
Needs and Demands for eHealth Pain Management Interventions in Chronic Pain Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sociodemographic, Medical, and Psychometric Data
3.2. Needs and Demands of Chronic Pain Patients
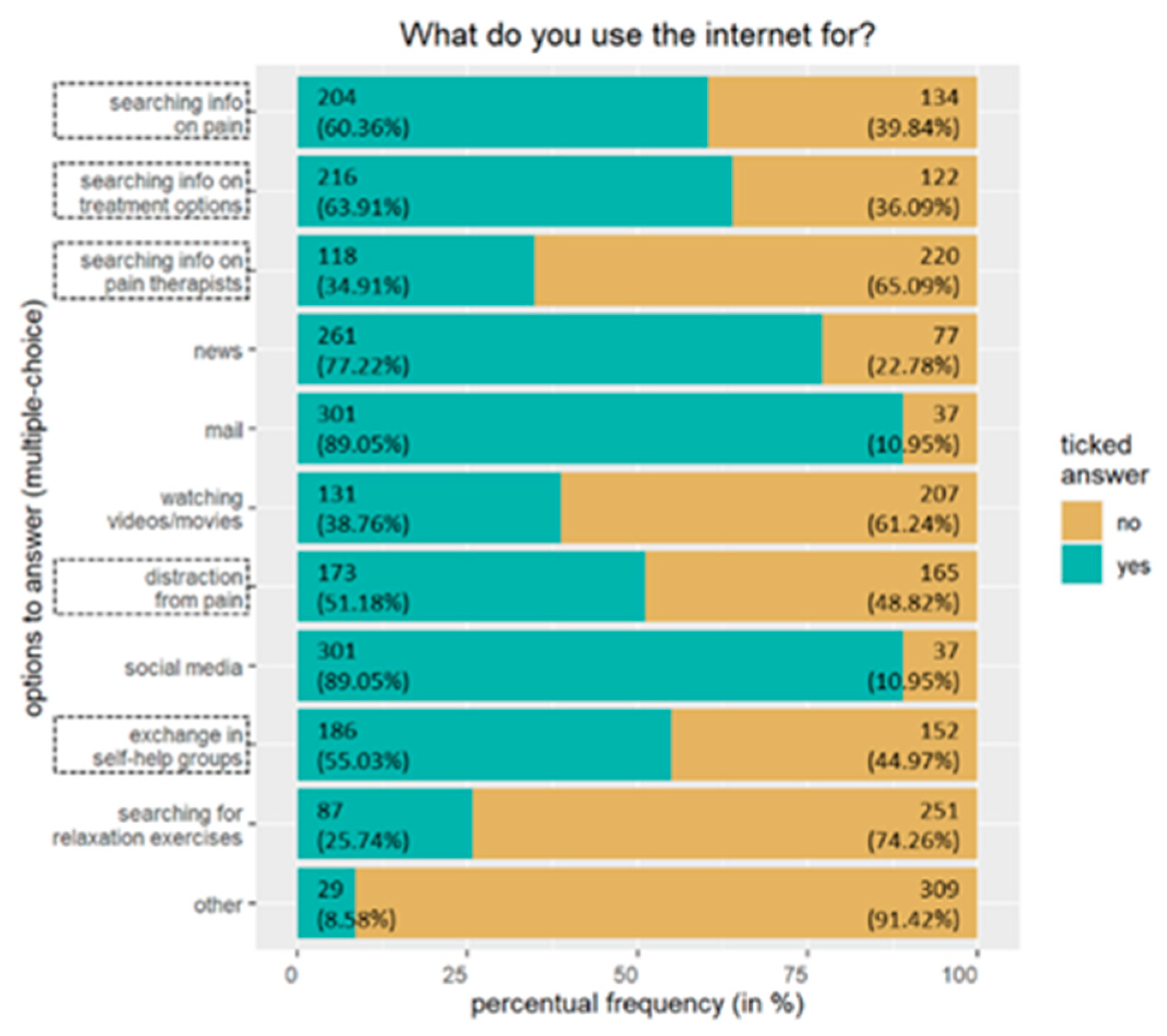
3.2.1. Internet Usage
3.2.2. eHealth: Prior Experiences
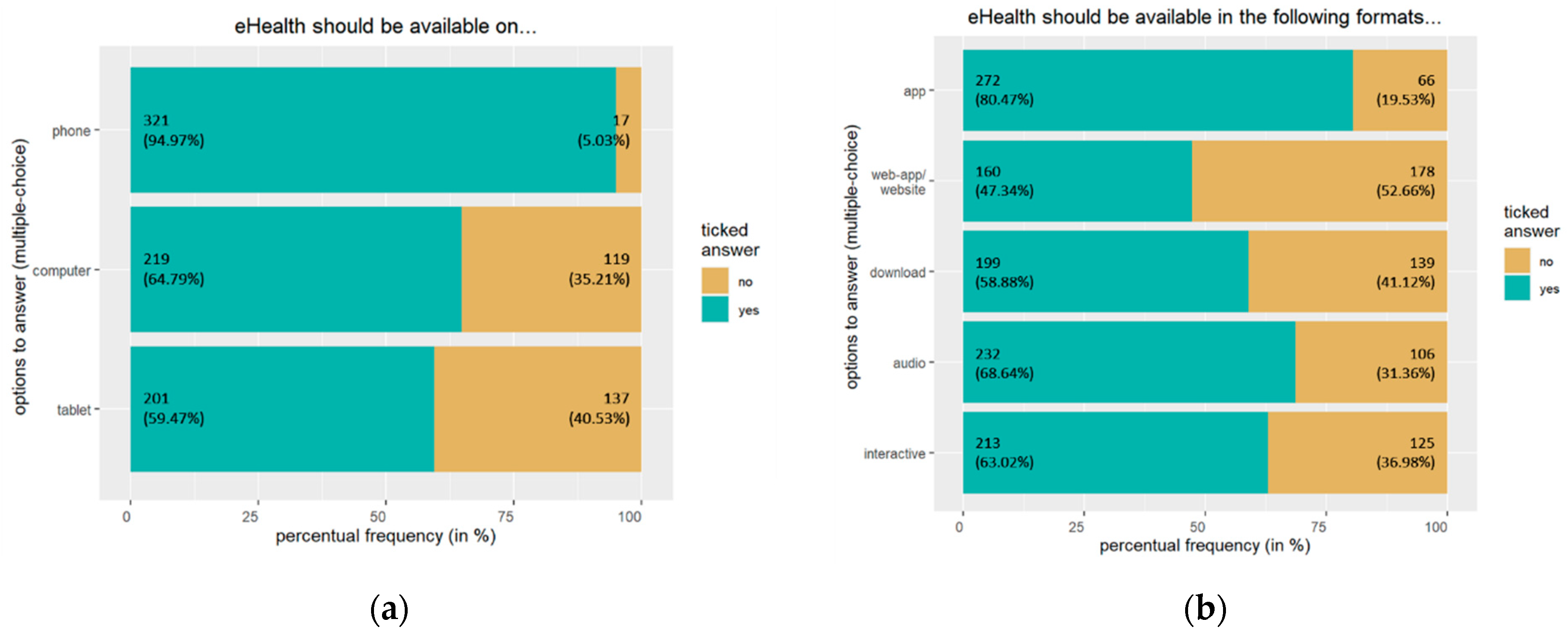
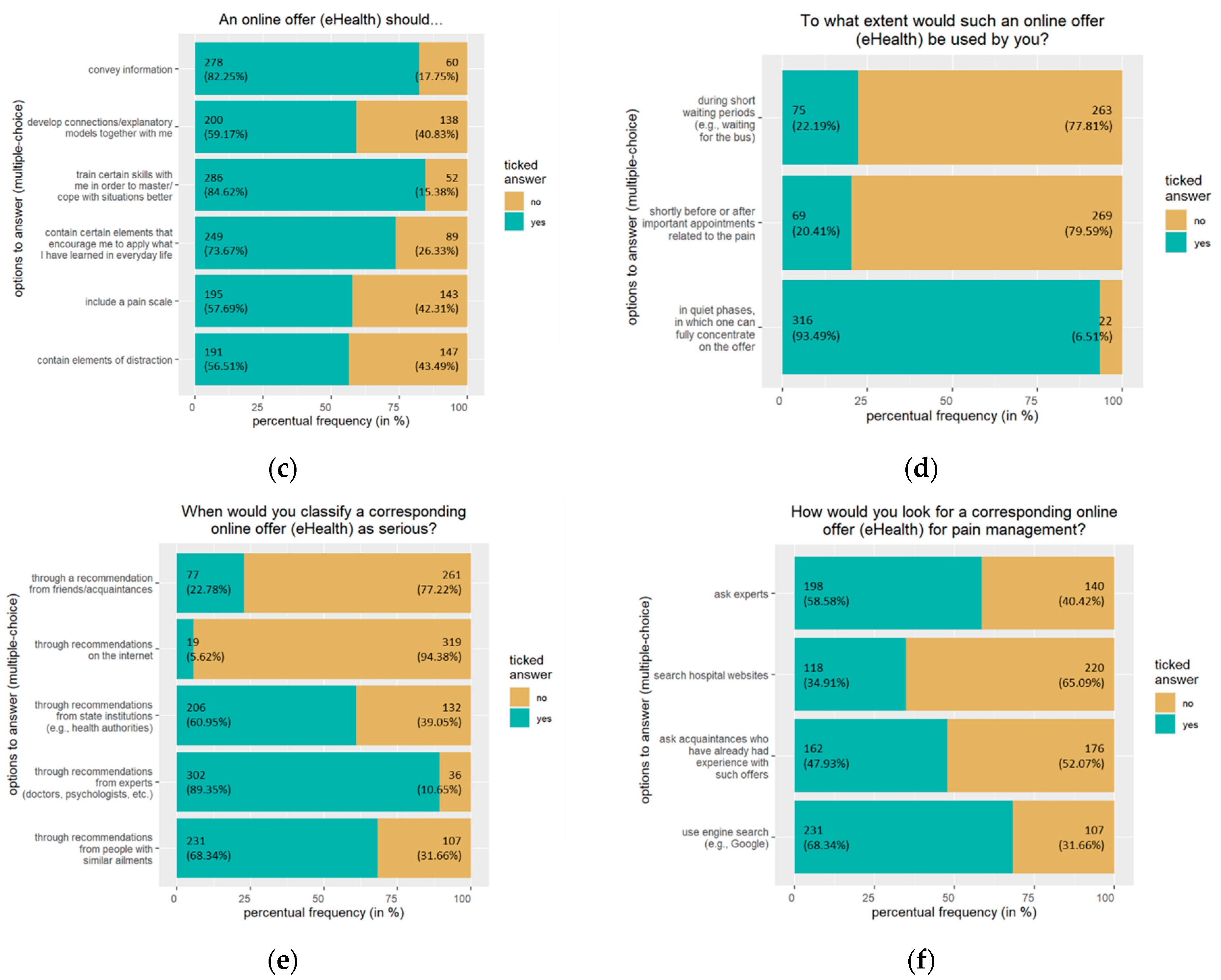
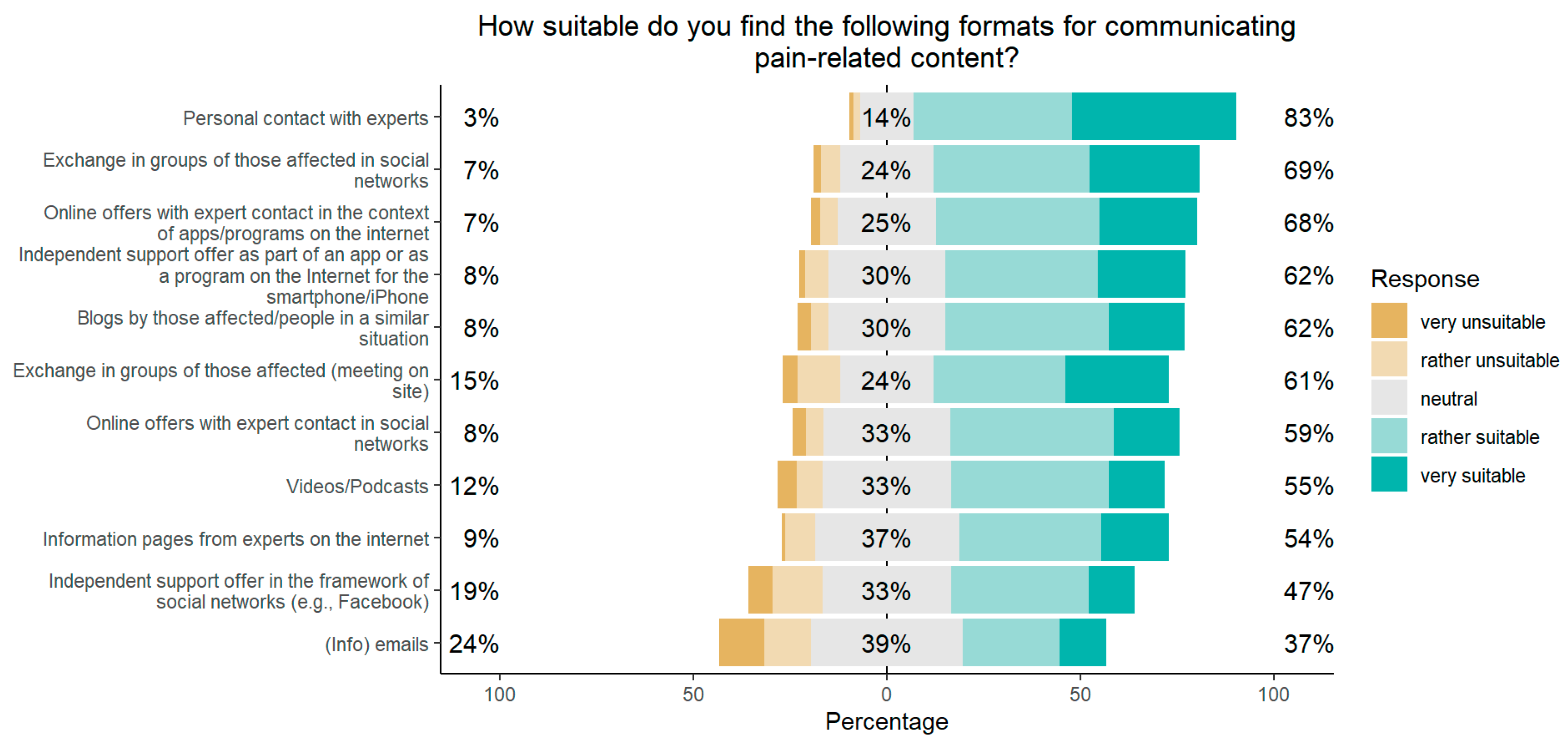
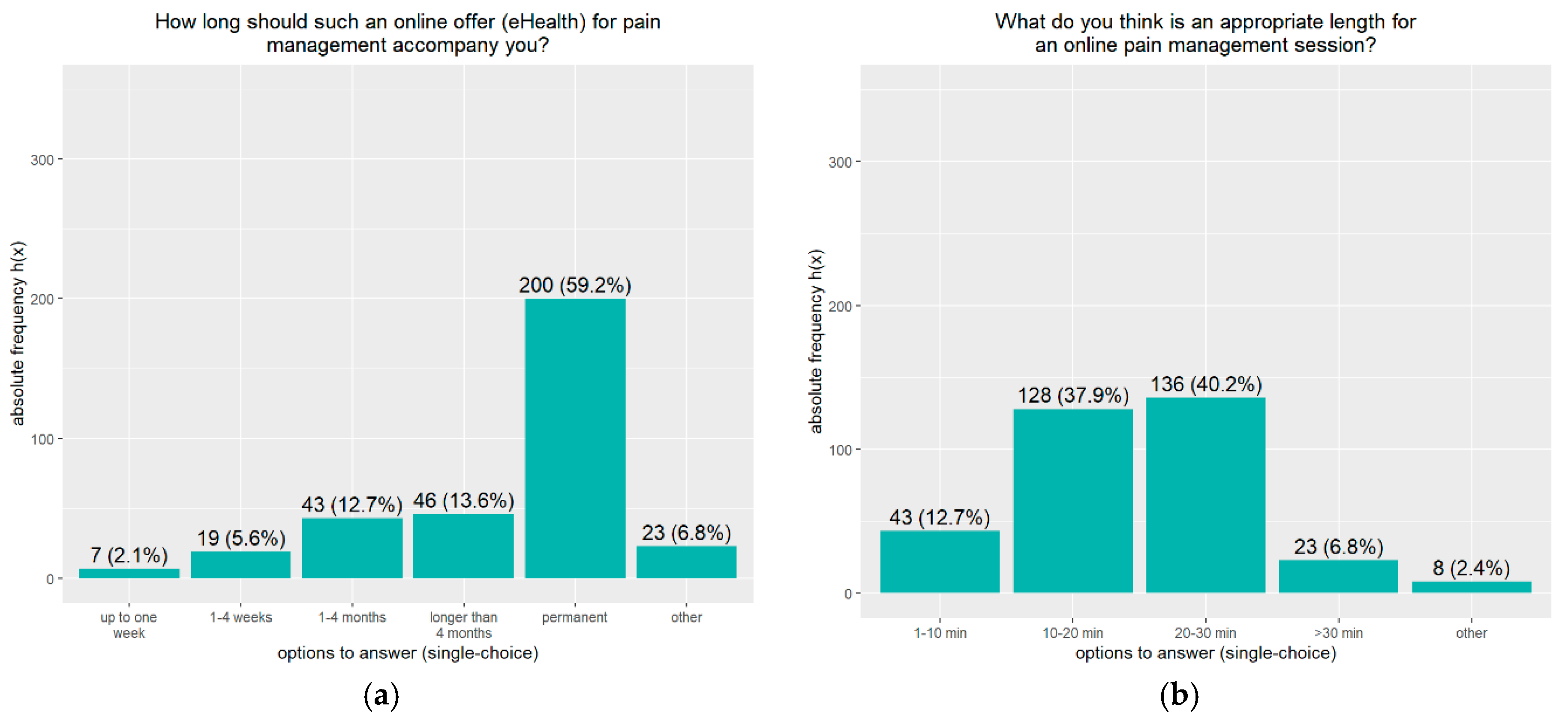
3.2.3. eHealth: Needs and Demands
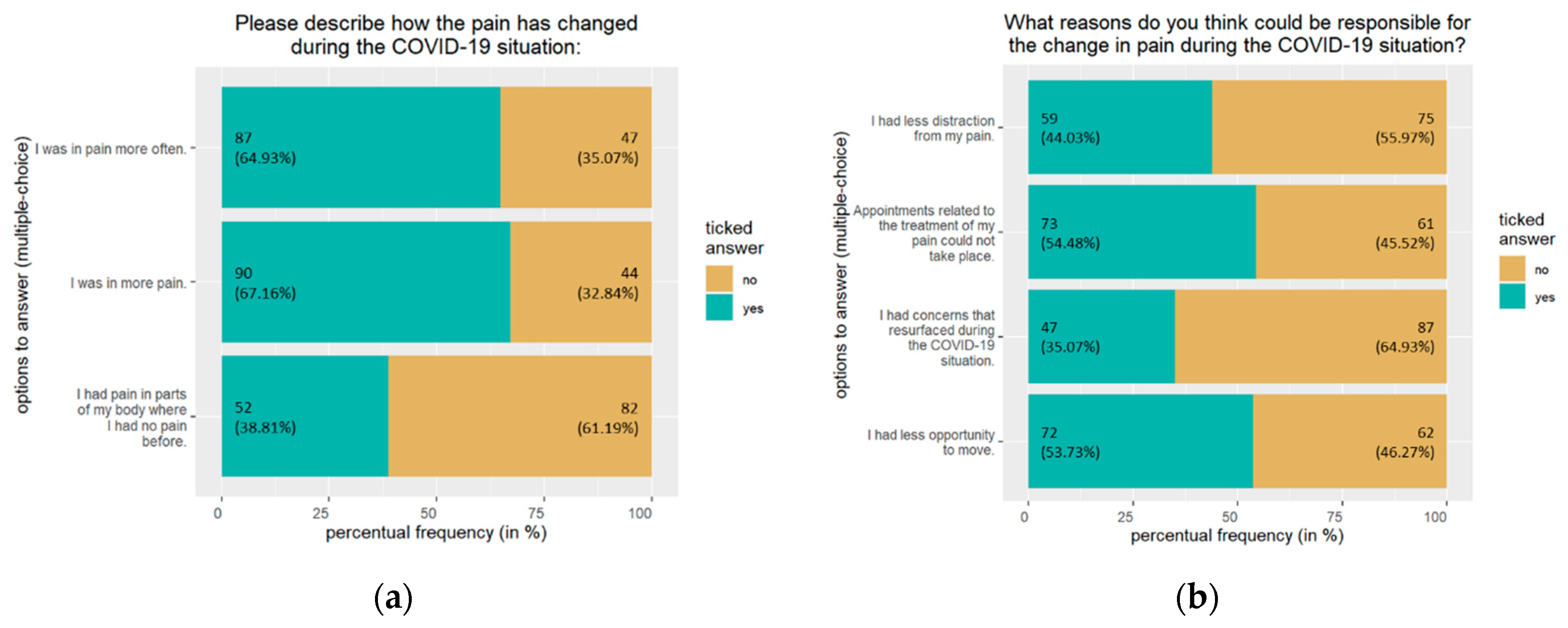
3.2.4. eHealth: Context of the COVID-19 Pandemic
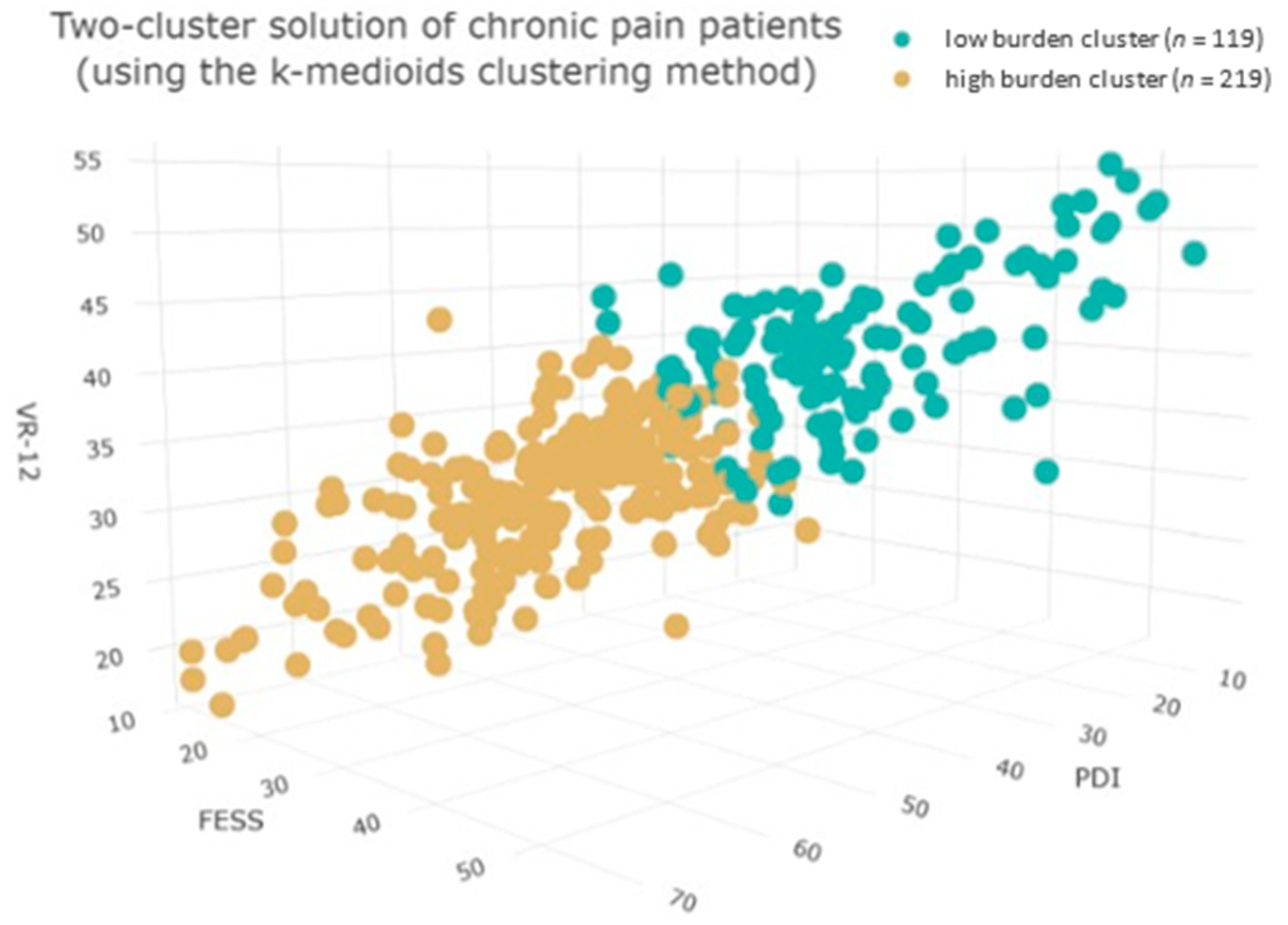
3.3. Cluster Analysis
Group Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A




Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Response Option |
|---|---|
| Do you have private internet access? | Yes/No |
How often do you use the following technologies privately?
| Never (I don’t own that)/Rather less (less than 1x/week)/Moderate (more than 1x/week)/Often (daily)/Very often (more than 1x/day) |
| How long do you use the Internet for private purposes on average per day? | 0–1 h/1–2 h/2–3 h/3–4 h/more than 4 h |
| What do you use the Internet for? | Searching for information about chronic pain/Searching for information about treatment options/Searching for information about pain therapists/News/E-mail/Watching videos/movies/To distract from pain/Social media (Facebook, Instagram, Twitter, etc.)/ Sharing with people in a similar situation/contacting support groups/Search for relaxation exercises/Other (Please name) |
Have you already had experience with online offers for pain management (e.g., Pain-T, schmerzApp, Pain Tracer, etc.)?
| Yes, I have already made use of online offers for pain management/Yes, I know about the possibility of using online offers for pain management, but I have not tried any yet./No, I am not aware of the possibility of making use of online offers for pain management |
| If you have already had experience with online offers for pain management: How would you rate your experience with the offerings? | Poor/Rather poor/Neutral/Rather good/Very good |
How appropriate do you find the following formats for teaching pain-related content?
| Very unsuitable/rather unsuitable/neutral/rather suitable/very suitable |
| eHealth pain management intervention should be available on: | Smartphone/iPhone/Computer/laptop/Tablet/iPad/Other (Please name) |
| eHealth should be available in the following formats: | Program on the Internet (web app/website)/Application (app) directly on the device/Information page on the Internet/Material for downloading/Audio/video material (e.g., relaxation exercises set to music)/Interactive tasks and exercises/Other (Please name) |
| How long should such an online offer for pain management accompany you? | Up to one week/1–4 weeks/1–4 months/Longer than four months/Permanent/Other (Please specify) |
| In what kind of frequency should the different/respectively new sessions of the online offer be available? | Daily/Weekly/Every two weeks/Other (Please name) |
| What do you think is an appropriate length for a session in the online pain management service? | 1–10 min/10–20 min/20–30 min/More than 30 min/Other (Please specify) |
| An online offer should… | convey information/work out connections/explanatory models together with me/train certain skills with me in order to better master/manage situations/include certain elements that encourage me to apply what I have learned in everyday life/include a scale to record pain/include elements for distraction/Other (Please name) |
| To what extent would such an online offer be used by you? | In short waiting periods (e.g., waiting for the bus)/Shortly before or after important appointments that are related to pain/During quiet periods when one can concentrate completely on the offer/Other (Please name) |
| When would you classify a corresponding online offer as serious? | Through a recommendation from friends/acquaintances/Through recommendations on the Internet/through recommendations from government institutions (e.g., public health department)/Through recommendations from experts (doctors, psychologists, etc.)/Through recommendations from persons with similar complaints/Other (Please name) |
| How would you look for a corresponding online offer for pain management? | Asking experts/Searching the homepages of hospitals/Asking acquaintances who have already had experience with corresponding offers/Searching in search engines (e.g., Google)/Other (Please name) |
References
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef] [PubMed]
- Eccleston, C.; Blyth, F.M.; Dear, B.F.; Fisher, E.A.; Keefe, F.J.; Lynch, M.E.; Palermo, T.M.; Reid, M.C.; Williams, A.C.C. Managing patients with chronic pain during the COVID-19 outbreak: Considerations for the rapid introduction of remotely supported (eHealth) pain management services. Pain 2020, 161, 889–893. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Nalamasu, R.; Pergolizzi, J.V.; Gharibo, C. Pain Management During the COVID-19 Pandemic. Pain Ther. 2020, 9, 453–466. [Google Scholar] [CrossRef]
- Müßgens, D.; Burgard, L.C.; Kleine-Borgmann, J.; Frettlöh, J.; Sorgatz, H.; Bingel, U. Impact of the COVID-19 pandemic on patients with chronic pain in Germany: Associations with expectations and control beliefs. Eur. J. Pain 2022, 26, 1343–1354. [Google Scholar] [CrossRef] [PubMed]
- Coluzzi, F.; Marinangeli, F.; Pergolizzi, J. Managing chronic pain patients at the time of COVID-19 pandemic. Minerva Anestesiol. 2020, 86, 797–799. [Google Scholar] [CrossRef]
- Hedman, E.; Andersson, E.; Ljótsson, B.; Andersson, G.; Rück, C.; Lindefors, N. Cost-effectiveness of Internet-based cognitive behavior therapy vs. cognitive behavioral group therapy for social anxiety disorder: Results from a randomized controlled trial. Behav. Res. Ther. 2011, 49, 729–736. [Google Scholar] [CrossRef]
- Pfeifer, A.-C.; Uddin, R.; Schröder-Pfeifer, P.; Holl, F.; Swoboda, W.; Schiltenwolf, M. Mobile Application-Based Interventions for Chronic Pain Patients: A Systematic Review and Meta-Analysis of Effectiveness. J. Clin. Med. 2020, 9, 3557. [Google Scholar] [CrossRef]
- Macea, D.D.; Gajos, K.; Daglia Calil, Y.A.; Fregni, F. The Efficacy of Web-Based Cognitive Behavioral Interventions for Chronic Pain: A Systematic Review and Meta-Analysis. J. Pain 2010, 11, 917–929. [Google Scholar] [CrossRef]
- Enam, A.; Torres-Bonilla, J.; Eriksson, H. Evidence-Based Evaluation of eHealth Interventions: Systematic Literature Review. J. Med. Internet Res. 2018, 20, e10971. [Google Scholar] [CrossRef]
- Rigby, M.; Ammenwerth, E. The need for evidence in health informatics. Stud. Health Technol. Inf. 2016, 222, 3–13. [Google Scholar] [CrossRef]
- Thurnheer, S.E.; Gravestock, I.; Pichierri, G.; Steurer, J.; Burgstaller, J.M. Benefits of Mobile Apps in Pain Management: Systematic Review. JMIR Mhealth Uhealth 2018, 6, e11231. [Google Scholar] [CrossRef]
- Cranen, K.; Groothuis-Oudshoorn, C.G.; Vollenbroek-Hutten, M.M.; MJ, I.J. Toward Patient-Centered Telerehabilitation Design: Understanding Chronic Pain Patients’ Preferences for Web-Based Exercise Telerehabilitation Using a Discrete Choice Experiment. J. Med. Internet Res. 2017, 19, e26. [Google Scholar] [CrossRef]
- Cranen, K.; Drossaert, C.H.; Brinkman, E.S.; Braakman-Jansen, A.L.; Ijzerman, M.J.; Vollenbroek-Hutten, M.M. An exploration of chronic pain patients’ perceptions of home telerehabilitation services. Health Expect. 2012, 15, 339–350. [Google Scholar] [CrossRef]
- Terhorst, Y.; Messner, E.-M.; Schultchen, D.; Paganini, S.; Portenhauser, A.; Eder, A.-S.; Bauer, M.; Papenhoff, M.; Baumeister, H.; Sander, L.B. Systematic evaluation of content and quality of English and German pain apps in European app stores. Internet Interv. 2021, 24, 100376. [Google Scholar] [CrossRef]
- Solem, I.K.L.; Varsi, C.; Eide, H.; Kristjansdottir, O.B.; Børøsund, E.; Schreurs, K.M.G.; Waxenberg, L.B.; Weiss, K.E.; Morrison, E.J.; Haaland-Øverby, M.; et al. A User-Centered Approach to an Evidence-Based Electronic Health Pain Management Intervention for People with Chronic Pain: Design and Development of EPIO. J. Med. Internet Res. 2020, 22, e15889. [Google Scholar] [CrossRef]
- van Gemert-Pijnen, J.E.; Nijland, N.; van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A holistic framework to improve the uptake and impact of eHealth technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef]
- Eysenbach, G. The Law of Attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems 11th Revision: The Global Standard for Diagnostic Health Information. Available online: https://icd.who.int/ (accessed on 17 September 2022).
- Tait, R.C.; Pollard, C.A.; Margolis, R.B.; Duckro, P.N.; Krause, S.J. The Pain Disability Index: Psychometric and validity data. Arch. Phys. Med. Rehabil. 1987, 68, 438–441. [Google Scholar] [PubMed]
- Blanz, M. Forschungsmethoden und Statistik für Die Soziale Arbeit: Grundlagen und Anwendungen; Kohlhammer Verlag: Stuttgart, Germany, 2021. [Google Scholar]
- Buchholz, I.; Kohlmann, T.; Buchholz, M. Vergleichende Untersuchung der Psychometrischen Eigenschaften des SF-36/SF-12 vs VR-36/VR-12; Institut für Community Medicine der Universitätsmedizin Greifswald: Greifswald, Germany, 2017; Available online: https://www.reha-vffr.de/images/vffrpdf/projekte/2017/VR-Abschlussbericht_vffr205.pdf (accessed on 11 April 2023).
- Buchholz, I.; Feng, Y.-S.; Buchholz, M.; Kazis, L.E.; Kohlmann, T. Translation and Adaptation of the German Version of the Veterans Rand—36/12 Item Health Survey. Health Qual. Life Outcomes 2021, 19, 137. [Google Scholar] [CrossRef] [PubMed]
- Hüppe, M.; Schneider, K.; Casser, H.-R.; Knille, A.; Kohlmann, T.; Lindena, G.; Nagel, B.; Nelles, J.; Pfingsten, M.; Petzke, F. Kennwerte und teststatistische Güte des Veterans RAND 12-Item Health Survey (VR-12) bei Patienten mit chronischem Schmerz. Schmerz 2022, 36, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Selim, A.J.; Rogers, W.; Fleishman, J.A.; Qian, S.X.; Fincke, B.G.; Rothendler, J.A.; Kazis, L.E. Updated U.S. population standard for the Veterans RAND 12-item Health Survey (VR-12). Qual. Life Res. 2009, 18, 43–52. [Google Scholar] [CrossRef]
- Mangels, M.; Schwarz, S.; Sohr, G.; Holme, M.; Rief, W. Der Fragebogen zur Erfassung der schmerzspezifischen Selbstwirksamkeit (FESS). Diagnostica 2009, 55, 84–93. [Google Scholar] [CrossRef]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 11 April 2023).
- Jin, X.; Han, J. K-Medoids Clustering. In Encyclopedia of Machine Learning and Data Mining; Sammut, C., Webb, G.I., Eds.; Springer: Boston, MA, USA, 2017; pp. 697–700. [Google Scholar]
- Lüdecke, M.; Ben-Shachar, P.; Højsgaard, W.L.; Arel-Bundock, G.; Maimone, O.; Ezra, M. Luchman Package ‘Parameters’: Processing of Model Parameters. Available online: https://cran.r-project.org/web/packages/parameters/parameters.pdf (accessed on 17 September 2022).
- Goldberg, D.S.; McGee, S.J. Pain as a global public health priority. BMC Public Health 2011, 11, 770. [Google Scholar] [CrossRef]
- Geiger, S.; Steinbach, J.; Skoda, E.M.; Jahre, L.; Rentrop, V.; Kocol, D.; Jansen, C.; Schüren, L.; Niedergethmann, M.; Teufel, M.; et al. Needs and Demands for e-Mental Health Interventions in Individuals with Overweight and Obesity: User-Centered Design Approach. Obes. Facts 2022, 16, 173–183. [Google Scholar] [CrossRef]
- Solem, I.K.L.; Varsi, C.; Eide, H.; Kristjansdottir, O.B.; Mirkovic, J.; Borosund, E.; Haaland-Overby, M.; Heldal, K.; Schreurs, K.M.; Waxenberg, L.B.; et al. Patients’ Needs and Requirements for eHealth Pain Management Interventions: Qualitative Study. J. Med. Internet Res. 2019, 21, e13205. [Google Scholar] [CrossRef]
- Statistisches Bundesamt (Destatis). Wirtschaftsrechnungen. Ausstattung Privater Haushalte mit Ausgewählten Gebrauchsgütern. 2022. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Einkommen-Konsum-Lebensbedingungen/Ausstattung-Gebrauchsgueter/Publikationen/Downloads-Ausstattung/ausstattung-privater-haushalte-2150200227004.pdf?__blob=publicationFile (accessed on 11 April 2023).
- Salive, M.E. Multimorbidity in older adults. Epidemiol. Rev. 2013, 35, 75–83. [Google Scholar] [CrossRef]
- Eccleston, C. Chronic pain and distraction: An experimental investigation into the role of sustained and shifting attention in the processing of chronic persistent pain. Behav. Res. Ther. 1995, 33, 391–405. [Google Scholar] [CrossRef]
- Mackintosh, C.; Elson, S.; Fernandes, T. Chronic pain: Clinical features, assessment and treatment. Nurs. Stand. 2008, 23, 48. [Google Scholar] [CrossRef]
- Dassieu, L.; Pagé, M.G.; Lacasse, A.; Laflamme, M.; Perron, V.; Janelle-Montcalm, A.; Hudspith, M.; Moor, G.; Sutton, K.; Thompson, J.M.; et al. Chronic pain experience and health inequities during the COVID-19 pandemic in Canada: Qualitative findings from the chronic pain & COVID-19 pan-Canadian study. Int. J. Equity Health 2021, 20, 147. [Google Scholar] [CrossRef]
- Lynch, M.E.; Campbell, F.; Clark, A.J.; Dunbar, M.J.; Goldstein, D.; Peng, P.; Stinson, J.; Tupper, H. A systematic review of the effect of waiting for treatment for chronic pain. Pain 2008, 136, 97–116. [Google Scholar] [CrossRef] [PubMed]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef] [PubMed]




| Variable | n 1 | (%) 2 | M 3 | (SD) 4 |
|---|---|---|---|---|
| Gender | ||||
| Male | 27 | (7.99) | ||
| Female | 310 | (91.72) | ||
| Diverse | 1 | (0.00) | ||
| Educational qualification | ||||
| University degree | 75 | (22.19) | ||
| High school diploma | 90 | (26.63) | ||
| Secondary school certificate | 131 | (38.76) | ||
| Secondary/Elementary school certificate | 38 | (11.24) | ||
| No school-leaving certificate | 0 | (0.00) | ||
| Other | 4 | (1.18) | ||
| Occupation | ||||
| Retired | 49 | (14.50) | ||
| Employed | 191 | (56.51) | ||
| Unemployed | 57 | (16.86) | ||
| Other | 41 | (12.13) | ||
| Place of residence (population size) | ||||
| Large city (>100,000) | 96 | (28.40) | ||
| Medium sized city (>20,000) | 100 | (29.59) | ||
| Small town (>5000) | 69 | (20.41) | ||
| Rural municipality (<5000) | 73 | (21.60) | ||
| Relationship status | ||||
| Single | 62 | (18.34) | ||
| Married | 170 | (50.30) | ||
| In a relationship | 70 | (20.71) | ||
| Divorced/separated | 32 | (9.47) | ||
| Widowed | 4 | (1.18) | ||
| FESS 6 | 30.02 | (10.05) | ||
| PDI 7 | 41.36 | (13.05) | ||
| VR-12 8 | 34.23 | (7.52) 5 | ||
| PCS 9 | 32.08 | (9.54) | ||
| MCS 10 | 36.38 | (11.69) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoppok, P.; Frewer, A.-L.; Schweda, A.; Geiger, S.; Skoda, E.-M.; Müßgens, D.; Bingel, U.; Teufel, M.; Bäuerle, A. Needs and Demands for eHealth Pain Management Interventions in Chronic Pain Patients. J. Pers. Med. 2023, 13, 675. https://doi.org/10.3390/jpm13040675
Stoppok P, Frewer A-L, Schweda A, Geiger S, Skoda E-M, Müßgens D, Bingel U, Teufel M, Bäuerle A. Needs and Demands for eHealth Pain Management Interventions in Chronic Pain Patients. Journal of Personalized Medicine. 2023; 13(4):675. https://doi.org/10.3390/jpm13040675
Chicago/Turabian StyleStoppok, Paula, Anna-Lena Frewer, Adam Schweda, Sheila Geiger, Eva-Maria Skoda, Diana Müßgens, Ulrike Bingel, Martin Teufel, and Alexander Bäuerle. 2023. "Needs and Demands for eHealth Pain Management Interventions in Chronic Pain Patients" Journal of Personalized Medicine 13, no. 4: 675. https://doi.org/10.3390/jpm13040675