
Analgesic Efficacies of Intraoperative Pectoralis Nerve II Block under Direct Vision in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction: A Prospective, Randomized Controlled Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
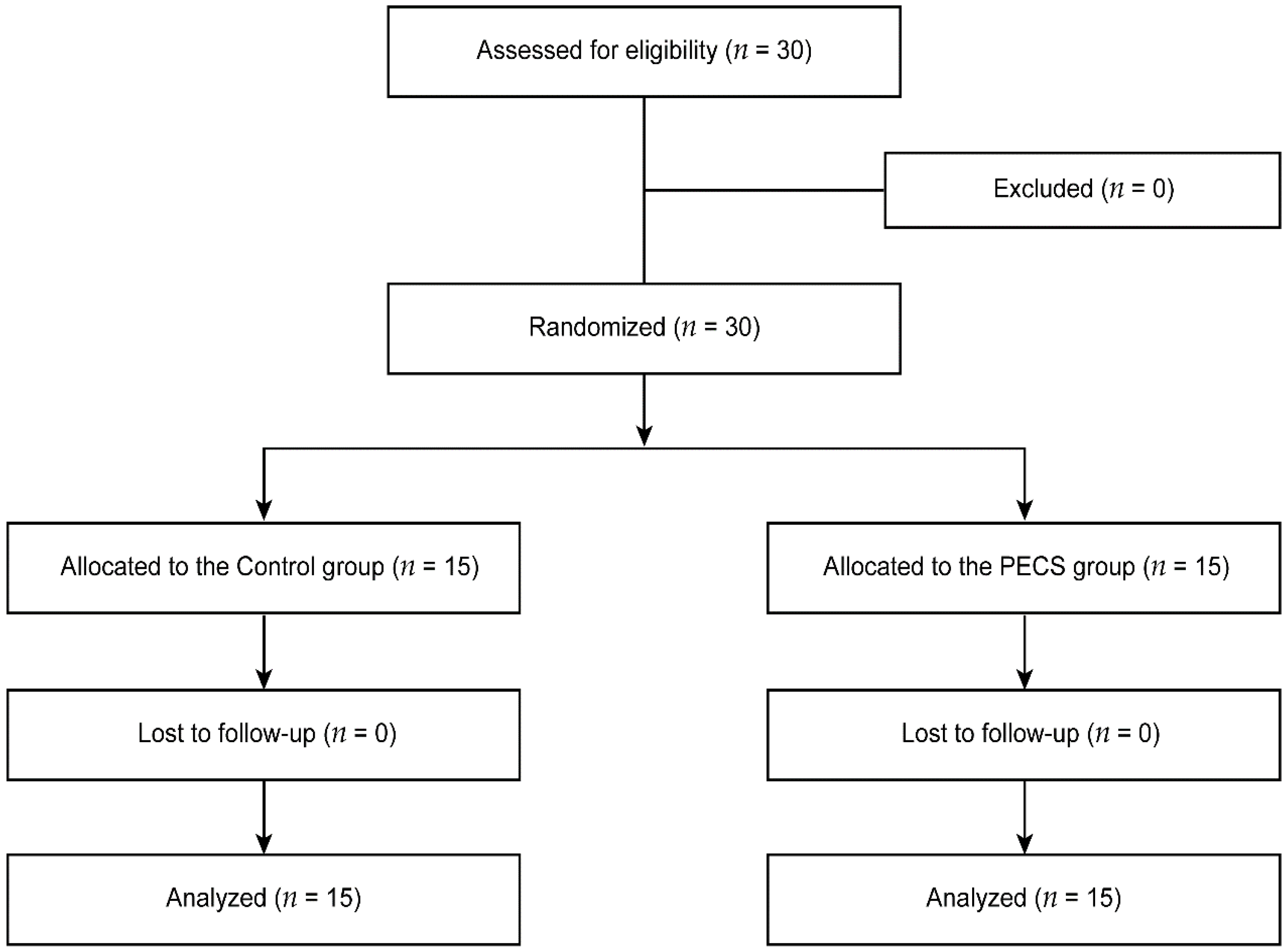
2.2. Randomization and Intervention
2.3. Procedures
2.3.1. Anesthesia
2.3.2. RNSM
2.3.3. IBR
2.4. Postoperative Pain Management
2.5. Outcomes
2.6. Data Collection
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blanco, R.; Fajardo, M.; Parras Maldonado, T. Ultrasound description of Pecs (modified Pecs I): A novel approach to breast surgery. Rev. Esp. Anestesiol. Reanim. 2012, 59, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Versyck, B.; van Geffen, G.J.; Chin, K.J. Analgesic efficacy of the pecs II block: A systematic review and meta-analysis. Anaesthesia 2019, 74, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Lovett-Carter, D.; Kendall, M.C.; McCormick, Z.L.; Suh, E.I.; Cohen, A.D.; De Oliveira, G.S. Pectoral nerve blocks and postoperative pain outcomes after mastectomy: A meta-analysis of randomized controlled trials. Reg. Anesth. Pain Med. 2019, 44, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Neethu, M.; Pandey, R.K.; Sharma, A.; Darlong, V.; Punj, J.; Sinha, R.; Singh, P.M.; Hamshi, N.; Garg, R.; Chandralekha, C.; et al. Pectoral nerve blocks to improve analgesia after breast cancer surgery: A prospective, randomized and controlled trial. J. Clin. Anesth. 2018, 45, 12–17. [Google Scholar]
- Blanco, R. The ‘pecs block’: A novel technique for providing analgesia after breast surgery. Anaesthesia 2011, 66, 847–848. [Google Scholar] [CrossRef] [PubMed]
- Woodworth, G.E.; Ivie, R.M.J.; Nelson, S.M.; Walker, C.M.; Maniker, R.B. Perioperative breast analgesia: A qualitative review of anatomy and regional techniques. Reg. Anesth. Pain Med. 2017, 42, 609–631. [Google Scholar] [CrossRef] [PubMed]
- Toesca, A.; Peradze, N.; Galimberti, V.; Manconi, A.; Intra, M.; Gentilini, O.; Sances, D.; Negri, D.; Veronesi, G.; Rietjens, M.; et al. Robotic nipple-sparing mastectomy and immediate breast reconstruction with implant: First report of surgical technique. Ann. Surg. 2017, 266, e28–e30. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Lee, J.; Lee, D.W.; Song, S.Y.; Lew, D.H.; Kim, S.I.; Cho, Y.U. Robot-assisted nipple-sparing mastectomy with immediate breast reconstruction: An initial experience. Sci. Rep. 2019, 9, 15669. [Google Scholar] [CrossRef]
- Thomas, M.; Philip, F.A.; Mathew, A.P.; Jagathnath Krishna, K.M. Intraoperative pectoral nerve block (pec) for breast cancer surgery: A randomized controlled trial. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 318–323. [Google Scholar] [PubMed]
- Hinchcliff, K.M.; Hylton, J.R.; Orbay, H.; Wong, M.S. Intraoperative placement of pectoral nerve block catheters: Description of a novel technique and review of the literature. Ann. Plast. Surg 2017, 78, S189–S193. [Google Scholar] [CrossRef]
- Haydon, N.B.; van der Rijt, R.; Downs, C.; Buckland, G. A novel technique of intraoperative lateral pectoral nerve block during subpectoral breast implant placement. Plast. Reconstr. Surg. Glob. Open 2016, 4, e646. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Lee, J.; Lee, H.; Lee, K.; Song, S.Y.; Toesca, A. Development of robotic mastectomy using a single-port surgical robot system. J. Breast Cancer 2020, 23, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, H.S.; Lee, H.; Lee, K.; Han, D.H.; Lee, D.W. Axillary lymph node dissection using a robotic surgical system: Initial experience. J. Surg. Oncol. 2020, 122, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, B.; Struk, S.; Leymarie, N.; Honart, J.F.; Alkhashnam, H.; de Fremicourt, K.T.; Conversano, A.; Rimareix, F.; Simon, M.; Michiels, S.; et al. Robotic prophylactic nipple-sparing mastectomy with immediate prosthetic breast reconstruction: A prospective study. Ann. Surg. Oncol. 2018, 25, 2579–2586. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, J.H.; Lee, D.W.; Song, S.Y.; Park, S.; Kim, S.I.; Ryu, D.H.; Cho, Y.U. Gasless robot-assisted nipple-sparing mastectomy: A case report. J. Breast Cancer 2018, 21, 334–338. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Kaur, U.; Shamshery, C.; Agarwal, A.; Prakash, N.; Valiveru, R.C.; Mishra, P. Evaluation of postoperative pain in patients undergoing modified radical mastectomy with pectoralis or serratus-intercostal fascial plane blocks. Korean J. Anesthesiol. 2020, 73, 425–433. [Google Scholar] [CrossRef]
- Diab, D.G.; Elmaddawy, A.A.; Elganainy, A. Intra-articular morphine versus dexmedetomedine for knee arthroscopy under local anesthesia. Anesth. Essays Res. 2019, 13, 7–12. [Google Scholar]
- Caljouw, M.A.; van Beuzekom, M.; Boer, F. Patient’s satisfaction with perioperative care: Development, validation, and application of a questionnaire. Br. J. Anaesth. 2008, 100, 637–644. [Google Scholar] [CrossRef]
- Kumar, S.; Goel, D.; Sharma, S.K.; Ahmad, S.; Dwivedi, P.; Deo, N.; Rani, R. A randomised controlled study of the post-operative analgesic efficacy of ultrasound-guided pectoral nerve block in the first 24 h after modified radical mastectomy. Indian J. Anaesth. 2018, 62, 436–442. [Google Scholar]
- Kim, D.H.; Kim, S.; Kim, C.S.; Lee, S.; Lee, I.G.; Kim, H.J.; Lee, J.H.; Jeong, S.M.; Choi, K.T. Efficacy of pectoral nerve block type ii for breast-conserving surgery and sentinel lymph node biopsy: A prospective randomized controlled study. Pain Res. Manag. 2018, 2018, 4315931. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhang, X.; Zhang, T.; Yue, H.; Sun, S.; Zhao, H.; Zhou, P. The efficacy of ultrasound-guided type II pectoral nerve blocks in perioperative pain management for immediate reconstruction after modified radical mastectomy: A prospective, randomized study. Clin. J. Pain 2018, 34, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Versyck, B.; van Geffen, G.J.; Van Houwe, P. Prospective double blind randomized placebo-controlled clinical trial of the pectoral nerves (pecs) block type II. J. Clin. Anesth. 2017, 40, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Bashandy, G.M.; Abbas, D.N. Pectoral nerves i and ii blocks in multimodal analgesia for breast cancer surgery: A randomized clinical trial. Reg. Anesth. Pain Med. 2015, 40, 68–74. [Google Scholar] [CrossRef]
- Bakshi, S.G.; Karan, N.; Parmar, V. Pectoralis block for breast surgery: A surgical concern? Indian J. Anaesth. 2017, 61, 851–852. [Google Scholar] [CrossRef]
- Apfel, C.C.; Laara, E.; Koivuranta, M.; Greim, C.A.; Roewer, N. A simplified risk score for predicting postoperative nausea and vomiting: Conclusions from cross-validations between two centers. Anesthesiology 1999, 91, 693–700. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 15) | PECS Group (n = 15) | p Value | |
|---|---|---|---|
| Age, years | 43 ± 7 | 44 ± 7 | 0.734 |
| BMI, kg/m2 | 22.3 ± 2.9 | 20.7 ± 3.3 | 0.164 |
| ASA physical status | 0.143 | ||
| I | 5 (33%) | 9 (60%) | |
| II | 10 (67%) | 6 (40%) | |
| Smoking history | >0.999 | ||
| Nonsmoker | 14 (93%) | 15 (100%) | |
| Exsmoker | 1 (7%) | 0 (0%) | |
| Menopause status | >0.999 | ||
| Premenopausal | 14 (93%) | 13 (87%) | |
| Postmenopausal | 1 (7%) | 2 (13%) | |
| Motion sickness | 0 (0%) | 5(33%) | 0.042 * |
| PONV history | 0 (0%) | 2 (13%) | 0.483 |
| Neoadjuvant chemotherapy | 4 (27%) | 1 (7%) | 0.330 |
| Control Group (n = 15) | PECS Group (n = 15) | p Value | |
|---|---|---|---|
| Anesthesia time, min | 297 ± 47 | 295 ± 37 | 0.865 |
| Operation time, min | 252 ± 41 | 260 ± 41 | 0.573 |
| Mastectomy time, min | 146 ± 31 | 149 ± 33 | 0.765 |
| Reconstruction time, min | 103 ± 18 | 100 ± 31 | 0.756 |
| Blood loss | >0.999 | ||
| ≤100 mL | 13 (87%) | 14 (93%) | |
| >100 mL | 2 (13%) | 1 (7%) | |
| Total fluid intake, mL | 1943 ± 479 | 2155 ± 291 | 0.154 |
| Urine output, mL | 631 ± 597 | 646 ± 384 | 0.935 |
| Intraoperative administered remifentanil, mg | 0.8 ± 0.1 | 0.9 ± 0.3 | 0.417 |
| Intraoperative administered phenylephrine, mg | 4.1 ± 2.6 | 4.7 ± 1.3 | 0.475 |
| Location | 0.464 | ||
| Right | 9 (60%) | 7 (47%) | |
| Left | 6 (40%) | 8 (53%) | |
| Type of reconstruction | 0.682 | ||
| Direct-to-implant | 12 (80%) | 10 (67%) | |
| Tissue expander insertion | 3 (20%) | 5 (33%) | |
| Lymph node procedure | >0.999 | ||
| Sentinel lymph node biopsy | 12 (80%) | 11 (73%) | |
| Axillary lymph node dissection | 3 (20%) | 4 (27%) | |
| Specimen weight, g | 349 ± 113 | 324 ± 141 | 0.612 |
| Control Group (n = 15) | PECS Group (n = 15) | p Value | |
|---|---|---|---|
| Postoperative hospital stays, days | 7.5 ± 1.8 | 6.7 ± 1.7 | 0.223 |
| Patient satisfaction score | 2.8 ± 0.4 | 3.5 ± 0.6 | 0.002 * |
| Nausea, n | 0.486 | ||
| None | 11 (73%) | 10 (26%) | |
| Mild | 1 (7%) | 3 (20%) | |
| Moderate | 1 (7%) | 2 (13%) | |
| Severe | 2 (13%) | 0 (0%) | |
| Vomiting, n | 3 (20%) | 3 (20%) | >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, J.; Park, H.S.; Kim, J.Y.; Lee, H.S.; Jeon, S.; Lee, D.; Bai, S.J.; Kim, N.Y. Analgesic Efficacies of Intraoperative Pectoralis Nerve II Block under Direct Vision in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction: A Prospective, Randomized Controlled Study. J. Pers. Med. 2022, 12, 1309. https://doi.org/10.3390/jpm12081309
Moon J, Park HS, Kim JY, Lee HS, Jeon S, Lee D, Bai SJ, Kim NY. Analgesic Efficacies of Intraoperative Pectoralis Nerve II Block under Direct Vision in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction: A Prospective, Randomized Controlled Study. Journal of Personalized Medicine. 2022; 12(8):1309. https://doi.org/10.3390/jpm12081309
Chicago/Turabian StyleMoon, Jiae, Hyung Seok Park, Jee Ye Kim, Hye Sun Lee, Soyoung Jeon, Dongwoo Lee, Sun Joon Bai, and Na Young Kim. 2022. "Analgesic Efficacies of Intraoperative Pectoralis Nerve II Block under Direct Vision in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction: A Prospective, Randomized Controlled Study" Journal of Personalized Medicine 12, no. 8: 1309. https://doi.org/10.3390/jpm12081309