Distribution and Characteristics of Hypouricemia within the Japanese General Population: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
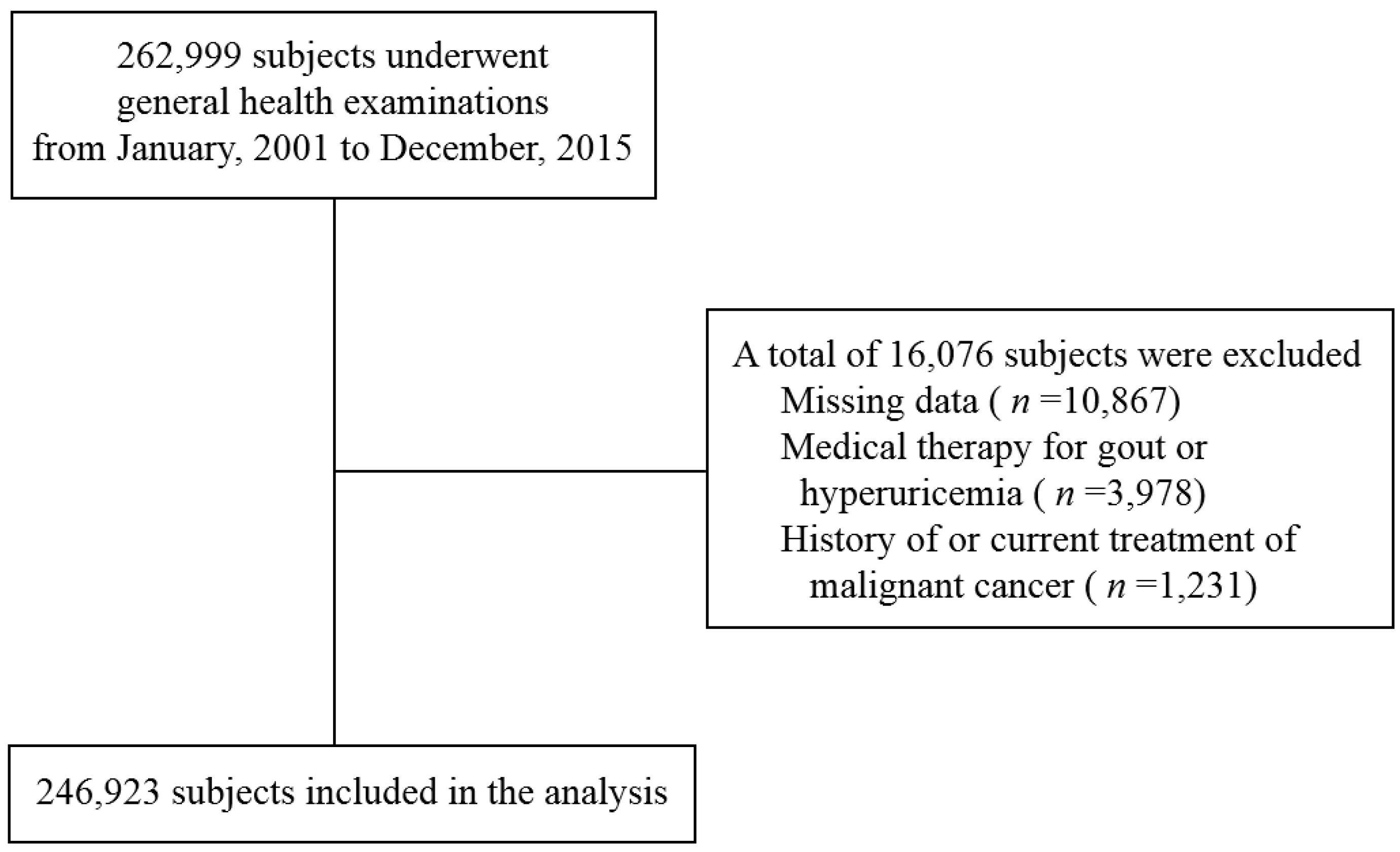
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
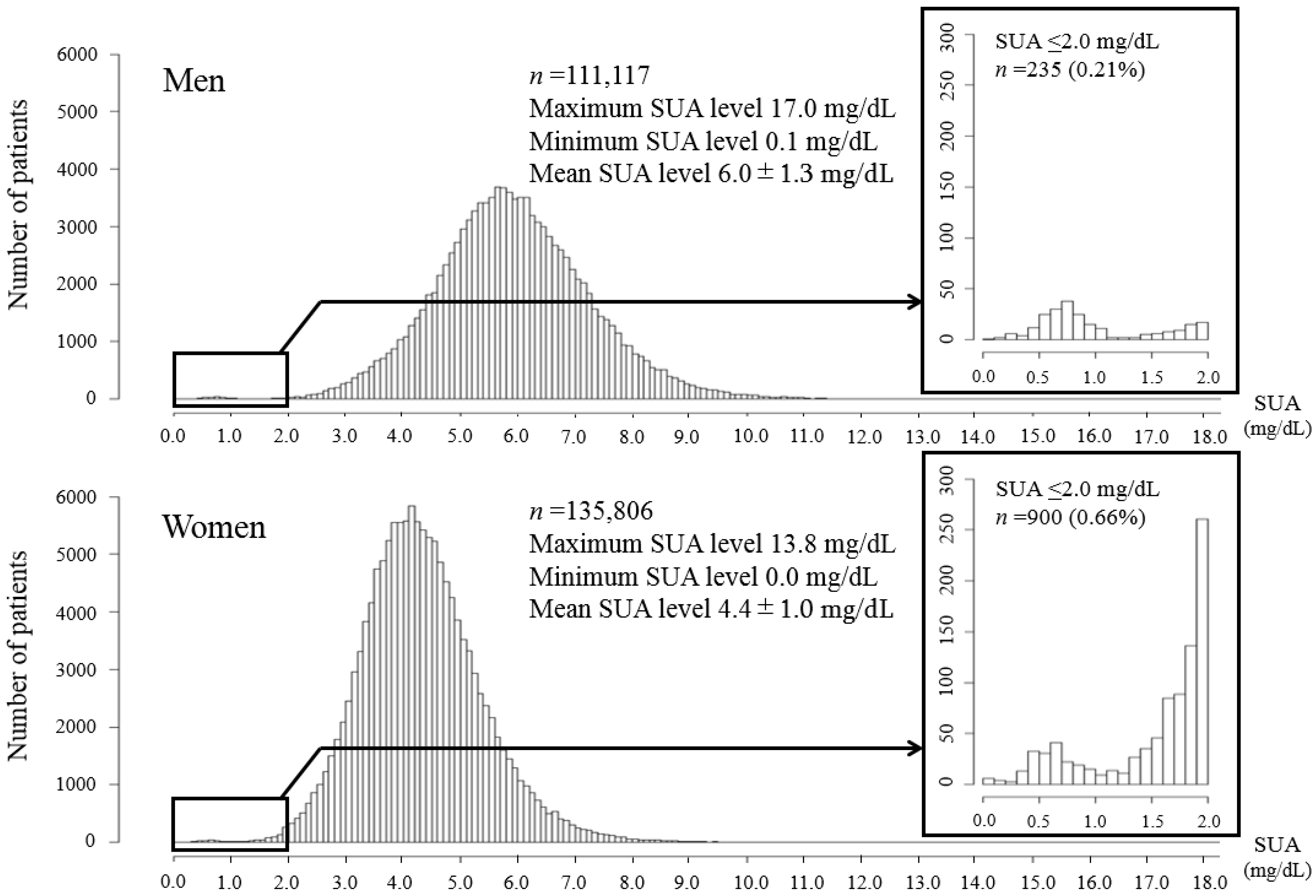
3.1. Prevalence of Hypouricemia
3.2. Two Hypouricemia Distributions
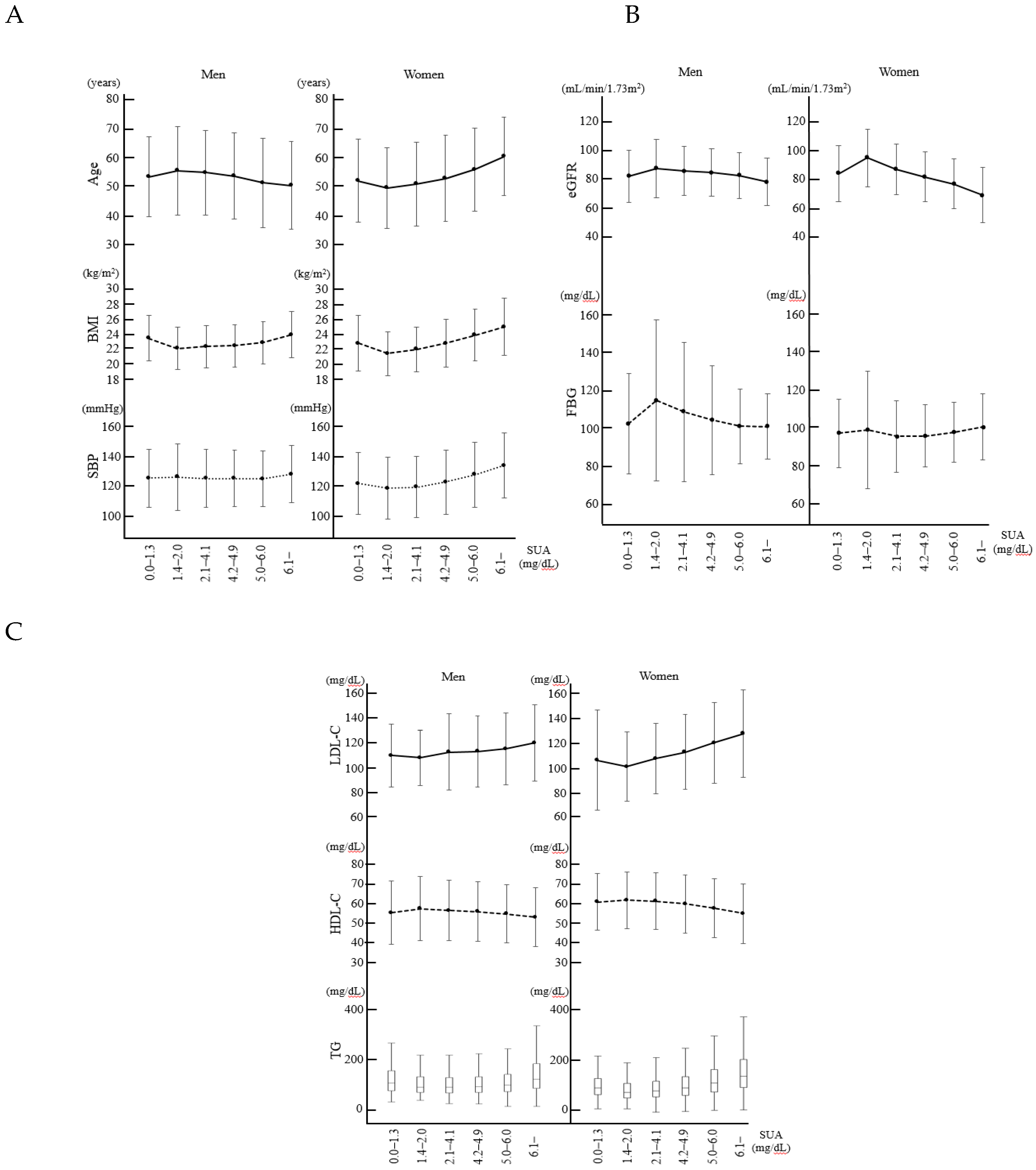
3.3. Characteristics of the Study Population Categorized According to the Serum Uric Acid Levels
3.4. Characteristics in the Lower and Higher Hypouricemia Groups
3.5. Possible Cardiovascular Risks Associated with the Bottom of the J-Shaped Curve
4. Discussion
4.1. Prevalence of Hypouricemia
4.2. Difference of the Characteristics between the Two Groups of Hypouricemia
4.3. SUA Values Associated with the Bottom of Cardiovascular Risks
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Esparza, M.N.; García, N.V. Hypouricemia and tubular transport of uric acid. Nefrologia 2011, 31, 44–50. [Google Scholar]
- Sebesta, I.; Stiburkova, B.; Bartl, J.; Ichida, K.; Hosoyamada, M.; Taylor, J.; Marinaki, A. Diagnostic tests for primary renal hypouricemia. Nucleosides Nucleotides Nucleic Acids 2011, 30, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, Y.; Koga, H.; Yasutomo, Y.; Kawabata, Y.; Shimizu, E.; Naruse, M.; Kiyama, S.; Nonoguchi, H.; Tomita, K.; Sasatomi, Y.; et al. Patients with renal hypouricemia with exercise-induced acute renal failure and chronic renal dysfunction. Clin Nephrol. 2000, 53, 467–472. [Google Scholar]
- Ohta, T.; Sakano, T.; Igarashi, T.; Itami, N.; Ogawa, T.; ARF Assocoated with Renal Hypouricemia Research Group. Exercise-induced acute renal failure associated with renal hypouricaemia: results of a questionnaire-based survey in Japan. Nephrol. Dial. Transplant. 2004, 19, 1447–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enomoto, A.; Kimura, H.; Chairoungdua, A.; Shigeta, Y.; Jutabha, P.; Cha, S.H.; Hosoyamada, M.; Takeda, M.; Sekine, T.; Igarashi, T.; et al. Molecular identification of a renal urate anion exchanger that regulates blood urate levels. Nature 2002, 417, 447–452. [Google Scholar] [CrossRef]
- Matsuo, H.; Chiba, T.; Nagamori, S.; Nakayama, A.; Domoto, H.; Phetdee, K.; Wiriyasermkul, P.; Kikuchi, Y.; Oda, T.; Nishiyama, J. Mutations in glucose transporter 9 gene SLC2A9 cause renal hypouricemia. Am. J. Hum. Genet. 2008, 83, 744–751. [Google Scholar] [CrossRef]
- Bos, M.J.; Koudstaal, P.J.; Hofman, A.; Witteman, J.C.; Breteler, M.M. Uric acid is a risk factor for myocardial infarction and stroke: The Rotterdam study. Stroke 2006, 37, 1503–1507. [Google Scholar] [CrossRef] [PubMed]
- Tamariz, L.; Harzand, A.; Palacio, A.; Verma, S.; Jones, J.; Hare, J. Uric acid as a predictor of all-cause mortality in heart failure: A meta-analysis. Congest Heart Fail. 2011, 17, 25–30. [Google Scholar] [CrossRef]
- Kuwabara, M.; Niwa, K.; Ohtahara, A.; Hamada, T.; Miyazaki, S.; Mizuta, E.; Ogino, K.; Hisatome, I. Prevalence and complications of hypouricemia in a general population: A large-scale cross-sectional study in Japan. PLoS ONE 2017, 12, e0176055. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Bugdayci, G.; Balaban, Y.; Sahin, O. Causes of hypouricemia among outpatients. Lab. Med. 2008, 39, 550–552. [Google Scholar] [CrossRef]
- Son, C.N.; Kim, J.M.; Kim, S.H.; Cho, S.K.; Choi, C.B.; Sung, Y.K.; Kim, T.H.; Bae, S.C.; Yoo, D.H.; Jun, J.B. Prevalence and possible causes of hypouricemia at a tertiary care hospital. Korean J. Intern. Med. 2016, 31, 971–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakasugi, M.; Kazama, J.J.; Narita, I.; Konta, T.; Fujimoto, S.; Iseki, K.; Moriyama, T.; Yamagata, K.; Tsuruya, K.; Asahi, K.; et al. Association between hypouricemia and reduced kidney function: A cross-sectional population-based study in Japan. Am. J. Nephrol. 2015, 41, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, S.; Hisatome, I.; Kuwabara, M.; Niwa, K.; Maharani, N.; Kato, M.; Ogino, K.; Hamada, T.; Ninomiya, H.; Higashi, Y.; et al. Depletion of Uric Acid Due to SLC22A12 (URAT1) Loss-of-Function Mutation Causes Endothelial Dysfunction in Hypouricemia. Circ. J. 2015, 79, 1125–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeun, J.Y.; Hasbargen, J.A. Renal hypouricemia: prevention of exercise-induced acute renal failure and a review of the literature. Am. J. Kidney Dis. 1995, 25, 937–946. [Google Scholar] [CrossRef]
- Komoda, F.; Sekine, T.; Inatomi, J.; Enomoto, A.; Endou, H.; Ota, T.; Matsuyama, T.; Ogata, T.; Ikeda, M.; Awazu, M.; et al. The W258X mutation in SLC22A12 is the predominant cause of Japanese renal hypouricemia. Pediatr. Nephrol. 2004, 19, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Ichida, K.; Hosoyamada, M.; Hisatome, I.; Enomoto, A.; Hikita, M.; Endou, H.; Hosoya, T. Clinical and molecular analysis of patients with renal hypouricemia in Japan-influence of URAT1 gene on urinary urate excretion. J. Am. Soc. Nephrol. 2004, 15, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Siener, R.; Hesse, A. The effect of a vegetarian and different omnivorous diets on urinary risk factors for uric acid stone formation. Eur. J. Nutr. 2003, 42, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Szeto, Y.T.; Kwok, T.C.; Benzie, I.F. Effects of a long-term vegetarian diet on biomarkers of antioxidant status and cardiovascular disease risk. Nutrition 2004, 20, 863–866. [Google Scholar] [CrossRef] [PubMed]
- Ramsdell, C.M.; Kelley, W.N. The clinical significance of hypouricemia. Ann. Intern. Med. 1973, 78, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Hisatome, I.; Ogino, K.; Kotake, H.; Ishiko, R.; Saito, M.; Hasegawa, J.; Mashiba, H.; Nakamoto, S. Cause of persistent hypouricemia in outpatients. Nephron 1989, 51, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Schillaci, G.; Reboldi, G.; Santeusanio, F.; Porcellati, C.; Brunetti, P. Relation between serum uric acid and risk of cardiovascular disease in essential hypertension. The PIUMA study. Hypertension 2000, 36, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Mazza, A.; Zamboni, S.; Rizzato, E.; Pessina, A.C.; Tikhonoff, V.; Schiavon, L.; Casiglia, E. Serum uric acid shows a J-shaped trend with coronary mortality in non-insulin-dependent diabetic elderly people. The CArdiovascular STudy in the ELderly (CASTEL). Acta Diabetol. 2007, 44, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Ames, B.N.; Cathcart, R.; Schwiers, E.; Hochstein, P. Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: A hypothesis. Proc. Natl. Acad. Sci. USA 1981, 78, 6858–6862. [Google Scholar] [CrossRef] [PubMed]
- Hedayat, M.; Mahmoudi, M.J.; Rose, N.R.; Rezaei, N. Proinflammatory cytokines in heart failure: double-edged swords. Heart Fail. Rev. 2010, 15, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Nishikura, T.; Koba, S.; Yokota, Y.; Hirano, T.; Tsunoda, F.; Shoji, M.; Hamazaki, Y.; Suzuki, H.; Itoh, Y.; Katagiri, T.; et al. Elevated small dense low-density lipoprotein cholesterol as a predictor for future cardiovascular events in patients with stable coronary artery disease. J. Atheroscler. Thromb. 2014, 21, 755–767. [Google Scholar] [CrossRef] [PubMed]
- Assmann, G.; Schulte, H.; von Eckardstein, A. Hypertriglyceridemia and elevated lipoprotein(a) are risk factors for major coronary events in middle-aged men. Am. J. Cardiol. 1996, 77, 1179–1184. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Men | |||||||
| SUA | |||||||
| First Quartile | Second Quartile | Third Quartile | Fourth Quartile | P Value | |||
| Lower Hypouricemia Group | Higher Hypouricemia Group | ||||||
| 0.0–1.3 mg/dL | 1.4–2.0 mg/dL | 2.1–4.1 mg/dL | 4.2–4.9 mg/dL | 5.0–6.0 mg/dL | ≥6.1 mg/dL | ||
| n = 173 | n = 62 | n = 8402 | n = 14,918 | n = 36,811 | n = 50,751 | ||
| Age (years) | 53.5 ± 13.7 | 55.6 ± 15.2 | 54.9 ± 14.5 | 53.7 ± 14.8 | 51.4 ± 15.3 | 50.5 ± 15.0 | <0.001 |
| BMI (kg/m2) | 23.4 ± 3.1 | 22.0 ± 2.9 | 22.3 ± 2.9 | 22.3 ± 2.9 | 22.8 ± 2.9 | 23.9 ± 3.2 | <0.001 |
| SBP (mmHg) | 124.9 ± 20.2 | 125.7 ± 23.1 | 124.7 ± 20.0 | 124.6 ± 19.6 | 124.5 ± 19.4 | 127.5 ± 19.8 | <0.001 |
| TP (g/dL) | 7.5 ± 0.5 | 7.4 ± 0.4 | 7.4 ± 0.5 | 7.4 ± 0.5 | 7.5 ± 0.5 | 7.6 ± 0.5 | <0.001 |
| AST (IU/L) | 25 {20,31} | 23 {18,30.25} | 23 {19,28} | 23 {19,28} | 23 {19,29} | 25 {21,32} | <0.001 |
| ALT (IU/L) | 19 {14,30.5} | 18 {13.75,24.25} | 18 {13,24} | 18 {13,24} | 18 {14,26} | 22 {15,32} | <0.001 |
| T-bil (mg/dL) | 0.83 ± 0.38 | 0.84 ± 0.45 | 0.82 ± 0.36 | 0.80 ± 0.35 | 0.81 ± 0.36 | 0.81 ± 0.36 | 0.065 |
| eGFR (mL/min.1.73 m2) | 81.9 ± 18.6 | 87.5 ± 20.6 | 85.5 ± 17.4 | 84.5 ± 16.7 | 82.4 ± 16.4 | 78.1 ± 17.0 | <0.001 |
| TC (mg/dL) | 193.1 ± 35.4 | 193.6 ± 36.3 | 193.5 ± 34.8 | 193.7 ± 34.4 | 195.2 ± 34.6 | 202.1 ± 36.5 | <0.001 |
| TG (mg/dL) | 104 {73.5,152.5} | 88 {65.75,128} | 88 {65.5,125} | 89 {66,128} | 95 {69,138} | 119 {82,182} | <0.001 |
| LDL-C (mg/dL) | 109.3 ± 25.8 | 107.4 ± 22.9 | 112.2 ± 31.5 | 112.6 ± 29.2 | 114.8 ± 29.5 | 119.8 ± 31.4 | <0.001 |
| HDL-C (mg/dL) | 55.5 ± 15.8 | 57.5 ± 15.9 | 56.6 ± 14.9 | 56.1 ± 14.8 | 55.0 ± 14.6 | 53.2 ± 14.6 | <0.001 |
| FBG (mg/dL) | 102.4 ± 26.9 | 114.9 ± 43.4 | 108.7 ± 37.7 | 104.3 ± 29.5 | 101.0 ± 20.1 | 100.9 ± 17.5 | <0.001 |
| Current smoking, n (%) | 77 (44.5) | 25 (40.3) | 3,649 (43.4) | 6,835 (45.8) | 16,926 (46.0) | 22,416 (44.2) | <0.001 |
| Frequent alcohol drinker, n (%) | 97 (56.1) | 32 (51.6) | 4,396 (52.3) | 7,944 (53.2) | 20,480 (55.6) | 31,870 (62.8) | <0.001 |
| Medication for hypertension, n (%) | 18 (10.4) | 9 (14.5) | 776 (9.2) | 1,300 (8.7) | 3,454 (9.4) | 6,581 (13.0) | <0.001 |
| Medication for diabetes, n (%) | 4 (2.3) | 5 (8.1) | 368 (4.4) | 526 (3.5) | 779 (2.1) | 664 (1.3) | <0.001 |
| Medication for dyslipidemia, n (%) | 5 (2.9) | 0 (0.0) | 107 (1.3) | 150 (1.0) | 408 (1.1) | 797 (1.6) | <0.001 |
| Women | |||||||
| SUA | |||||||
| First quartile | Second Quartile | Third Quartile | Fourth Quartile | P Value | |||
| Lower Hypouricemia Group | Higher Hypouricemia Group | ||||||
| 0.0–1.3 mg/dL | 1.4–2.0 mg/dL | 2.1–4.1 mg/dL | 4.2–4.9 mg/dL | 5.0–6.0 mg/dL | ≥6.1 mg/dL | ||
| n = 221 | n = 679 | n = 58,697 | n = 40,966 | n = 26,941 | n = 8,302 | ||
| Age (years) | 52.1 ± 14.2 | 49.6 ± 13.7 | 51.0 ± 14.2 | 52.9 ± 14.7 | 55.9 ± 14.2 | 60.3 ± 13.3 | <0.001 |
| BMI (kg/m2) | 22.8 ± 3.7 | 21.4 ± 2.9 | 22.0 ± 3.0 | 22.8 ± 3.2 | 23.9 ± 3.5 | 25.0 ± 3.8 | <0.001 |
| SBP (mmHg) | 121.7 ± 20.6 | 118.6 ± 20.7 | 119.4 ± 20.3 | 122.7 ± 21.3 | 127.7 ± 21.8 | 133.8 ± 21.9 | <0.001 |
| TP (g/dL) | 7.6 ± 0.5 | 7.5 ± 0.5 | 7.6 ± 0.5 | 7.6 ± 0.5 | 7.7 ± 0.5 | 7.8 ± 0.5 | <0.001 |
| AST (IU/L) | 21 {17,25} | 19 {16,23} | 20 {17,24} | 21 {18,25} | 22 {19,27} | 24 {20,29} | <0.001 |
| ALT (IU/L) | 15 {11,20} | 12 {9,17} | 13 {10,17} | 14 {11,19} | 16 {12,22} | 18 {13,25} | <0.001 |
| T-bil (mg/dL) | 0.75 ± 0.28 | 0.74 ± 0.33 | 0.74 ± 0.30 | 0.74 ± 0.30 | 0.73 ± 0.29 | 0.72 ± 0.29 | <0.001 |
| eGFR (mL/min/1.73 m2) | 83.4 ± 19.4 | 94.3 ± 19.9 | 86.3 ± 17.7 | 81.1 ± 17.3 | 76.3 ± 17.2 | 68.3 ± 19.3 | <0.001 |
| TC (mg/dL) | 204.3 ± 35.2 | 195.2 ± 34.7 | 200.6 ± 35.6 | 206.8 ± 36.4 | 213.5 ± 37.2 | 219.8 ± 38.5 | <0.001 |
| TG (mg/dL) | 84 {62.5,111} | 70 {54,96} | 75 {56,103} | 84 {61,117} | 98 {71,138} | 118 {85,169} | <0.001 |
| LDL-C (mg/dL) | 105.8 ± 41.4 | 100.5 ± 28.8 | 107.2 ± 29.3 | 112.6 ± 30.9 | 120.4 ± 33.5 | 128.1 ± 36.2 | <0.001 |
| HDL-C (mg/dL) | 61.1 ± 14.2 | 62.0 ± 14.2 | 61.5 ± 14.2 | 60.1 ± 14.5 | 58.0 ± 14.6 | 55.3 ± 14.9 | <0.001 |
| FBG (mg/dL) | 97.7 ± 18.6 | 99.5 ± 31.9 | 96.0 ± 19.5 | 96.3 ± 16.7 | 98.1 ± 16.2 | 101.0 ± 17.9 | <0.001 |
| Current smoking, n (%) | 12 (5.4) | 34 (5.0) | 2,776 (4.7) | 2,123 (5.2) | 1,426 (5.3) | 468 (5.6) | <0.001 |
| Frequent alcohol drinker, n (%) | 24 (10.9) | 42 (6.2) | 4,362 (7.4) | 3,641 (8.9) | 2,676 (9.9) | 909 (11.0) | <0.001 |
| Medication for hypertension, n (%) | 30 (13.6) | 66 (9.7) | 4,661 (7.9) | 5,003 (12.2) | 5,231 (19.4) | 2,729 (32.9) | <0.001 |
| Medication for diabetes, n (%) | 3 (1.4) | 18 (2.7) | 794 (1.4) | 465 (1.1) | 392 (1.5) | 154 (1.9) | <0.001 |
| Medication for dyslipidemia, n (%) | 3 (1.4) | 12 (1.8) | 1,171 (2.0) | 1,158 (2.8) | 1,139 (4.2) | 464 (5.6) | <0.001 |
| Men | |||
| SUA 0.0–2.0 mg/dL | SUA ≥ 2.1 mg/dL | PValue | |
| n = 235 | n = 110882 | ||
| Age (years) | 54.0 ± 14.1 | 51.6 ± 15.1 | 0.012 |
| BMI (kg/m2) | 23.1 ± 3.1 | 23.2 ± 3.1 | 0.420 |
| SBP (mmHg) | 125.1 ± 21.0 | 125.9 ± 19.7 | 0.526 |
| TP (g/dL) | 7.5 ± 0.5 | 7.5 ± 0.5 | 0.170 |
| AST (IU/L) | 24 {19,31} | 24 {20,30} | 0.802 |
| ALT (IU/L) | 18 {14,29} | 19 {14,28} | 0.323 |
| T-bil (mg/dL) | 0.83 ± 0.40 | 0.81 ± 0.36 | 0.347 |
| TC (mg/dL) | 193.3 ± 35.6 | 198.0 ± 35.7 | 0.042 |
| TG (mg/dL) | 98 {71,148} | 103 {73,154} | 0.220 |
| LDL-C (mg/dL) | 113.4 ± 30.7 | 116.6 ± 34.5 | 0.154 |
| HDL-C (mg/dL) | 56.0 ± 15.8 | 54.5 ± 14.7 | 0.101 |
| FBG (mg/dL) | 105.7 ± 32.4 | 102.0 ± 22.7 | 0.013 |
| Current smoking, n (%) | 102 (43.4) | 49,826 (44.9) | 0.637 |
| Frequent alcohol drinker, n (%) | 129 (54.9) | 64,690 (58.3) | 0.284 |
| Medication for hypertension, n (%) | 27 (11.5) | 12,111 (10.9) | 0.781 |
| Medication for diabetes, n (%) | 9 (3.8) | 2337 (2.1) | 0.067 |
| Medication for dyslipidemia, n (%) | 5 (2.1) | 1462 (1.3) | 0.278 |
| eGFR (mL/min.1.73 m2) | 83.4 ± 19.2 | 81.0 ± 17.0 | 0.029 |
| Women | |||
| SUA 0.0–2.0 mg/dL | SUA ≥ 2.1 mg/dL | P value | |
| n = 900 | n = 134906 | ||
| Age (years) | 50.2 ± 13.9 | 53.2 ± 14.5 | <0.001 |
| BMI (kg/m2) | 21.8 ± 3.1 | 22.8 ± 3.3 | <0.001 |
| SBP (mmHg) | 119.4 ± 20.7 | 123.0 ± 21.4 | <0.001 |
| TP (g/dL) | 7.5 ± 0.5 | 7.6 ± 0.5 | <0.001 |
| AST (IU/L) | 21 {18,25} | 20 {16.25,24} | <0.001 |
| ALT (IU/L) | 13 {10,17} | 14 {11,19} | <0.001 |
| T-bil (mg/dL) | 0.74 ± 0.32 | 0.74 ± 0.30 | 0.654 |
| TC (mg/dL) | 197.4 ± 35.0 | 206.2 ± 36.9 | <0.001 |
| TG (mg/dL) | 74 {56.25,102} | 84 {61,118} | <0.001 |
| LDL-C (mg/dL) | 118.6 ± 30.7 | 126.6 ± 33.4 | <0.001 |
| HDL-C (mg/dL) | 61.8± 14.2 | 60.0 ± 14.6 | <0.001 |
| FBG (mg/dL) | 99.1 ± 29.2 | 96.8 ± 18.0 | <0.001 |
| Current smoking, n (%) | 46 (5.1) | 6793 (5.0) | 0.918 |
| Frequent alcohol drinker, n (%) | 66 (7.3) | 11,588 (8.6) | 0.180 |
| Medication for hypertension, n (%) | 96 (10.7) | 17,624 (13.1) | 0.033 |
| Medication for diabetes, n (%) | 21 (2.3) | 1805 (1.3) | 0.010 |
| Medication for dyslipidemia, n (%) | 15 (1.7) | 3932 (2.9) | 0.026 |
| eGFR (mL/min.1.73 m2) | 91.6 ± 20.3 | 81.6 ± 18.3 | <0.001 |
| Men | ||||||
| SUA 0.0–1.3 mg/dL (A) | SUA 1.4–2.0 mg/dL (B) | SUA ≥ 2.1 mg/dL (C) | Comparison I (A) vs. (B) | Comparison II (A) vs. (C) | Comparison III (B) vs. (C) | |
| n = 173 | n = 62 | n = 110,882 | P Value | P Value | P Value | |
| Age (years) | 53.5 ± 13.7 | 55.6 ± 15.2 | 51.6 ± 15.1 | 0.295 | 0.099 | 0.033 |
| BMI (kg/m2) | 23.4 ± 3.1 | 22.0 ± 2.9 | 23.2 ± 3.1 | 0.002 | 0.365 | 0.002 |
| SBP (mmHg) | 124.9 ± 20.2 | 125.7 ± 23.1 | 125.9 ± 19.7 | 0.795 | 0.492 | 0.928 |
| TP (g/dL) | 7.5 ± 0.5 | 7.4 ± 0.4 | 7.5 ± 0.5 | 0.292 | 0.507 | 0.117 |
| AST (IU/L) | 25 {20,31} | 23 {18,30.25} | 24 {20,30} | 0.337 | 0.452 | 0.442 |
| ALT (IU/L) | 19 {14,30.5} | 18 {13.75,24.25} | 19 {14,28} | 0.344 | 0.751 | 0.162 |
| T-bil (mg/dL) | 0.82 ± 0.38 | 0.84 ± 0.45 | 0.81 ± 0.36 | 0.810 | 0.503 | 0.476 |
| TC (mg/dL) | 193.1 ± 34.5 | 193.6 ± 36.3 | 198.0 ± 35.7 | 0.936 | 0.073 | 0.327 |
| TG (mg/dL) | 104 {73.5,152.5} | 88 {65.75,128} | 103 {73,154} | 0.045 | 0.935 | 0.024 |
| LDL-C (mg/dL) | 112.6 ± 29.9 | 115.5 ± 32.9 | 116.6 ± 34.5 | 0.523 | 0.130 | 0.807 |
| HDL-C (mg/dL) | 55.5 ± 15.8 | 57.5 ± 15.9 | 54.5 ± 14.7 | 0.413 | 0.339 | 0.109 |
| FBG (mg/dL) | 102.4 ± 26.9 | 114.9 ± 43.4 | 102.0 ± 22.7 | 0.009 | 0.802 | <0.001 |
| Current smoking, n (%) | 77 (44.5) | 25 (40.3) | 49,826 (44.9) | 0.568 | 0.910 | 0.465 |
| Frequent alcohol drinker, n (%) | 97 (56.1) | 32 (51.6) | 64,690 (58.3) | 0.545 | 0.545 | 0.283 |
| Medication for hypertension, n (%) | 18 (10.4) | 9 (14.5) | 12,111 (10.9) | 0.384 | 0.827 | 0.365 |
| Medication for diabetes, n (%) | 4 (2.3) | 5 (8.1) | 2,337 (2.1) | 0.056 | 0.852 | 0.002 |
| Medication for dyslipidemia, n (%) | 5 (2.9) | 0 (0.0) | 1,462 (1.3) | 0.329 | 0.070 | 0.363 |
| eGFR (mL/min.1.73 m2) | 81.9 ± 18.6 | 87.5 ± 20.6 | 81.0 ± 17.0 | 0.051 | 0.459 | 0.003 |
| Women | ||||||
| SUA 0.0–1.3 mg/dL (A) | SUA 1.4–2.0 mg/dL (B) | SUA ≥ 2.1 mg/dL (C) | Comparison I (A) vs. (B) | Comparison II (A) vs. (C) | Comparison III (B) vs. (C) | |
| n = 221 | n = 679 | n = 134,906 | P Value | P Value | P Value | |
| Age (years) | 52.1 ± 14.2 | 49.6 ± 13.7 | 53.2 ± 14.5 | 0.022 | 0.27 | <0.001 |
| BMI (kg/m2) | 22.8 ± 3.7 | 21.4 ± 2.9 | 22.8 ± 3.3 | <0.001 | 0.865 | <0.001 |
| SBP (mmHg) | 121.7 ± 20.6 | 118.6 ± 20.7 | 123.0 ± 21.4 | 0.052 | 0.400 | <0.001 |
| TP (g/dL) | 7.6 ± 0.5 | 7.5 ± 0.5 | 7.6 ± 0.5 | 0.026 | 0.600 | <0.001 |
| AST (IU/L) | 21 {17,25} | 19 {16,23} | 21 {18,25} | <0.001 | 0.931 | <0.001 |
| ALT (IU/L) | 15 {11,20} | 12 {9,17} | 14 {11,19} | <0.001 | 0.587 | <0.001 |
| T-bil (mg/dL) | 0.75 ± 0.28 | 0.74 ± 0.33 | 0.74 ± 0.30 | 0.643 | 0.514 | 0.885 |
| TC (mg/dL) | 204.3 ± 35.2 | 195.2 ± 34.7 | 206.2 ± 36.9 | <0.001 | 0.440 | <0.001 |
| TG (mg/dL) | 84 {62.5,111} | 70 {54,96} | 104 {73,153} | <0.001 | 0.951 | <0.001 |
| LDL-C (mg/dL) | 123.8 ± 33.2 | 116.9 ± 29.7 | 126.6 ± 33.4 | 0.004 | 0.218 | <0.001 |
| HDL-C (mg/dL) | 61.1 ± 14.2 | 62.0 ± 14.2 | 60.0 ± 14.6 | 0.393 | 0.248 | <0.001 |
| FBG (mg/dL) | 97.7 ± 18.6 | 99.5 ± 31.9 | 96.8 ± 18.0 | 0.429 | 0.449 | <0.001 |
| Current smoking, n (%) | 12 (5.4) | 34 (5.0) | 6,793 (5.0) | 0.804 | 0.789 | 0.974 |
| Frequent alcohol drinker, n (%) | 24 (10.9) | 42 (6.2) | 11,588 (8.6) | 0.021 | 0.229 | 0.026 |
| Medication for hypertension, n (%) | 30 (13.6) | 66 (9.7) | 17,624 (13.1) | 0.107 | 0.841 | 0.010 |
| Medication for diabetes, n (%) | 3 (1.4) | 18 (2.7) | 1,805 (1.3) | 0.269 | 0.980 | 0.003 |
| Medication for dyslipidemia, n (%) | 3 (1.4) | 12 (1.8) | 3,932 (2.9) | 0.679 | 0.169 | 0.076 |
| eGFR (mL/min.1.73 m2) | 83.4 ± 19.4 | 94.3 ± 19.9 | 81.6 ± 18.3 | <0.001 | 0.139 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawasoe, S.; Ide, K.; Usui, T.; Kubozono, T.; Yoshifuku, S.; Miyahara, H.; Maenohara, S.; Ohishi, M.; Kawakami, K. Distribution and Characteristics of Hypouricemia within the Japanese General Population: A Cross-Sectional Study. Medicina 2019, 55, 61. https://doi.org/10.3390/medicina55030061
Kawasoe S, Ide K, Usui T, Kubozono T, Yoshifuku S, Miyahara H, Maenohara S, Ohishi M, Kawakami K. Distribution and Characteristics of Hypouricemia within the Japanese General Population: A Cross-Sectional Study. Medicina. 2019; 55(3):61. https://doi.org/10.3390/medicina55030061
Chicago/Turabian StyleKawasoe, Shin, Kazuki Ide, Tomoko Usui, Takuro Kubozono, Shiro Yoshifuku, Hironori Miyahara, Shigeho Maenohara, Mitsuru Ohishi, and Koji Kawakami. 2019. "Distribution and Characteristics of Hypouricemia within the Japanese General Population: A Cross-Sectional Study" Medicina 55, no. 3: 61. https://doi.org/10.3390/medicina55030061