
Clinical Characteristics and Distribution of Pediatric Fractures at a Tertiary Hospital in Northern France: A 20-Year-Distance Comparative Analysis (1999–2019)

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
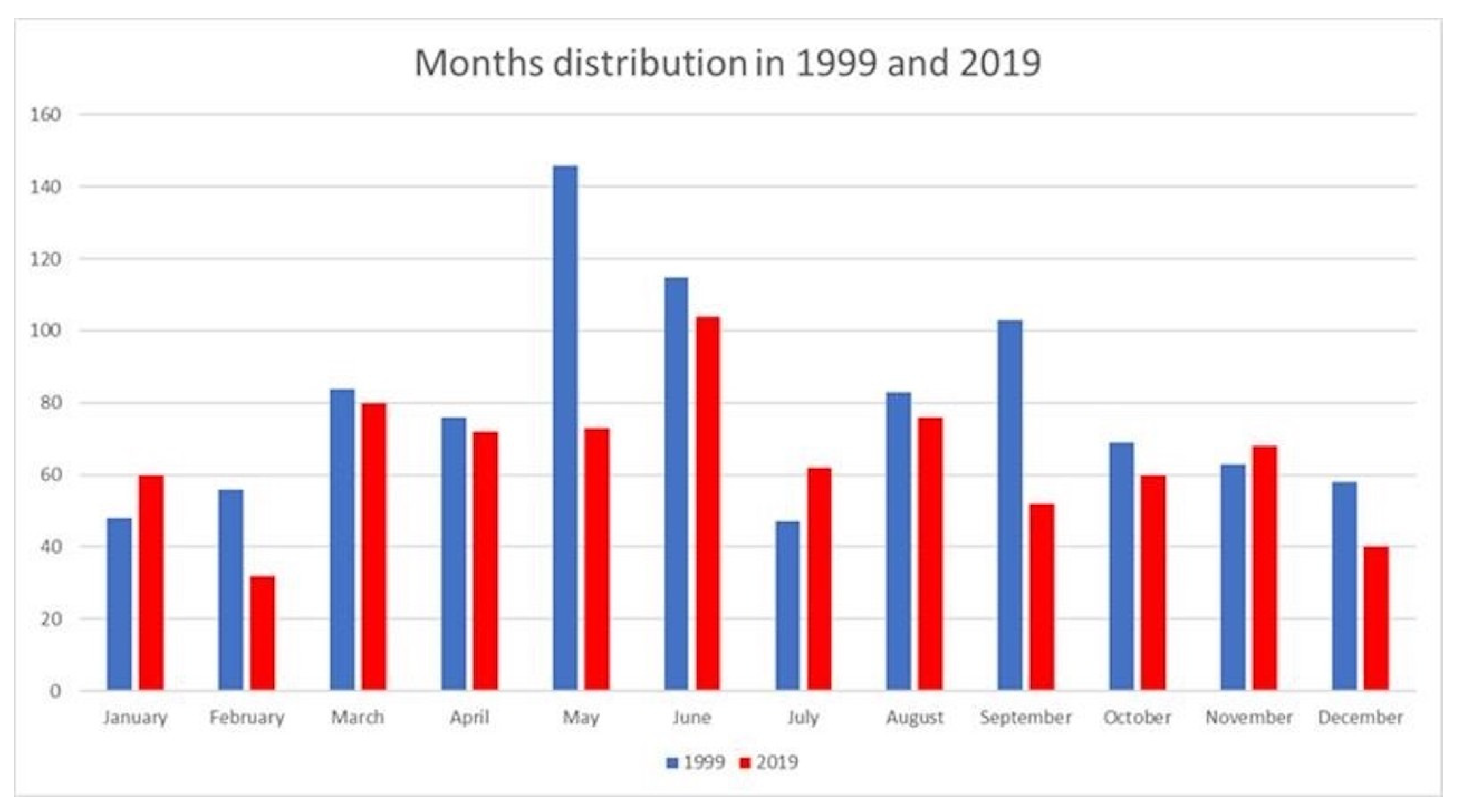
3.1. Month of Injury
3.2. Age
3.3. Mechanism of Injury
3.4. Fractures Treated Surgically
3.5. Site and Type of Fracture
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bayrak, A.; Öztürk, V.; Koluman, A.; Ziroğlu, N.; Duramaz, A. Injury characteristics and management of orthopaedic trauma in refugee children. Int. Orthop. 2021, 45, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Perkins, C.; Scannell, B.; Brighton, B.; Seymour, R.; Vanderhave, K. Orthopaedic firearm injuries in children and adolescents: An eight-year experience at a major urban trauma center. Injury 2016, 47, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Maccagnano, G.; Notarnicola, A.; Pesce, V.; Tafuri, S.; Mudoni, S.; Nappi, V.; Moretti, B. Failure Predictor Factors of Conservative Treatment in Pediatric Forearm Fractures. Biomed. Res. Int. 2018, 2018, 5930106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, E.M. The epidemiology of fractures in otherwise healthy children. Curr. Osteoporos. Rep. 2014, 12, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Castro-Lemus, N.; Romero-Blanco, C.; García-Coll, V.; Aznar, S. Gender-Differentiated Analysis of the Correlation between Active Commuting to School vs. Active Commuting to Extracurricular Physical Activity Practice during Adolescence. Int. J. Environ. Res. Public Health. 2021, 18, 5520. [Google Scholar] [CrossRef] [PubMed]
- Kuritz, A.; Mall, C.; Schnitzius, M.; Mess, F. Physical Activity and Sedentary Behavior of Children in Afterschool Programs: An Accelerometer-Based Analysis in Full-Day and Half-Day Elementary Schools in Germany. Front. Public Health 2020, 8, 463. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Wen, L.M.; Rissel, C. Associations of parental influences with physical activity and screen time among young children: A systematic review. J. Obes. 2015, 2015, 546925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Königshausen, M.; Gothner, M.; Kruppa, C.; Dudda, M.; Godry, H.; Schildhauer, T.A.; Seybold, D. Trampolinassoziierte Verletzungen im Kindesalter. Ein zunehmendes Problem [Trampoline-related injuries in children: An increasing problem]. Sportverletz Sportschaden. 2014, 28, 69–74. [Google Scholar] [PubMed]
- Beck, S.; Barker, L.; Chan, A.; Stanbridge, S. Emergency department impact following the introduction of an electric scooter sharing service. Emerg. Med. Australas. 2020, 32, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inkelis, S.H.; Stroberg, A.J.; Keller, E.L.; Christenson, P.D. Roller skating injuries in children. Pediatr. Emerg. Care 1988, 4, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Reinberg, O.; Reinberg, A.; Téhard, B.; Mechkouri, M. Accidents in children do not happen at random: Predictable time-of-day incidence of childhood trauma. Chronobiol. Int. 2002, 19, 615–631. [Google Scholar] [CrossRef] [PubMed]
- Une Croissance Démographique Régulière en Hauts-de-France, Mais des Disparités Territoriales—Insee Analyses Hauts-de-France—48 n.d. Available online: https://www.insee.fr/fr/statistiques/2664808 (accessed on 27 May 2021).
- O’Farrell, D.A.; Ridha, H.M.; Keenan, P.; McManus, F.W.; Stephens, M. An epidemic of roller-blade injuries in children. Injury 1997, 28, 377–379. [Google Scholar] [CrossRef]
- eAccueil|Sécurité Routière n.d. Available online: https://www.securite-routiere.gouv.fr/ (accessed on 1 March 2021).
- Cooper, C.; Dennison, E.M.; Leufkens, H.G.M.; Bishop, N.; van Staa, T.P. Epidemiology of childhood fractures in Britain: A study using the general practice research database. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2004, 19, 1976–1981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khosla, S.; Melton, L.J.; Dekutoski, M.B.; Achenbach, S.J.; Oberg, A.L.; Riggs, B.L. Incidence of childhood distal forearm fractures over 30 years: A population-based study. JAMA 2003, 290, 1479–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedström, E.M.; Svensson, O.; Bergström, U.; Michno, P. Epidemiology of fractures in children and adolescents. Acta Orthop. 2010, 81, 148–153. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1999 (n = 939) | 2019 (n = 781) | p-Value | ||
|---|---|---|---|---|
| Age group, n | 11–15 years | 408 (43%) | 195 (25%) | <0.001 |
| 6–10 years | 307 (33%) | 294 (38%) | <0.001 | |
| 1–5 years | 224 (24%) | 281 (36%) | <0.001 | |
| <1 years | 0 (0%) | 11 (1.4%) | <0.001 |
| 1999 (n = 939) | 2019 (n = 781) | n | ||
|---|---|---|---|---|
| Mechanism, n | Fall | 249 (27%) | 319 (41%) | 568 |
| Direct trauma | 237 (25%) | 100 (13%) | 337 | |
| Collective sports | 133 (14%) | 81 (10%) | 214 | |
| Scooter/bicycle | 125 (13%) | 80 (10%) | 205 | |
| Domicile/school/park | 114 (12%) | 20 (2.6%) | 134 (Non interpretable) | |
| Trampoline | 0 (0%) | 109 (14%) | 110 (Non interpretable) | |
| Individual sports | 20 (2.1%) | 61 (7.8%) | 81 | |
| MVA | 60 (6.4%) | 11 (1.4%) | 71 |
| 1999 (n = 138) | 2019 (n = 133) | n | ||
|---|---|---|---|---|
| Age at surgical treatment, n | 11–15 years | 62 (45%) | 41 (31%) | 103 |
| 6–10 years | 52 (38%) | 50 (38%) | 102 | |
| 1–5 years | 24 (17%) | 41 (31%) | 65 | |
| <1 year | 0 (0%) | 1 (0.75%) | 1 |
| 1999 (n = 939) | 2019 (n = 781) | n | ||
|---|---|---|---|---|
| Site, n | Forearm/wrist | 517 (55%) | 319 (41%) | 836 |
| Ankle and foot | 102 (11%) | 144 (18%) | 246 | |
| Elbow | 100 (11%) | 128 (16%) | 228 | |
| Clavicle | 74 (7.9%) | 78 (10%) | 152 | |
| Thigh and knee | 49 (5.2%) | 38 (4.9%) | 87 | |
| Leg | 52 (5.5%) | 27 (3.5%) | 79 | |
| Shoulder and arm | 30 (3.2%) | 37 (4.7%) | 67 | |
| Spine and pelvis | 10 (1.1%) | 10 (1.3%) | 20 |
| 1999 (n = 939) | 2019 (n = 781) | n | p-Value | Test | ||
|---|---|---|---|---|---|---|
| Age, mean | 8.81 (±4.12) | 7.19 (±4.00) | 1720 | <0.001 | Welch | |
| Mechanism of injury, n | Fall | 249 (27%) | 319 (41%) | 568 | <0.001 | Chi2 |
| Direct trauma | 237 (25%) | 100 (13%) | 337 | - | - | |
| Group sports | 133 (14%) | 81 (10%) | 214 | - | - | |
| Scooter/bicycle | 125 (13%) | 80 (10%) | 205 | - | - | |
| Home/school | 114 (12%) | 20 (2.6%) | 134 | - | - | |
| Trampoline and games | 1 (0.11%) | 109 (14%) | 110 | - | - | |
| Individual sports | 20 (2.1%) | 61 (7.8%) | 81 | - | - | |
| MVA | 60 (6.4%) | 11 (1.4%) | 71 | - | - | |
| Site, n | Forearm/wrist | 517 (55%) | 319 (41%) | 836 | <0.001 | Fisher |
| Ankle and foot | 102 (11%) | 144 (18%) | 246 | - | - | |
| Elbow | 100 (11%) | 128 (16%) | 228 | - | - | |
| Clavicle | 74 (7.9%) | 78 (10%) | 152 | - | - | |
| Thigh and knee | 49 (5.2%) | 38 (4.9%) | 87 | - | - | |
| Leg | 52 (5.5%) | 27 (3.5%) | 79 | - | - | |
| Shoulder and arm | 30 (3.2%) | 37 (4.7%) | 67 | - | - | |
| Spine and pelvis | 10 (1.1%) | 10 (1.3%) | 20 | - | - | |
| Elbow | 5 (0.53%) | 0 (0%) | 5 | - | - | |
| Treatment, n | Orthopedic | 801 (85%) | 648 (83%) | 1449 | 0.19 | Chi2 |
| Surgical | 138 (15%) | 133 (17%) | 271 | - | - | |
| Age group, n | 11–15 years | 408 (43%) | 195 (25%) | 603 | <0.001 | Fisher |
| 6–10 years | 307 (33%) | 294 (38%) | 601 | - | - | |
| 1–5 years | 224 (24%) | 281 (36%) | 505 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monget, F.; Sapienza, M.; McCracken, K.L.; Nectoux, E.; Fron, D.; Andreacchio, A.; Pavone, V.; Canavese, F. Clinical Characteristics and Distribution of Pediatric Fractures at a Tertiary Hospital in Northern France: A 20-Year-Distance Comparative Analysis (1999–2019). Medicina 2022, 58, 610. https://doi.org/10.3390/medicina58050610
Monget F, Sapienza M, McCracken KL, Nectoux E, Fron D, Andreacchio A, Pavone V, Canavese F. Clinical Characteristics and Distribution of Pediatric Fractures at a Tertiary Hospital in Northern France: A 20-Year-Distance Comparative Analysis (1999–2019). Medicina. 2022; 58(5):610. https://doi.org/10.3390/medicina58050610
Chicago/Turabian StyleMonget, Faustine, Marco Sapienza, Kathryn Louise McCracken, Eric Nectoux, Damien Fron, Antonio Andreacchio, Vito Pavone, and Federico Canavese. 2022. "Clinical Characteristics and Distribution of Pediatric Fractures at a Tertiary Hospital in Northern France: A 20-Year-Distance Comparative Analysis (1999–2019)" Medicina 58, no. 5: 610. https://doi.org/10.3390/medicina58050610