
Atherosclerosis Development and Progression: The Role of Atherogenic Small, Dense LDL

 , , ,
, , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
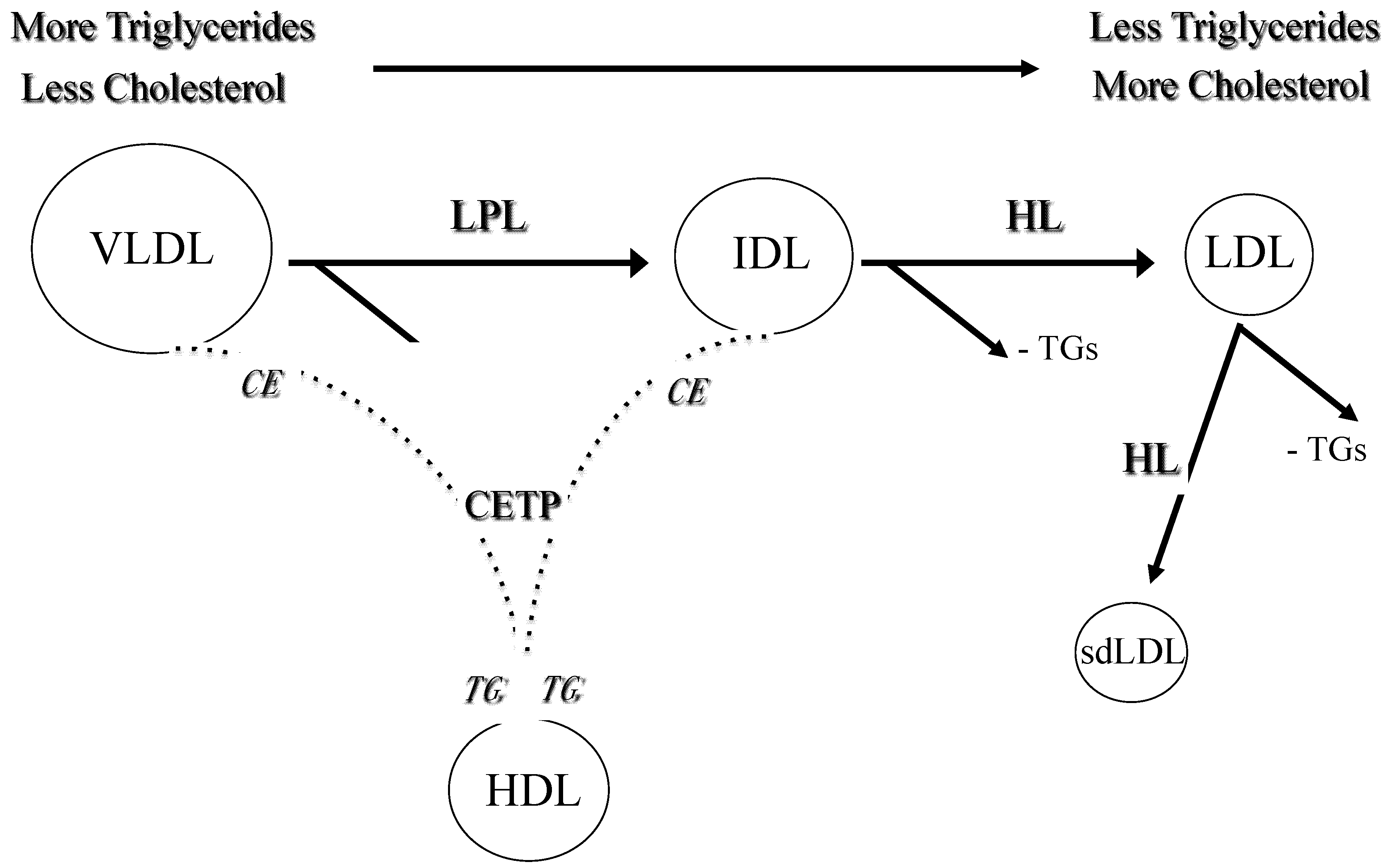
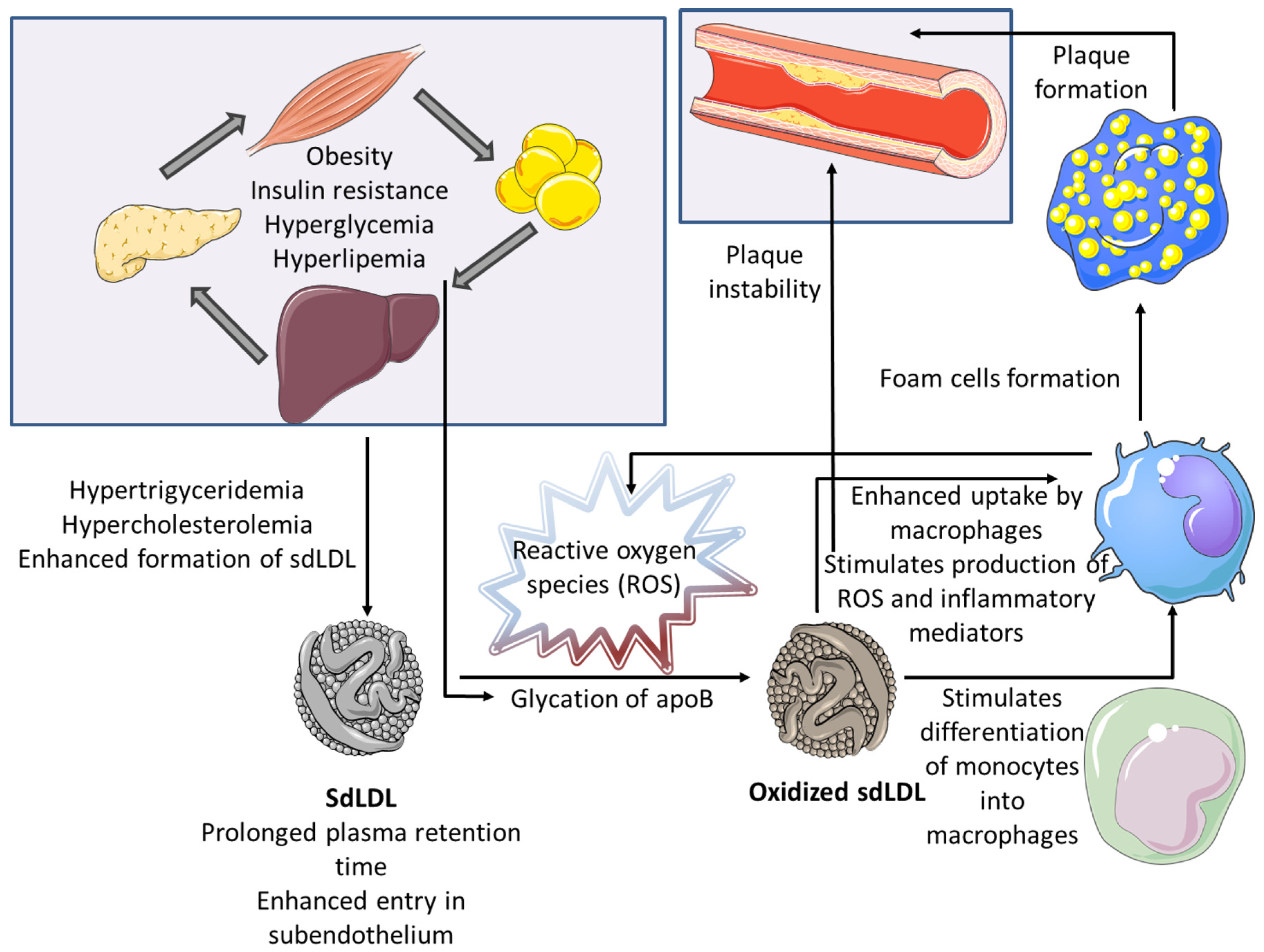
2. Formation and Progression of Atherosclerotic Plaque: The Role of Small, Dense LDL
3. Genetic and Epigenetic Factors Affecting the Formation of Small, Dense LDL
4. Atherogenic Properties of Small, Dense LDL and the Association with Cardiovascular Risk
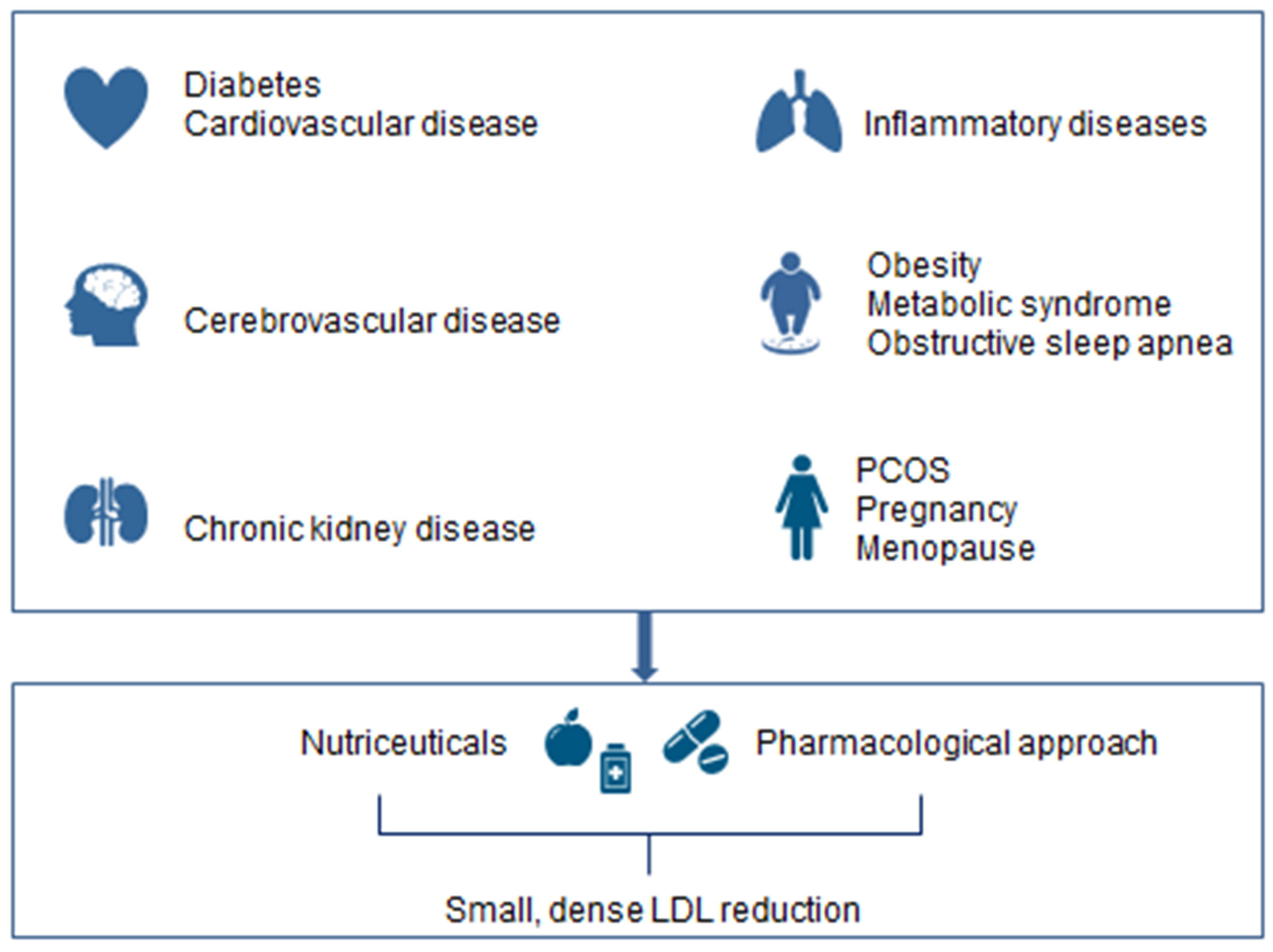
5. Small, Dense LDL in Obesity, Diabetes and Chronic Kidney Disease
6. Small, Dense LDL and Endocrine Disorders, Pregnancy and Menopause
7. Conclusions
Funding
Acknowledgments
Conflicts of Interest
Disclosures
References
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardio-vascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Berneis, K. Should we measure routinely the LDL peak particle size? Int. J. Cardiol. 2006, 107, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, A.A.; Stoian, A.P.; Janez, A.; Rizzo, M. Lipoproteins and Cardiovascular Disease: An Update on the Clinical Significance of Atherogenic Small, Dense LDL and New Therapeutical Options. Biomedicines 2021, 9, 1579. [Google Scholar] [CrossRef]
- Rizzo, M.; Kotur-Stevuljevic, J.; Berneis, K.; Spinas, G.; Rini, G.B.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V.; Vekic, J. Atherogenic dyslipidemia and oxidative stress: A new look. Transl. Res. 2009, 153, 217–223. [Google Scholar] [CrossRef]
- Vekic, J.; Kotur-Stevuljevic, J.; Jelić-Ivanović, Z.; Spasic, S.; Spasojević-Kalimanovska, V.; Topić, A.; Zeljkovic, A.; Stefanovic, A.; Žunić, G. Association of oxidative stress and PON1 with LDL and HDL particle size in middle-aged subjects. Eur. J. Clin. Investig. 2007, 37, 715–723. [Google Scholar] [CrossRef]
- Sekimoto, T.; Koba, S.; Mori, H.; Sakai, R.; Arai, T.; Yokota, Y.; Sato, S.; Tanaka, H.; Masaki, R.; Oishi, Y.; et al. Small Dense Low-Density Lipoprotein Cholesterol: A Residual Risk for Rapid Progression of Non-Culprit Coronary Lesion in Patients with Acute Coronary Syndrome. J. Atheroscler. Thromb. 2021, 28, 1161–1174. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Chisolm, G.M.; Steinberg, D. The oxidative modification hypothesis of atherogenesis: An overview. Free Radic. Biol. Med. 2000, 28, 1815–1826. [Google Scholar] [CrossRef]
- Rizzo, M.; Berneis, K.; Zeljkovic, A.; Vekic, J. Should we routinely measure low-density and high-density lipoprotein subclasses? Clin. Lab. 2009, 55, 421–429. [Google Scholar] [PubMed]
- Rizzo, M.; Berneis, K. Who needs to care about small, dense low-density lipoproteins? Int. J. Clin. Pract. 2007, 61, 1949–1956. [Google Scholar] [CrossRef] [PubMed]
- Bayram, F.; Kocer, D.; Gundogan, K.; Kaya, A.; Demir, O.; Coskun, R.; Sabuncu, T.; Karaman, A.; Cesur, M.; Rizzo, M.; et al. Prevalence of dyslipidemia and associated risk factors in Turkish adults. J. Clin. Lipidol. 2014, 8, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Krauss, R.M. Lipids and Lipoproteins in Patients with Type 2 Diabetes. Diabetes Care 2004, 27, 1496–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, M.; Rini, G.B.; Berneis, K. The clinical relevance of LDL size and subclasses modulation in patients with type-2 diabetes. Exp. Clin. Endocrinol. Diabetes 2007, 115, 477–482. [Google Scholar] [CrossRef]
- Mikhailidis, D.P.; Elisaf, M.; Rizzo, M.; Berneis, K.; Griffin, B.; Zambon, A.; Athyros, V.; De Graaf, J.; Marz, W.; Parhofer, K.G.; et al. “European Panel on Low Density Lipoprotein (LDL) Subclasses”: A Statement on the Pathophysiology, Atherogenicity and Clinical Significance of LDL Subclasses. Curr. Vasc. Pharmacol. 2011, 9, 533–571. [Google Scholar] [CrossRef]
- Goedecke, J.H.; Utzschneider, K.; Faulenbach, M.V.; Rizzo, M.; Berneis, K.; Spinas, G.A.; Dave, J.A.; Levitt, N.S.; Lambert, E.V.; Olsson, T.; et al. Ethnic differences in serum lipoproteins and their determi-nants in South African women. Metabolism 2010, 59, 1341–1350. [Google Scholar] [CrossRef]
- Crone, B.; Krause, A.M.; Hornsby, W.E.; Willer, C.J.; Surakka, I. Translating genetic association of lipid levels for biological and clinical application. Cardiovasc. Drugs Ther. 2021, 35, 617–626. [Google Scholar] [CrossRef]
- Wood, L.; Aslibekyan, S.; Absher, D.M.; Hopkins, P.N.; Sha, J.; Tsai, M.; Tiwari, H.K.; Waite, L.L.; Zhi, D.; Arnett, D.K. Methylation at CPT1A locus is associated with lipoprotein subfraction profiles. J. Lipid Res. 2014, 55, 1324–1330. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Alonso, M.D.C.; Kretschmer, A.; Wilson, R.; Pfeiffer, L.; Karhunen, V.; Seppälä, I.; Zhang, W.; Mittelstraß, K.; Wahl, S.; Matias-Garcia, P.R.; et al. DNA methylation and lipid metabolism: An EWAS of 226 metabolic measures. Clin. Epigenet. 2021, 13, 1–19. [Google Scholar] [CrossRef]
- Jhun, M.-A.; Mendelson, M.; Wilson, R.; Gondalia, R.; Joehanes, R.; Salfati, E.; Zhao, X.; Braun, K.V.E.; Do, A.N.; Hedman, Å.K.; et al. A multi-ethnic epigenome-wide association study of leukocyte DNA methylation and blood lipids. Nat. Commun. 2021, 12, 1–13. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Stefanovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V. Obesity and dyslipidemia. Metabolism 2019, 92, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Chisolm, G.M.; Chai, Y.-C. Regulation of cell growth by oxidized LDL. Free Radic. Biol. Med. 2000, 28, 1697–1707. [Google Scholar] [CrossRef]
- Abate, N.; Sallam, H.S.; Rizzo, M.; Nikolic, D.; Obradovic, M.; Bjelogrlic, P.; Isenovic, E.R. Resistin: An in-flammatory cytokine. Role in cardiovascular diseases, diabetes and the metabolic syndrome. Curr. Pharm. Des. 2014, 20, 4961–4969. [Google Scholar] [CrossRef]
- Hansson, G.K. Inflammation, Atherosclerosis, and Coronary Artery Disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farahi, L.; Sinha, S.K.; Lusis, A.J. Roles of Macrophages in Atherogenesis. Front. Pharmacol. 2021, 12, 785220. [Google Scholar] [CrossRef] [PubMed]
- Ai, M.; Otokozawa, S.; Asztalos, B.F.; Ito, Y.; Nakajima, K.; White, C.C.; Cupples, L.A.; Wilson, P.W.; Schaefer, E.J. Small Dense LDL Cholesterol and Coronary Heart Disease: Results from the Framingham Offspring Study. Clin. Chem. 2010, 56, 967–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikezaki, H.; Lim, E.; Cupples, L.A.; Liu, C.; Asztalos, B.F.; Schaefer, E.J. Small Dense Low-Density Lipoprotein Cholesterol Is the Most Atherogenic Lipoprotein Parameter in the Prospective Framingham Offspring Study. J. Am. Hear. Assoc. 2021, 10, e019140. [Google Scholar] [CrossRef]
- Duran, E.K.; Aday, A.; Cook, N.R.; Buring, J.E.; Ridker, P.M.; Pradhan, A.D. Triglyceride-Rich Lipoprotein Cholesterol, Small Dense LDL Cholesterol, and Incident Cardiovascular Disease. J. Am. Coll. Cardiol. 2020, 75, 2122–2135. [Google Scholar] [CrossRef]
- Liou, L.; Kaptoge, S. Association of small, dense LDL-cholesterol concentration and lipoprotein particle characteristics with coronary heart disease: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0241993. [Google Scholar] [CrossRef]
- Duan, R.; Xue, W.; Wang, K.; Yin, N.; Hao, H.; Chu, H.; Wang, L.; Meng, P.; Diao, L. Estimation of the LDL subclasses in ischemic stroke as a risk factor in a Chinese population. BMC Neurol. 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Liu, J.; Wang, L.; Feng, W.; Cao, Z.; Wang, P.; Liu, G.; Sun, C.; Shen, Y.; Wang, L.; et al. Association of Small Dense Low-Density Lipoprotein Cholesterol with Stroke Risk, Severity and Prognosis. J. Atheroscler. Thromb. 2020, 27, 1310–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeljkovic, A.; Vekic, J.; Spasojevic-Kalimanovska, V.; Jelic-Ivanovic, Z.; Bogavac-Stanojevic, N.; Gulan, B.; Spasic, S. LDL and HDL subclasses in acute ischemic stroke: Prediction of risk and short-term mortality. Atherosclerosis 2010, 210, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.; Grundy, M.D.; Stone, N.; Alison, L.; Bailey, M.D.; Kim, K.; Roger, S.; Lynne, T.; Joseph, F.-T.; Daniel, E. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary. J. Am. Coll. Cardiol. 2019, 73, 3168–3209. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Higashioka, M.; Sakata, S.; Honda, T.; Hata, J.; Yoshida, D.; Hirakawa, Y.; Shibata, M.; Goto, K.; Kitazono, T.; Osawa, H.; et al. Small Dense Low-Density Lipoprotein Cholesterol and the Risk of Coronary Heart Disease in a Japanese Community. J. Atheroscler. Thromb. 2020, 27, 669–682. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Lee, H.; Lee, D.-C.; Lee, H.-S.; Lee, J.-W. Predominance of small dense LDL differentiates metabolically unhealthy from metabolically healthy overweight adults in Korea. Metabolism 2014, 63, 415–421. [Google Scholar] [CrossRef]
- Janac, J.M.; Zeljkovic, A.; Jelic-Ivanovic, Z.D.; Dimitrijevic-Sreckovic, V.S.; Vekic, J.; Miljkovic, M.M.; Stefanovic, A.; Kotur-Stevuljevic, J.M.; Ivanisevic, J.M.; Spasojevic-Kalimanovska, V.V. Increased Oxidized High-Density Lipoprotein/High-Density Lipoprotein–Cholesterol Ratio as a Potential Indicator of Disturbed Metabolic Health in Overweight and Obese Individuals. Lab. Med. 2020, 51, 24–33. [Google Scholar] [CrossRef]
- Miyashita, M.; Okada, T.; Kuromori, Y.; Harada, K. LDL particle size, fat distribution and insulin resistance in obese children. Eur. J. Clin. Nutr. 2006, 60, 416–420. [Google Scholar] [CrossRef]
- Sopkova, Z.; Berneis, K.; Rizzo, M.; Spinas, G.A.; Dorkova, Z.; Tisko, R.; Tkacova, R. Size and Subclasses of Low-Density Lipoproteins in Patients with Obstructive Sleep Apnea. Angiology 2012, 63, 617–621. [Google Scholar] [CrossRef]
- Rizzo, M.; Berneis, K.; Altinova, A.E.; Toruner, F.B.; Akturk, M.; Ayvaz, G.; Rini, G.B.; Spinas, G.A.; Arslan, M. Atherogenic lipoprotein phenotype and LDL size and subclasses in women with gestational diabe-tes. Diabet Med. 2008, 25, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Berneis, K.; Rizzo, M.; Stettler, C.; Chappuis, B.; Braun, M.; Diem, P.; Christ, E.R. Comparative effects of rosiglitazone and pioglitazone on fasting and postprandial low-density lipoprotein size and sub-classes in patients with Type 2 diabetes. Expert Opin. Pharmacother. 2008, 9, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Nikolic, D.; Patti, A.M.; Mannina, C.; Montalto, G.; McAdams, B.S.; Rizvi, A.A.; Cosentino, F. GLP-1 receptor agonists and reduction of cardiometabolic risk: Potential underlying mechanisms. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2814–2821. [Google Scholar] [CrossRef] [PubMed]
- Giglio, R.V.; Patti, A.M.; Cicero, A.F.G.; Lippi, G.; Rizzo, M.; Toth, P.P.; Banach, M. Polyphenols: Potential Use in the Prevention and Treatment of Cardiovascular Diseases. Curr. Pharm. Des. 2018, 24, 239–258. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Banach, M.; Mikhailidis, D.P.; Bruckert, E.; Toth, P.P.; Watts, G.F.; Reiner, Ž.; Mancini, J.; Rizzo, M.; Mitchenko, O.; et al. Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group; International Lipid Expert Panel (ILEP). Safety of red yeast rice supplementation: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2019, 143, 1–16. [Google Scholar] [CrossRef]
- Fan, J.; Liu, Y.; Yin, S.; Chen, N.; Bai, X.; Ke, Q.; Shen, J.; Xia, M. Small dense LDL cholesterol is associated with metabolic syndrome traits independently of obesity and inflammation. Nutr. Metab. 2019, 16, 7. [Google Scholar] [CrossRef]
- Bojanin, D.; Vekic, J.; Milenkovic, T.; Vukovic, R.; Zeljkovic, A.; Stefanovic, A.; Janac, J.; Ivanisevic, J.; Mitrovic, K.; Miljkovic, M.; et al. Association between proprotein convertase subtilisin/kexin 9 (PCSK9) and lipoprotein subclasses in children with type 1 diabetes mellitus: Effects of glycemic control. Atherosclerosis 2019, 280, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Mikolasevic, I.; Žutelija, M.; Mavrinac, V.; Orlic, L. Dyslipidemia in patients with chronic kidney disease: Etiology and management. Int. J. Nephrol. Renov. Dis. 2017, 10, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Filler, G.; Taheri, S.; McIntyre, C.; Smith, C.; Subramanian, L.; Fusch, G.; Fusch, C. Chronic kidney disease stage affects small, dense low-density lipoprotein but not glycated low-density lipoprotein in younger chronic kidney disease patients: A cross-sectional study. Clin. Kidney J. 2018, 11, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Savić, J.; Zeljkovic, A.; Bogavac-Stanojevic, N.; Simic-Ogrizovic, S.; Kravljaca, M.; Stosovic, M.; Vekic, J.; Spasojevic-Kalimanovska, V.; Jelic-Ivanovic, Z.; Gojkovic, T.; et al. Association of small, dense low-density lipoprotein cholesterol and galectin-3 in patients with chronic kidney disease. Scand. J. Clin. Lab. Investig. 2014, 74, 637–643. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Jelic-Ivanovic, Z.; Damjanovic, T.; Suvakov, S.; Matic, M.; Savic-Radojevic, A.; Simic, T.; Spasojevic-Kalimanovska, V.; Gojkovic, T.; et al. Association of glutathione-S-transferase gene polymorphism and lipoprotein subclasses in hemodialysis patients. Clin. Biochem. 2014, 47, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Zeljkovic, A.; Vekic, J.; Spasojevic-Kalimanovska, V.; Jelic-Ivanovic, Z.; Peco-Antic, A.; Kostic, M.; Vasic, D.; Spasic, S. Characteristics of low-density and high-density lipoprotein subclasses in pediatric renal transplant recipients. Transpl. Int. 2011, 24, 1094–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, D.; Paulsen, K.; Türk, K.; Brandt, B.; Freitag-Wolf, S.; Hagen, I.; Zeuner, R.; Schröder, J.; Lieb, W.; Franke, A.; et al. Small dense LDL cholesterol in human subjects with different chronic inflammatory diseases. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Gentile, M.; Peluso, R.; Di Minno, M.N.D.; Costa, L.; Caso, F.; de Simone, B.; Iannuzzo, G.; Scarpa, R.; Rubba, P. Association between small dense LDL and sub-clinical atherosclerosis in patients with psoriatic arthritis. Clin. Rheumatol. 2016, 35, 2023–2029. [Google Scholar] [CrossRef]
- Ozbalkan, Z.; Efe, C.; Cesur, M.; Ertek, S.; Nasiroglu, N.; Berneis, K.; Rizzo, M. An update on the relationships between rheumatoid arthritis and atherosclerosis. Atherosclerosis 2010, 212, 377–382. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V.; Spasic, S.; Videnovic-Ivanov, J.; Ivanisevic, J.; Vucinic-Mihailovic, V.; Gojkovic, T. Distribution of Low-Density Lipoprotein and High-Density Lipoprotein Subclasses in Patients With Sarcoidosis. Arch. Pathol. Lab. Med. 2013, 137, 1780–1787. [Google Scholar] [CrossRef]
- Ivanisevic, J.; Vekic, J.; Zeljkovic, A.; Stefanovic, A.; Kotur-Stevuljevic, J.; Spasojevic-Kalimanovska, V.; Spasic, S.; Vucinic-Mihailovic, V.; Videnovic-Ivanov, J.; Jelic-Ivanovic, Z. Associations of lipoprotein subclasses and oxidative stress status in pulmonary and pulmonary plus extrapulmonary sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2018, 35, 198–205. [Google Scholar]
- Vukovic, R.; Zeljkovic, A.; Bufan, B.; Spasojevic-Kalimanovska, V.; Milenkovic, T.; Vekic, J. Hashimoto Thyroiditis and Dyslipidemia in Childhood: A Review. Front. Endocrinol. 2019, 10, 868. [Google Scholar] [CrossRef] [Green Version]
- Bansal, S.K. A Study of the Extended Lipid Profile including Oxidized LDL, Small Dense LDL, Lipoprotein (a) and Apolipoproteins in the Assessment of Cardiovascular Risk in Hypothyroid Patients. J. Clin. Diagn. Res. 2016, 10, BC04–BC08. [Google Scholar] [CrossRef]
- Saric, M.S.; Jurasic, M.-J.; Sovic, S.; Kranjcec, B.; Glivetic, T.; Demarin, V. Dyslipidemia in subclinical hypothyroidism requires assessment of small dense low density lipoprotein cholesterol (sdLDL-C). Rom. J. Intern. Med. 2017, 55, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Dumesic, D.A.; Abbott, D.H.; Sanchita, S.; Chazenbalk, G.D. Endocrine–metabolic dysfunction in polycystic ovary syndrome: An evolutionary perspective. Curr. Opin. Endocr. Metab. Res. 2020, 12, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.; Abbas, F.J.M.; Parkinson, L.; Chakraborty, J.; Akanji, F.A.O. LDL Species Heterogeneity in the Atherogenic Dyslipidemia of Polycystic Ovary Syndrome. Am. J. Clin. Pathol. 2008, 129, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Berneis, K.; Rizzo, M.; Hersberger, M.; Rini, G.B.; Di Fede, G.; Pepe, I.; Spinas, G.A.; Carmina, E. Athero-genic forms of dyslipidaemia in women with polycystic ovary syndrome. Int. J. Clin. Pract. 2009, 63, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Wekker, V.; van Dammen, L.; Koning, A.; Heida, K.Y.; Painter, R.C.; Limpens, J.; Laven, J.S.E.; Roeters van Lennep, J.E.; Roseboom, T.J.; Hoek, A. Long-term cardiometabolic disease risk in women with PCOS: A systematic review and meta-analysis. Hum. Reprod. Update 2020, 26, 942–960. [Google Scholar] [CrossRef]
- Roe, A.; Hillman, J.; Butts, S.; Smith, M.; Rader, D.; Playford, M.; Mehta, N.N.; Dokras, A. Decreased Cholesterol Efflux Capacity and Atherogenic Lipid Profile in Young Women With PCOS. J. Clin. Endocrinol. Metab. 2014, 99, E841–E847. [Google Scholar] [CrossRef]
- Kim, J.G.; Chae, S.J.; Choi, Y.M.; Hwang, K.R.; Song, S.H.; Yoon, S.H.; Kim, S.M.; Ku, S.Y.; Moon, S.Y. Atherogenic changes in low-density lipoprotein particle profiles were not observed in non-obese women with polycystic ovary syndrome. Hum. Reprod. 2013, 28, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- Blagojevic, I.M.P.; Vekic, J.Z.; Macut, D.P.; Ignjatovic, S.D.; Miljkovic-Trailovic, M.M.; Zeljkovic, A.R.; Spasojevic-Kalimanovska, V.V.; Bozic-Antic, I.B.; Bjekic-Macut, J.D.; Kastratovic-Kotlica, B.A.; et al. Overweight and obesity in polycystic ovary syndrome: Association with inflammation, oxidative stress and dyslipidaemia. Br. J. Nutr. 2021, 1–9. [Google Scholar] [CrossRef]
- Charlton, F.; Tooher, J.; Rye, K.-A.; Hennessy, A. Cardiovascular Risk, Lipids and Pregnancy: Preeclampsia and the Risk of Later Life Cardiovascular Disease. Hear. Lung Circ. 2014, 23, 203–212. [Google Scholar] [CrossRef]
- Zeljkovic, A.; Vekic, J.; Spasic, S.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V.; Gojkovic, T.; Ardalic, D.; Mandic-Markovic, V.; Cerovic, N.; Mikovic, Z. Changes in LDL and HDL Subclasses in Normal Pregnancy and Associations with Birth Weight, Birth Length and Head Circumference. Matern. Child Heal. J. 2012, 17, 556–565. [Google Scholar] [CrossRef]
- Gugliucci, A.; Numaguchi, M.; Caccavello, R.; Kimura, S. Small-dense low-density lipoproteins are the predominant apoB-100-containing lipoproteins in cord blood. Clin. Biochem. 2014, 47, 475–477. [Google Scholar] [CrossRef]
- Li, Y.; He, J.; Zeng, X.; Zhao, S.; Wang, X.; Yuan, H. Non-fasting lipids detection and their significance in pregnant women. Lipids Heal. Dis. 2019, 18, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabunac, P.; Orlić, N.K.; Ardalić, D.; Banjac, G.; Ivanišević, J.; Janać, J.; Vekić, J.; Zeljković, A.; Mihajlović, M.; Rajović, N.; et al. Unraveling the role of oxidative stress and lipid status parameters in the onset of preeclampsia. Hypertens. Pregnancy 2021, 40, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Antonić, T.D.; Ardalić, D.Č.; Vladimirov, S.S.; Banjac, G.S.; Cabunac, P.J.; Zeljković, A.R.; Karadžov-Orlić, N.T.; Spasojević-Kalimanovska, V.V.; Miković, Ž.D.; Stefanović, A.Ž. Cholesterol homeostasis is dysregulated in women with preeclampsia. Pol. Arch. Intern. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gentile, M.; Iannuzzo, G.; Mattiello, A.; Marotta, G.; Rubba, F.; Iannuzzi, A.; Panico, S.; Rubba, P. Association between Lp(a) and small dense LDL in menopausal women without metabolic syndrome. Acta Cardiol. 2019, 74, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Mogarekar, M.R.; Kulkarni, S.K. Small Dense Low Density Lipoprotein Cholesterol, Paraoxonase 1 and Lipid Profile in Postmenopausal Women: Quality or Quantity? Arch. Med. Res. 2015, 46, 534–538. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V.; Bogavac-Stanojevic, N.; Memon, L.; Spasic, S. Small, dense LDL cholesterol and apolipoprotein B: Relationship with serum lipids and LDL size. Atherosclerosis 2009, 207, 496–501. [Google Scholar] [CrossRef]
- Izumida, T.; Nakamura, Y.; Sato, Y.; Ishikawa, S. Association among age, gender, menopausal status and small dense low-density lipoprotein cholesterol: A cross-sectional study. BMJ Open 2021, 11, e041613. [Google Scholar] [CrossRef]
- Al Mahmeed, W.; Al-Rasadi, K.; Banerjee, Y.; Ceriello, A.; Cosentino, F.; Galia, M.; Goh, S.Y.; Kempler, P.; Lessan, N.; Papanas, N. Cardiometabolic Panel of International experts on Syndemic COVID-19 (CAPISCO). Promoting a Syndemic Approach for Cardiometabolic Disease Management During COVID-19: The CAPISCO International Expert Panel. Front. Cardiovasc. Med. 2021, 8, 787761. [Google Scholar] [CrossRef]
- Stoian, A.P.; Banerjee, Y.; Rizvi, A.A.; Rizzo, M. Diabetes and the COVID-19 Pandemic: How Insights from Recent Experience Might Guide Future Management. Metab. Syndr. Relat. Disord. 2020, 18, 173–175. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vekic, J.; Zeljkovic, A.; Cicero, A.F.G.; Janez, A.; Stoian, A.P.; Sonmez, A.; Rizzo, M. Atherosclerosis Development and Progression: The Role of Atherogenic Small, Dense LDL. Medicina 2022, 58, 299. https://doi.org/10.3390/medicina58020299
Vekic J, Zeljkovic A, Cicero AFG, Janez A, Stoian AP, Sonmez A, Rizzo M. Atherosclerosis Development and Progression: The Role of Atherogenic Small, Dense LDL. Medicina. 2022; 58(2):299. https://doi.org/10.3390/medicina58020299
Chicago/Turabian StyleVekic, Jelena, Aleksandra Zeljkovic, Arrigo F. G. Cicero, Andrej Janez, Anca Pantea Stoian, Alper Sonmez, and Manfredi Rizzo. 2022. "Atherosclerosis Development and Progression: The Role of Atherogenic Small, Dense LDL" Medicina 58, no. 2: 299. https://doi.org/10.3390/medicina58020299