

Arthrodesis of the Proximal Interphalangeal Joint of the Finger—A Biomechanical Study of Primary Stability
 , ,
, ,
Abstract
:1. Introduction
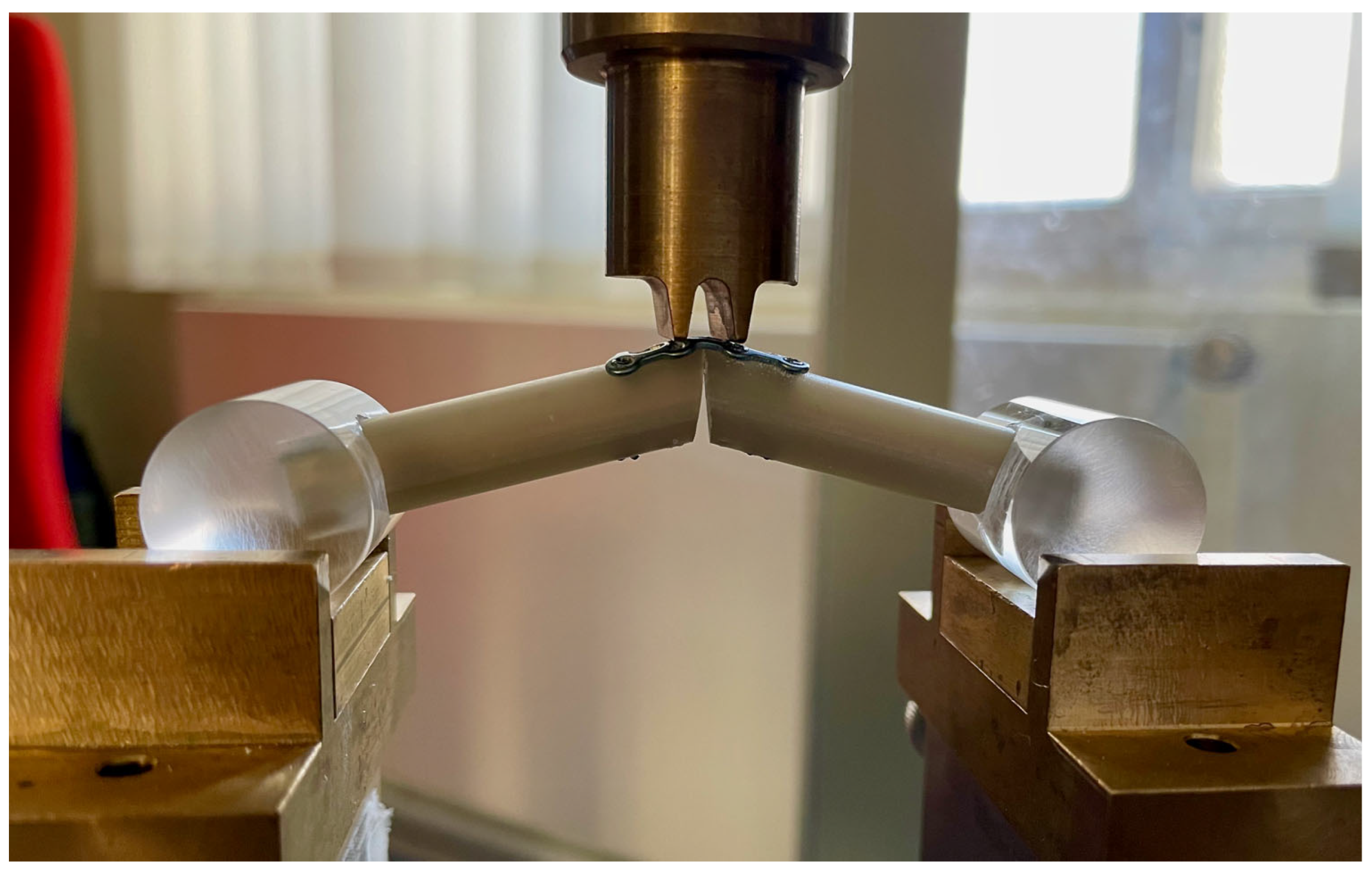
2. Materials and Methods
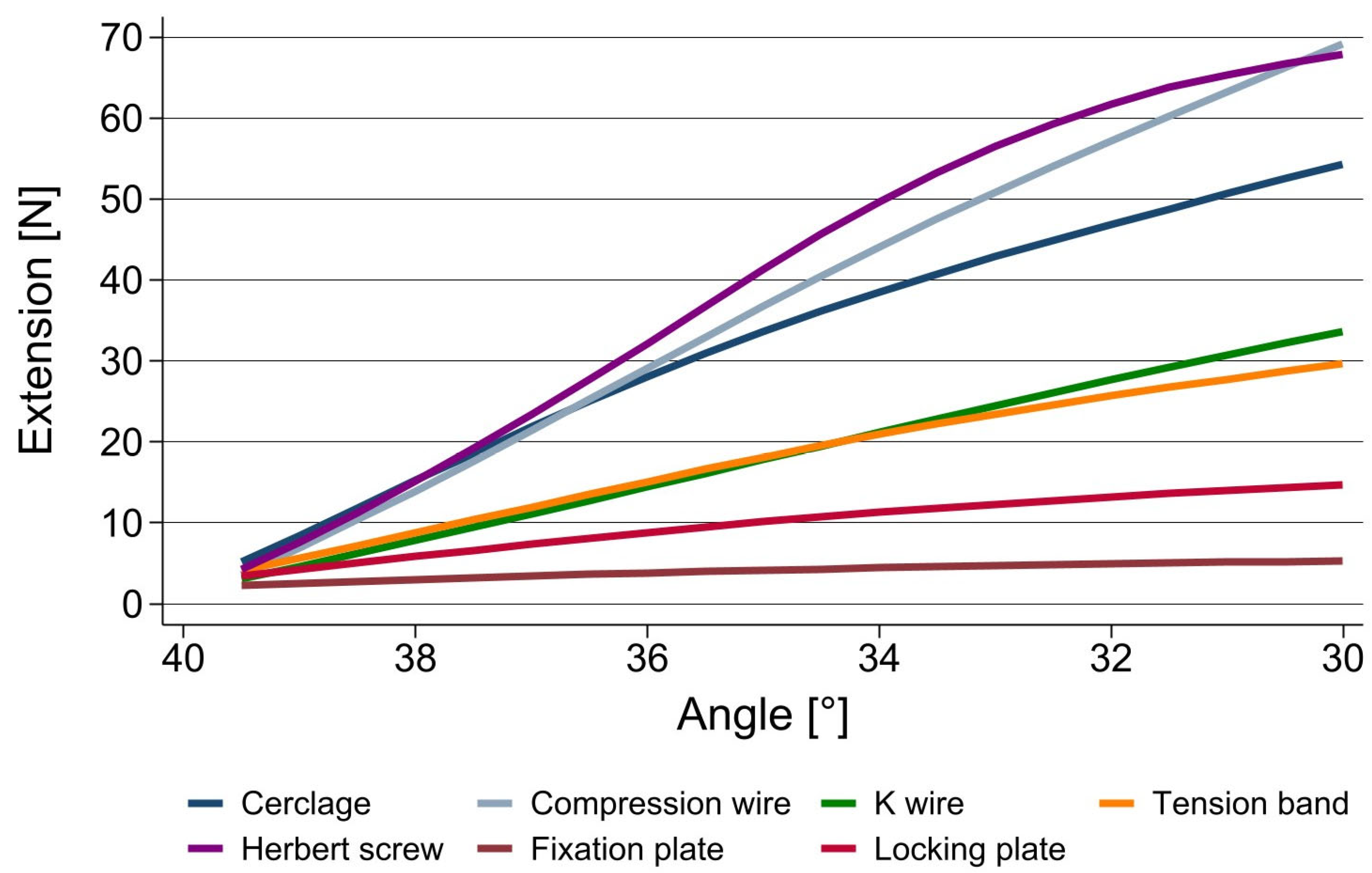
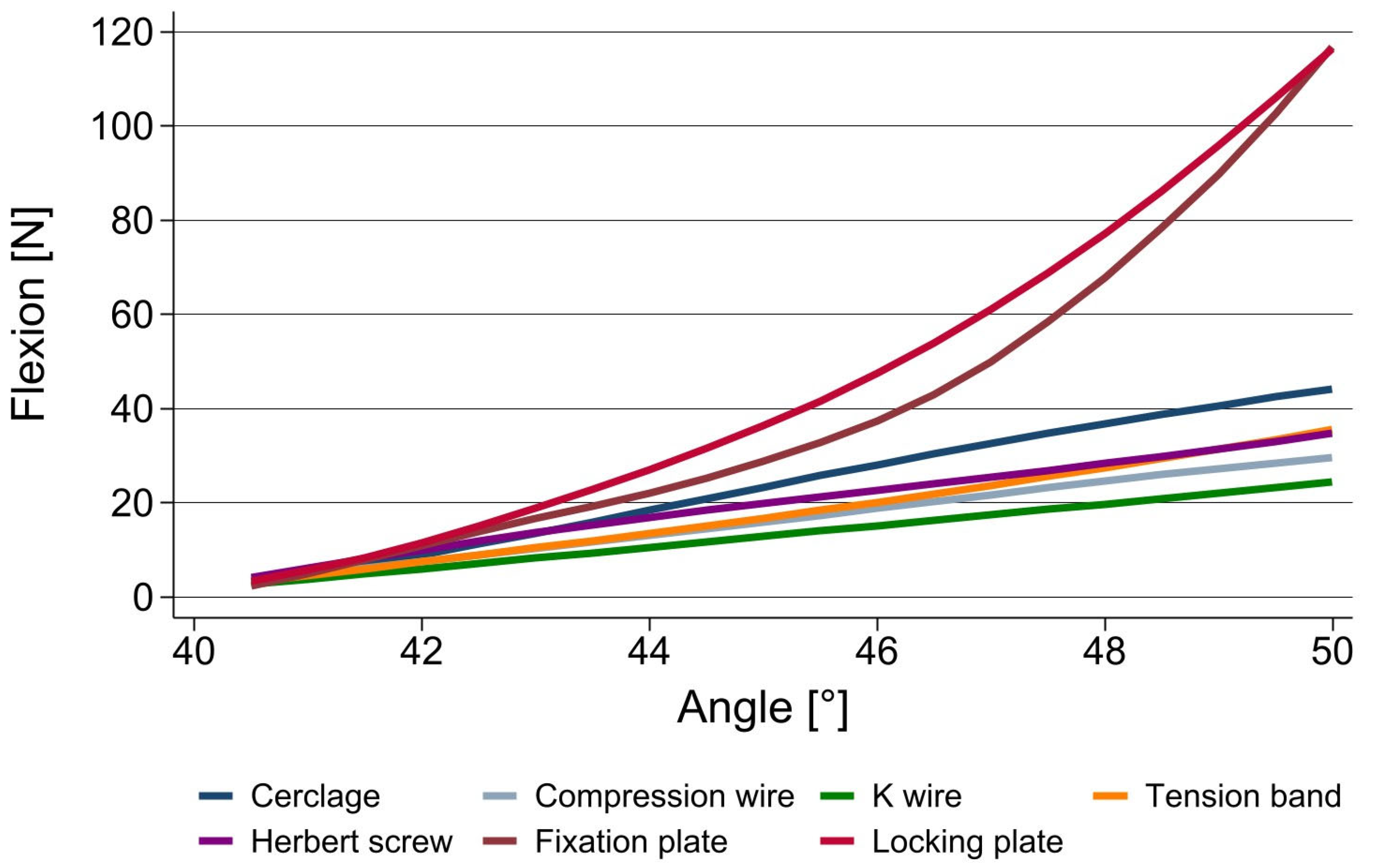
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herren, D. The proximal interphalangeal joint: Arthritis and deformity. EFORT Open Rev. 2019, 4, 254–262. [Google Scholar] [CrossRef]
- Pellegrini, V.D.; Burton, R.I. Osteoarthritis of the proximal interphalangeal joint of the hand: Arthroplasty or fusion? J. Hand. Surg. Am. 1990, 15, 194–209. [Google Scholar] [CrossRef]
- Jacobs, B.J.; Verbruggen, G.; Kaufmann, R.A. Proximal interphalangeal joint arthritis. J. Hand. Surg. Am. 2010, 35, 2107–2116. [Google Scholar] [CrossRef]
- Herren, D. Current European Practice in the Treatment of Proximal Interphalangeal Joint Arthritis. Hand. Clin. 2017, 33, 489–500. [Google Scholar] [CrossRef]
- Vitale, M.A.; Fruth, K.M.; Rizzo, M.; Moran, S.L.; Kakar, S. Prosthetic Arthroplasty Versus Arthrodesis for Osteoarthritis and Posttraumatic Arthritis of the Index Finger Proximal Interphalangeal Joint. J. Hand. Surg. Am. 2015, 40, 1937–1948. [Google Scholar] [CrossRef]
- Beldner, S.; Polatsch, D.B. Arthrodesis of the Metacarpophalangeal and Interphalangeal Joints of the Hand: Current Concepts. J. Am. Acad. Orthop. Surg. 2016, 24, 290–297. [Google Scholar] [CrossRef]
- Breyer, J.M.; Vergara, P.; Parra, L.; Sotelo, P.; Bifani, A.; Andrade, F. Metacarpophalangeal and interphalangeal joint arthrodesis: A comparative study between tension band and compression screw fixation. J. Hand. Surg. Eur. Vol. 2015, 40, 374–378. [Google Scholar] [CrossRef]
- Novoa-Parra, C.D.; Montaner-Alonso, D.; Pérez-Correa, J.I.; Morales-Rodríguez, J.; Rodrigo-Pérez, J.L.; Morales-Suarez-Varela, M. Arthrodesis of the proximal interphalangeal joint of the 4th and 5th finger using an interlocking screw device to treat severe recurrence of Dupuytren’s disease. Rev. Esp. Cir. Ortop. Traumatol. 2018, 62, 216–221. [Google Scholar] [CrossRef]
- Uhiara, O.; Hussain, S.; Deshmukh, S. Plate-augmented tension band wiring for arthrodesis of the proximal interphalangeal and metacarpophalangeal joints: A case series. J. Hand. Surg. Eur. Vol. 2021, 46, 679–681. [Google Scholar] [CrossRef]
- Tan, M.; Ho, S.W.L.; Sechachalam, S. Acute Arthrodesis of Interphalangeal Joints of the Hand in Traumatic Injuries. J. Hand. Microsurg. 2018, 10, 1–5. [Google Scholar] [CrossRef]
- Leibovic, S.J. Internal fixation for small joint arthrodeses in the hand. The interphalangeal joints. Hand. Clin. 1997, 13, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Millrose, M.; Gesslein, M.; Ittermann, T.; Kim, S.; Vonderlind, H.C.; Ruettermann, M. Arthrodesis of the proximal interphalangeal joint of the finger—A systematic review. EFORT Open Rev. 2022, 7, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.M. Management of stiff hand: An occupational therapy perspective. Hand. Surg. 2002, 7, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Neumeister, M.W.; Winters, J.N.; Maduakolum, E. Phalangeal and Metacarpal Fractures of the Hand: Preventing Stiffness. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3871. [Google Scholar] [CrossRef] [PubMed]
- Butz, K.D.; Merrell, G.; Nauman, E.A. A biomechanical analysis of finger joint forces and stresses developed during common daily activities. Comput. Methods Biomech. Biomed. Engin. 2012, 15, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Arauz, P.; DeChello, K.; Dagum, A.; Sisto, S.A.; Kao, I. Biomechanics and Pinch Force of the Index Finger Under Simulated Proximal Interphalangeal Arthrodesis. J. Hand. Surg. Am. 2017, 42, e1–e658. [Google Scholar] [CrossRef]
- Vonderlind, H.C.; Eisenschenk, A.; Juergensen, I.; Kim, S.; Millrose, M. Arthrodesis of the proximal interphalangeal joint—A review. Handchir. Mikrochir. Plast. Chir. 2019, 51, 6–18. [Google Scholar]
- Lister, G. Intraosseous wiring of the digital skeleton. J. Hand. Surg. Am. 1978, 3, 427–435. [Google Scholar] [CrossRef]
- Hohendorff, B.; Franke, J.; Spies, C.K.; Mueller, L.P.; Ries, C. Arthrodesis of the proximal interphalangeal joint of fingers with tension band wire. Oper. Orthop. Traumatol. 2017, 29, 385–394. [Google Scholar] [CrossRef]
- Kurzen, P.; Fusetti, C.; Bonaccio, M.; Nagy, L. Complications after plate fixation of phalangeal fractures. J. Trauma 2006, 60, 841–843. [Google Scholar] [CrossRef]
- Büchler, U.; Aiken, M.A. Arthrodesis of the proximal interphalangeal joint by solid bone grafting and plate fixation in extensive injuries to the dorsal aspect of the finger. J. Hand. Surg. Am. 1988, 13, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Lögters, T.T.; Lee, H.H.; Gehrmann, S.; Windolf, J.; Kaufmann, R.A. Proximal Phalanx Fracture Management. Hand 2018, 13, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Leibovic, S.J.; Strickland, J.W. Arthrodesis of the proximal interphalangeal joint of the finger: Comparison of the use of the Herbert screw with other fixation methods. J. Hand. Surg. Am. 1994, 19, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Martin, L. Arthrodeses of the thumb and long finger joints. Handchirurgie 1981, 13, 221–230. [Google Scholar]
- Murray, P.M. Treatment of the osteoarthritic hand and thumb. In Green’s Operative Hand Surgery, 7th ed.; Wolfe, S.W., Hotchkiss, R.N., Pederson, W.C., Kozin, S.H., Cohen, M.S., Eds.; Elsevier Inc.: Philadelphia, PA, USA, 2017; pp. 345–372. [Google Scholar]
- Xu, J.; Yong, F.C.; Lim, C.W.; Wong, K.J.H.; Teoh, L.C. The impact of various simulated arthrodesis angles of the proximal interphalangeal joint of the ring and middle finger on grip strength. Arch. Orthop. Trauma Surg. 2022, 142, 701–705. [Google Scholar] [CrossRef]
- Dimitrova, P.; Reger, A.; Prommersberger, K.J.; van Schoonhoven, J.; Mühldorfer-Fodor, M. Effect of a single proximal interphalangeal Joint Fusion of the Index, Middle or Ring Finger on the Grip and Finger Force and Load Distribution in the Hand. Handchir. Mikrochir. Plast. Chir. 2022, 54, 409–417. [Google Scholar]
- Millrose, M.; Zach, A.; Kim, S.; Güthoff, C.; Eisenschenk, A.; Vonderlind, H.C. Biomechanical comparison of the proximal interphalangeal joint arthrodesis using a compression wire. Arch. Orthop. Trauma Surg. 2019, 139, 577–581. [Google Scholar] [CrossRef]
- Vonderlind, H.C.; Zach, A.; Eichenauer, F.; Kim, S.; Eisenschenk, A.; Millrose, M. Proximal interphalangeal joint arthrodesis using a compression wire: A comparative biomechanical study. Hand. Surg. Rehabil. 2019, 38, 307–311. [Google Scholar] [CrossRef]
- Mittelmeier, W.; Lehner, S.; Gollwitzer, H.; Hauschild, M.; Werber, K.D.; Steinhauser, E. Comparing biomechanical investigations about different wiring techniques of finger joint arthrodesis. Arch. Orthop. Trauma Surg. 2005, 125, 145–152. [Google Scholar] [CrossRef]
- Elfar, J.; Menorca, R.M.; Reed, J.D.; Stanbury, S. Composite bone models in orthopaedic surgery research and education. J. Am. Acad. Orthop. Surg. 2014, 22, 111–120. [Google Scholar]
- Kovach, J.C.; Werner, F.W.; Palmer, A.K.; Greenkey, S.; Murphy, D.J. Biomechanical analysis of internal fixation techniques for proximal interphalangeal joint arthrodesis. J. Hand. Surg. Am. 1986, 11, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Mittelmeier, W.; Braun, C.; Hauschild, M.; Schäfer, R. Technique of finger arthrodesis by dorsal thread tension band fixation. Comparing biomechanical investigations. Unfallchirurg 1999, 102, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Jung, M.C. Ergonomic evaluation of biomechanical hand function. Saf. Health Work 2015, 6, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.E.; Jha, B.; Ross, M. Rehabilitation following surgery for flexor tendon injuries of the hand. Cochrane Database Syst. Rev. 2021, 1, CD012479. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| K Wire | Cerclage | Compression Wire | Tension Band | Compression Screw | Fixation Plate | Locking Plate | |
|---|---|---|---|---|---|---|---|
| n = 10 | n = 10 | n = 10 | n = 10 | n = 10 | n = 10 | n = 10 | |
| 39.5° | 3.16 ± 0.87 | 5.28 ± 3.56 | 3.43 ± 0.67 | 4.18 ± 1.31 | 4.60 ± 1.88 | 2.31 ± 0.09 | 3.32 ± 0.58 |
| 39° | 4.57 ± 1.52 | 8.46 ± 5.67 | 5.09 ± 1.70 | 5.74 ± 2.10 | 7.68 ± 3.58 | 2.58 ± 0.14 | 4.29 ± 0.76 |
| 38.5° | 6.17 ± 2.01 | 11.68 ± 6.95 | 8.05 ± 3.98 | 7.18 ± 2.76 | 11.03 ± 6.20 | 2.82 ± 0.16 | 5.06 ± 1.00 |
| 38° | 7.80 ± 2.64 | 15.03 ± 8.04 | 11.47 ± 6.56 | 8.52 ± 3.69 | 14.36 ± 8.80 | 3.03 ± 0.19 | 5.91 ± 1.05 |
| 37.5° | 9.37 ± 3.21 | 18.65 ± 8.82 | 14.73 ± 8.21 | 10.28 ± 3.97 | 17.48 ± 9.19 | 3.27 ± 0.21 | 6.72 ± 1.06 |
| 37° | 10.95 ± 3.72 | 22.21 ± 9.46 | 17.99 ± 9.75 | 11.95 ± 4.41 | 22.67 ± 13.84 | 3.47 ± 0.27 | 7.46 ± 1.04 |
| 36.5° | 12.52 ± 4.21 | 25.56 ± 10.16 | 21.65 ± 11.23 | 13.49 ± 4.89 | 27.36 ± 17.44 | 3.68 ± 0.25 | 8.24 ± 1.12 |
| 36° | 14.49 ± 4.75 | 28.80 ± 11.04 | 26.24 ± 12.48 | 15.18 ± 5.29 | 32.26 ± 20.00 | 3.87 ± 0.26 | 8.93 ± 1.16 |
| 35.5° | 16.21 ± 5.13 | 31.74 ± 11.70 | 31.10 ± 13.45 | 16.78 ± 5.58 | 37.12 ± 20.27 | 4.06 ± 0.28 | 9.57 ± 1.24 |
| 35° | 17.97 ± 5.46 | 34.63 ± 12.37 | 35.69 ± 14.42 | 18.41 ± 5.82 | 40.40 ± 17.00 | 4.21 ± 0.30 | 10.27 ± 1.19 |
| 34.5° | 19.60 ± 5.79 | 36.99 ± 12.54 | 39.89 ± 15.54 | 19.87 ± 5.98 | 45.71 ± 18.63 | 4.34 ± 0.29 | 10.97 ± 1.10 |
| 34° | 21.20 ± 6.13 | 39.38 ± 12.93 | 43.73 ± 16.72 | 21.18 ± 5.98 | 52.08 ± 17.90 | 4.47 ± 0.31 | 11.51 ± 1.06 |
| 33.5° | 22.74 ± 6.36 | 40.21 ± 13.37 | 47.17 ± 17.78 | 22.54 ± 6.11 | 55.29 ± 19.49 | 4.61 ± 0.32 | 11.97 ± 1.00 |
| 33° | 24.53 ± 6.29 | 42.93 ± 13.17 | 49.44 ± 18.26 | 23.76 ± 6.10 | 60.27 ± 20.60 | 4.72 ± 0.33 | 12.41 ± 0.92 |
| 32.5° | 26.26 ± 6.20 | 45.11 ± 13.23 | 53.06 ± 17.92 | 24.91 ± 6.18 | 61.47 ± 18.24 | 4.84 ± 0.34 | 12.87 ± 0.83 |
| 32° | 27.89 ± 5.87 | 47.10 ± 13.30 | 56.88 ± 16.71 | 25.92 ± 6.29 | 63.01 ± 16.00 | 4.97 ± 0.35 | 13.25 ± 0.79 |
| 31.5° | 29.35 ± 5.80 | 49.01 ± 13.39 | 60.43 ± 16.28 | 26.71 ± 6.29 | 64.25 ± 14.49 | 5.06 ± 0.36 | 13.68 ± 0.67 |
| 31° | 30.85 ± 5.77 | 50.78 ± 13.55 | 63.42 ± 16.28 | 27.80 ± 6.49 | 65.15 ± 13.45 | 5.15 ± 0.36 | 14.09 ± 0.58 |
| 30.5° | 32.18 ± 5.81 | 52.51 ± 13.58 | 66.19 ± 16.54 | 28.70 ± 6.50 | 66.35 ± 12.68 | 5.24 ± 0.35 | 14.43 ± 0.52 |
| 30° | 33.60 ± 5.43 | 54.11 ± 13.69 | 68.53 ± 16.85 | 29.62 ± 6.83 | 68.12 ± 11.07 | 5.33 ± 0.34 | 14.69 ± 0.50 |
| K Wire | Cerclage | Compression Wire | Tension Band | Compression Screw | Fixation Plate | Locking Plate | |
|---|---|---|---|---|---|---|---|
| n = 10 | n = 10 | n = 10 | n = 10 | n = 10 | n = 10 | n = 10 | |
| 40.5° | 2.80 ± 0.27 | 3.39 ± 1.41 | 3.37 ± 0.71 | 3.38 ± 0.82 | 4.06 ± 0.97 | 3.37 ± 1.35 | 3.81 ± 0.59 |
| 41° | 3.71 ± 0.21 | 4.53 ± 2.58 | 4.69 ± 1.71 | 4.37 ± 1.69 | 6.00 ± 1.82 | 4.45 ± 2.64 | 5.50 ± 1.06 |
| 41.5° | 4.81 ± 0.96 | 6.27 ± 4.01 | 6.07 ± 2.74 | 5.84 ± 2.23 | 7.97 ± 3.17 | 7.09 ± 7.78 | 7.85 ± 2.49 |
| 42° | 5.90 ± 1.57 | 8.43 ± 5.53 | 7.53 ± 3.69 | 7.35 ± 2.87 | 10.01 ± 4.25 | 10.15 ± 13.59 | 10.60 ± 4.75 |
| 42.5° | 6.94 ± 1.93 | 10.84 ± 7.13 | 9.00 ± 4.67 | 8.91 ± 3.58 | 11.94 ± 5.15 | 13.34 ± 19.38 | 12.71 ± 4.07 |
| 43° | 8.08 ± 2.36 | 13.28 ± 8.85 | 10.39 ± 5.52 | 10.46 ± 4.31 | 13.94 ± 6.01 | 16.73 ± 25.39 | 16.16 ± 5.69 |
| 43.5° | 9.29 ± 2.73 | 15.76 ± 10.48 | 11.66 ± 6.20 | 11.95 ± 4.97 | 15.88 ± 6.49 | 20.71 ± 31.61 | 21.46 ± 10.50 |
| 44° | 10.60 ± 3.15 | 18.22 ± 12.08 | 12.90 ± 6.80 | 13.28 ± 5.65 | 17.58 ± 6.65 | 24.48 ± 37.50 | 26.77 ± 14.80 |
| 44.5° | 11.83 ± 3.59 | 20.86 ± 13.36 | 14.19 ± 7.32 | 14.88 ± 6.35 | 19.06 ± 6.65 | 28.06 ± 43.89 | 31.88 ± 18.50 |
| 45° | 12.92 ± 3.91 | 23.54 ± 14.46 | 15.67 ± 7.85 | 16.67 ± 7.10 | 20.10 ± 6.19 | 22.19 ± 19.86 | 36.67 ± 21.96 |
| 45.5° | 13.94 ± 4.20 | 26.07 ± 15.49 | 17.14 ± 8.47 | 18.29 ± 7.86 | 21.18 ± 5.95 | 27.42 ± 29.08 | 41.10 ± 25.05 |
| 46° | 14.97 ± 4.44 | 28.48 ± 16.37 | 18.58 ± 8.99 | 19.97 ± 8.54 | 22.37 ± 5.99 | 33.00 ± 36.73 | 45.39 ± 28.24 |
| 46.5° | 16.29 ± 4.54 | 30.72 ± 17.18 | 20.17 ± 9.10 | 21.67 ± 9.37 | 23.62 ± 6.18 | 39.51 ± 44.44 | 48.50 ± 30.61 |
| 47° | 17.51 ± 4.79 | 32.88 ± 17.91 | 21.91 ± 9.64 | 23.37 ± 10.26 | 25.01 ± 6.45 | 47.12 ± 50.70 | 56.21 ± 34.41 |
| 47.5° | 18.55 ± 5.09 | 34.97 ± 18.66 | 23.46 ± 10.27 | 25.21 ± 11.33 | 26.58 ± 6.68 | 52.43 ± 56.39 | 65.25 ± 39.34 |
| 48° | 19.55 ± 5.27 | 36.96 ± 19.37 | 24.91 ± 10.92 | 27.12 ± 12.27 | 28.23 ± 6.93 | 61.08 ± 59.67 | 74.42 ± 44.06 |
| 48.5° | 20.75 ± 5.17 | 38.85 ± 20.00 | 26.14 ± 11.39 | 29.27 ± 12.95 | 29.82 ± 7.24 | 73.03 ± 59.49 | 84.60 ± 46.22 |
| 49° | 22.14 ± 5.21 | 40.76 ± 20.47 | 27.31 ± 11.72 | 31.45 ± 13.83 | 31.41 ± 7.56 | 88.06 ± 58.09 | 100.47 ± 49.59 |
| 49.5° | 23.36 ± 5.41 | 42.49 ± 20.96 | 28.40 ± 11.97 | 33.48 ± 14.72 | 33.03 ± 7.76 | 103.22 ± 56.54 | 100.71 ± 51.63 |
| 50° | 24.41 ± 5.61 | 44.00 ± 21.22 | 29.57 ± 12.17 | 35.41 ± 15.56 | 34.68 ± 7.97 | 118.37 ± 55.07 | 118.51 ± 56.84 |
| 37.5° | 35.0° | 32.5° | 30.0° | |
|---|---|---|---|---|
| Compression screw [N] | 17.5; p = 0.006 | 40.4; p = 0.002 | 61.5; p = 0.001 | 68.1; p < 0.001 |
| Compression wire [N] | 14.7; p = 0.142 | 35.7; p = 0.016 | 53.1; p = 0.004 | 68.5; p < 0.001 |
| Cerclage [N] | 18.6; p = 0.016 | 34.6; p = 0.009 | 45.1; p = 0.006 | 54.1; p = 0.003 |
| Tension band [N] | 10.3; p = 0.510 | 18.4; p = 0.844 | 24.9; p = 0.617 | 29.6; p = 0.145 |
| K wire [N] | 9.4 | 18.0 | 26.3 | 33.6 |
| Locking plate [N] | 6.7; p = 0.044 | 10.3; p = 0.003 | 12.9; p < 0.001 | 14.7; p < 0.001 |
| Fixation plate [N] | 3.3; p < 0.001 | 4.2; p < 0.001 | 4.8; p < 0.001 | 5.3; p < 0.001 |
| 42.5° | 45.0° | 47.5° | 50.0° | |
|---|---|---|---|---|
| Locking plate [N] | 12.7; p = 0.004 | 36.7; p = 0.011 | 65.2; p = 0.006 | 118.5; p < 0.001 |
| Fixation plate [N] | 13.3; p = 0.310 | 22.2; p = 0.147 | 52.4; p = 0.081 | 118.4; p < 0.001 |
| Cerclage [N] | 10.8; p = 0.153 | 23.5; p = 0.062 | 35.0; p = 0.030 | 44.0; p = 0.030 |
| Tension band [N] | 8.9; p = 0.217 | 16.7; p = 0.260 | 25.2; p = 0.213 | 35.4; p = 0.125 |
| Compression screw [N] | 11.9; p = 0.031 | 20.1; p = 0.012 | 26.6; p = 0.004 | 34.7; p < 0.001 |
| Compression wire [N] | 9.0; p = 0.263 | 15.7; p = 0.397 | 23.5; p = 0.232 | 29.6; p = 0.212 |
| K wire [N] | 6.9 | 12.9 | 18.5 | 24.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Millrose, M.; Vonderlind, H.C.; Thannheimer, A.; Ittermann, T.; Rüther, J.; Willauschus, M.; Bail, H.-J.; Eisenschenk, A. Arthrodesis of the Proximal Interphalangeal Joint of the Finger—A Biomechanical Study of Primary Stability. J. Pers. Med. 2023, 13, 465. https://doi.org/10.3390/jpm13030465
Millrose M, Vonderlind HC, Thannheimer A, Ittermann T, Rüther J, Willauschus M, Bail H-J, Eisenschenk A. Arthrodesis of the Proximal Interphalangeal Joint of the Finger—A Biomechanical Study of Primary Stability. Journal of Personalized Medicine. 2023; 13(3):465. https://doi.org/10.3390/jpm13030465
Chicago/Turabian StyleMillrose, Michael, Hans Christoph Vonderlind, Andreas Thannheimer, Till Ittermann, Johannes Rüther, Maximilian Willauschus, Hermann-Josef Bail, and Andreas Eisenschenk. 2023. "Arthrodesis of the Proximal Interphalangeal Joint of the Finger—A Biomechanical Study of Primary Stability" Journal of Personalized Medicine 13, no. 3: 465. https://doi.org/10.3390/jpm13030465