
Does Needle Design Affect the Regenerative Potential of Bone Marrow Aspirate? An In Vitro Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
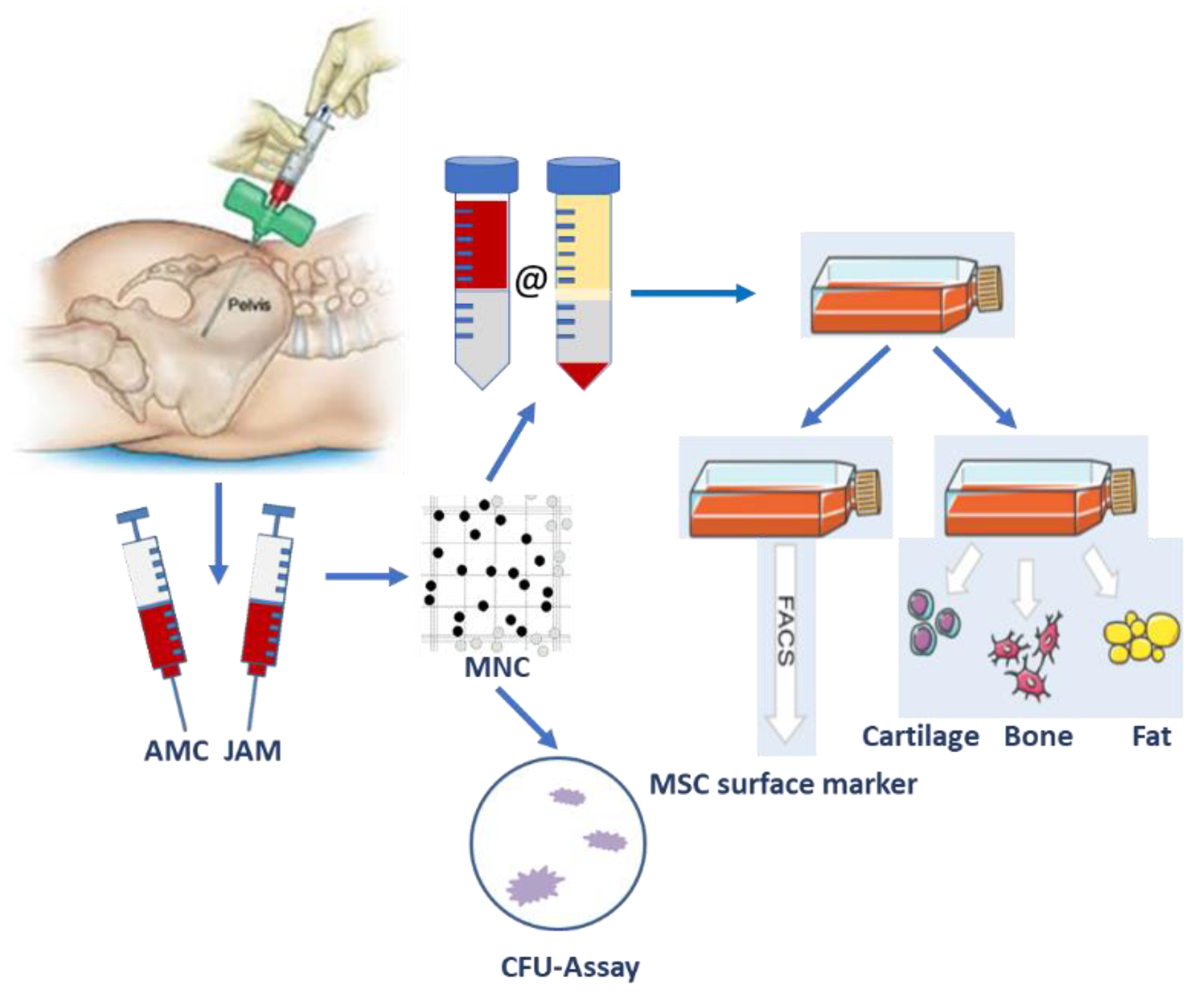
2.2. Bone Marrow Aspirate Sampling
2.3. Therapeutic Application
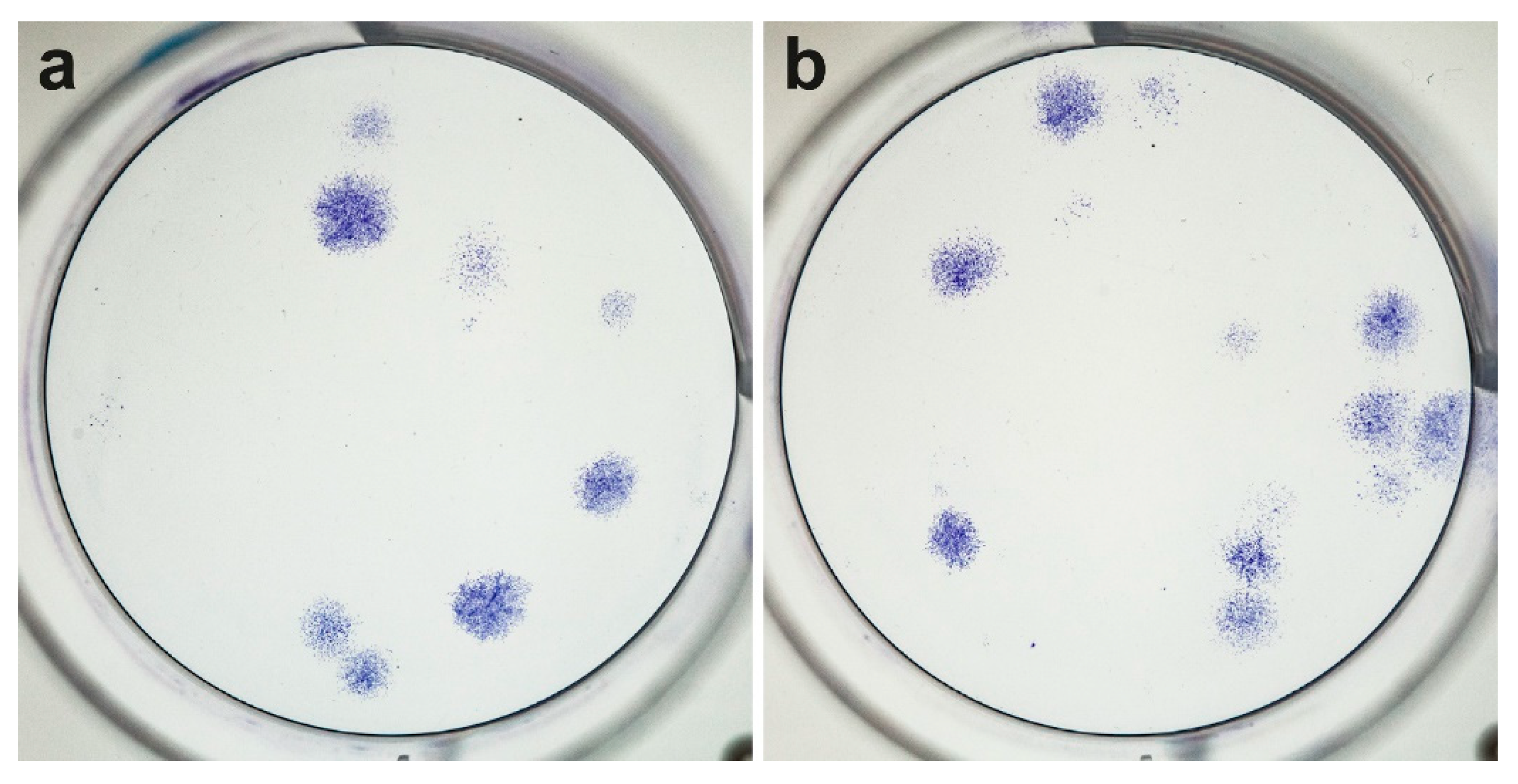
2.4. Cell Isolation and Colony-Forming Unit (CFU) Assay
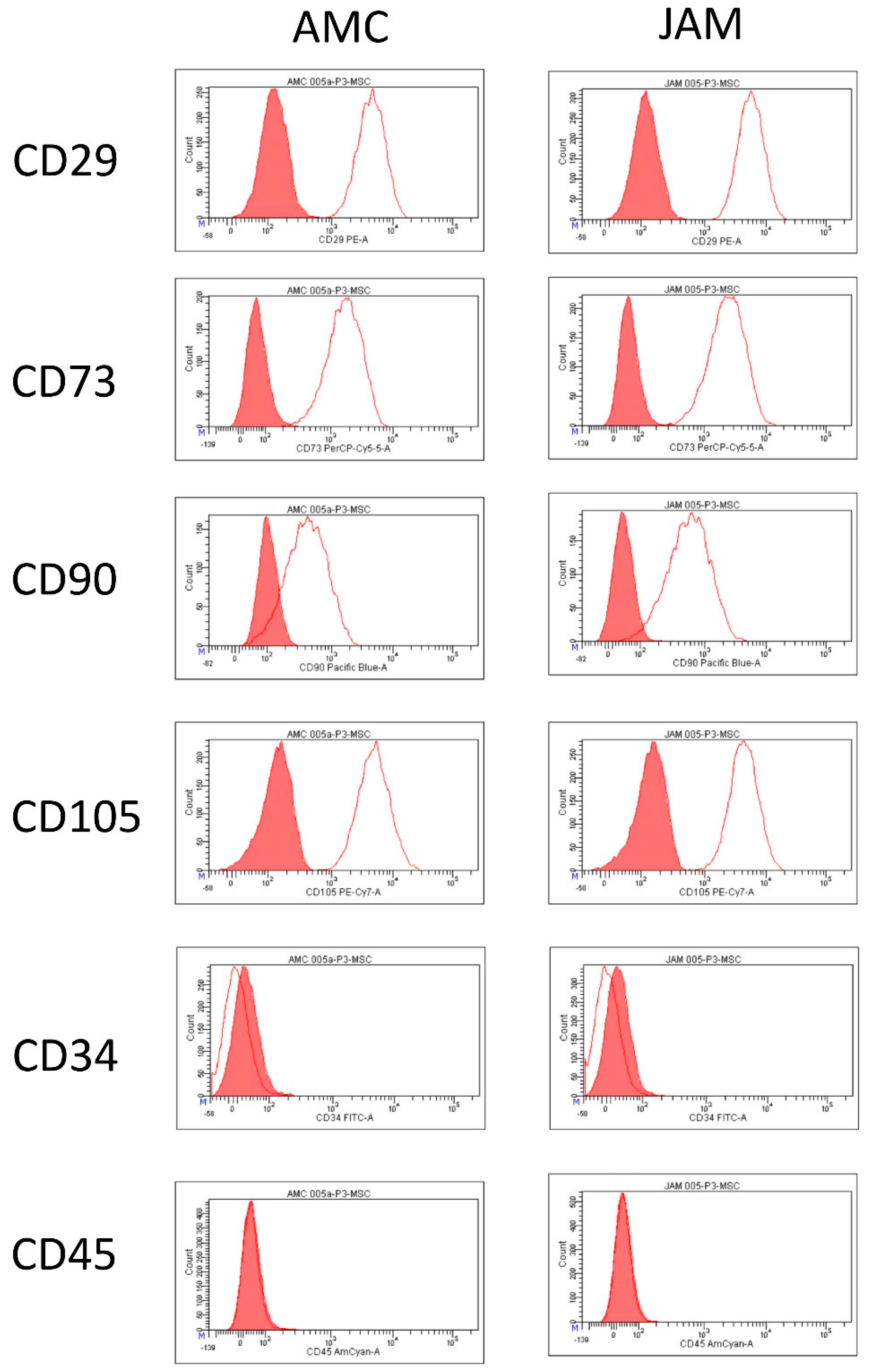
2.5. Flow Cytometric Characterization of MSCs
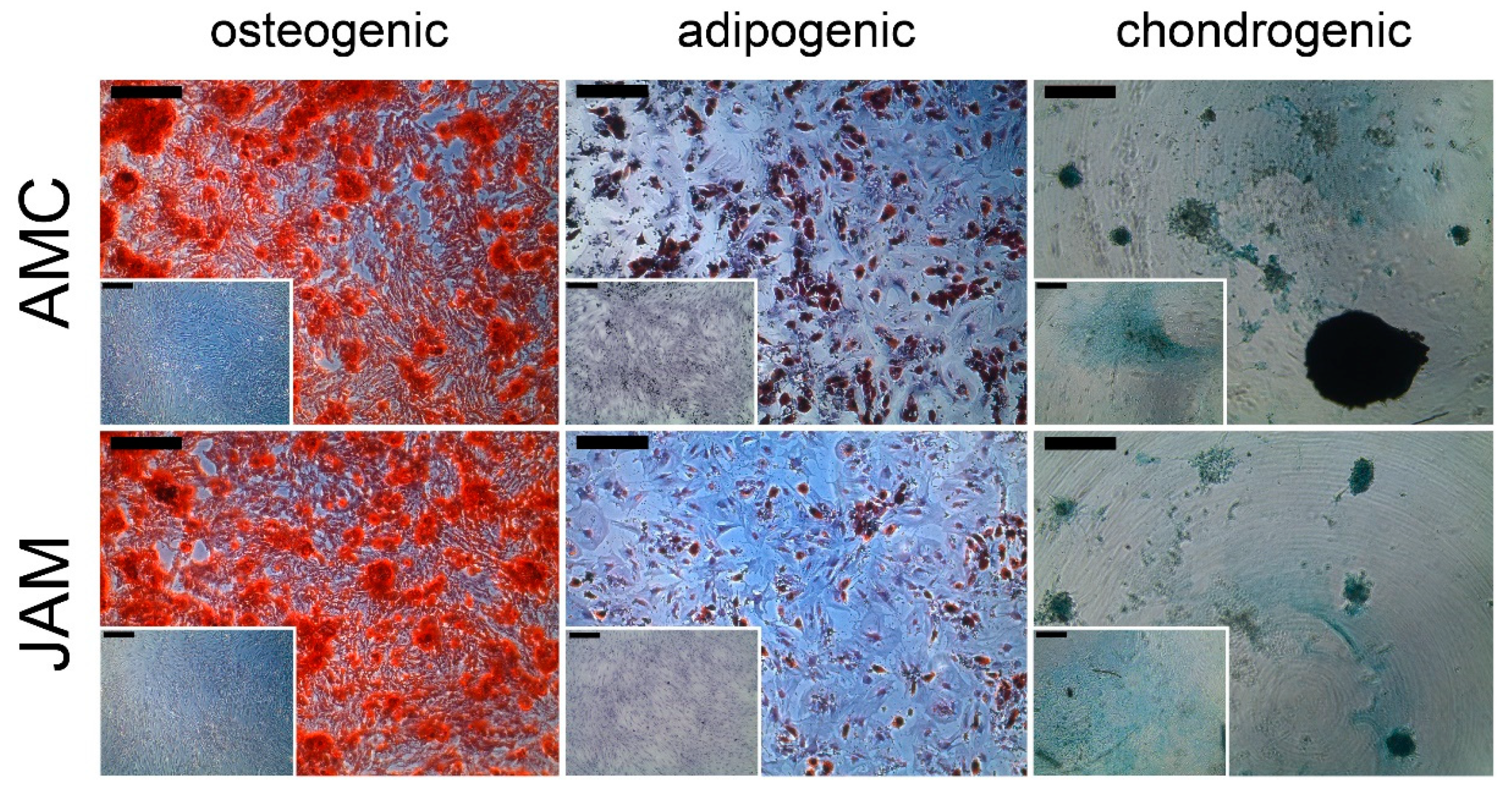
2.6. Cell Differentiation into the Three Lineages (Osteogenic, Adipogenic, Chondrogenic)
2.7. Statistics
3. Results
3.1. Patient Demographics
3.2. Mononuclear Cells–Yield and Generation Time
3.3. Regeneration Potential Based on the CFUs
3.4. Flow Cytometric Analysis and Differentiation Potential
4. Discussion
4.1. Previous Experience with the New AMC Needle
4.2. Multiple-Site Drawing Method
4.3. Comparing Harvesting Techniques
4.4. Further Processing of the Aspirate
4.5. Increasing the Local Concentration of MSCs
4.6. Increasing Clinical Relevance of Cell-Based Therapies with Bone Marrow Stromal Cells
4.7. How Many Cells Are Required to Heal a Bone Defect?
4.8. Limitations of the Present Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Evans, C.H. Advances in Regenerative Orthopedics. Mayo Clin. Proc. 2013, 88, 1323–1339. [Google Scholar] [CrossRef] [Green Version]
- Khan, Y.; Yaszemski, M.J.; Mikos, A.G.; Laurencin, C.T. Tissue engineering of bone: Material and matrix considerations. J. Bone Joint Surg. Am. 2008, 90 (Suppl. 1), 36–42. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.; Alcelik, I.; Bhatia, C.; Chuter, G.; Lingutla, K.; Budithi, C.; Krishna, M. Donor site morbidity following iliac crest bone harvesting for cervical fusion: A comparison between minimally invasive and open techniques. Eur. Spine J. 2008, 17, 845–852. [Google Scholar] [CrossRef] [Green Version]
- Busch, A.; Wegner, A.; Haversath, M.; Jäger, M. Bone Substitutes in Orthopaedic Surgery: Current Status and Future Perspectives. Z. Orthop. Unfall. 2021, 159, 304–313. [Google Scholar] [CrossRef]
- Kaur, G.; Kumar, V.; Baino, F.; Mauro, J.C.; Pickrell, G.; Evans, I.; Bretcanu, O. Mechanical properties of bioactive glasses, ceramics, glass-ceramics and composites: State-of-the-art review and future challenges. Mater. Sci. Eng. C 2019, 104, 109895. [Google Scholar] [CrossRef]
- Sallent, I.; Capella-Monsonís, H.; Procter, P.; Bozo, I.Y.; Deev, R.V.; Zubov, D.; Vasyliev, R.; Perale, G.; Pertici, G.; Baker, J.; et al. The few who made it: Commercially and clinically successful innovative bone grafts. Front. Bioeng. Biotechnol. 2020, 8, 952. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, R.M.; Kelly, C.M. The effect of AlloMatrix injectable putty on the outcome of long bone applications. Orthopedics 2003, 26, s567–s570. [Google Scholar] [CrossRef] [PubMed]
- Simpson, A.H.R.W.; Mills, L.; Noble, B. The role of growth factors and related agents in accelerating fracture healing. J. Bone Joint Surg. Br. 2006, 88, 701–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieske, O.; Wittmann, A.; Zaspel, J.; Loffler, T.J.; Rubenbauer, B.; Trentzsch, H.; Piltz, S. Autologous bone graft versus demineralized bone matrix in internal fixation of ununited long bones. J. Trauma Manag. Outcomes 2009, 3, 11. [Google Scholar] [CrossRef] [Green Version]
- De Grado, G.F.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Cavagna, R.; Daculsi, G.; Bouler, J.-M. Macroporous calcium phosphate ceramic: A prospective study of 106 cases in lumbar spinal fusion. J. Long Term Eff. Med. Implants 1999, 9, 403–412. [Google Scholar]
- Hernigou, P.; Beaujean, F. Treatment of Osteonecrosis with Autologous Bone Marrow Grafting. Clin. Orthop. Relat. Res. 2002, 405, 14–23. [Google Scholar] [CrossRef]
- Jager, M.; Jelinek, E.; Wess, K.; Scharfstadt, A.; Jacobson, M.; Kevy, S.; Krauspe, R. Bone Marrow Concentrate: A Novel Strategy for Bone Defect Treatment. Curr. Stem Cell Res. Ther. 2009, 4, 34–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jäger, M.; Herten, M.; Fochtmann, U.; Fischer, J.; Hernigou, P.; Zilkens, C.; Hendrich, C.; Krauspe, R. Bridging the gap: Bone marrow aspiration concentrate reduces autologous bone grafting in osseous defects. J. Orthop. Res. 2010, 29, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Poignard, A.; Beaujean, F.; Rouard, H. Percutaneous Autologous Bone-Marrow Grafting for NonunionsInfluence of the Number and Concentration of Progenitor Cells. J. Bone Joint Surg. Am. 2005, 87, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Gessmann, J.; Köller, M.; Godry, H.; Schildhauer, T.; Seybold, D. Regenerate augmentation with bone marrow concentrate after traumatic bone loss. Orthop. Rev. 2012, 4, e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Wang, W.; Yin, Z.S. Treatment of osteonecrosis of the femoral head with thorough debridement, bone grafting and bone-marrow mononuclear cells implantation. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 197–202. [Google Scholar] [CrossRef]
- Ajiboye, R.M.; Hamamoto, J.T.; Eckardt, M.A.; Wang, J.C. Clinical and radiographic outcomes of concentrated bone marrow aspirate with allograft and demineralized bone matrix for posterolateral and interbody lumbar fusion in elderly patients. Eur. Spine J. 2015, 24, 2567–2572. [Google Scholar] [CrossRef]
- Vogl, M.; Fischer, J.; Jäger, M.; Zilkens, C.; Krauspe, R.; Herten, M. Can thrombin-activated platelet releasate compensate the age-induced decrease in cell proliferation of MSC? J. Orthop. Res. 2013, 31, 1786–1795. [Google Scholar] [CrossRef]
- Ajiboye, R.M.; Eckardt, M.A.; Hamamoto, J.T.; Sharma, A.; Khan, A.Z.; Wang, J.C. Does age influence the efficacy of demineralized bone matrix enriched with concentrated bone marrow aspirate in lumbar fusions? Clin. Spine Surg. 2018, 31, E30–E35. [Google Scholar] [CrossRef] [PubMed]
- Hegde, V.; Shonuga, O.; Ellis, S.; Fragomen, A.; Kennedy, J.; Kudryashov, V.; Lane, J.M. A prospective comparison of 3 approved systems for autologous bone marrow concentration demonstrated nonequivalency in progenitor cell number and concentration. J. Orthop. Trauma 2014, 28, 591–598. [Google Scholar] [CrossRef] [Green Version]
- Hernigou, P.; Homma, Y.; Lachaniette, C.-H.F.; Poignard, A.; Allain, J.; Chevallier, N.; Rouard, H. Benefits of small volume and small syringe for bone marrow aspirations of mesenchymal stem cells. Int. Orthop. 2013, 37, 2279–2287. [Google Scholar] [CrossRef] [PubMed]
- PPiuzzi, N.S.; Mantripragada, V.P.; Sumski, A.; Selvam, S.; Boehm, C.; Muschler, G.F. Bone marrow-derived cellular therapies in orthopaedics. JBJS Rev. 2018, 6, e4. [Google Scholar] [CrossRef]
- Henze, K.; Herten, M.; Haversath, M.; Busch, A.; Brandau, S.; Hackel, A.; Flohé, S.B.; Jäger, M. Surgical vacuum filter-derived stromal cells are superior in proliferation to human bone marrow aspirate. Stem Cell Res. Ther. 2019, 10, 338. [Google Scholar] [CrossRef] [Green Version]
- El-Jawhari, J.; Ilas, D.; Jones, W.; Cuthbert, R.; Jones, E.; Giannoudis, P. Enrichment and preserved functionality of multipotential stromal cells in bone marrow concentrate processed by vertical centrifugation. Eur. Cells Mater. 2020, 40, 58–73. [Google Scholar] [CrossRef]
- Montgomery, F.U. Richtlinie zur Herstellung und Anwendung von hämatopoetischen Stammzellzubereitungen—Erste Fortschreibung. In Guideline for the Production and Use of Hematopoietic Stem Cell Preparations—First Update; Deutsches Ärzteblatt: Cologne, Germany, 2019; Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/downloads/pdf-Ordner/RL/2019-03-15_Bek_RiLi_Haematop_Online_FINAL.pdf. (accessed on 21 July 2021).
- Rennerfeldt, D.A.; Van Vliet, K.J. Concise review: When colonies are not clones: Evidence and implications of intracolony heterogeneity in mesenchymal stem cells. Stem Cells 2016, 34, 1135–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Fulwyler, M.J. Electronic separation of biological cells by volume. Science 1965, 150, 910–911. [Google Scholar] [CrossRef]
- Vallone, V.F.; Romaniuk, M.; Choi, H.; Labovsky, V.; Otaegui, J.; Chasseing, N. Mesenchymal stem cells and their use in therapy: What has been achieved? Differentiation 2013, 85, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Krampera, M.; Galipeau, J.; Shi, Y.; Tarte, K.; Sensebe, L.; MSC Committee of the International Society for Cellular Therapy (ISCT). Immunological characterization of multipotent mesenchymal stromal cells—The International Society for Cellular Therapy (ISCT) working proposal. Cytotherapy 2013, 15, 1054–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herten, M.; Sager, M.; Benga, L.; Fischer, J.; Jäger, M.; Betsch, M.; Wild, M.; Hakimi, M.; Jungbluth, P.; Grassmann, J.P. Bone marrow concentrate for autologous transplantation in minipigs. Vet Comp. Orthop. Traumatol. 2013, 26, 34–41. [Google Scholar] [CrossRef]
- Scarpone, M.; Kuebler, D.; Chambers, A.; De Filippo, C.M.; Amatuzio, M.; Ichim, T.E.; Patel, A.N.; CaraDonna, E. Isolation of clinically relevant concentrations of bone marrow mesenchymal stem cells without centrifugation. J. Transl. Med. 2019, 17, 10. [Google Scholar] [CrossRef]
- Oliver, K.; Awan, T.; Bayes, M. Single- versus multiple-site harvesting techniques for bone marrow concentrate: Evaluation of aspirate quality and pain. Orthop. J. Sports Med. 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jäger, M.; Hernigou, P.; Zilkens, C.; Herten, M.; Li, X.; Fischer, J.; Krauspe, R. Cell therapy in bone healing disorders. Orthop. Rev. 2010, 2, e20. [Google Scholar] [CrossRef] [Green Version]
- Muschler, G.F.; Boehm, C.; Easley, K. Aspiration to obtain osteoblast progenitor cells from human bone marrow. J. Bone Joint Surg. Am. 1997, 79, 1699–1709. [Google Scholar] [CrossRef]
- Anz, A.W.; Hubbard, R.; Rendos, N.; Everts, P.A.; Andrews, J.R.; Hackel, J.G. Bone marrow aspirate concentrate is equivalent to platelet-rich plasma for the treatment of knee osteoarthritis at 1 year: A prospective, randomized trial. Orthop. J. Sports Med. 2020, 8. [Google Scholar] [CrossRef] [Green Version]
- Gan, Y.; Dai, K.; Zhang, P.; Tang, T.; Zhu, Z.; Lu, J. The clinical use of enriched bone marrow stem cells combined with porous beta-tricalcium phosphate in posterior spinal fusion. Biomaterials 2008, 29, 3973–3982. [Google Scholar] [CrossRef] [PubMed]
- Kevy, S.V. Point of care concentrated bone marrow: A substitute for autograft. Bone Jt. J. 2018, 91, 332. [Google Scholar]
- Shapiro, S.A.; Kazmerchak, S.E.; Heckman, M.G.; Zubair, A.C.; O’Connor, M.I. A prospective, single-blind, placebo-controlled trial of bone marrow aspirate concentrate for knee osteoarthritis. Am. J. Sports Med. 2017, 45, 82–90. [Google Scholar] [CrossRef]
- Hyer, C.F.; Berlet, G.C.; Bussewitz, B.W.; Hankins, T.; Ziegler, H.L.; Philbin, T.M. Quantitative assessment of the yield of osteoblastic connective tissue progenitors in bone marrow aspirate from the iliac crest, tibia, and calcaneus. J. Bone Joint Surg. Am. 2013, 95, 1312–1316. [Google Scholar] [CrossRef] [PubMed]
- Vasiliadis, A.V.; Galanis, N. Human bone marrow-derived mesenchymal stem cells from different bone sources: A panorama. Stem Cell Investig. 2020, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- McLain, R.F.; Fleming, J.E.; Boehm, C.A.; Muschler, G.F. Aspiration of osteoprogenitor cells for augmenting spinal fusion. J. Bone Joint Surg. Am. 2005, 87, 2655–2661. [Google Scholar] [CrossRef] [Green Version]
- Odejide, O.O.; Cronin, A.M.; DeAngelo, D.J.; Bernazzoli, Z.A.; Jacobson, J.O.; Rodig, S.J.; LaCasce, A.S.; Mazeika, T.J.; Earles, K.D.; Abel, G.A. Improving the quality of bone marrow assessment. Cancer 2013, 119, 3472–3478. [Google Scholar] [CrossRef]
- Swords, R.T.; Anguita, J.; A Higgins, R.; Yunes, A.C.; Naski, M.; Padmanabhan, S.; Kelly, K.R.; Mahalingam, D.; Philbeck, T.; Miller, L.; et al. A prospective randomised study of a rotary powered device (OnControl) for bone marrow aspiration and biopsy. J. Clin. Pathol. 2011, 64, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Grønkjær, M.; Hasselgren, C.F.; Østergaard, A.S.L.; Johansen, P.; Korup, J.; Bøgsted, M.; Bilgrau, A.E.; Jensen, P. Bone marrow aspiration: A randomized controlled trial assessing the quality of bone marrow specimens using slow and rapid aspiration techniques and evaluating pain intensity. Acta Haematol. 2016, 135, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Sakai, S.; Mishima, H.; Ishii, T.; Akaogi, H.; Yoshioka, T.; Uemura, T.; Ochiai, N. Concentration of bone marrow aspirate for osteogenic repair using simple centrifugal methods. Acta Orthop. 2008, 79, 445–448. [Google Scholar] [CrossRef]
- Available online: www.clinicaltrials.gov (accessed on 6 December 2020).
- Hernigou, P.; Mathieu, G.; Poignard, A.; Manicom, O.; Beaujean, F.; Rouard, H. Percutaneous autologous bone-marrow grafting for nonunions. J. Bone Joint Surg. Am. 2006, 88 Pt 2 (Suppl. 1), 322–327. [Google Scholar] [CrossRef] [Green Version]
- Lachaniette, C.-H.F.; Heyberger, C.; Bouthors, C.; Roubineau, F.; Chevallier, N.; Rouard, H.; Hernigou, P. Osteogenic progenitors in bone marrow aspirates have clinical potential for tibial non-unions healing in diabetic patients. Int. Orthop. 2016, 40, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Arthur, A.; Gronthos, S. Clinical application of bone marrow mesenchymal stem/stromal cells to repair skeletal tissue. Int. J. Mol. Sci. 2020, 21, 9759. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AMC MNC × 109 | 4.3 | 5.1 | 2.5 | 5.1 | 6.2 | 7.2 | 5.7 | 6.8 | 8.8 | 4.0 | 3.6 | 3.9 |
| JAM MNC × 109 | 8.5 | 3.3 | 2.0 | 3.3 | 4.6 | 4.0 | 4.9 | 9.9 | 7.6 | 3.1 | 3.1 | 3.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feddahi, N.; Herten, M.; Tassemeier, T.; Rekasi, H.; Hackel, A.; Haversath, M.; Jäger, M. Does Needle Design Affect the Regenerative Potential of Bone Marrow Aspirate? An In Vitro Study. Life 2021, 11, 748. https://doi.org/10.3390/life11080748
Feddahi N, Herten M, Tassemeier T, Rekasi H, Hackel A, Haversath M, Jäger M. Does Needle Design Affect the Regenerative Potential of Bone Marrow Aspirate? An In Vitro Study. Life. 2021; 11(8):748. https://doi.org/10.3390/life11080748
Chicago/Turabian StyleFeddahi, Nadia, Monika Herten, Tjark Tassemeier, Heike Rekasi, Alexander Hackel, Marcel Haversath, and Marcus Jäger. 2021. "Does Needle Design Affect the Regenerative Potential of Bone Marrow Aspirate? An In Vitro Study" Life 11, no. 8: 748. https://doi.org/10.3390/life11080748