Cannabidiol and Vitamin D3 Impact on Osteogenic Differentiation of Human Dental Mesenchymal Stem Cells

 ,
, 
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Tissue Samples
2.2. Stem Cell Isolation
2.3. Characterization of the Isolated Cells
2.3.1. Immunocytochemical Characterization by Flow Cytometry
2.3.2. Reverse Transcription Polymerase Chain Reaction (RT-PCR)
2.3.3. Multipotential Ability-Differentiation Experiments
Osteogenic Differentiation
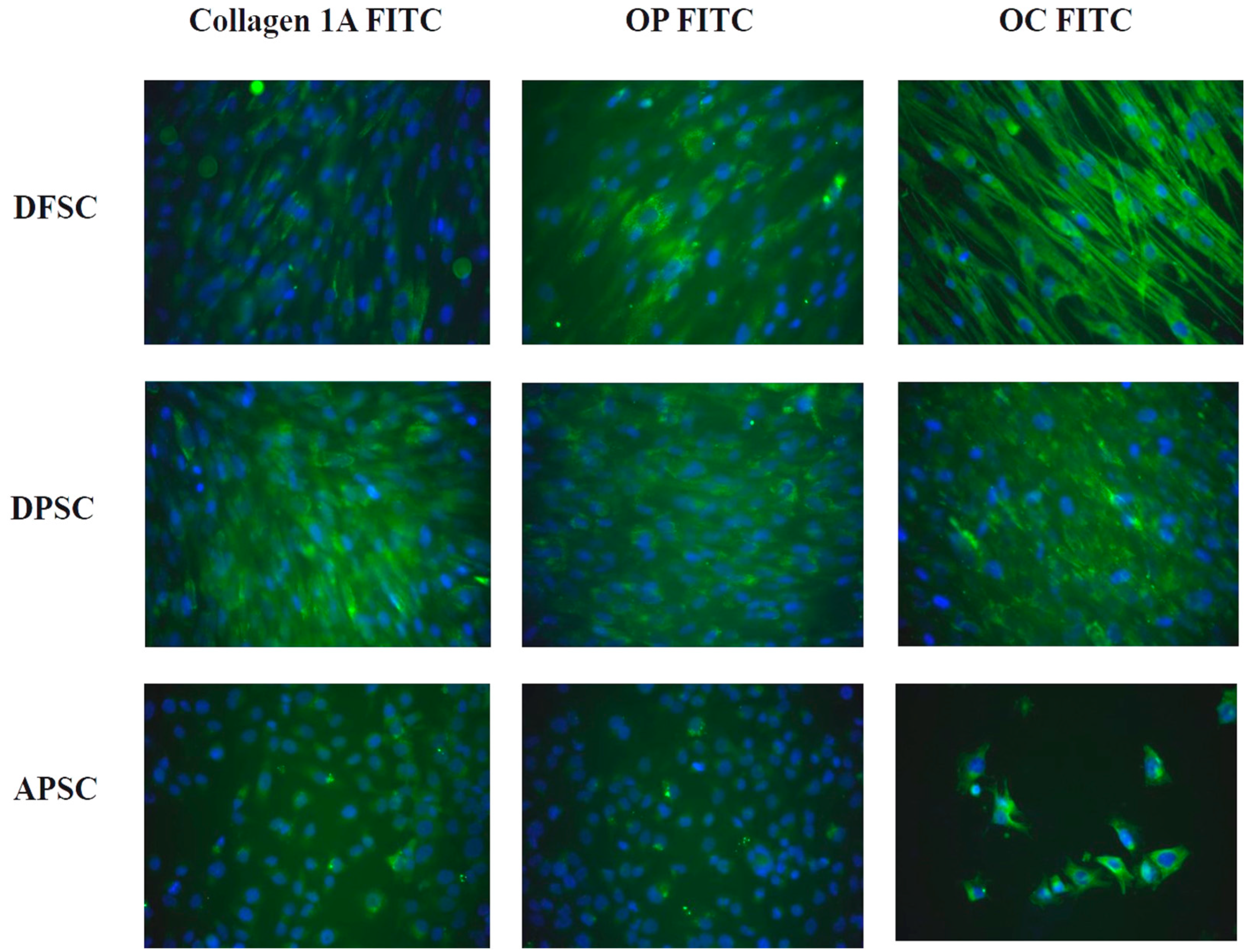
Immunocytochemical Staining for Osteogenic Markers
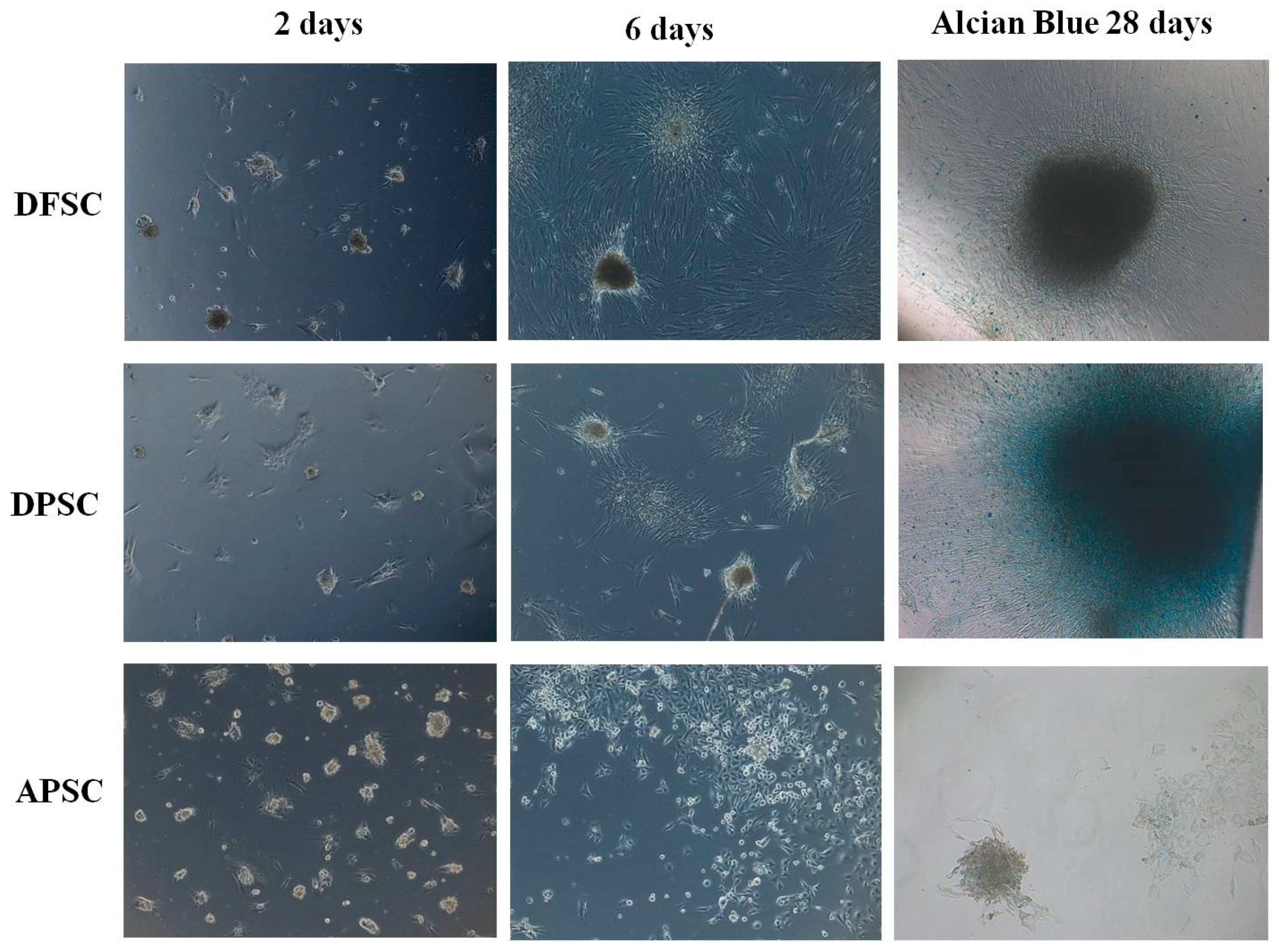
Chondrogenic Differentiation
Adipogenic Differentiation
2.4. Evaluation of Canabidiol Effects on Dental Tissues Derived Stem Cells
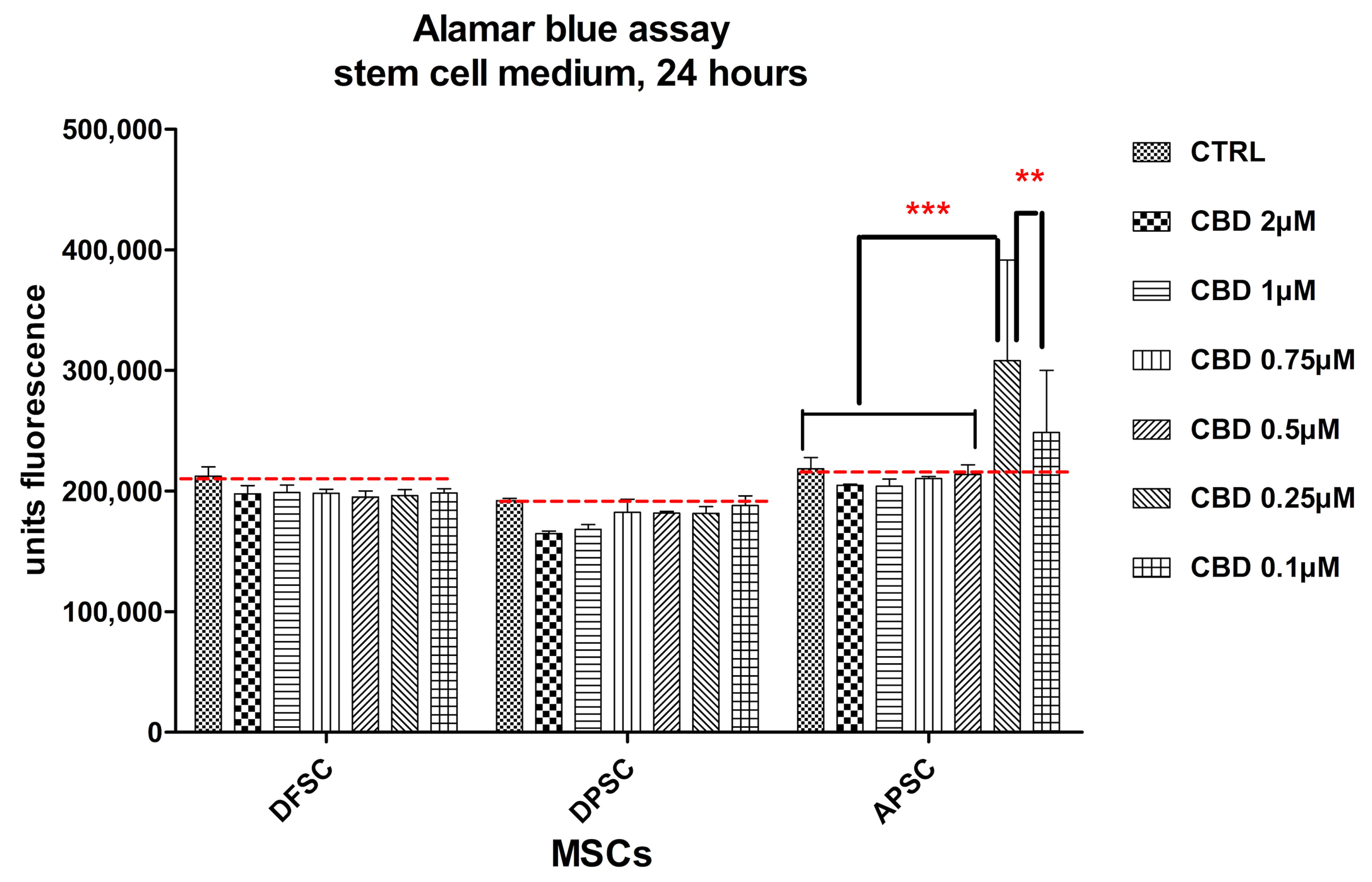
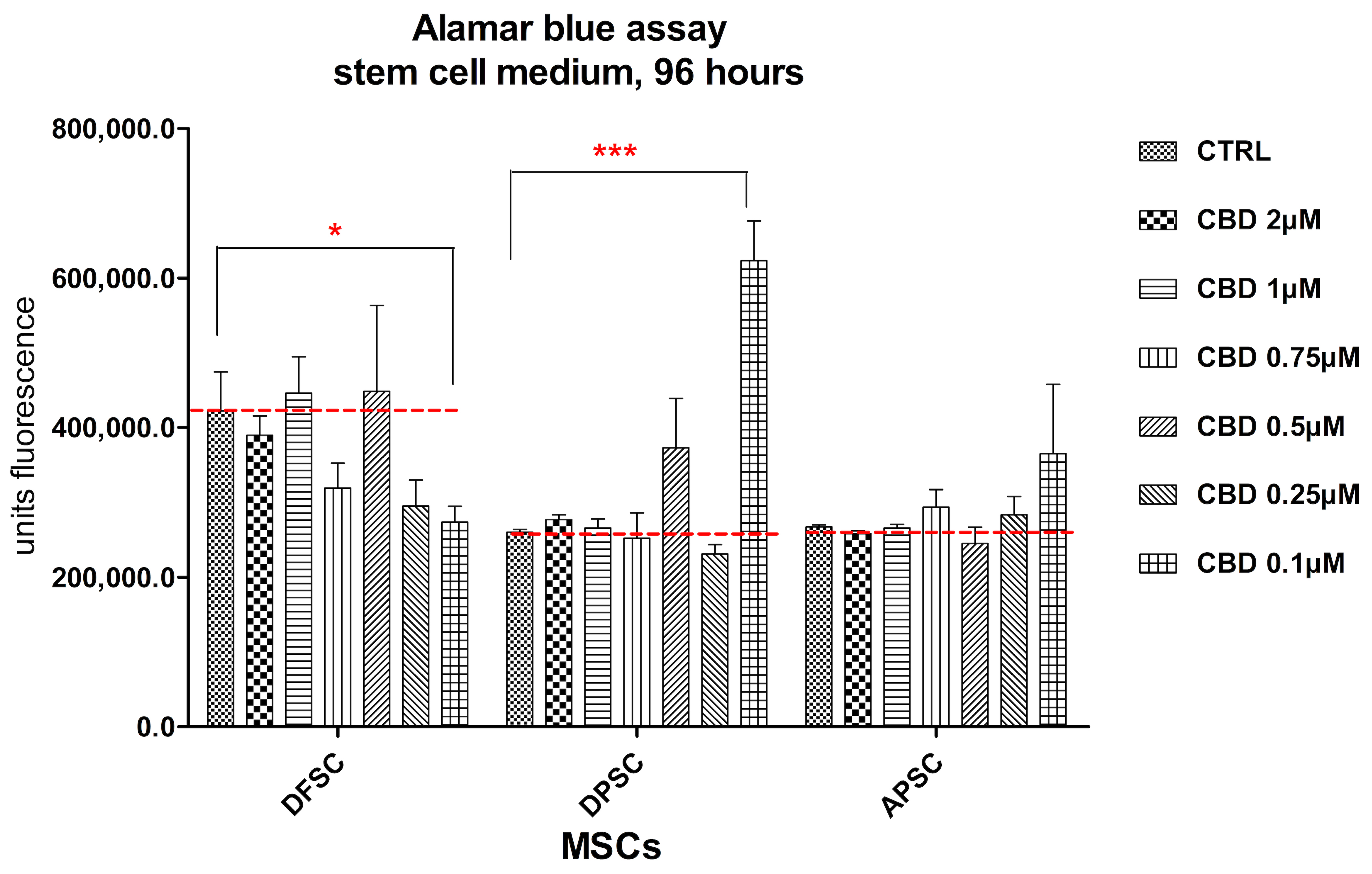
2.4.1. Alamar Blue Cell Viability Assay
2.4.2. Evaluation by RT-PCR of Genes Implicated in Osteogenic Differentiation
3. Results
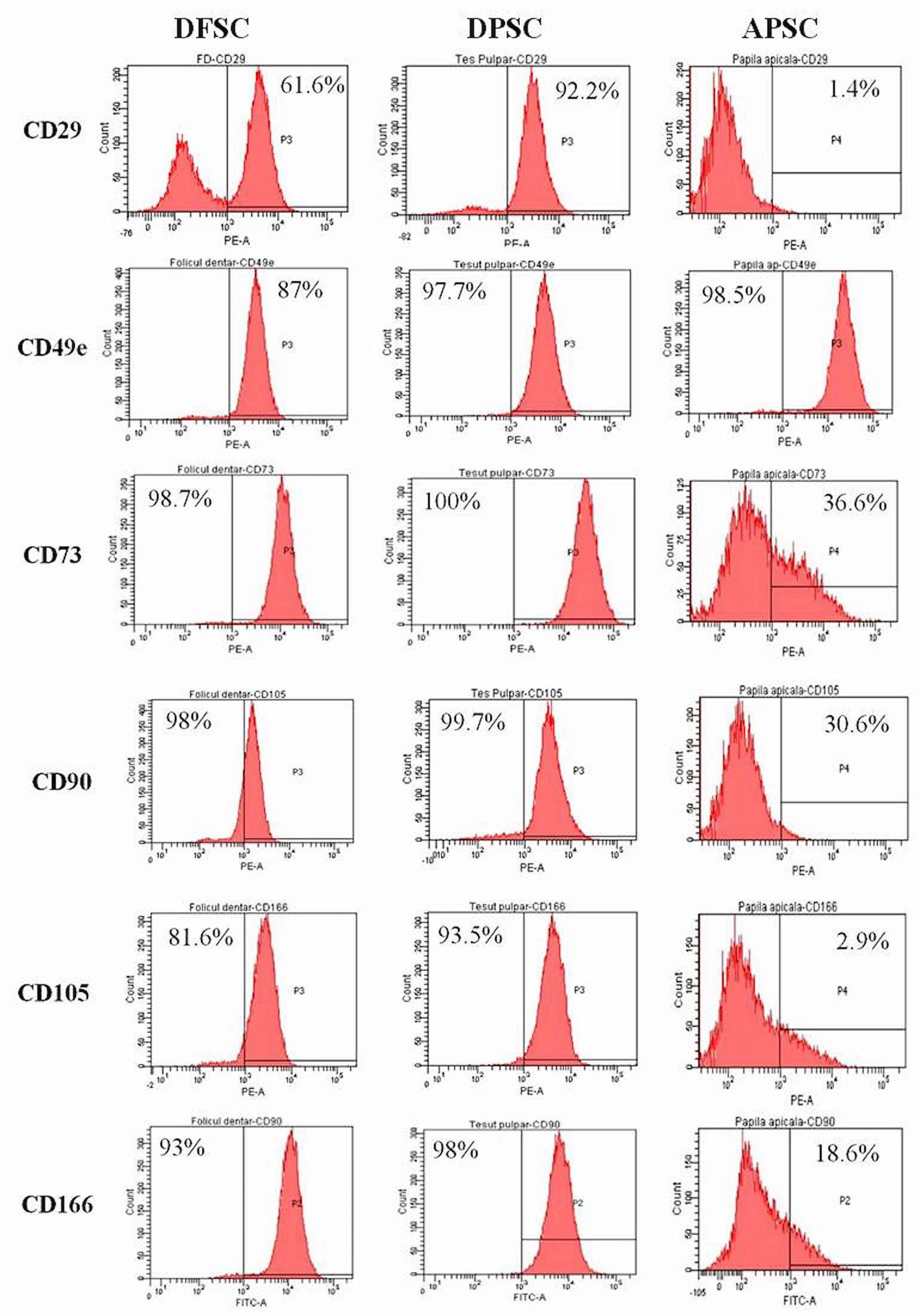
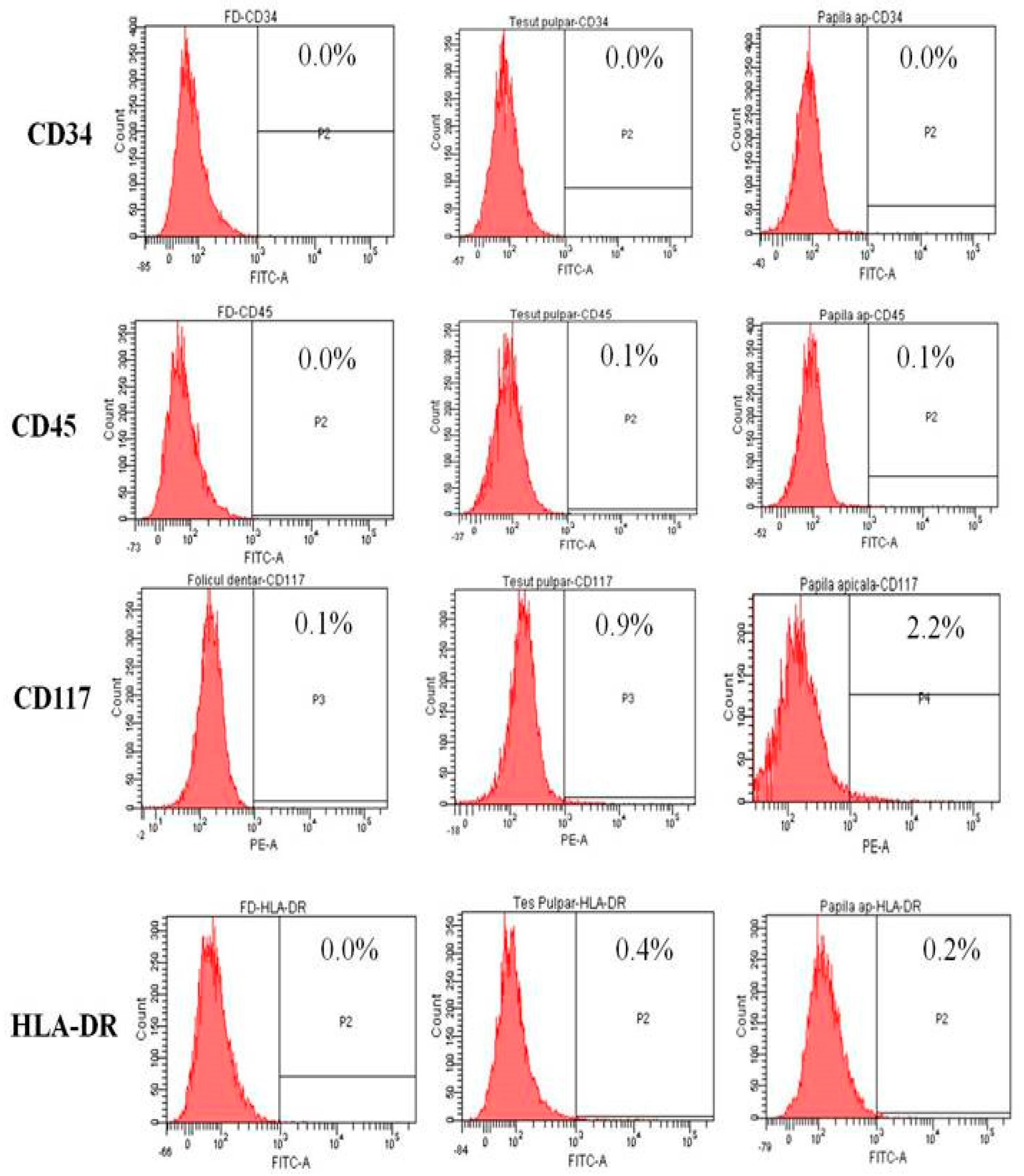
3.1. Flow Cytometry
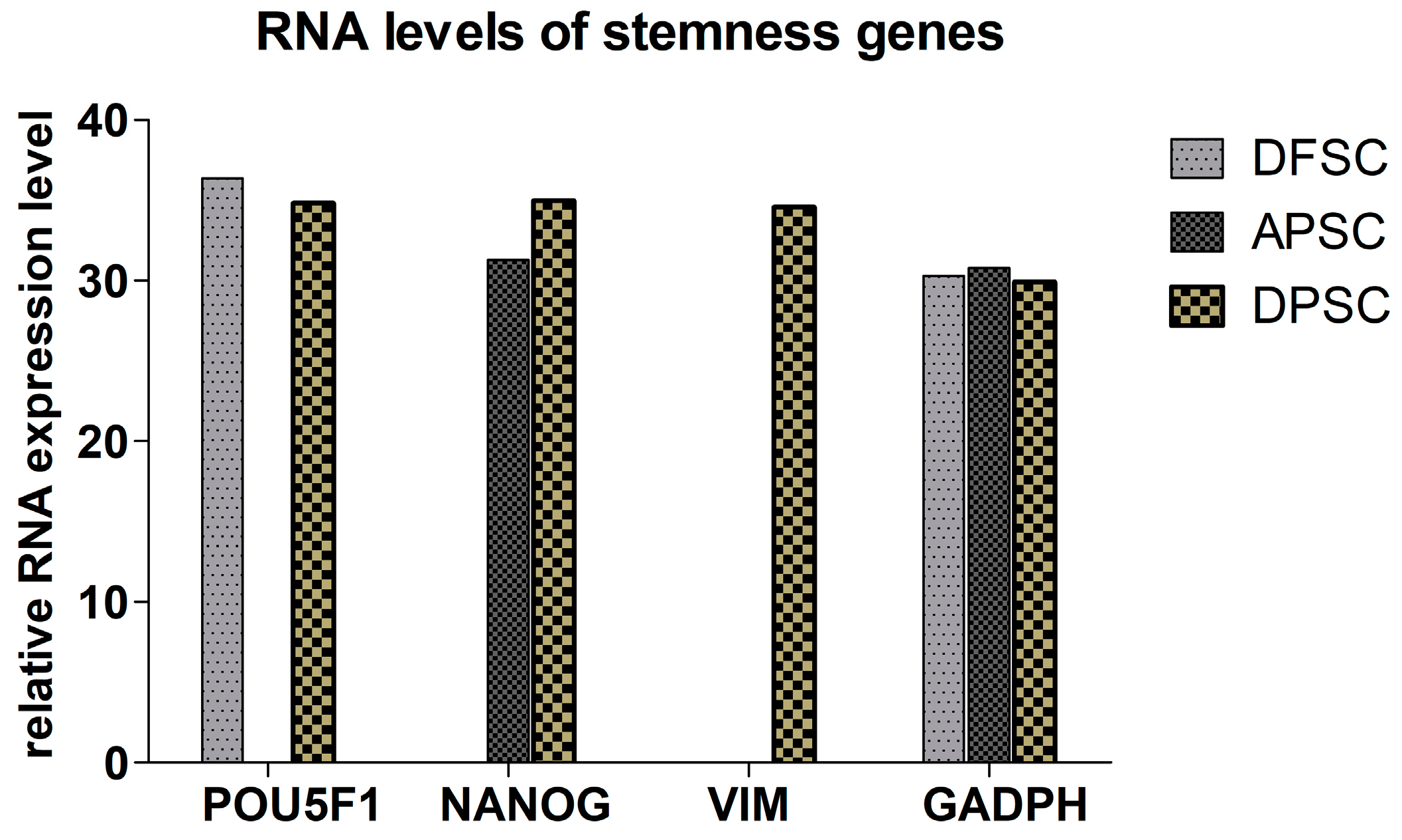
3.2. RT-PCR-for Stemness Markers
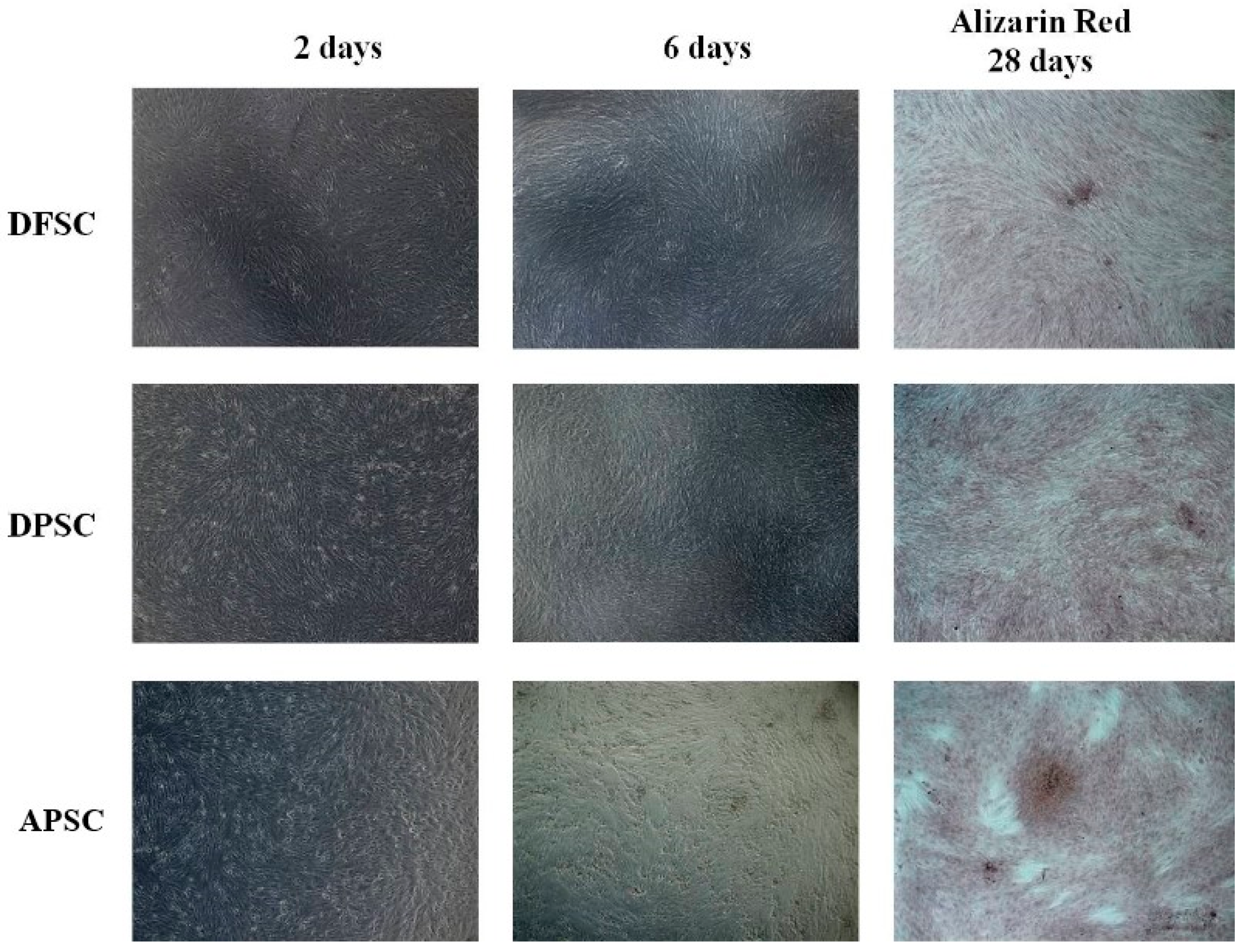
3.3. Osteogenic Differentiation with Osteoinductive Medium
3.4. Chondroblastic Differentiation
3.5. Adipogenic Differentiation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lucaciu, O.; Crisan, B.; Crisan, L.; Baciut, M.; Soritau, O.; Bran, S.; Biris, A.R.; Hurubeanu, L.; Hedesiu, M.; Vacaras, S.; et al. In quest of optimal drug-supported and targeted bone regeneration in the cranio facial area: A review of techniques and methods. Drug Metab. Rev. 2015, 47, 455–469. [Google Scholar] [CrossRef] [PubMed]
- Apostu, D.; Lucaciu, O.; Mester, A.; Benea, H.; Oltean-Dan, D.; Onisor, F.; Baciut, M.; Bran, S. Cannabinoids and bone regeneration. Drug Metab. Rev. 2019, 51, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Barba, M.; Di Taranto, G.; Lattanzi, W. Adipose-derived stem cell therapies for bone regeneration. Expert Opin. Biol. Ther. 2017, 17, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Li, B. MicroRNA Regulation in Osteogenic and Adipogenic Differentiation of Bone Mesenchymal Stem Cells and its Application in Bone Regeneration. Curr. Stem. Cell Res. Ther. 2018, 13, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Mazur, M.M.; Buck, A.C.; Wandtke, M.E.; Liu, J.; Ebraheim, N.A. Prospective Review of Mesenchymal Stem Cells Differentiation into Osteoblasts. Orthop. Surg. 2017, 9, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullah, I.; Subbarao, R.B.; Rho, G.J. Human mesenchymal stem cells—Current trends and future prospective. Biosci. Rep. 2015, 35, e00191. [Google Scholar] [CrossRef]
- Liu, J.; Yu, F.; Sun, Y.; Jiang, B.; Zhang, W.; Yang, J.; Xu, G.-T.; Liang, A.; Liu, S. Concise reviews: Characteristics and potential applications of human dental tissue-derived mesenchymal stem cells. Stem. Cells 2015, 33, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jiang, C.-M.; An, S.; Cheng, Q.; Huang, Y.-F.; Wang, Y.-T.; Gou, Y.-C.; Xiao, L.; Yu, W.-J.; Wang, J. Immunomodulatory properties of dental tissue-derived mesenchymal stem cells. Oral Dis. 2014, 20, 25–34. [Google Scholar] [CrossRef]
- Estrela, C.; Goncalves de Alencar, A.H.; Kitten, G.T.; Vencio, E.F.; Gava, E. Mesenchymal stem cells in the dental tissues: Perspectives for tissue regeneration. Braz. Dent. J. 2011, 22, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Tamaki, Y.; Nakahara, T.; Ishikawa, H.; Sato, S. In vitro analysis of mesenchymal stem cells derived from human teeth and bone marrow. Odontology 2013, 101, 121–132. [Google Scholar] [CrossRef]
- Kunimatsu, R.; Nakajima, K.; Awada, T.; Tsuka, Y.; Abe, T.; Ando, K.; Hiraki, T.; Kimura, A.; Tanimoto, K. Comparative characterization of stem cells from human exfoliated deciduous teeth, dental pulp, and bone marrow-derived mesenchymal stem cells. Biochem. Biophys. Res. Commun. 2018, 501, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Cavacas, M.A.; Machado, V.; Mendes, J.J. Dental stem cells: Recent progresses in tissue engineering and regenerative medicine. Ann. Med. 2017, 49, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Hamada, K.; Miura, M.; Yamaguchi, S. Neural crest stem cell property of apical pulp cells derived from human developing tooth. Cell Biol. Int. 2012, 36, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Gibon, E.; Lu, L.Y.; Nathan, K.; Goodman, S.B. Inflammation, ageing, and bone regeneration. J. Orthop. Translat. 2017, 10, 28–35. [Google Scholar] [CrossRef]
- Schrot, R.J.; Hubbard, J.R. Cannabinoids: Medical Implications. Ann. Med. 2016, 48, 128–141. [Google Scholar] [CrossRef]
- Fraguas-Sanchez, A.I.; Torres-Suarez, A.I. Medical Use of Cannabinoids. Drugs 2018, 78, 1665–1703. [Google Scholar] [CrossRef]
- Ibeas Bih, C.; Chen, T.; Nunn, A.V.; Bazelot, M.; Dallas, M.; Whalley, B.J. Molecular Targets of Cannabidiol in Neurological Disorders. Neurotherapeutics 2015, 12, 699–730. [Google Scholar] [CrossRef] [Green Version]
- Gui, H.; Tong, Q.; Qu, W.; Mao, C.-M.; Dai, S.-M. The Endocannabinoid System and Its Therapeutic Implications in Rheumatoid Arthritis. Int. Immunopharmacol. 2015, 26, 86–91. [Google Scholar] [CrossRef]
- Ofek, O.; Karsak, M.; Leclerc, N.; Fogel, M.; Frenkel, B.; Wright, K.; Tam, J.; Attar-Namdar, M.; Kram, V.; Shohami, E.; et al. Peripheral cannabinoid receptor, CB2, regulates bone mass. Proc. Natl. Acad. Sci. USA 2006, 103, 696–701. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Lu, H.-X.; Wang, J. Cannabinoid receptors in osteoporosis and osteoporotic pain: A narrative update of review. J. Pharm. Pharmacol. 2019, 71, 1469–1474. [Google Scholar] [CrossRef] [Green Version]
- Idris, A.I.; van’t Hof, R.J.; Greig, I.R.; Ridge, S.A.; Baker, D.; Ross, R.A.; Ralston, S.H. Regulation of bone mass, bone loss and osteoclast activity by cannabinoid receptors. Nat. Med. 2005, 11, 774–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehrenkranz, J.; Levine, M.A. Bones and Joints: The Effects of Cannabinoids on the Skeleton. J. Clin. Endocrinol. Metab. 2019, 104, 4683–4694. [Google Scholar] [CrossRef] [PubMed]
- Bab, I.; Zimmer, A. Cannabinoid receptors and the regulation of bone mass. Br. J. Pharmacol. 2008, 153, 182–188. [Google Scholar] [CrossRef]
- Argenziano, M.; Tortora, C.; Giulia Bellini, G.; Di Paola, A.; Punzo, F.; Rossi, F. The Endocannabinoid System in Pediatric Inflammatory and Immune Diseases. Int. J. Mol. Sci. 2019, 20, 5875. [Google Scholar] [CrossRef] [Green Version]
- The National Center for Biotechnology Information. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Cannabidiol (accessed on 7 October 2020).
- McAllister, S.D.; Murase, R.; Christian, R.T.; Lau, D.; Zielinski, A.J.; Allison, J.; Almanza, C.; Pakdel, A.; Lee, J.; Limbad, C.; et al. Pathways mediating the effects of cannabidiol on the reduction of breast cancer cell proliferation, invasion, and metastasis. Breast Cancer Res. Treat. 2011, 129, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Kamali, A.; Oryan, A.; Hosseini, S.; Ghanian, M.H.; Alizadeh, M.; Eslaminejad, M.B.; Baharvand, H. Cannabidiol-loaded microspheres incorporated into osteoconductive scaffold enhance mesenchymal stem cell recruitment and regeneration of critical-sized bone defects. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 101, 64–75. [Google Scholar] [CrossRef]
- Kato, H.; Ochiai-Shino, H.; Onodera, S.; Saito, A.; Shibahara, T.; Azuma, T. Promoting effect of 1,25(OH)2 vitamin D3 in osteogenic differentiation from induced pluripotent stem cells to osteocyte-like cells. Open Biol. 2015, 5, 140201. [Google Scholar] [CrossRef] [Green Version]
- Turner, A.G.; Hanrath, M.A.; Morris, H.A.; Atkins, G.J.; Anderson, P.H. The local production of 1,25(OH)2D3 promotes osteoblast and osteocyte maturation. J. Steroid Biochem. Mol. Biol. 2014, 144, 114–118. [Google Scholar] [CrossRef]
- Posa, F.; Di Benedetto, A.; Cavalcanti-Adam, E.A.; Colaianni, G.; Porro, C.; Trotta, T.; Brunetti, G.; Lo Muzio, L.; Grano, M.; Mori, G. Vitamin D Promotes MSC Osteogenic Differentiation Stimulating Cell Adhesion and αV β3 Expression. Stem. Cells Int. 2018, 2018, 6958713. [Google Scholar] [CrossRef]
- Centeno, E.G.Z.; Ferrua, C.P.; Nedel, F.; Tarquinio, S.B.C.; Demarco, F.F. Explant technique for the isolation of stem cell from the dental pulp of permanent teeth. BMC Proc. 2014, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Ferrua, C.P.; Centeno, E.G.Z.; Rosa, L.C.D.; Amaral, C.C.D.; Severo, R.F.; Sarkis-Onofre, R.; Nascimento, G.G.; Cordenonzi, G.; Bast, R.K.; Demarco, F.F.; et al. How has dental pulp stem cells isolation been conducted? A scoping review. Braz. Oral Res. 2017, 31, e87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egusa, H.; Sonoyama, W.; Nishimura, M.; Atsuta, I.; Akiyama, K. Stem Cells in Dentistry—Part I: Stem Cell Sources. J. Prosthodont. Res. 2012, 56, 151–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowran, A.; McKayed, K.; Campbell, V.A. The cannabinoid receptor type 1 is essential for mesenchymal stem cell survival and differentiation: Implications for bone health. Stem. Cells Int. 2013, 796715. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Wang, X.; Mittal, A.; Dhiman, S.; Hou, S.-Y.; Degenhardt, K.; Astrof, S. Mesodermal expression of integrin Œ±5Œ≤1 regulates neural crest development and cardiovascular morphogenesis. Dev. Biol. 2014, 395, 232–244. [Google Scholar] [CrossRef] [Green Version]
- Nanci, A. Ten Cate’s Oral Histology: Development, Structure and Function (Oral Anatomy), 7th ed.; Mosby: St. Louis, MO, USA, 2008; p. 411. [Google Scholar]
- Ashri, N.Y.; Ajlan, S.A.; Aldahmash, A.M. Dental pulp stem cells. Biology and use for periodontal tissue engineering. Saudi Med. J. 2015, 36, 1391–1399. [Google Scholar] [CrossRef]
- Dave, J.R.; Tomar, G.B. Dental Tissue-Derived Mesenchymal Stem Cells: Applications in Tissue Engineering. Crit. Rev. Biomed. Eng. 2018, 46, 429–468. [Google Scholar] [CrossRef]
- Chalisserry, E.P.; Nam, S.Y.; Park, S.H.; Anil, S. Therapeutic potential of dental stem cells. J. Tissue Eng. 2017, 8. [Google Scholar] [CrossRef]
- Rodriguez-Lozano, F.-J.; Insausti, C.-L.; Iniesta, F.; Blanquer, M.; Ramirez, M.-d.-C.; Meseguer, L.; Meseguer-Henarejos, A.-B.; Marin, N.; Martinez, S.; Moraleda, J.-M. Mesenchymal dental stem cells in regenerative dentistry. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e1062-7. [Google Scholar] [CrossRef] [Green Version]
- Gronthos, S.; Mankani, M.; Brahim, J.; Gehron Robey, P.; Shi, S. Postnatal human dental pulp stem cells (DPSCs) in vitro and in vivo. Proc. Natl. Acad. Sci. USA 2000, 97, 13625–13630. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Lozano, F.J.; Bueno, C.; Insausti, C.L.; Meseguer, L.; Ramirez, M.C.; Blanquer, M.; Marin, N.; Martinez, S.; Moraleda, J.M. Mesenchymal stem cells derived from dental tissues. Int. Endod. J. 2011, 44, 800–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin, S.; Sahin, F. Stem Cells Derived from Dental Tissues. Adv. Exp. Med. Biol. 2019, 1144, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-Y.; Choung, P.-H. USP1 Inhibitor ML323 Enhances Osteogenic Potential of Human Dental Pulp Stem Cells. Biochem. Biophys. Res. Commun. 2020, 530, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Ji, F.; Pan, J.; Shen, Z.; Yang, Z.; Wang, J.; Bai, X.; Tao, J. The Circular RNA circRNA124534 Promotes Osteogenic Differentiation of Human Dental Pulp Stem Cells through Modulation of the miR-496/β-Catenin Pathway. Front. Cell Dev. Biol. 2020, 8, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okajcekova, T.; Strnadel, J.; Pokusa, M.; Zahumenska, R.; Janickova, M.; Halasova, E.; Skovierova, H. A Comparative In Vitro Analysis of the Osteogenic Potential of Human Dental Pulp Stem Cells Using Various Differentiation Conditions. Int. J. Mol. Sci. 2020, 21, 2280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucaciu, O.; Soritau, O.; Gheban, D.; Rus Ciuca, D.; Virtic, O.; Vulpoi, A.; Dirzu, N.; Campian, R.; Baciut, G.; Popa, C.; et al. Dental Follicle Stem Cells in Bone Regeneration on Titanium Implants. BMC Biotechnol. 2015, 15, 114. [Google Scholar] [CrossRef] [Green Version]
- Rezai-Rad, M.; Bova, J.F.; Orooji, M.; Pepping, J.; Qureshi, A.; Del Piero, F.; Hayes, D.; Yao, S. Evaluation of Bone Regeneration Potential of Dental Follicle Stem Cells for Treatment of Craniofacial Defects. Cytotherapy 2015, 17, 1572–1581. [Google Scholar] [CrossRef] [Green Version]
- Jafar, H.; Abuarqoub, D.; Ababneh, N.; Hasan, M.; Al-Sotari, S.; Aslam, N.; Kailani, M.; Ammoush, M.; Shraideh, Z.; Awidi, A. hPL Promotes Osteogenic Differentiation of Stem Cells in 3D Scaffolds. PLoS ONE 2019, 14, e0215667. [Google Scholar] [CrossRef] [Green Version]
- Amirikia, M.; Jorsaraei, S.G.A.; Shariatzadeh, S.M.A.; Mehranjani, M.S. Differentiation of Stem Cells from the Apical Papilla into Osteoblasts by the Elastic Modulus of Porous Silk Fibroin Scaffolds. Biologicals 2019, 57, 1–8. [Google Scholar] [CrossRef]
- Schmuhl, E.; Ramer, R.; Salamon, A.; Peters, K.; Hinz, B. Increase of mesenchymal stem cell migration by cannabidiol via activation of p42/44 MAPK. Biochem. Pharmacol. 2014, 87, 489–501. [Google Scholar] [CrossRef]
- Hammell, D.C.; Zhang, L.P.; Ma, F.; Abshire, S.M.; McIlwrath, S.L.; Stinchcomb, A.L.; Westlund, K.N. Transdermal cannabidiol reduces inflammation and pain-related behaviours in a rat model of arthritis. Eur. J. Pain 2016, 20, 936–948. [Google Scholar] [CrossRef] [PubMed]
- Sainz-Cort, A.; Müller-Sánchez, C.; Espel, E. Anti-proliferative and cytotoxic effect of cannabidiol on human cancer cell lines in presence of serum. BMC Res. Notes 2020, 13, 389. [Google Scholar] [CrossRef]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants (Basel) 2019, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Polizzi, A.; Patini, R.; Ferlito, S.; Alibrandi, A.; Palazzo, G. Association among serum and salivary A. actinomycetemcomitans specific immunoglobulin antibodies and periodontitis. BMC Oral Health 2020, 20, 283. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Alibrandi, A.; Curro, M.; Matarese, M.; Ricca, S.; Matarese, G.; Ientile, R.; Kocher, T. Evaluation of salivary and serum ADMA levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J. Periodontol. 2020, 91, 1076–1084. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Iorio-Siciliano, V.; Alibrandi, A.; Ramaglia, L.; Leonardi, R. Effectiveness of a nutraceutical agent in the non-surgical periodontal therapy: A randomized, controlled clinical trial. Clin. Oral Investig. 2020. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NANOG left: | NANOG right: |
| 5′ CAGTCTGGACACTGGCTGAA 3′ | 5′ CACGTGGTTTCCAAACAAGA 3′ |
| ZFP42 left: | ZFP42 right: |
| 5′ GGCCTTCACTCTAGTAGTGCTCA 3′ | 5′ CTCCAGGCAGTAGTGATCTGAGT 3′ |
| VIM left: | VIM right: |
| 5′ TGGTCTAACGGTTTCCCCTA 3′ | 5′ GACCTCGGAGCGAGAGTG 3′ |
| POU5F1 left: | POU5F1 right: |
| 5′ TGAGTAGTCCCTTCGCAAGC 3′ | 5′ GAGAAGGCGAAATCCGAAG 3′ |
| GAPDH right (rw): | GAPDH left (fw): |
| 5′ GCATGGACTGTGGTCTGCAA 3′ | 5′ GGACTGAGGCTCCCACCTTT 3′ |
| ACTB left: 5′ TCCAAATATGAGATGCGTTGTT 3′ | ACTB right: 5′ TGCTATCACCTCCCCTGTGT 3′ |
| GAPDH left (rw): 5′ GCATGGACTGTGGTCTGCAA 3′ | GAPDH right (fw): 5′ GGACTGAGGCTCCCACCTTT 3′ |
| Osteonectin Left: 5′ TCTTCCCTGTACACTGGCAGTTC 3′ | Osteonectin Right: 5′ AGCTCGGTGTGGGAGAGGTA 3′ |
| Colagen1 Left: 5′ GGGATTCCCTGGACCTAAAG 3′ | Colagen1 Right: 5′ GGAACACCTCGCTCTCCA 3′ |
| Osteopontin Left: 5′ CAGTGACCAGTTCATCAGATTCATC 3′ | Osteopontin Right: 5′ CTAGGCATCACCTGTGCCATACC 3′ |
| Osteocalcin Left: 5′ ATGAGAGCCCTCACACTCCT 3′ | Osteocalcin Right: 5′ CAAGGGGAAGAGGAAAGAAG 3′ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrescu, N.B.; Jurj, A.; Sorițău, O.; Lucaciu, O.P.; Dirzu, N.; Raduly, L.; Berindan-Neagoe, I.; Cenariu, M.; Boșca, B.A.; Campian, R.S.; et al. Cannabidiol and Vitamin D3 Impact on Osteogenic Differentiation of Human Dental Mesenchymal Stem Cells. Medicina 2020, 56, 607. https://doi.org/10.3390/medicina56110607
Petrescu NB, Jurj A, Sorițău O, Lucaciu OP, Dirzu N, Raduly L, Berindan-Neagoe I, Cenariu M, Boșca BA, Campian RS, et al. Cannabidiol and Vitamin D3 Impact on Osteogenic Differentiation of Human Dental Mesenchymal Stem Cells. Medicina. 2020; 56(11):607. https://doi.org/10.3390/medicina56110607
Chicago/Turabian StylePetrescu, Nausica B., Ancuta Jurj, Olga Sorițău, Ondine P. Lucaciu, Noemi Dirzu, Lajos Raduly, Ioana Berindan-Neagoe, Mihai Cenariu, Bianca A. Boșca, Radu S. Campian, and et al. 2020. "Cannabidiol and Vitamin D3 Impact on Osteogenic Differentiation of Human Dental Mesenchymal Stem Cells" Medicina 56, no. 11: 607. https://doi.org/10.3390/medicina56110607