
The Influence of Serum Uric Acid Level on Non-Motor Symptoms Occurrence and Severity in Patients with Idiopathic Parkinson’s Disease and Atypical Parkinsonisms—A Systematic Review

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
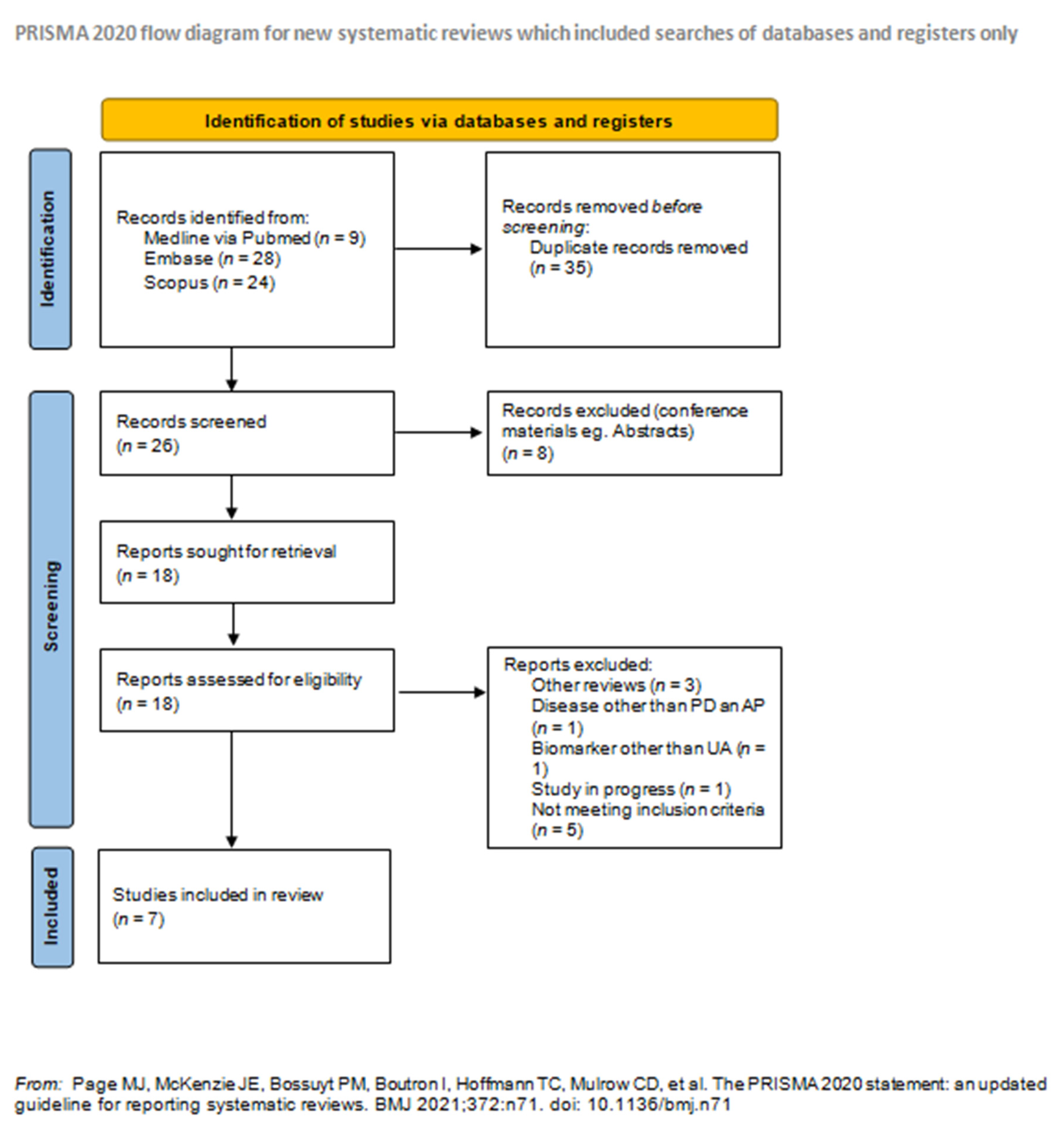
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
3. Results
3.1. Methodology of Included Studies
3.1.1. Inclusion Criteria
3.1.2. Exclusion Criteria
3.1.3. Assessment of Disease Advancement
3.1.4. Means of NMS Assessment
3.1.5. Means of UA Measurement
3.2. Results Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jesús, S.; Pérez, I.; Cáceres-Redondo, M.T.; Carrillo, F.; Carballo, M.; Gómez-Garre, P.; Mir, P. Low serum uric acid concentration in Parkinson’s disease in southern Spain. Eur. J. Neurol. 2012, 20, 208–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzschild, M.A.; Ascherio, A.; Beal, M.F.; Cudkowicz, M.E.; Curhan, G.C.; Hare, J.M.; Hooper, D.C.; Kieburtz, K.D.; Macklin, E.; Oakes, D.; et al. Inosine to Increase Serum and Cerebrospinal Fluid Urate in Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2014, 71, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, I.; Schlesinger, N. Uric acid in Parkinson’s disease. Mov. Disord. 2008, 23, 1653–1657. [Google Scholar] [CrossRef]
- Ou, R.; Cao, B.; Wei, Q.; Hou, Y.; Xu, Y.; Song, W.; Zhao, B.; Shang, H. Serum uric acid levels and freezing of gait in Parkinson’s disease. Neurol. Sci. 2017, 38, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Weisskopf, M.G.; O’Reilly, E.; Chen, H.; Schwarzschild, M.A.; Ascherio, A. Plasma Urate and Risk of Parkinson’s Disease. Am. J. Epidemiol. 2007, 166, 561–567. [Google Scholar] [CrossRef]
- Deutschländer, A.B.; Ross, O.; Dickson, D.W.; Wszolek, Z.K. Atypical parkinsonian syndromes: A general neurologist’s perspective. Eur. J. Neurol. 2017, 25, 41–58. [Google Scholar] [CrossRef]
- Oropesa-Ruiz, J.M.; Huertas-Fernández, I.; Jesús, S.; Cáceres-Redondo, M.T.; Vargas-González, L.; Carrillo, F.; Carballo, M.; Gómez-Garre, P.; Mir, P. Low serum uric acid levels in progressive Supranuclear Palsy: Uric Acid in PSP. Mov. Disord. 2016, 31, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Sakuta, H.; Suzuki, K.; Miyamoto, T.; Miyamoto, M.; Numao, A.; Fujita, H.; Watanabe, Y.; Hirata, K. Serum uric acid levels in Parkinson’s disease and related disorders. Brain Behav. 2016, 7, e00598. [Google Scholar] [CrossRef]
- Grażyńska, A.; Urbaś, W.; Antoniuk, S.; Adamczewska, K.; Bień, M.; Chmiela, T.; Siuda, J. Comparative analysis of non-motor symptoms in patients with Parkinson’s Disease and atypical parkinsonisms. Clin. Neurol. Neurosurg. 2020, 197, 106088. [Google Scholar] [CrossRef]
- Schaeffer, E.; Berg, D. Dopaminergic Therapies for Non-motor Symptoms in Parkinson’s Disease. CNS Drugs 2017, 31, 551–570. [Google Scholar] [CrossRef]
- Maillet, A.; Krack, P.; Lhommée, E.; Metereau, E.; Klinger, H.; Favre, E.; Le Bars, D.; Schmitt, E.; Bichon, A.; Pelissier, P.; et al. The prominent role of serotonergic degeneration in apathy, anxiety and depression inde novoParkinson’s disease. Brain 2016, 139, 2486–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhuri, K.R.; Martinez-Martin, P.; Schapira, A.; Stocchi, F.; Sethi, K.D.; Odin, P.; Brown, R.; Koller, W.C.; Barone, P.; A Macphee, G.J.; et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: The NMSQuest study: Nonmotor Symptoms and PD. Mov. Disord. 2006, 21, 916–923. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Martinez-Martin, P.; Brown, R.; Sethi, K.; Stocchi, F.; Odin, P.; Ondo, W.; Abe, K.; Macphee, G.; MacMahon, D.; et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: Results from an international pilot study. Mov. Disord. 2007, 22, 1901–1911. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Huang, X.; Ng, S.Y.-E.; Chia, N.S.-Y.; Acharyya, S.; Setiawan, F.; Lu, Z.-H.; Ng, E.; Tay, K.-Y.; Au, W.-L.; Tan, E.-K.; et al. Serum uric acid level and its association with motor subtypes and non-motor symptoms in early Parkinson’s disease: PALS study. Park. Relat. Disord. 2018, 55, 50–54. [Google Scholar] [CrossRef]
- Moccia, M.; Picillo, M.; Erro, R.; Vitale, C.; Longo, K.; Amboni, M.; Santangelo, G.; Spina, E.; De Rosa, A.; De Michele, G.; et al. Is serum uric acid related to non-motor symptoms in de-novo Parkinson’s disease patients? Park. Relat. Disord. 2014, 20, 772–775. [Google Scholar] [CrossRef]
- Pan, M.; Gao, H.; Long, L.; Xu, Y.; Liu, M.; Zou, J.; Wu, A.; Wei, X.; Chen, X.; Tang, B.; et al. Serum Uric Acid in Patients with Parkinson’s Disease and Vascular Parkinsonism: A Cross-Sectional Study. Neuroimmunomodulation 2013, 20, 19–28. [Google Scholar] [CrossRef]
- van Wamelen, D.J.; Taddei, R.N.; Calvano, A.; Titova, N.; Leta, V.; Shtuchniy, I.; Jenner, P.; Martinez-Martin, P.; Katunina, E.; Chaudhuri, K.R. Serum Uric Acid Levels and Non-Motor Symptoms in Parkinson’s Disease. J. Park. Dis. 2020, 10, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Moccia, M.; Picillo, M.; Erro, R.; Vitale, C.; Longo, K.; Amboni, M.; Santangelo, G.; Palladino, R.; Capo, G.; Orefice, G.; et al. Presence and progression of non-motor symptoms in relation to uric acid inde novoParkinson’s disease. Eur. J. Neurol. 2014, 22, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Wei, X.; Zou, J.; Wang, R.; Liu, X.; Xu, X.; Lu, J.; Wang, Z.; Tang, B.; Wang, B.; et al. Contra-Directional Expression of Serum Homocysteine and Uric Acid as Important Biomarkers of Multiple System Atrophy Severity: A Cross-Sectional Study. Front. Cell. Neurosci. 2015, 9, 247. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.; Zhan, Z.; Zhang, L.; Zhu, J.; Liu, Y.; Zhang, L.; Ge, J.; Zhao, Y.; Zhang, L.; Dong, J. Prevalence and Risk Factors for Malnutrition in Patients With Parkinson’s Disease. Front. Neurol. 2020, 11, 533731. [Google Scholar] [CrossRef] [PubMed]
- Gilman, S.; Low, P.; Quinn, N.; Albanese, A.; Ben-Shlomo, Y.; Fowler, C.; Kaufmann, H.; Klockgether, T.; Lang, A.; Lantos, P.; et al. Consensus statement on the diagnosis of multiple system atrophy. J. Neurol. Sci. 1999, 163, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Wenning, G.K.; Krismer, F. Multiple system atrophy. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2013; Volume 117, pp. 229–241. ISBN 978-0-444-53491-0. [Google Scholar]
- Martín, R.U.-S.; Francke, P.V.; Illanes, F.L.; Gazmuri, A.J.; Rivera, J.S.; Ferńndez, J.G.; Martínez, J.S.; Juri, C. Plasma Urate in REM Sleep Behavior Disorder: Plasma Urate in Rem Sleep Behavior Disorder. Mov. Disord. 2013, 28, 1150–1151. [Google Scholar] [CrossRef]
- Chou, Y.-T.; Li, C.-H.; Shen, W.-C.; Yang, Y.-C.; Lu, F.-H.; Wu, J.-S.; Chang, C.-J. Association of sleep quality and sleep duration with serum uric acid levels in adults. PLoS ONE 2020, 15, e0239185. [Google Scholar] [CrossRef]
- Papandreou, C.; Babio, N.; Díaz-López, A.; Martínez-González, M.; Becerra-Tomas, N.; Corella, D.; Schröder, H.; Romaguera, D.; Vioque, J.; Alonso-Gómez, M.; et al. Sleep Duration is Inversely Associated with Serum Uric Acid Concentrations and Uric Acid to Creatinine Ratio in an Elderly Mediterranean Population at High Cardiovascular Risk. Nutrients 2019, 11, 761. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Wang, L.; Teng, W.; Huang, K.; Shang, X. Correlation of Fatigue during the Acute Stage of Stroke with Serum Uric Acid and Glucose Levels, Depression, and Disability. Eur. Neurol. 2014, 72, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Naviaux, R.K.; Naviaux, J.C.; Li, K.; Bright, A.T.; Alaynick, W.A.; Wang, L.; Baxter, A.; Nathan, N.; Anderson, W.; Gordon, E. Metabolic features of chronic fatigue syndrome. Proc. Natl. Acad. Sci. USA 2016, 113, E5472–E5480. [Google Scholar] [CrossRef] [Green Version]
- Dogan, V.B.; Koksal, A.; Dirican, A.; Baybas, S.; Dirican, A.; Dogan, G.B. Independent effect of fatigue on health-related quality of life in patients with idiopathic Parkinson’s disease. Neurol. Sci. 2015, 36, 2221–2226. [Google Scholar] [CrossRef]
- Annanmaki, T.; Pessala-Driver, A.; Hokkanen, L.; Murros, K. Uric acid associates with cognition in Parkinson’s disease. Park. Relat. Disord. 2008, 14, 576–578. [Google Scholar] [CrossRef]
- Gao, X.; O’Reilly, J.; Schwarzschild, M.A.; Ascherio, A. Prospective study of plasma urate and risk of Parkinson disease in men and women. Neurology 2016, 86, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Ton, T.; Boudreau, R.; Yang, M.; Thacker, E.; Studenski, S.; Longstreth, J.W.; Strotmeyer, E.; Newman, A.B. The Risk of Parkinson Disease Associated with Urate in a Community-Based Cohort of Older Adults. Neuroepidemiology 2011, 36, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Reilly, E.J.; Gao, X.; Weisskopf, M.G.; Chen, H.; Schwarzschild, M.A.; Spiegelman, D.; Ascherio, A. Plasma Urate and Parkinson’s Disease in Women. Am. J. Epidemiol. 2010, 172, 666–670. [Google Scholar] [CrossRef] [Green Version]
- Bartoli, F.; Crocamo, C.; Mazza, M.G.; Clerici, M.; Carrà, G. Uric acid levels in subjects with bipolar disorder: A comparative meta-analysis. J. Psychiatr. Res. 2016, 81, 133–139. [Google Scholar] [CrossRef]
- Lyngdoh, T.; Bochud, M.; Glaus, J.; Castelao, E.; Waeber, G.; Vollenweider, P.; Preisig, M. Associations of Serum Uric Acid and SLC2A9 Variant with Depressive and Anxiety Disorders: A Population-Based Study. PLoS ONE 2013, 8, e76336. [Google Scholar] [CrossRef] [Green Version]
- Wen, S.; Cheng, M.; Wang, H.; Yue, J.; Wang, H.; Li, G.; Zheng, L.; Zhong, Z.; Peng, F. Serum uric acid levels and the clinical characteristics of depression. Clin. Biochem. 2011, 45, 49–53. [Google Scholar] [CrossRef]
- Gaenslen, A.; Wurster, I.; Brockmann, K.; Huber, H.; Godau, J.; Faust, B.; Lerche, S.; Eschweiler, G.W.; Maetzler, W.; Berg, D. Prodromal features for Parkinson’s disease—baseline data from the TREND study. Eur. J. Neurol. 2014, 21, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Bohnen, N.I.; Müller, M.L.T.M.; Kotagal, V.; Koeppe, R.A.; Kilbourn, M.A.; Albin, R.L.; Frey, K.A. Olfactory dysfunction, central cholinergic integrity and cognitive impairment in Parkinson’s disease. Brain 2010, 133, 1747–1754. [Google Scholar] [CrossRef] [Green Version]
- Casjens, S.; Eckert, A.; Woitalla, D.; Ellrichmann, G.; Turewicz, M.; Stephan, C.; Eisenacher, M.; May, C.; Meyer, H.E.; Brüning, T.; et al. Diagnostic Value of the Impairment of Olfaction in Parkinson’s Disease. PLoS ONE 2013, 8, e64735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buhmann, C.; Kassubek, J.; Jost, W.H. Management of Pain in Parkinson’s Disease. J. Park. Dis. 2020, 10, S37–S48. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, D.-S.; An, C.-Y.; Liu, Y.-Z.; Liu, X.-H.; Zhang, F.; Ning, L.-N.; Li, C.-L.; Ma, C.-M.; Hu, R.-T. Association between serum uric acid level and multiple system atrophy: A meta-analysis. Clin. Neurol. Neurosurg. 2018, 169, 16–20. [Google Scholar] [CrossRef]
- Santos-García, D.; COPPADIS Study Group; Mir, P.; Cubo, E.; Vela, L.; Rodríguez-Oroz, M.C.; Martí, M.J.; Arbelo, J.M.; Infante, J.; Kulisevsky, J.; et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), a global –clinical evaluations, serum biomarkers, genetic studies and neuroimaging–prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016, 16, 26. [Google Scholar] [CrossRef]


{kind=link}
| Domain in NMSS (NMS-Quest) | Huang X. et al. [15] | Moccia M. et al. [16] | Pan M. et al. [17] | van Wamelen et al. [18] | Moccia M. et. al. [19] | Chen D. et al. [20] | Yang T. et al. [21] |
|---|---|---|---|---|---|---|---|
| Total NMSS (NMS-Quest) | - | + | + | + | - | - | - |
| Cardiovascular (Cardiovascular) | - | + | - | + | + | - | - |
| Sleep/fatigue (Sleep) | + | + | + | + | - | - | - |
| Mood (Depression/anxiety) | - | + | + | - | + | - | - |
| Perceptual (Hallucinations/delusions) | - | - | + | - | - | - | - |
| Attention/memory (Attention/memory) | + | + | + | - | + | - | - |
| Gastrointestinal (Gastrointestinal) | - | - | + | - | - | - | - |
| Urinary (Urinary) | - | - | - | - | - | - | - |
| Sexual (Sexual) | - | - | - | - | - | - | - |
| Miscellany (Miscellany) | - | - | - | + | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grażyńska, A.; Adamczewska, K.; Antoniuk, S.; Bień, M.; Toś, M.; Kufel, J.; Urbaś, W.; Siuda, J. The Influence of Serum Uric Acid Level on Non-Motor Symptoms Occurrence and Severity in Patients with Idiopathic Parkinson’s Disease and Atypical Parkinsonisms—A Systematic Review. Medicina 2021, 57, 972. https://doi.org/10.3390/medicina57090972
Grażyńska A, Adamczewska K, Antoniuk S, Bień M, Toś M, Kufel J, Urbaś W, Siuda J. The Influence of Serum Uric Acid Level on Non-Motor Symptoms Occurrence and Severity in Patients with Idiopathic Parkinson’s Disease and Atypical Parkinsonisms—A Systematic Review. Medicina. 2021; 57(9):972. https://doi.org/10.3390/medicina57090972
Chicago/Turabian StyleGrażyńska, Anna, Klaudia Adamczewska, Sofija Antoniuk, Martyna Bień, Mateusz Toś, Jakub Kufel, Weronika Urbaś, and Joanna Siuda. 2021. "The Influence of Serum Uric Acid Level on Non-Motor Symptoms Occurrence and Severity in Patients with Idiopathic Parkinson’s Disease and Atypical Parkinsonisms—A Systematic Review" Medicina 57, no. 9: 972. https://doi.org/10.3390/medicina57090972