The Threat of Multiple Liver Carcinogens in the Population of Laos: A Review
by

Philavanh Sitbounlang
1, 
Agnès Marchio
2,
Eric Deharo
3,4,
Phimpha Paboriboune
1 and
Pascal Pineau
2,* 1
Center for Infectiology Lao-Christophe Mérieux CILM, Ministry of Health, Samsenthai Road, Sisathanak District, Vientiane 3888, Laos
2
Unité “Organisation Nucléaire et Oncogenèse”, INSERM U993, Institut Pasteur, 28, rue du Docteur Roux, 75724 Paris, France
3
Institut de Recherche pour le Développement, Ban Naxai, Saysettha District, Vientiane 5992, Laos
4
Faculté de Pharmacie-Université Paul Sabatier-Toulouse III, Pharmaco-Chimie et Biologie Pour le Développement PHARMA-DEV, UMR-152 IRD-UPS, 35 Chemin des Maraîchers, 31400 Toulouse, France
*
Author to whom correspondence should be addressed.
Livers 2021, 1(1), 49-59; https://doi.org/10.3390/livers1010005
Submission received: 12 January 2021
/
Revised: 19 February 2021
/
Accepted: 26 February 2021
/
Published: 5 March 2021
Abstract
:Laos is a landlocked country in South East Asia, ranking fifth for primary liver cancer incidence worldwide. Risk factors that might explain this worrying situation are poorly known. We conducted a review of the literature concerning the etiologies of terminal liver diseases in Laos. A double infectious burden with hepatitis B and C viruses and the liver fluke Opisthorchis viverrini seems to be the main cause of the high liver cancer incidence. Moreover, it was also suggested that mutagenic substances frequently found in tobacco, alcoholic beverages, fermented fish, and mold-contaminated cereals or nuts, which are all substances heavily consumed by Lao people, lead to the accumulation of DNA mutations in the liver cell genome causing tumor processes. However, the respective proportions of liver cancer cases attributable to each category of infections and substances consumed, as well as the histological nature of the neoplasia are still not precisely documented in Laos. The international medical and scientific communities as well as public health stakeholders should urgently consider the alarming situation of liver health in Laos to stimulate both research and subsequent implementation of prevention policies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
Laos is the least densely populated country with 30 people/km2 and with the lowest life expectancy of 66 years in mainland Southeast Asia/Indochinese peninsula. According to Coker et al., the endemic presence of severe infectious diseases is a factor both preventing population expansion and increase of life expectancy in the region [1]. Furthermore, Laos is affected by a worrying pattern of non-communicable diseases that includes a high age-adjusted death rate in the 15–59-years population, high levels of tobacco use in men of 64%, and a significant proportion of the population is overweight (>35%) [2].
It was estimated that Laos has an incidence of primary liver cancer (PLC) of 22.4 cases/100,000 people, which is currently the second highest rate in Southeast Asia, behind Vietnam (see Figure 1). It was estimated that around 1100 new cases occur yearly in the country, equally affecting men and women, an unusual situation as worldwide women are usually relatively less affected by this disease. However, these figures are mere estimates from the World Health Organization (WHO), taking neighboring nations as references. There have been significant variations in estimates of the incidence of PLC in Laos, illustrated by the last two GLOBOCAN reports. These variations are not supported by any obvious changes in the epidemiology of risk factors. There is currently no comprehensive cancer registry in Laos and very few pathologists. For reasons that will be discussed below, it is thus highly plausible that PLC incidence is largely underestimated in Laos. The underestimation of PLC cases is common worldwide, even in high-income countries [3,4].
To explain the high incidence of PLC in Laos, we should first state that various infectious burdens, including chronic hepatitis B and C and frequent liver infestation with the fluke Opisthorchis viverrini (OV) afflict Lao people. The respective contributions of the different viruses and parasites to the local burden of PLC are, however, still unknown and therefore national incidences of cholangiocarcinoma (CCA), due to OV or hepatocellular carcinoma (HCC), due to hepatitis viruses are hypothetical. Furthermore, the impact of their interactions on liver carcinogenesis in case of co-presence has not yet been properly characterized [5]. More remarkably, no description of PLC in the Laotian population is currently available in the medical literature.
2. Methods
Relevant literature included in this short review was collected in keeping with the guidelines proposed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) [6]. Records were retrieved from relevant online databases’ (Medline, PubMed, Google Scholar) collection of publications ending in October 2020. Our search was targeted on terms corresponding to liver diseases and carcinogenic factors in the region (hepatitis viruses B and C, O. viverrini, aflatoxin B1, nitrosamines, alcoholic beverage, fatty liver, liver cirrhosis, liver cancer, cholangiocarcinoma, hepatocellular carcinoma) and country names. We primarily focused our search on the literature treating Laos (or Lao People’s Democratic Republic, Lao PDR, also frequently used in the medical literature), but when no record was available, we explored publications from immediately neighboring countries (Cambodia, Myanmar, Thailand, Vietnam). Relevant medical literature from China was only marginally approached and mostly focused on the Yunnan province, the only Chinese province to share a border with Laos. Articles were first selected after reviewing the title and abstract, and subsequently by reading the full text of papers initially retained.
3. Results
3.1. Viral Risk Factors
3.1.1. Hepatitis B Virus
In Laos, the situation of persistent infection with hepatitis B virus (HBV) corresponds to that of a highly endemic country. More than 8% of the population are chronically infected. A decade ago, 8.7% of blood donors were seropositive for HBV surface antigen (HBsAg) and this rate remained stable, but steadily increasing (at 9.6%), in a more recent study [7,8]. Additional evidence in adolescents from Vientiane and Luang Prabang confirms these preliminary estimates, detailing rates of 10.2% [9]. Furthermore, it was shown that more than 10% of HBsAg-blood donors present circulating HBV DNA, i.e., an occult hepatitis B infection (OBI). This observation implies that in reality, around 20% of the Laotian population might be chronically infected with HBV. Moreover, in a study conducted in Vientiane on 3857 HBV-infected patients, it was shown that 50% of patients were under 37 and almost 60% had a viral load higher than 10,000 IU/mL, the threshold value for high risk of developing liver cancer. Among the patients, 10.6% had both a high level of HBV DNA over 10,000 IU/mL and elevated aminotransferases. However, only 2.4% of them received treatment for chronic hepatitis [10,11].
Finally, several surveys conducted on mothers and immunized newborns indicated that hepatitis B vaccination is remarkably inefficient in Laos, and results in protection only in a minority of newborns [12,13,14]. In addition, despite mass vaccination campaigns, only a minority of newborns actually receive the birth dose of anti-hepatitis B vaccine [15]. Taken together, the data show that HBV will still be a significant public health problem in Laos in the next decades. Finally, it was demonstrated that the HBV strains circulating in Lao blood donors predominantly belong to subtypes C1 and B4. However, mixed infections are frequent and more importantly, recombinant viruses between B and C genotypes, including the rare genotype I, which is dominant in around 5% of cases [16]. This is surprising, as HBV is believed to be transmitted pseudo-vertically at birth from mother to newborn in Laos. The circumstances that explain multiple strain infections are poorly known, as are the consequences of this situation for disease progression.
3.1.2. Hepatitis C Virus
In comparison, hepatitis C virus (HCV) is a lesser problem, as seroprevalence for anti-HCV virus reaches “only” 1.1% in Lao people. In Laos, seropositivity for HCV affects older subsets of the population, suggesting the virus circulated more widely in the past than now. In this regard, a case-control survey on acute hepatitis conducted two decades ago measured anti-HCV prevalence around 60% in patients over 50 years [17]. More recently, a retrospective study conducted on 1765 HCV-infected patients showed that, in Vientiane, 28% had high viral loads (>6log10). About 23% of patients had levels of aminotransferases indicative of liver damage >40 IU/mL, but less than 20% of them received antiviral drugs [10,11]. In Laos, circulating strains overwhelmingly belong to genotype 6 >95%, the Southeast Asian version of HCV, with frequent viral isolates specific to the local population [18,19,20]. Overall, Laos exhibits the highest HCV genotype 6 diversity in Asia, suggesting that the country might be the place where this virus originated. Another specificity of Laos is that no rapid expansion of HCV subtype was observed in Laos during the 20th century, a situation that contrasts with neighboring countries. As for other HCV genotypes, the origin of genotype 6 entry in human populations is remote, dating back 1100–1350 years ago [18]. Its original host is unknown. During recent decades, a large number of novel hepacivirus species have been identified in various mammals including bats [21]. In this context, the well-known capacity of hepaciviruses to cross species barriers, illustrated by the recent transmission of equine hepacivirus to dogs, appears to be especially relevant [22]. In this regard, although animal hepaciviruses circulating in Laos are still unknown, there are a large diversity of chiropters [23]. These animals, well-known for their capacity to transmit viruses to humans, are occasionally consumed as bushmeat by the Laotian population, and also found in highly frequented Buddhist cave temples such the Pak Ou caves. These circumstances may possibly represent an appropriate configuration for the efficient crossing of species barriers by hepaciviruses [24,25].
Subsequent to its entry in the human population of Laos, HCV circulation could have been maintained for centuries through the practice of Sak Yant tattooing, Buddhist monk tattoos, or by variolation practiced by traditional healers for smallpox protection since its possible import in the early 19th century by the French [26,27].
3.2. Parasitic Risk Factors
3.2.1. Opisthorchiasis
The epidemiology of opisthorchiasis, responsible for bile duct inflammation cholangitis, cholecystitis, periportal fibrosis, and intra-hepatic cholangiocarcinoma, is well described in Laos. The prevalence of OV infection is high in Laos; an estimated 2 million people are infected. Southern provinces of the country, with a high proportion of populations living on the banks of the Mekong river are more heavily affected, with a 50% prevalence, while central areas like Vientiane are around 20%. A survey conducted in Saravane province showed that the prevalence increases with age, reaching 85% in older population subsets of 46–55 years, but tending to already reach a plateau of 70% as soon as 20 years of age [28]. This situation is primarily due to the consumption of raw, fermented, or brined cyprinoid fish padek infected with OV metacercaria in a context where absence of latrines facilitates the perpetuation of the parasite cycle by the daily shedding of parasites eggs in stools of infected patients.
3.2.2. Other Helminths
Furthermore, multiple parasitism with other helminths and protozoa is common in populations of southern Laos and might play some role in liver disease progression [29]. In this context, Schistosoma mekongi (Sm), responsible for hepatomegaly, liver fibrosis, and portal hypertension is present in the same region where OV prevalence is high and OV/Sm co-infestation was shown to be synergistic in liver pathology [30].
3.3. Chemical/Environmental Risk Factors
It is well known that cancer is primarily a genetic disease characterized by the accumulation of mutations in a cell clone. Recent genomic data indicate that liver infections, rather than being mutagenic per se, instead create a tissue microenvironment that is favorable for tumor development [33]. Infected liver tissue becomes the target for decades of inflammatory infiltrates that kill both infected and uninfected cells. The resulting regeneration and DNA replication that occur on a daily basis as an emergency response to cell death are associated with intrinsically poor genome maintenance due to lack of time. During this accelerated tissue repair process, concomitant presence of mutagenic substances such as polycyclic aromatic hydrocarbons (PAH) produced by tobacco combustion, aldehydes, or carbamates present in alcoholic beverages, nitrosamines generated during fish fermentation (an important component of Laotian cuisine), aristolochic acid found in herbal teas or aflatoxin B1 (AFB1) present in cereals or nuts will invariably lead to accumulation of mutations that promote tumor processes [34,35,36,37]. As mentioned above, many of these mutagens are prevalent in Laos, such as PAH produced by tobacco combustion in a country where the majority of men and a substantial proportion of women are smokers [2]. Other mutagenic contaminants may be found in unrecorded spirits. Lao-Lao rice whiskey and Lao Hai rice wine consumption were studied only from an anthropological point of view and chemical contaminants in these home-made alcoholic beverages (Figure 2) are unknown [38,39]. It is known, however, that spirits resulting from rice fermentation may contain traces of carcinogenic substances such as ethyl carbamate, acetaldehyde, and/or arsenic [40,41,42].
Other important compounds, nitrosamines, are mutagens produced during fermentation of fish. Nitrosamines directly ingested with food or endogenously produced by OV-infected patients have been long suspected to play an important role in cholangiocytes transformation [43,44,45,46].
Another of the mutagens potentially present in Laos is AFB1, a carcinogenic mycotoxin produced by Aspergillus species. Unfortunately, there are no publications about AFB1 in Laos. However, the toxin has been found in food from all neighboring countries, Thailand, Cambodia, Vietnam, Myanmar, and China [47,48,49,50]. It seems, therefore, reasonable to assume that AFB1 is present in Laos as well. AFB1 is known for its molecular fingerprints in liver cancer, as it was shown to generate mutation due to transversion of G to T at codon 249 of TP53 gene leading to the replacement of an ARG by a SER. Such mutations, clonally present in developing HCC, have already been found in neighboring Thailand [51].
Finally, it is worth briefly mentioning the issue of Agent Orange. Agent Orange (AO) was the principal herbicide derived from chlorinated phenoxyacetic acid used by the US Army during the Vietnam war (1955–1975). It was sprayed to remove the forest cover that was hiding North Vietnamese military units particularly along the Ho Chi Minh trail linking North to South Vietnam and occasionally passing through Laotian territory. Laos was thus affected to some extent essentially in the Savannakhet province. It was estimated that 1.8 million liters of AO were sprayed on Laos [52]. AO turned out to be contaminated by dioxin (in fact tetrachlorodibenzodioxin, TCDD), an environmentally-stable non-mutagenic tumor promoter [53]. Recent surveys conducted in Laos on small series of breast milk, blood, and food samples observed only very low levels of contamination with dioxin [54,55]. US government acknowledges the fact that AO exposure is associated with some tumors in US veterans (lymphoma, soft tissue sarcomas, and possibly prostate cancer). Some Asian and European researchers found an epidemiological association of AO exposure with PLC development, while surveys conducted on US Army veterans did not reach similar conclusions [56,57,58,59]. It seems that the liver tumor-promoting activity of dioxin or phenoxyacetic acid derivatives develops primarily when combined with chronic HBV infection, a condition obviously more frequent in Indochinese populations than among US Army veterans [57]. We consider that molecular studies, rather than epidemiological ones, are warranted to uncover hypothetical fingerprints of dioxin exposure in Laotian patients with PLC.
3.4. Non-Communicable Liver Diseases
Chronic liver disease with an infectious origin or exposure to mutagens are not the only threats for liver health in Lao PDR. Non-communicable diseases (NCD) such as alcoholic liver disease (ALD) or non-alcoholic fatty liver disease (NAFLD) both characterized by the presence of significant steatosis in liver tissue emerged in the last decades as a major threat at a global level [60].
There is, actually, a dearth of data concerning both ALD and NAFLD in Laos. However, NAFLD is considered the most frequent chronic liver disease in Southeast Asia, with a 40% prevalence according to a recent meta-analysis [61]. Abdominal ultrasound assessment of the liver is the most convenient screening method to evaluate the consequences of O. viverrini infection. A recent survey observed a 12% prevalence of fatty liver changes in a series of 431 patients from southern Laos [31]. Consistent rates are also observed in similar patients from Thailand (12–19%) [62,63].
NAFLD is primarily associated with metabolic diseases (obesity, type 2 diabetes, metabolic syndrome) linked to excessive nutritional intake, lack of physical activity, and aging. The Laotian population is, however, far to have reached the affluence and food security observed in some of its neighboring countries and there is in the country a double nutritional burden [64]. A significant subset of the adult population is affected with malnutrition (underweight, body mass index, BMI < 18.5, 10%) while another segment is on the contrary affected by obesity with substantial variations in prevalence (6–25.2%) depending on which criteria (WHO or Asian-specific) are retained [2,65]. Overall, the prevalence of obesity in Laos is one of the lowest in the Western Pacific region [66]. Likewise, the prevalence of diabetes is mild in Laos (5.7%) [2,67]. As a consequence, the proportions of NAFLD only-associated deaths from liver cirrhosis (12–19%) or PLC (10%) can be considered as still limited in Laos [68,69].
The medical literature concerning ALD is similarly scarce in Laos. However, as most countries in Southeast Asia, alcohol per capita consumption increased significantly in Laos in the last decade. The annual consumption of alcohol by Laotians is 10.6 L/year, the highest in Southeast Asia. As a consequence, with a rate of 81/100,000, Laotian population is affected by the heaviest alcohol-attributable burden of death in the region [70]. According to a recent review, the alcohol-attributable fractions of death is 41% for liver cirrhosis and 39% for PLC, i.e., the highest proportions in Southeast Asia [68,69].
Overall, ALD represents the largest NCD affecting the liver and is currently a more worrisome health problem than NAFLD in Laos.
4. Conclusions
In conclusion, populations in Laos suffer from a heavy but imprecisely quantified burden of PLC. This situation is due to the pressure applied on Laotian populations by highly prevalent and deleterious risk factors such as chronic infections, either with hepatitis viruses or with carcinogenic trematodes from Opisthorchis genus, responsible for HCC and CCA, respectively (Figure 3). The disturbingly high level of alcohol intake per capita in Laos represents an additional contributor to the situation. The proportions of cancer cases, which can be attributed to each agent are unknown, just as are their respective implications in liver cirrhosis or severe periductal fibrosis prevalence among Lao citizens. Likewise, virus or parasite subtypes/strains potentially endowed with an increased carcinogenic potency are unknown in Laos.
Finally, carcinomas are invariably multifactorial, and the high incidence of PLC in Laos is also due to the exposure of infected patients to mutagens, e.g., aflatoxins, nitrosamines present in foodstuffs and acting synergistically with infectious agents to trigger liver tumorigenesis. Molecular fingerprints left by these chemicals in DNA have never been characterized in Laos.
Overall, the issue of severe liver diseases among Lao people could be tackled through a holistic approach gathering expertise from different fields. The production of data through sound clinical and translational studies is a crucial and mandatory milestone to design and implement prevention policies that will benefit the youngest and future generations of Laotian citizens.
Author Contributions
Conceptualization: P.P. (Pascal Pineau), P.S., and E.D.; methodology: P.P. (Pascal Pineau) and P.S.; writing—original draft: P.P. (Pascal Pineau), reviewing—editing: P.S., A.M., E.D., P.P. (Phimpha Paboriboune) and P.P. (Pascal Pineau). All authors have read and agreed to the published version of the manuscript.
Funding
Philavanh Sitbounlang is supported by the European Union’s Horizon 2020 Marie Sklodowska-Curie Actions MSCA—Research and Innovation Staff Exchange—RISE under grant agreement No 823935.
Acknowledgments
We are grateful to Elizabeth Elliott for editorial assistance and constructive criticisms. The authors would like to thank Jean Marc Dubost for the photo of artisanal alcohol production device, taken in Sayaboury Province, Laos.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Coker, R.; Hunter, B.; Rudge, J.; Liverani, M.; Hanvoravongchai, P. Emerging infectious diseases in southeast Asia: regional challenges to control. Lancet 2011, 377, 599–609. [Google Scholar] [CrossRef]
- Dans, A.; Ng, N.; Varghese, C.; Tai, E.; Firestone, R.; Bonita, R. The rise of chronic non-communicable diseases in southeast Asia: time for action. Lancet 2011, 377, 680–689. [Google Scholar] [CrossRef]
- Hong, T.; Gow, P.; Fink, M.; Dev, A.; Roberts, S.; Nicoll, A.; Lubel, J.; Kronborg, I.; Arachchi, N.; Ryan, M.; et al. Novel Population-Based Study Finding Higher Than Reported Hepatocellular Carcinoma Incidence Suggests an Updated Approach Is Needed. Hepatology 2016, 63, 1206–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Törner, A.; Stokkeland, K.; Svensson, Å.; Dickman, P.W.; Hultcrantz, R.; Montgomery, S.; Duberg, A.-S. The underreporting of hepatocellular carcinoma to the cancer register and a log-linear model to estimate a more correct incidence. Hepatology 2016, 65, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Pinyosophon, A.; Wiwanitkit, V. The Prevalence of Hepatitis B Seropositivity among Patients with Cholangiocarcinoma. Viral Immunol. 2002, 15, 655–657. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Jutavijittum, P.; Yousukh, A.; Samountry, B.; Samountry, K.; Ounavong, A.; Thammavong, T.; Keokhamphue, J.; Toriyama, K. Seroprevalence of hepatitis B and C virus infections among Lao blood donors. Southeast Asian J. Trop. Med. Public Health 2007, 38, 674–679. [Google Scholar]
- Jutavijittum, P.; Andernach, I.E.; Yousukh, A.; Samountry, B.; Samountry, K.; Thammavong, T.; Keokhamphue, J.; Toriyama, K.; Muller, C.P. Occult hepatitis B infections among blood donors in Lao PDR. Vox Sang. 2014, 106, 31–37. [Google Scholar] [CrossRef]
- Black, A.P.; Nouanthong, P.; Nanthavong, N.; Souvannaso, C.; Vilivong, K.; Jutavijittum, P.; Samountry, B.; Lütteke, N.; Hübschen, J.M.; Goossens, S.; et al. Hepatitis B virus in the Lao People’s Democratic Republic: A cross sectional serosurvey in different cohorts. BMC Infect. Dis. 2014, 14, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paboriboune, P.; Vial, T.; Sitbounlang, P.; Bertani, S.; Trepo, C.; Deny, P.; Babin, F.-X.; Steenkeste, N.; Pineau, P.; Deharo, E. Hepatitis C in Laos: A 7-Year Retrospective Study on 1765 Patients. Virol. Sin. 2018, 33, 295–303. [Google Scholar] [CrossRef]
- Paboriboune, P.; Vial, T.; Chassagne, F.; Sitbounlang, P.; Soundala, S.; Bertani, S.; Sengmanothong, D.; Babin, F.-X.; Steenkeste, N.; Deny, P.; et al. A Seven-Year Retrospective Study on the Surveillance of Hepatitis B in Laos. Int. J. Hepatol. 2018, 2018, 9462475. [Google Scholar] [CrossRef] [Green Version]
- Xeuatvongsa, A.; Komada, K.; Kitamura, T.; Vongphrachanh, P.; Pathammavong, C.; Phounphenghak, K.; Sisouk, T.; Phonekeo, D.; Sengkeopaseuth, B.; Som-Oulay, V.; et al. Chronic Hepatitis B Prevalence among Children and Mothers: Results from a Nationwide, Population-Based Survey in Lao People’s Democratic Republic. PLoS ONE 2014, 9, e88829. [Google Scholar] [CrossRef] [PubMed]
- Evdokimov, K.; Sayasinh, K.; Nouanthong, P.; Vilivong, K.; Samountry, B.; Phonekeo, D.; Strobel, M.; Haegeman, F.; Heimann, P.; Muller, C.; et al. Low and disparate seroprotection after pentavalent childhood vaccination in the Lao People’s Democratic Republic: A cross-sectional study. Clin. Microbiol. Infect. 2017, 23, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Norizuki, M.; Kitamura, T.; Komada, K.; Sugiyama, M.; Mizokami, M.; Xeuatvongsa, A.; Som-Oulay, V.; Vongphrachanh, P.; Machida, M.; Wada, K.; et al. Serologic testing of randomly selected children after hepatitis B vaccination: A cross-sectional population-based study in Lao People’s Democratic Republic. BMC Infect. Dis. 2019, 19, 507. [Google Scholar] [CrossRef] [PubMed]
- Deharo, E.; Paboriboune, P.; Bourdy, G.; Elliott, E.; Rakotomalala, D.; Sengxeu, N.; Manylert, S.; Celhay, O.; Torres, J.; Lai, J.; et al. Issues, Barriers, and Facilitators that Influence Access to Immunization Programs for People Living in the Mekong Border Regions of Lao PDR; Institut de Recherche pour le Développment, University of Health Sciences, Centre d’Infectiologie Lao Christophe Mérieux: Vientiane, Laos, 2018; p. 67. [Google Scholar]
- Andernach, I.E.; Jutavijittum, P.; Samountry, B.; Yousukh, A.; Thammavong, T.; Hübschen, J.M.; Muller, C.P. A High Variability of Mixed Infections and Recent Recombinations of Hepatitis B Virus in Laos. PLoS ONE 2012, 7, e30245. [Google Scholar] [CrossRef] [PubMed]
- Bounlu, K.; Insisiengmay, S.; Vanthanouvong, K.; Widjaja, S.; Iinuma, K.; Matsubayashi, K.; Laras, K.; Putri, M.; Endy, T.; Vaughn, D.W.; et al. Acute jaundice in Vientiane, Lao People’s Democratic Republic. Clin. Infect. Dis. 1998, 27, 717–721. [Google Scholar] [CrossRef] [Green Version]
- Pybus, O.G.; Barnes, E.; Taggart, R.; Lemey, P.; Markov, P.V.; Rasachak, B.; Syhavong, B.; Phetsouvanah, R.; Sheridan, I.; Humphreys, I.S.; et al. Genetic History of Hepatitis C Virus in East Asia. J. Virol. 2008, 83, 1071–1082. [Google Scholar] [CrossRef] [Green Version]
- Hübschen, J.; Jutavijittum, P.; Thammavong, T.; Samountry, B.; Yousukh, A.; Toriyama, K.; Sausy, A.; Muller, C. High genetic diversity including potential new subtypes of hepatitis C virus genotype 6 in Lao People’s Democratic Republic. Clin. Microbiol. Infect. 2011, 17, E30–E34. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Barnes, E.; Newton, P.N.; Fu, Y.; Vongsouvath, M.; Klenerman, P.; Okamoto, H.; Abe, K.; Pybus, O.G.; Lu, L. An expanded taxonomy of hepatitis C virus genotype 6: Characterization of 22 new full-length viral genomes. Virology 2015, 476, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Hartlage, A.S.; Cullen, J.M.; Kapoor, A. The Strange, Expanding World of Animal Hepaciviruses. Annu. Rev. Virol. 2016, 3, 53–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pybus, O.G.; Thézé, J. Hepacivirus cross-species transmission and the origins of the hepatitis C virus. Curr. Opin. Virol. 2016, 16, 1–7. [Google Scholar] [CrossRef]
- Thomas, N.M.; Duckworth, J.W.; Douangboubpha, B.; Williams, M.; Francis, C.M. A Checklist of Bats (Mammalia: Chiroptera) from Lao PDR. Acta Chiropterol. 2013, 15, 193–260. [Google Scholar] [CrossRef]
- Calisher, C.H.; Childs, J.E.; Field, H.E.; Holmes, K.V.; Schountz, T. Bats: Important Reservoir Hosts of Emerging Viruses. Clin. Microbiol. Rev. 2006, 19, 531–545. [Google Scholar] [CrossRef] [Green Version]
- Quan, P.-L.; Firth, C.; Conte, J.M.; Williams, S.H.; Zambrana-Torrelio, C.M.; Anthony, S.J.; Ellison, J.A.; Gilbert, A.T.; Kuzmin, I.V.; Niezgoda, M.; et al. Bats are a major natural reservoir for hepaciviruses and pegiviruses. Proc. Natl. Acad. Sci. USA 2013, 110, 8194–8199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guénel, A. Lutte contre la variole en Indochine: Variolisation contre vaccination. Hist. Philos. Life Sci. 1995, 17, 55–79. [Google Scholar] [PubMed]
- Monnais-Rousselot, L. Autopsie d’un mal exotique à part: La variole et la vaccine en Indochine française (1860–1939). Rev. Française D’histoire D’outre-Mer 1995, 82, 505–527. [Google Scholar] [CrossRef]
- Sayasone, S.; Odermatt, P.; Phoumindr, N.; Vongsaravane, X.; Sensombath, V.; Phetsouvanh, R.; Choulamany, X.; Strobel, M. Epidemiology of Opisthorchis viverrini in a rural district of southern Lao PDR. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Sayasone, S.; Mak, T.K.; Vanmany, M.; Rasphone, O.; Vounatsou, P.; Utzinger, J.; Akkhavong, K.; Odermatt, P. Helminth and Intestinal Protozoa Infections, Multiparasitism and Risk Factors in Champasack Province, Lao People’s Democratic Republic. PLOS Negl. Trop. Dis. 2011, 5, e1037. [Google Scholar] [CrossRef] [Green Version]
- Sayasone, S.; Rasphone, O.; Vanmany, M.; Vounatsou, P.; Utzinger, J.; Tanner, M.; Akkhavong, K.; Hatz, C.; Odermatt, P. Severe morbidity due to Opisthorchis viverrini and Schistosoma mekongi infection in Lao People’s Democratic Republic. Clin. Inf. Dis. 2012, 55, e54–e57. [Google Scholar] [CrossRef] [Green Version]
- Soukhathammavong, P.A.; Rajpho, V.; Phongluxa, K.; Vonghachack, Y.; Hattendorf, J.; Hongvanthong, B.; Rasaphon, O.; Sripa, B.; Akkhavong, K.; Hatz, C.; et al. Subtle to severe hepatobiliary morbidity in Opisthorchis viverrini endemic settings in southern Laos. Acta Trop. 2015, 141, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Khieu, V.; Sayasone, S.; Muth, S.; Kirinoki, M.; Laymanivong, S.; Ohmae, H.; Huy, R.; Chanthapaseuth, T.; Yajima, A.; Phetsouvanh, R.; et al. Elimination of Schistosomiasis Mekongi from Endemic Areas in Cambodia and the Lao People’s Democratic Republic: Current Status and Plans. Trop. Med. Infect. Dis. 2019, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.D.; Nakamura, I.; Roberts, L.R. The tumor microenvironment in hepatocellular carcinoma: Current status and therapeutic targets. Semin. Cancer Biol. 2011, 21, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, S.P.; Schwank, J.; Staib, F.; Wang, X.W.; Harris, C.C. TP53 mutations and hepatocellular carcinoma: Insights into the etiology and pathogenesis of liver cancer. Oncogene 2007, 26, 2166–2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nedelko, T.; Arlt, V.M.; Phillips, D.H.; Hollstein, M. TP53mutation signature supports involvement of aristolochic acid in the aetiology of endemic nephropathy-associated tumours. Int. J. Cancer 2009, 124, 987–990. [Google Scholar] [CrossRef]
- Tanase, A.-M.; Marchio, A.; Dumitrascu, T.; Dima, S.; Herlea, V.; Oprisan, G.; Dejean, A.; Popescu, I.; Pineau, P. Mutation spectrum of hepatocellular carcinoma from eastern-European patients betrays the impact of a complex exposome. J. Expo. Sci. Environ. Epidemiol. 2014, 25, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; He, H.; Zang, M.; Wu, Q.; Zhao, H.; Lu, L.; Jiao, Y. Genetic features of aflatoxin-associated hepatocellular carcinoma. Gastroenterology 2017, 153, 249–262. [Google Scholar] [CrossRef] [Green Version]
- Hatsadong; Douangsila, K.; Gibson, P. Rice-based traditions and ritual in the Mekong River Valley. In Rice in Laos; Schiller, J., Chanphengxay, M., Linquist, B., Appa Rao, S., Eds.; International Rice Research Institute: Los Banos, Philippines, 2006; pp. 65–78. [Google Scholar]
- Delang, C. Keeping the Spirit Alive: Rice whiskey production in Northern Lao P.D.R. Ethnobot. Res. Appl. 2008, 6, 459–470. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Zou, H.; Fu, J.; Zhou, J.; Du, G.; Chen, J. Metabolic Engineering of the Regulators in Nitrogen Catabolite Repression to Reduce the Production of Ethyl Carbamate in a Model Rice Wine System. Appl. Environ. Microbiol. 2013, 80, 392–398. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Li, X.; Shen, C.; Lu, J.; Chen, J.; Xie, G. Decreased ethyl carbamate generation during Chinese rice wine fermentation by disruption of CAR1 in an industrial yeast strain. Int. J. Food Microbiol. 2014, 180, 19–23. [Google Scholar] [CrossRef]
- Newman, I.M.; Qian, L.; Tamrakar, N.; Zhang, B.-B. Chemical Composition and Safety of Unrecorded Grain Alcohol (Bai Jiu) Samples from Three Provinces in China. Int. J. Environ. Res. Public Health 2018, 15, 2710. [Google Scholar] [CrossRef] [Green Version]
- Mitacek, E.J.; Brunnemann, K.D.; Suttajit, M.; Martin, N.; Limsila, T.; Ohshima, H.; Caplan, L.S. Exposure to N-nitroso compounds in a population of high liver cancer regions in Thailand: Volatile nitrosamine (VNA) levels in Thai food. Food Chem. Toxicol. 1999, 37, 297–305. [Google Scholar] [CrossRef]
- Sripa, B.; Brindley, P.J.; Mulvenna, J.; Laha, T.; Smout, M.J.; Mairiang, E.; Bethony, J.M.; Loukas, A. The tumorigenic liver fluke Opisthorchis viverrini—Multiple pathways to cancer. Trends Parasitol. 2012, 28, 395–407. [Google Scholar] [CrossRef] [Green Version]
- Srivatanakul, P.; Sukaryodhin, S.; Ohshima, H.; Khlat, M.; Parkin, M.; Brouet, I.; Bartsch, H. opisthorchis viverrini infestation and endogenous nitrosamines as risk factors for cholangiocarcinoma in thailand. Int. J. Cancer 1991, 48, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Sripa, B.; Kaewkes, S.; Sithithaworn, P.; Mairiang, E.; Laha, T.; Smout, M.; Pairojkul, C.; Bhudhisawasdi, V.; Tesana, S.; Thinkamrop, B.; et al. Liver Fluke Induces Cholangiocarcinoma. PLoS Med. 2007, 4, e201. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, K.C.; Kobbeman, K.; Montalbano, B.G.; Cotty, P.J. Aflatoxin-producing Aspergillus species from Thailand. Int. J. Food Microbiol. 2007, 114, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Sorn, V.; Meas, P.; Pin, T.; Gummert, M. Effects of drying and storage management on fungi (Aflatoxin B1) accumulation and rice quality in Cambodia. J. Agric. Rural Dev. Trop. Subtrop. 2017, 118, 141–148. [Google Scholar]
- Huong, B.T.M.; Tuyen, L.D.; Madsen, H.; Brimer, L.; Friis, H.; Dalsgaard, A. Total Dietary Intake and Health Risks Associated with Exposure to Aflatoxin B1, Ochratoxin A and Fuminisins of Children in Lao Cai Province, Vietnam. Toxins 2019, 11, 638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aye, C.N.N.; Nakagawa, H.; Kushiro, M. Occurrence of aflatoxins in processed chili pepper sold in Myanmar. JSM Mycotoxins 2019, 69, 9–13. [Google Scholar] [CrossRef]
- Galy, O.; Chemin, I.; Le Roux, E.; Villar, S.; Le Calvez-Kelm, F.; Lereau, M.; Gouas, D.; Vieco, B.; Suarez, I.; Navas, M.-C.; et al. Mutations in TP53 and CTNNB1 in Relation to Hepatitis B and C Infections in Hepatocellular Carcinomas from Thailand. Hepat. Res. Treat. 2011, 2011, 697162. [Google Scholar] [CrossRef]
- Stellman, J.M.; Stellman, S.D.; Christian, R.; Weber, T.; Tomasallo, C. The extent and patterns of usage of Agent Orange and other herbicides in Vietnam. Nat. Cell Biol. 2003, 422, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, G.D.; Nukaya, M.; Moran, S.M.; Glover, E.; Weinberg, S.; Balbo, S.; Hecht, S.S.; Pitot, H.C.; Drinkwater, N.R.; Bradfield, C.A. Liver Tumor Promotion by 2,3,7,8-Tetrachlorodibenzo-p-dioxin Is Dependent on the Aryl Hydrocarbon Receptor and TNF/IL-1 Receptors. Toxicol. Sci. 2014, 140, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Schecter, A.; Pavuk, M.; Päpke, O.; Ryan, J.J. Dioxin, dibenzofuran, and coplanar PCB levels in Laotian blood and milk from agent orange-sprayed and nonsprayed areas, 2001. J. Toxicol. Environ. Health Part A 2003, 66, 2067–2075. [Google Scholar] [CrossRef]
- Schecter, A.; Pavuk, M.; Malisch, R.; Ryan, J. Dioxin, Dibenzofuran, and Polychlorinated Biphenyl (PCB) Levels in Food from Agent Orange–sprayed and Nonsprayed Areas of Laos. J. Toxicol. Environ. Health Part A 2003, 66, 2165–2186. [Google Scholar] [CrossRef]
- Van Ha, M. Some peculiarities of hepatobiliary diseases in Vietnam. J. Gastroenterol. Hepatol. 1997, 12, S15–S18. [Google Scholar]
- Cordier, S.; Thuy, L.T.B.; Verger, P.; Bard, D.; Dai, L.C.; Larouzé, B.; Dazza, M.C.; Quinh, H.T.; Abenhaim, L. Viral infections and chemical exposures as risk factors for hepatocellular carcinoma in Vietnam. Int. J. Cancer 1993, 55, 196–201. [Google Scholar] [CrossRef]
- Yi, S.-W.; Ryu, S.Y.; Ohrr, H.; Hong, J.-S. Agent Orange exposure and risk of death in Korean Vietnam veterans: Korean Veterans Health Study. Int. J. Epidemiol. 2014, 43, 1825–1834. [Google Scholar] [CrossRef] [Green Version]
- Krishnamurthy, P.; Hazratjee, N.; Opris, D.; Agrawal, S.; Markert, R. Is exposure to Agent Orange a risk factor for hepatocellular cancer? A single-center retrospective study in the U.S. veteran population. J. Gastrointest. Oncol. 2016, 7, 426–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, J.; Wang, F.; Wong, N.-K.; He, J.; Zhang, R.; Sun, R.; Xu, Y.; Liu, Y.; Li, W.; Koike, K.; et al. Global liver disease burdens and research trends: Analysis from a Chinese perspective. J. Hepatol. 2019, 71, 212–221. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Zou, B.; Yeo, Y.H.; Feng, Y.; Xie, X.; Lee, D.H.; Fujii, H.; Wu, Y.; Kam, L.Y.; Ji, F.; et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 389–398. [Google Scholar] [CrossRef]
- Mairiang, E.; Laha, T.; Bethony, J.M.; Thinkhamrop, B.; Kaewkes, S.; Sithithaworn, P.; Tesana, S.; Loukas, A.; Brindley, P.J.; Sripa, B. Ultrasonography assessment of hepatobiliary abnormalities in 3359 subjects with Opisthorchis viverrini infection in endemic areas of Thailand. Parasitol. Int. 2012, 61, 208–211. [Google Scholar] [CrossRef] [Green Version]
- Khuntikeo, N.; Titapun, A.; Loilome, W.; Yongvanit, P.; Thinkhamrop, B.; Chamadol, N.; Boonmars, T.; Nethanomsak, T.; Andrews, R.H.; Petney, T.N.; et al. Current Perspectives on Opisthorchiasis Control and Cholangiocarcinoma Detection in Southeast Asia. Front. Med. 2018, 5, 117. [Google Scholar] [CrossRef] [Green Version]
- Bühler, D.; Hartje, R.; Grote, U.; Dorothee, B.; Rebecca, H. Matching food security and malnutrition indicators: Evidence from Southeast Asia. Agric. Econ. 2018, 49, 481–495. [Google Scholar] [CrossRef]
- Pengpid, S.; Vonglokham, M.; Kounnavong, S.; Sychareun, V.; Peltzer, K. The prevalence of underweight and overweight/obesity and its correlates among adults in Laos: A cross-sectional national population-based survey, 2013. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 25, 265–273. [Google Scholar] [CrossRef]
- Fan, J.-G.; Kim, S.-U.; Wong, V.W.-S. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef] [Green Version]
- Vonglokham, M.; Kounnavong, S.; Sychareun, V.; Pengpid, S.; Peltzer, K. Prevalence and social and health determinants of pre-diabetes and diabetes among adults in Laos: A cross-sectional national population-based survey, 2013. Trop. Med. Int. Health 2018, 24, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.C.S.; Huang, J.L.W.; George, J.; Huang, J.; Leung, C.; Eslam, M.; Chan, H.L.Y.; Ng, S.C. The changing epidemiology of liver diseases in the Asia–Pacific region. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 57–73. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Kumar, M.; Eslam, M.; George, J.; Al Mahtab, M.; Akbar, S.M.F.; Jia, J.; Tian, Q.; Aggarwal, R.; Muljono, D.H.; et al. Liver diseases in the Asia-Pacific region: A Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol. Hepatol. 2020, 5, 167–228. [Google Scholar] [CrossRef] [Green Version]
- Sornpaisarn, B.; Shield, K.; Manthey, J.; Limmade, Y.; Low, W.Y.; Van Thang, V.; Rehm, J. Alcohol consumption and attributable harm in middle-income South-East Asian countries: Epidemiology and policy options. Int. J. Drug Policy 2020, 83, 102856. [Google Scholar] [CrossRef]
Figure 1.
(A) Incidence of primary liver cancer (PLC) in Laos and neighboring countries. Myanmar is clearly less affected than all other countries of the region. (B) Male to female M:F sex ratios of PLC in the same countries. An increased sex ratio is observed in Vietnam suggesting a strong dominance of hepatitis B virus in PLC etiology. (C) Ratios of liver cancer/gallbladder cancer in the region. The low ratio observed in Thailand indicates the epidemiological importance of gallbladder and bile ducts carcinomas cases supposedly triggered by O. viverrini. In contrast, PLC is hyper-dominant over gallbladder in Vietnam, suggesting that the role played by flukes is less important in this country. All values have been calculated from Globocan 2018 https://gco.iarc.fr/today/home, accessed on 15 October 2020.
Figure 1.
(A) Incidence of primary liver cancer (PLC) in Laos and neighboring countries. Myanmar is clearly less affected than all other countries of the region. (B) Male to female M:F sex ratios of PLC in the same countries. An increased sex ratio is observed in Vietnam suggesting a strong dominance of hepatitis B virus in PLC etiology. (C) Ratios of liver cancer/gallbladder cancer in the region. The low ratio observed in Thailand indicates the epidemiological importance of gallbladder and bile ducts carcinomas cases supposedly triggered by O. viverrini. In contrast, PLC is hyper-dominant over gallbladder in Vietnam, suggesting that the role played by flukes is less important in this country. All values have been calculated from Globocan 2018 https://gco.iarc.fr/today/home, accessed on 15 October 2020.

Figure 2.
Traditional alcohol production device still in use in the Sayaboury province of Laos.

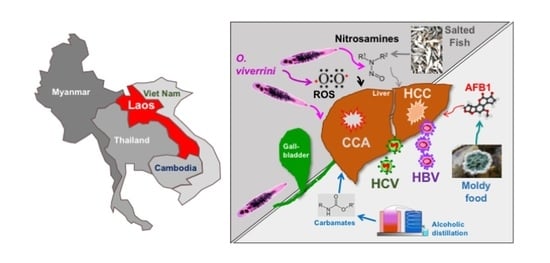
Figure 3.
Schematic representation of the liver carcinogenic risk factors strongly prevalent in Laos. O. viverrini: Opisthorchis viverrini, ROS: radical oxygen species, HCC: hepatocellular carcinoma, CCA: cholangiocarcinoma, HBV: hepatitis B virus, HCV: hepatitis C virus, AFB1: aflatoxin B1.
Figure 3.
Schematic representation of the liver carcinogenic risk factors strongly prevalent in Laos. O. viverrini: Opisthorchis viverrini, ROS: radical oxygen species, HCC: hepatocellular carcinoma, CCA: cholangiocarcinoma, HBV: hepatitis B virus, HCV: hepatitis C virus, AFB1: aflatoxin B1.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sitbounlang, P.; Marchio, A.; Deharo, E.; Paboriboune, P.; Pineau, P. The Threat of Multiple Liver Carcinogens in the Population of Laos: A Review. Livers 2021, 1, 49-59. https://doi.org/10.3390/livers1010005
AMA Style
Sitbounlang P, Marchio A, Deharo E, Paboriboune P, Pineau P. The Threat of Multiple Liver Carcinogens in the Population of Laos: A Review. Livers. 2021; 1(1):49-59. https://doi.org/10.3390/livers1010005
Chicago/Turabian StyleSitbounlang, Philavanh, Agnès Marchio, Eric Deharo, Phimpha Paboriboune, and Pascal Pineau. 2021. "The Threat of Multiple Liver Carcinogens in the Population of Laos: A Review" Livers 1, no. 1: 49-59. https://doi.org/10.3390/livers1010005