRef]
- Little, N.J.; Busch, C.A.; Gallagher, J.A.; Rorabeck, C.H.; Bourne, R.B. Acetabular Polyethylene Wear and Acetabular Inclination and Femoral Offset. Clin. Orthop. Relat. Res. 2009, 467, 2895–2900. [Google Scholar] [CrossRef] [Green Version]
- Grammatopoulos, G.; Thomas, G.E.R.; Pandit, H.; Beard, D.J.; Gill, H.S.; Murray, D.W. The Effect of Orientation of the Acetabular Component on Outcome Following Total Hip Arthroplasty with Small Diameter Hard-on-Soft Bearings. Bone Jt. J. 2015, 97, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef]
- Pierrepont, J.W.; Feyen, H.; Miles, B.P.; Young, D.A.; Baré, J.V.; Shimmin, A.J. Functional Orientation of the Acetabular Component in Ceramic-on-Ceramic Total Hip Arthroplasty and Its Relevance to Squeaking. Bone Jt. J. 2016, 98, 910–916. [Google Scholar] [CrossRef]
- Sexton, S.A.; Yeung, E.; Jackson, M.P.; Rajaratnam, S.; Martell, J.M.; Walter, W.L.; Zicat, B.A.; Walter, W.K. The Role of Patient Factors and Implant Position in Squeaking of Ceramic-on-Ceramic Total Hip Replacements. J. Bone Jt. Surg. Br. 2011, 93, 439–442. [Google Scholar] [CrossRef] [Green Version]
- Walter, W.L.; O’Toole, G.C.; Walter, W.K.; Ellis, A.; Zicat, B.A. Squeaking in Ceramic-on-Ceramic Hips. J. Arthroplast. 2007, 22, 496–503. [Google Scholar] [CrossRef]
- Grammatopoulos, G.; Pandit, H.; Glyn-Jones, S.; McLardy-Smith, P.; Gundle, R.; Whitwell, D.; Gill, H.S.; Murray, D.W. Optimal Acetabular Orientation for Hip Resurfacing. J. Bone Jt. Surg. Br. 2010, 92, 1072–1078. [Google Scholar] [CrossRef] [Green Version]
- Callanan, M.C.; Jarrett, B.; Bragdon, C.R.; Zurakowski, D.; Rubash, H.E.; Freiberg, A.A.; Malchau, H. The John Charnley Award: Risk Factors for Cup Malpositioning: Quality Improvement Through a Joint Registry at a Tertiary Hospital. Clin. Orthop. Relat. Res. 2011, 469, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Bhaskar, D.; Rajpura, A.; Board, T. Current Concepts in Acetabular Positioning in Total Hip Arthroplasty. Indian J. Orthop. 2017, 51, 386. [Google Scholar] [CrossRef]
- Snijders, T.E.; Willemsen, K.; van Gaalen, S.M.; Castelein, R.M.; Weinans, H.; de Gast, A. Lack of Consensus on Optimal Acetabular Cup Orientation Because of Variation in Assessment Methods in Total Hip Arthroplasty: A Systematic Review. HIP Int. 2019, 29, 41–50. [Google Scholar] [CrossRef]
- Murray, D. The Definition and Measurement of Acetabular Orientation. J. Bone Jt. Surg. Br. 1993, 75, 228–232. [Google Scholar] [CrossRef] [Green Version]
- DiGioia, A.M.; Jaramaz, B.; Plakseychuk, A.Y.; Moody, J.E.; Nikou, C.; LaBarca, R.S.; Levison, T.J.; Picard, F. Comparison of a Mechanical Acetabular Alignment Guide with Computer Placement of the Socket. J. Arthroplast. 2002, 17, 359–364. [Google Scholar] [CrossRef]
- Minoda, Y.; Kadowaki, T.; Kim, M. Acetabular Component Orientation in 834 Total Hip Arthroplasties Using a Manual Technique. Clin. Orthop. Relat. Res. 2006, 445, 186–191. [Google Scholar] [CrossRef]
- Saxler, G.; Marx, A.; Vandevelde, D.; Langlotz, U.; Tannast, M.; Wiese, M.; Michaelis, U.; Kemper, G.; Grützner, P.A.; Steffen, R.; et al. The Accuracy of Free-Hand Cup Positioning—A CT Based Measurement of Cup Placement in 105 Total Hip Arthroplasties. Int. Orthop. 2004, 28, 198–201. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, M.; Feinberg, J.R.; Capello, W.N.; D’Antonio, J.A. The Frank Stinchfield Award: Morphologic Features of the Acetabulum and Femur: Anteversion Angle and Implant Positioning. Clin. Orthop. Relat. Res. 2001, 393, 52–65. [Google Scholar] [CrossRef]
- Ha, Y.-C.; Yoo, J.J.; Lee, Y.-K.; Kim, J.Y.; Koo, K.-H. Acetabular Component Positioning Using Anatomic Landmarks of the Acetabulum. Clin. Orthop. Relat. Res. 2012, 470, 3515–3523. [Google Scholar] [CrossRef] [Green Version]
- Archbold, H.A.P.; Mockford, B.; Molloy, D.; McConway, J.; Ogonda, L.; Beverland, D. The Transverse Acetabular Ligament: An Aid to Orientation of the Acetabular Component during Primary Total Hip Replacement. J. Bone Jt. Surg. Br. 2006, 88, 883–886. [Google Scholar] [CrossRef] [Green Version]
- Williams, H.L.M.; Bartlett, G.E.; Norton, M.R.; Middleton, R.G. The Posterior Acetabular Wall (PAW): An Aid to Acetabular Orientation at Primary THA. HIP Int. 2018, 28, 29–32. [Google Scholar] [CrossRef]
- Deep, K.; Prabhakara, A.; Mohan, D.; Mahajan, V.; Sameer, M. Orientation of Transverse Acetabular Ligament with Reference to Anterior Pelvic Plane. Arthroplast. Today 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Mihalko, W.M.; Kammerzell, S.; Saleh, K.J. Acetabular Orientation with Different Pelvic Registration Landmarks. Orthopedics 2009, 32, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Archbold, H.A.P.; Slomczykowski, M.; Crone, M.; Eckman, K.; Jaramaz, B.; Beverland, D.E. The Relationship of the Orientation of the Transverse Acetabular Ligament and Acetabular Labrum to the Suggested Safe Zones of Cup Positioning in Total Hip Arthroplasty. Hip Int. 2008, 18, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Grammatopoulos, G.; Pandit, H.G.; da Assunção, R.; McLardy-Smith, P.; De Smet, K.A.; Gill, H.S.; Murray, D.W. The Relationship between Operative and Radiographic Acetabular Component Orientation. Bone Jt. J. 2014, 96, 1290–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grammatopoulos, G.; Alvand, A.; Monk, A.P.; Mellon, S.; Pandit, H.; Rees, J.; Gill, H.S.; Murray, D.W. Surgeons’ Accuracy in Achieving Their Desired Acetabular Component Orientation. J. Bone Jt. Surg. 2016, 98, e72. [Google Scholar] [CrossRef] [Green Version]
- Van Duren, B.H.; Al Ashqar, M.; Lamb, J.N.; Pandit, H.G.; Brew, C. A Novel Mechanical Inclinometer Device to Measure Acetabular Cup Inclination in Total Hip Arthroplasty. J. Med. Eng. Technol. 2020, 44, 481–488. [Google Scholar] [CrossRef]
- Graham, D.; Suzuki, A.; Reitz, C.; Saxena, A.; Kuo, J.; Tetsworth, K. Measurement of Rotational Deformity: Using a Smartphone Application Is More Accurate than Conventional Methods. ANZ J. Surg. 2013, 83, 937–941. [Google Scholar] [CrossRef]
- Silberberg, J.M.; Nilo, A.; Roces-García, J. Enhancement of External Rotation after Latissimus Dorsi Tendon Transfer (LDTT): A Cadaveric Study. Medicina 2021, 57, 305. [Google Scholar] [CrossRef]
- Chapanis, A. Theory and Methods for Analyzing Errors in Man-Machine Systems. Ann. N. Y. Acad. Sci. 1951, 51, 1179–1203. [Google Scholar] [CrossRef]
- Schmidt, R.; Lee, T.; Carolee, W.; Wulf, G.; Zelaznik, H. Motor Control and Learning: A Behavioral Emphasis, 6th ed.; Human Kinetics: Champaign, IL, USA, 2019; ISBN 9781492547754. [Google Scholar]
- Grammatopoulos, G.; Gofton, W.; Cochran, M.; Dobransky, J.; Carli, A.; Abdelbary, H.; Gill, H.S.; Beaulé, P.E. Pelvic Positioning in the Supine Position Leads to More Consistent Orientation of the Acetabular Component after Total Hip Arthroplasty. Bone Jt. J. 2018, 100, 1280–1288. [Google Scholar] [CrossRef]
- Renner, L.; Janz, V.; Perka, C.; Wassilew, G.I. What Do We Get from Navigation in Primary THA? EFORT Open Rev. 2016, 1, 205–210. [Google Scholar] [CrossRef]
- Jacofsky, D.J.; Allen, M. Robotics in Arthroplasty: A Comprehensive Review. J. Arthroplast. 2016, 31, 2353–2363. [Google Scholar] [CrossRef]
- Miyake, J.; Murase, T.; Oka, K.; Moritomo, H.; Sugamoto, K.; Yoshikawa, H. Computer-Assisted Corrective Osteotomy for Malunited Diaphyseal Forearm Fractures. J. Bone Jt. Surg. 2012, 94, e150. [Google Scholar] [CrossRef]
- Bernstein, M.; Walsh, A.; Petit, A.; Zukor, D.J.; Antoniou, J. Femoral Head Size Does Not Affect Ion Values in Metal-on-Metal Total Hips. Clin. Orthop. Relat. Res. 2011, 469, 1642–1650. [Google Scholar] [CrossRef] [Green Version]
- Langton, D.J.; Jameson, S.S.; Joyce, T.J.; Webb, J.; Nargol, A.V.F. The Effect of Component Size and Orientation on the Concentrations of Metal Ions after Resurfacing Arthroplasty of the Hip. J. Bone Jt. Surg. Br. 2008, 90, 1143–1151. [Google Scholar] [CrossRef] [Green Version]
- Lusty, P.J.; Watson, A.; Tuke, M.A.; Walter, W.L.; Walter, W.K.; Zicat, B. Orientation and Wear of the Acetabular Component in Third Generation Alumina-on-Alumina Ceramic Bearings. J. Bone Jt. Surg. Br. 2007, 89, 1158–1164. [Google Scholar] [CrossRef]
- Zubiaur González, M. El Feedback Extrínseco en el Aprendizaje de Una Respuesta Motriz; Universidad de Salamanca: Salamanca, Spain, 1996. [Google Scholar]
- Logishetty, K.; Western, L.; Morgan, R.; Iranpour, F.; Cobb, J.P.; Auvinet, E. Can an Augmented Reality Headset Improve Accuracy of Acetabular Cup Orientation in Simulated THA? A Randomized Trial. Clin. Orthop. Relat. Res. 2019, 477, 1190–1199. [Google Scholar] [CrossRef]
- Gofton, W.; Dubrowski, A.; Tabloie, F.; Backstein, D. The Effect of Computer Navigation on Trainee Learning of Surgical Skills. J. Bone Jt. Surg. Am. 2007, 89, 2819–2827. [Google Scholar] [CrossRef]
- Snijders, T.; van Gaalen, S.M.; de Gast, A. Precision and Accuracy of Imageless Navigation versus Freehand Implantation of Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. Int. J. Med. Robot Comput. Assist. Surg. 2017, 13, e1843. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.; von Kunow, F.; Innmann, M.; Meyer, M.; Thieme, M.; Jerabek, S.; Renkawitz, T. Which Safe Zone Is Safe in Total Hip Arthroplasty? The Effect of Bony Impingement. J. Pers. Med. 2022, 12, 812. [Google Scholar] [CrossRef]
- Ishikura, H.; Nakamura, M.; Nakamura, S.; Tanaka, T.; Kawano, H.; Tanaka, S. Relationship between the Accuracy of the Acetabular Cup Angle and BMI in Posterolateral Total Hip Arthroplasty with CT-Based Navigation. Medicina 2022, 58, 856. [Google Scholar] [CrossRef]
- Zurmühle, C.A.; Zickmantel, B.; Christen, M.; Christen, B.; Zheng, G.; Schwab, J.M.; Tannast, M.; Steppacher, S.D. Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness. Medicina 2022, 58, 832. [Google Scholar] [CrossRef]
- Brady, A.W.; Tatka, J.; Fagotti, L.; Kemler, B.R.; Fossum, B.W. Accuracy and Reliability of Software Navigation for Acetabular Component Placement in THA: An In Vitro Validation Study. Medicina 2022, 58, 663. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Group A—Orthopedic Surgeons | 36 | 33.6% |
| Experience | ||
| Resident | 4 | 11.1% |
| 0–25 total hip replacements a year | 3 | 8.3% |
| 25–50 total hip replacements a year | 2 | 5.6% |
| 50–100 total hip replacements a year | 9 | 25.0% |
| More than 100 total hip replacements a year | 18 | 50.0% |
| Position | ||
| Resident | 4 | 11.1% |
| Consultant | 25 | 69.4% |
| Head of department | 7 | 19.4% |
| Group B—Control | 71 | 66.4% |
| Occupation | ||
| Clerical work | 4 | 5.6% |
| Warehousing | 14 | 19.7% |
| Customer service | 11 | 15.5% |
| Accounts | 11 | 15.5% |
| Information technology | 8 | 11.3% |
| Marketing | 8 | 11.3% |
| Logistics | 8 | 11.3% |
| Other | 7 | 9.9% |
| Total | 107 | 100% |
| Group A Surgeons | Group B Control | p-Value | |
|---|---|---|---|
| Mean age | 47.14 | 40.23 | 0.005 * |
| Sex | |||
| Males | 30 (83.3%) | 40 (56.3%) | 0.006 * |
| Females | 6 (16.7%) | 31 (43.7%) |
| Group A Surgeons | Group B Control | p-Value | |
|---|---|---|---|
| Mean error—Inclination | 7.84 (±5.53) | 6.70 (±4.03) | 0.226 |
| Mean error—Anteversion | 5.85 (±4.52) | 5.48 (±3.44) | 0.639 |
| Total mean error—Inclination + anteversion | 13.69 (±7.76) | 12.18 (±5.32) | 0.298 |
| Inclination Error | Anteversion Error | ||||
|---|---|---|---|---|---|
| N | Mean | p Value | Mean | p Value | |
| Group A—Orthopedic surgeons | |||||
| Experience-based classification (number of surgeries a year) | |||||
| Less than 100 | 18 | 8.01 | 0.852 | 5.83 | 0.981 |
| More than 100 | 18 | 7.67 | 5.87 | ||
| Seniority-based classification | |||||
| Resident | 4 | 9.00 | 0.879 | 6.67 | 0.854 |
| Consultant | 25 | 7.84 | 5.93 | ||
| Head of department | 7 | 7.19 | 5.10 | ||
| Inclination Error | Anteversion Error | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Too Horizontal | Right Inclination | Too Vertical | Less Anteversion | Right Anteversion | More Anteversion | |||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Surgeons | 84 | 77.8 | 7 | 6.5 | 17 | 15.7 | 75 | 69.4 | 6 | 5.6 | 27 | 25.0 |
| Control | 96 | 45.1 | 8 | 3.8 | 109 | 51.2 | 91 | 42.7 | 13 | 6.1 | 109 | 51.2 |
| Mean Error (Degrees) | ||||
|---|---|---|---|---|
| N | One Angle | Inclination | Anteversion | |
| Graham (2013) | 31 | 5.4 (±5.3) | - | - |
| Duren (2020) | 18 | - | 6.4 (±4.4) | - |
| Grammatopoulos (2016) | 21 | - | 5.0 (±10) | 5.0 (±15) |
| Present study | 36 | - | 7.8 (±5.5) | 5.9 (±4.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreta, J.; Gayoso, Ó.; Donaire-Hoyas, D.; Roces-García, J.; Gómez-Vallejo, J.; Moya-Gómez, E.; Raya-Roldán, D.; Albert-Ullibarri, A.; Marqués-López, F.; Albareda, J. Orthopedic Surgeons’ Accuracy When Orienting an Acetabular Cup. A Comparison with Untrained Individuals. Medicina 2022, 58, 973. https://doi.org/10.3390/medicina58070973
Moreta J, Gayoso Ó, Donaire-Hoyas D, Roces-García J, Gómez-Vallejo J, Moya-Gómez E, Raya-Roldán D, Albert-Ullibarri A, Marqués-López F, Albareda J. Orthopedic Surgeons’ Accuracy When Orienting an Acetabular Cup. A Comparison with Untrained Individuals. Medicina. 2022; 58(7):973. https://doi.org/10.3390/medicina58070973
Chicago/Turabian StyleMoreta, Jesús, Óscar Gayoso, Daniel Donaire-Hoyas, Jorge Roces-García, Jesús Gómez-Vallejo, Esther Moya-Gómez, David Raya-Roldán, Alberto Albert-Ullibarri, Fernando Marqués-López, and Jorge Albareda. 2022. "Orthopedic Surgeons’ Accuracy When Orienting an Acetabular Cup. A Comparison with Untrained Individuals" Medicina 58, no. 7: 973. https://doi.org/10.3390/medicina58070973