Polymorphism rs2066865 in the Fibrinogen Gamma Chain (FGG) Gene Increases Plasma Fibrinogen Concentration and Is Associated with an Increased Microvascular Thrombosis Rate

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Laboratory Workup
2.3. Genotyping
2.4. Data Statistical Analysis
3. Results
3.1. Clinical Course
3.2. The relationship between single nucleotide polymorphism rs2066865 in the FGG gene and free flap thrombotic complications.
3.3. The Relationship between Single Nucleotide Polymorphism rs2066865 in the FGG gene and Inflammatory Parameters and Platelet Count.
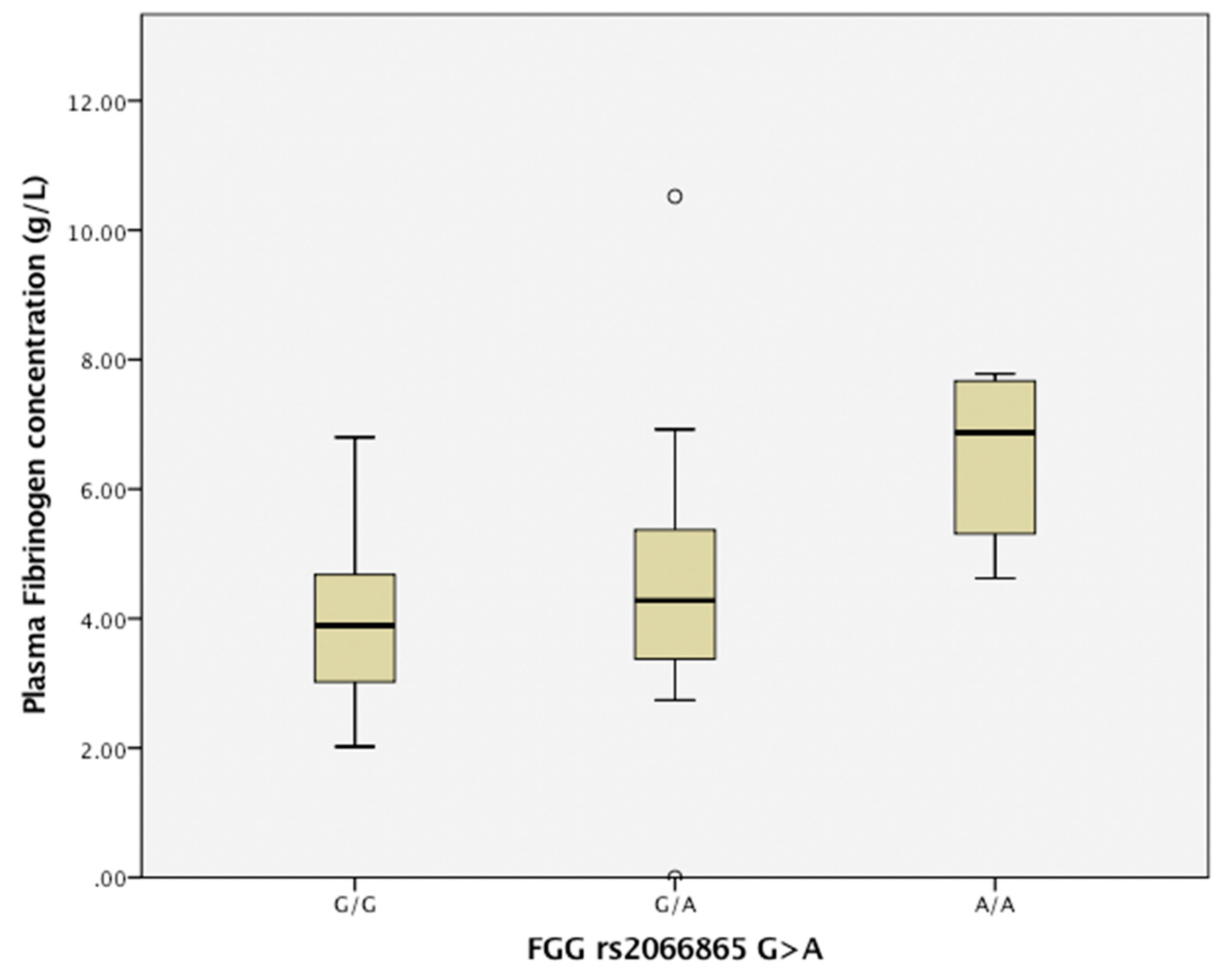
3.4. The Relationship between Single Nucleotide Polymorphism Rs2066865 in the FGG Gene and the Plasma Fibrinogen Level.
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Bowman, K.G.; Carty, M.J. Flap Complications and Thrombophilia: An Evidence-Based Model and Cost Analysis for Preoperative Screening. Open Access J. Plast. Surg. 2011, 11, 32. [Google Scholar]
- Friedman, T.; Coon, D.O.B.; Michaels, J.; Bontempo, F.; Young, V.L.; Clavijo, J.A.; Rubin, J.P. Hereditary coagulopathies: Practical diagnosis and management for the plastic surgeon. Plast. Reconstr. Surg. 2010, 125, 1544–1552. [Google Scholar] [CrossRef] [PubMed]
- Davison, S.P.; Kessler, C.M.; Al-Attar, A. Microvascular free flap failure caused by unrecognised hypercoagulability. Plast. Reconstr. Surg. 2009, 124, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Rosendaal, F.R. Venous thrombosis: A multicausal disease. Lancet 1993, 353, 1167–1173. [Google Scholar] [CrossRef]
- de Willige, S.U.; de Visser, M.C.; Houwing-Duistermaat, J.J.; Rosendaal, F.R.; Vos, H.L.; Bertina, R.M. Genetic variation in the fibrinogen gamma gene increases the risk for deep venous thrombosis by reducing plasma fibrinogen γ′ levels. Blood 2005, 106, 4176–4183. [Google Scholar] [CrossRef] [PubMed]
- Danesh, J.; Collins, R.; Appleby, P.; Peto, R. Association of fibrinogen, C-reactive protein, albumin or leukocyte count with coronary heart disease: Meta-analyses of prospective studies. JAMA 1998, 279, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Koenig, W. Fibrin (ogen) in cardiovascular disease: An update. Thromb. Haemost. 2003, 89, 601–609. [Google Scholar] [CrossRef]
- van Hylckama Vlieg, A.; Rosendaal, F.R. High levels of fibrinogen are associated with the risk of deep venous thrombsis mainly in the elderly. Thromb. Haemost. 2003, 1, 2677–2678. [Google Scholar] [CrossRef]
- Alexander, K.S.; Madden, T.E.; Farrell, D.H. Association between γ′ fibrinogen levels and inflammation. Thromb. Haemost. 2011, 105, 605–609. [Google Scholar] [CrossRef]
- Schlimp, C.J.; Ponschab, M.; Voelckel, W.; Treichl, B.; Maegele, M.; Schöchl, H. Fibrinogen levels in trauma patients during the first seven days after fibrinogen concentrate therapy: A retrospective study. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 29. [Google Scholar] [CrossRef]
- Tang, L.; Liu, K.; Wang, J.; Wang, C.; Zhao, P.; Liu, J. High preoperative plasma fibrinogen levels are associated with distant metastasis and impacted prognosis after curative resection in patients with colorectal cancer. J. Surg. Oncol. 2010, 102, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Falanga, A.; Piccioli, A. Cancer and venous thromboembolism. Lancet Oncol. 2005, 6, 401–410. [Google Scholar] [CrossRef]
- Henschen, A.; Lottspeich, F.; Kehl, M.; Southan, C. Covalent structure of fibrinogen. Ann. NY Acad. Sci. 1983, 408, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Kant, J.A.; Fornace, A.J.; Saxe, D.; Simon, M.I.; McBride, O.W.; Crabtree, G.R. Evaluation and organization of the fibrinogen locus on chromosome 4: Gene duplication by transposition and inversion. Proc. Natl. Acad. Sci. USA 1985, 82, 2344–2348. [Google Scholar] [CrossRef] [PubMed]
- El-Galaly, T.C.; Severinsen, M.T.; Overvad, K.; Steffensen, R.; Vistisen, A.K.; Tjønneland, A.; Kristensen, S.R. Single nucleotide poly morphisms and the risk of venous thrombosis: Results from a Danish case-cohort study. Br. J. Haemat. 2013, 160, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Farrell, D.H. γ′ Fibrinogen as a novel marker of thrombotic disease. Clin. Chem. Lab. Med. 2012, 50, 1903–1909. [Google Scholar] [CrossRef] [PubMed]
- Mackie, I.J.; Kitchen, S.; Machin, S.J.; Lowe, G.D.; Haemostasis and Thrombosis Task Force of the British Committee for Standards in Haematology. Guidelines on fibrinogen assays. Br. J. Haematol. 2003, 121, 396–404. [Google Scholar] [CrossRef] [Green Version]
- Livak, K.J. Allelic discrimination using fluorogenic probes and the 5′ nuclease assay. Genet. Anal. 1999, 14, 143–149. [Google Scholar] [CrossRef]
- Shechter, S.; Arad, E.; Inbal, A.; Friedman, O.; Gur, E.; Barnea, Y. DIEP flap breast reconstruction complication rate in previously irradiated internal mammary nodes. J. Reconstr. Microsurg. 2018, 6, 246–252. [Google Scholar] [CrossRef]
- Bendon, C.L.; Giele, H.P. Success of free flap anastomoses performed within the zone of trauma in acute lower limb reconstruction. J. Past. Reconstr. Aesthet. Surg. 2016, 69, 888–893. [Google Scholar] [CrossRef]
- Cho, E.H.; Bauder, A.R.; Centkowski, S.; Shammas, R.L.; Mundy, L.; Kovach, S.J.; Levin, L.S.; Hollenbeck, S.T. Preoperative platelet count predicts lower extremity free flap thrombosis: A multi-institutional experience. Plast. Reconstr. Surg. 2017, 139, 220–230. [Google Scholar] [CrossRef]
- Mateo, J.; Oliver, A.; Borrell, M.; Sala, N.; Fontcuberta, J.; EMET Group. Laboratory evaluation and clinical characteristics of 2132 consecutive unselected patients with venous thromboembolism—Results of the Spanish Multicentric Study on Throm bophilia (EMET-Study). Thromb. Haemost. 1997, 77, 444–451. [Google Scholar] [PubMed]
- Rosenblum, W.I. Effects of Dextran 40 on Blood Viscosity in Experimental Macroglobulinemia. Nature 1968, 218, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Robless, P.; Okonko, D.; Mikhailidis, D.P.; Stansby, G. Dextran 40 reduces in vitro platelet aggregation in peripheral arterial disease. Platelets 2004, 15, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Madjdpour, C.; Dettori, N.; Frascarolo, P.; Burki, M.; Boll, M.; Fisch, A.; Bombeli, T.; Spahn, D.R. Molecular weight of hydroxyethyl starch: Is there an effect on blood coagulation and pharmacokinetics? Br. J. Anaesth. 2005, 94, 569–576. [Google Scholar] [CrossRef]
- Pannuci, C.J.; Kovach, S.J.; Cuker, A. Microsurgery and the hyper coagulable state: A haematologist’s perspective. Plast. Reconstr. Surg. 2015, 4, 545–552. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| SNP rs2066865 (G > A) In the fibrinogen gamma chain (FGG) Gene | G/G n = 79 | G/A n = 22 | A/A n = 3 |
|---|---|---|---|
| Age (M ± SD) | 39.62 (13.03) | 46.21 (12.49) | 52.0 (14.39) |
| Sex, female | 7 (8.8) | 4 (18.1) | 1 (33.3) |
| Free flap thrombosis | 6 (7.59) | 5 (22.7) | 1 (33.3) |
| History of thrombosis: | 2 (2.53) | 3 (13.6) | 2 (66.7) |
| arterial (MI; CI) | 2 (2.53) | - | |
| venous (DVT; PATE) | - | 3 (13.6) | 2 (66.7) |
| Family history of thrombosis | 7 (8.9) | 3 (13.6) | 2 (66.7) |
| arterial (MI; CI) | 5 (6.37) | - | - |
| venous (DVT; PATE) | 2 (2.53) | 3 (13.6) | 2 (66.7) |
| Medication | |||
| antithrombotics | 2 (2.53) | 1 (4.5) | 3 (100) |
| oral contraceptives | - | 1 (4.5) | - |
| Smoking | 22 (27.8) | 15 (68.1) | 3 (100) |
| Metabolic disturbances ∗ | 8 (10.1) | 2 (9.1) | 1 (33.3) |
| Alcohol abuse | 6 (7.6) | 1 (4.54) | 1 (33.3) |
| Defect etiology: trauma | 32 (41) | 12 (54.5) | 43(100) |
| recent trauma, (<30 d) | 22 (27.8) | 8 (36.3) | 2 (66.7) |
| polytrauma | 6 (7.6) | 2 (9.1) | - |
| chronic inflammation | 15 (19) | 10 (45.5) | 1 (33.3) |
| malignancy | 4 (5.1) | 4 (18.2) | 1 (33.3) |
| burn | 1 (1.3) | 1 (4.5) | - |
| Flap | Etiology | Defect Localization | Time to Thrombosis | Thrombosis Venue | Re-Anastomosis | Flap Necrosis | Salvage Measure |
|---|---|---|---|---|---|---|---|
| Scapular/Parascapular | osteomyelitis | lower extremity | 18 h | venous | yes | no | additional vein anastomosis |
| Medial plantar artery flap | osteomyelitis | lower extremity | no data | arterial | yes | no | additional vein anastomosis |
| LAF | trauma | lower extremity | 23 h 55 min | venous | yes | no | additional vein anastomosis |
| Scapular/Parascapular | osteomyelitis | lower extremity | 23 h 30 min | venous | yes | no | - |
| Scapular/Parascapular | polytrauma | lower extremity | 23 h 15 min | venous | yes | yes | additional vein anastomosis |
| Sartorius free flap | trauma | lower extremity | no data | arterial and venous | no | yes | NPWT; STSG |
| Osteocutaneus FF | trauma | lower extremity | 120 h | arterial and venous | yes | yes | local muscle flap and STSG |
| Osteocutaneus FF | osteomyelitis | lower extremity | 144 h | arterial and venous | yes | yes | local flap |
| Serratus anterior muscle flap | osteomyelitis | lower extremity | 74 h 20 min | arterial and venous | yes | yes | NPWT; STSG |
| RFF | malignancy | orofacial | 13 h 10 min | arterial | yes | yes | local flap |
| LAF | trauma | upper extremity | no data | venous | yes | yes | ALT flap |
| Scapular/Parascapular | trauma | lower extremity | 49 h | venous | no | yes | local flap; STSG |
| SNP (Gene) | Genotypes | Thrombosis Group | Non-Thrombosis Group | OR (CI, 95%) a | p |
|---|---|---|---|---|---|
| rs2066865 in FGG | GG/GA/AA | 6/5/1 | 73/17/2 | 0.30 (0.044 to 0.57) | 0.016 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drizlionoka, K.; Zariņš, J.; Ozoliņa, A.; Ņikitina-Zaķe, L.; Mamaja, B. Polymorphism rs2066865 in the Fibrinogen Gamma Chain (FGG) Gene Increases Plasma Fibrinogen Concentration and Is Associated with an Increased Microvascular Thrombosis Rate. Medicina 2019, 55, 563. https://doi.org/10.3390/medicina55090563
Drizlionoka K, Zariņš J, Ozoliņa A, Ņikitina-Zaķe L, Mamaja B. Polymorphism rs2066865 in the Fibrinogen Gamma Chain (FGG) Gene Increases Plasma Fibrinogen Concentration and Is Associated with an Increased Microvascular Thrombosis Rate. Medicina. 2019; 55(9):563. https://doi.org/10.3390/medicina55090563
Chicago/Turabian StyleDrizlionoka, Karina, Jānis Zariņš, Agnese Ozoliņa, Liene Ņikitina-Zaķe, and Biruta Mamaja. 2019. "Polymorphism rs2066865 in the Fibrinogen Gamma Chain (FGG) Gene Increases Plasma Fibrinogen Concentration and Is Associated with an Increased Microvascular Thrombosis Rate" Medicina 55, no. 9: 563. https://doi.org/10.3390/medicina55090563