
Analgesia Effect of Verum and Sham Acupuncture Treatments in Primary Dysmenorrhea: A MRI Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Acupuncture Treatment
2.4. MRI Acquisition
2.5. MRI Data Processing
2.6. Statistical Analysis
3. Results
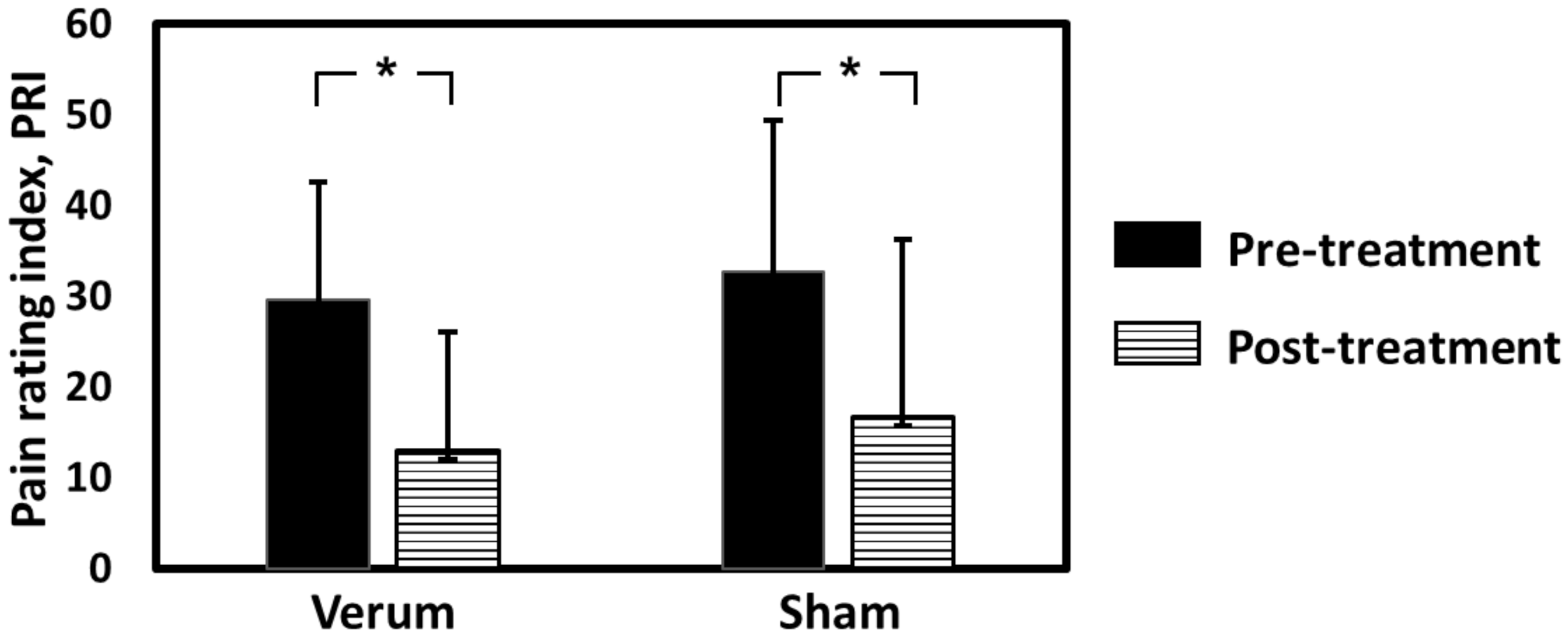
3.1. Demographic and Clinical Information
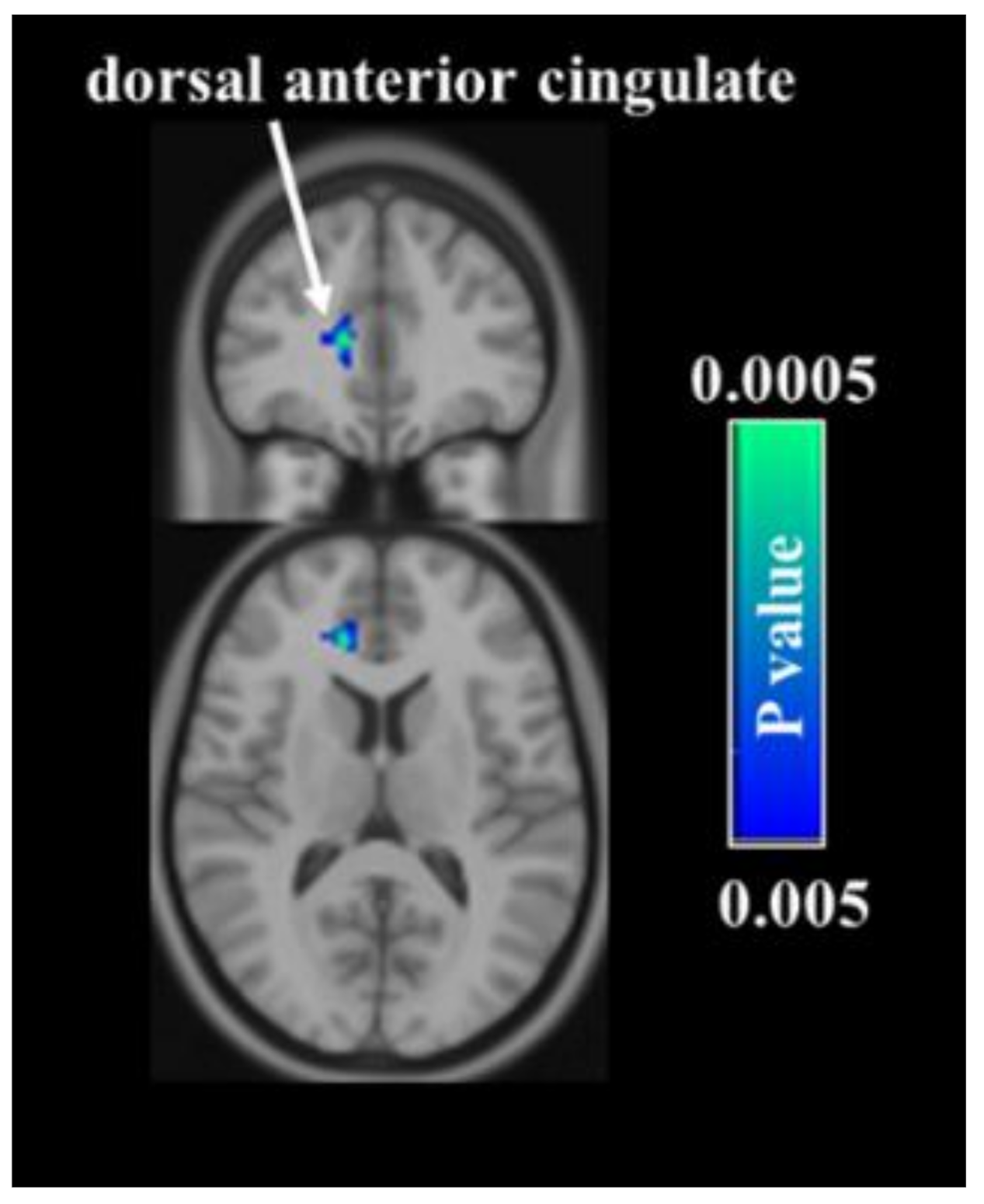
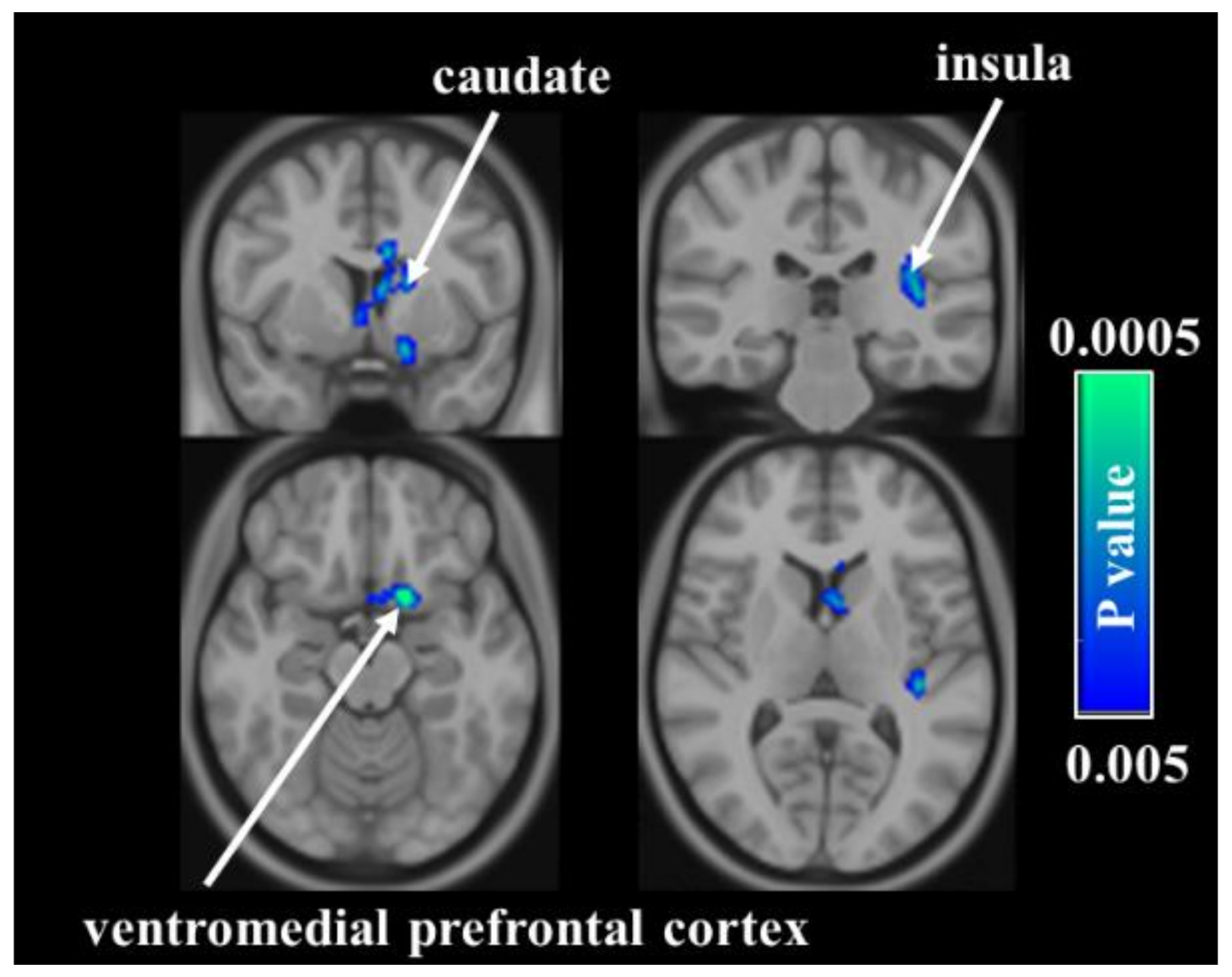
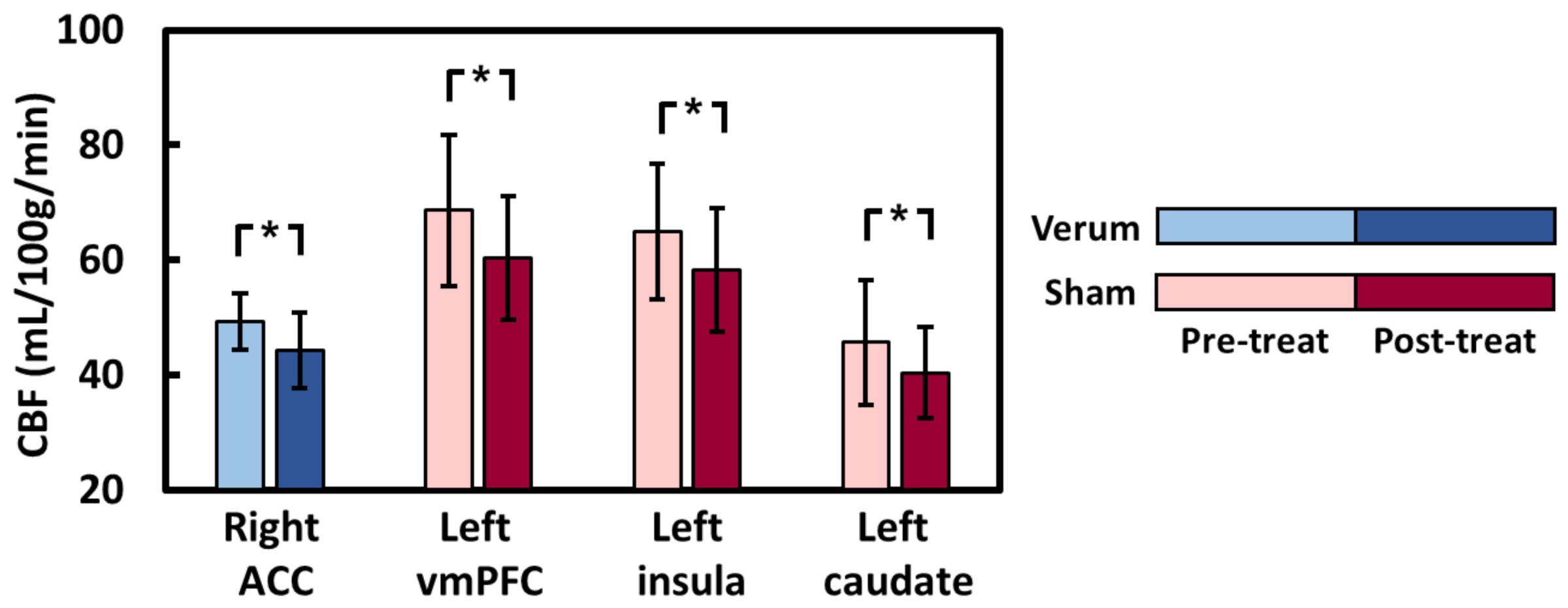
3.2. CBF Voxelwise Analyses
3.3. Regression Analysis between Changes in Total PRI and Baseline CBF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tu, C.-H.; Lin, C.-L.; Yang, S.-T.; Shen, W.-C.; Chen, Y.-H. Hormonal Contraceptive Treatment May Reduce the Risk of Fibromyalgia in Women with Dysmenorrhea: A Cohort Study. J. Pers. Med. 2020, 10, 280. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Lazzeri, L.; Perelli, F.; Reis, F.M.; Petraglia, F. Dysmenorrhea and related disorders. F1000Research 2017, 6, 1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petraglia, F.; Parke, S.; Serrani, M.; Mellinger, U.; Römer, T. Estradiol valerate plus dienogest versus ethinylestradiol plus levonorgestrel for the treatment of primary dysmenorrhea. Int. J. Gynecol. Obstet. 2014, 125, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Marjoribanks, J.; Proctor, M.; Farquhar, C.; Derks, R.S. Nonsteroidal anti-inflammatory drugs for primary dysmenorrhoea. Cochrane Database Syst. Rev. 2010, 7, CD001751. [Google Scholar]
- Steinberger, A. The Treatment of Dysmenorrhea by Acupuncture. Am. J. Chin. Med. 1981, 9, 57–60. [Google Scholar] [CrossRef]
- Campbell, M.A.; McGrath, P.J. Non-pharmacologic Strategies Used by Adolescents for the Management of Menstrual Discomfort. Clin. J. Pain 1999, 15, 313–320. [Google Scholar] [CrossRef]
- Chao, M.T.; Wade, C.M.; Abercrombie, P.D.; Gomolak, D. An innovative acupuncture treatment for primary dysmenorrhea: A randomized, crossover pilot study. Altern. Ther. Health Med. 2014, 20, 49–56. [Google Scholar]
- Woo, H.L.; Ji, H.R.; Pak, Y.K.; Lee, H.; Heo, S.J.; Lee, J.M.; Park, K.S. The efficacy and safety of acupuncture in women with primary dysmenorrhea: A systematic review and meta-analysis. Medicine 2018, 97, e11007. [Google Scholar] [CrossRef]
- Yu, S.; Xie, M.; Liu, S.; Guo, X.; Tian, J.; Wei, W.; Zhang, Q.; Zeng, F.; Liang, F.; Yang, J. Resting-State Functional Connectivity Patterns Predict Acupuncture Treatment Response in Primary Dysmenorrhea. Front. Neurosci. 2020, 14, 559191. [Google Scholar] [CrossRef]
- Egorova, N.; Gollub, R.L.; Kong, J. Repeated verum but not placebo acupuncture normalizes connectivity in brain regions dysregulated in chronic pain. NeuroImage Clin. 2015, 9, 430–435. [Google Scholar] [CrossRef] [Green Version]
- Tu, Y.; Ortiz, A.; Gollub, R.L.; Cao, J.; Gerber, J.; Lang, C.; Park, J.; Wilson, G.; Shen, W.; Chan, S.-T.; et al. Multivariate resting-state functional connectivity predicts responses to real and sham acupuncture treatment in chronic low back pain. NeuroImage Clin. 2019, 23, 101885. [Google Scholar] [CrossRef]
- Liu, J.; Mu, J.; Liu, Q.; Dun, W.; Zhang, M.; Tian, J. Brain structural properties predict psychologically mediated hypoalgesia in an 8-week sham acupuncture treatment for migraine. Hum. Brain Mapp. 2017, 38, 4386–4397. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-N.; Huang, Y.-R.; Liu, J.-L.; Zhang, F.-Q.; Zhang, B.-Y.; Wu, J.-C.; Ma, Y.; Xia, J.; Hao, Y.; Huo, J.-W. Aberrant resting-state cerebral blood flow and its connectivity in primary dysmenorrhea on arterial spin labeling MRI. Magn. Reson. Imaging 2020, 73, 84–90. [Google Scholar] [CrossRef]
- Zhang, Y.-N.; Huo, J.-W.; Huang, Y.-R.; Hao, Y.; Chen, Z.-Y. Altered amplitude of low-frequency fluctuation and regional cerebral blood flow in females with primary dysmenorrhea: A resting-state fMRI and arterial spin labeling study. J. Pain Res. 2019, 12, 1243–1250. [Google Scholar] [CrossRef] [Green Version]
- Hashmi, J.A.; Kong, J.; Spaeth, R.; Khan, S.; Kaptchuk, T.J.; Gollub, R.L. Functional network architecture predicts psychologically mediated analgesia related to treatment in chronic knee pain patients. J. Neurosci. 2014, 34, 3924–3936. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Kaptchuk, T.J.; Polich, G.; Kirsch, I.; Vangel, M.; Zyloney, C.; Rosen, B.; Gollub, R.L. Expectancy and treatment interactions: A dissociation between acupuncture analgesia and expectancy evoked placebo analgesia. NeuroImage 2009, 45, 940–949. [Google Scholar] [CrossRef] [Green Version]
- Harris, R.E.; Zubieta, J.K.; Scott, D.J.; Napadow, V.; Gracely, R.H.; Clauw, D.J. Traditional Chinese acupuncture and placebo (sham) acupuncture are differentiated by their effects on mu-opioid receptors (MORs). NeuroImage 2009, 47, 1077–1085. [Google Scholar] [CrossRef] [Green Version]
- Hui, Y.L.; Chen, A.C. Analysis of headache in a Chinese patient population. Ma Zui Xue Za Zhi Anaesthesiol. Sin. 1989, 27, 13–18. [Google Scholar]
- Shi, G.-X.; Liu, C.Z.; Zhu, J.; Guan, L.-P.; Wang, D.-J.; Wu, M.-M. Effects of Acupuncture at Sanyinjiao (SP6) on Prostaglandin Levels in Primary Dysmenorrhea Patients. Clin. J. Pain 2011, 27, 258–261. [Google Scholar] [CrossRef]
- Streitberger, K.; Kleinhenz, J. Introducing a placebo needle into acupuncture research. Lancet 1998, 352, 364–365. [Google Scholar] [CrossRef]
- Peng, S.; Chen, C. The influence of obesity on cerebral blood flow in young adults using arterial spin labeling MRI. NMR Biomed. 2020, 33, 4375. [Google Scholar] [CrossRef] [PubMed]
- Hui, K.K.S.; Nixon, E.E.; Vangel, M.G.; Liu, J.; Marina, O.; Napadow, V.; Hodge, S.M.; Rosen, B.R.; Makris, N.; Kennedy, D.N. Characterization of the "deqi" response in acupuncture. BMC Complement. Altern. Med. 2007, 7, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dougherty, D.D.; Kong, J.; Webb, M.; Bonab, A.A.; Fischman, A.J.; Gollub, R.L. A combined [11C]diprenorphine PET study and fMRI study of acupuncture analgesia. Behav. Brain Res. 2008, 193, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sora, I.; Takahashi, N.; Funada, M.; Ujike, H.; Revay, R.S.; Donovan, D.M.; Miner, L.L.; Uhl, G.R. Opiate receptor knockout mice define mu receptor roles in endogenous nociceptive responses and morphine-induced analgesia. Proc. Natl. Acad. Sci. USA 1997, 94, 1544–1549. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.H.; Greve, D.N.; Dai, G.; Marota, J.J.; Mandeville, J.B. Remifentanil administration reveals biphasic phMRI temporal responses in rat consistent with dynamic receptor regulation. NeuroImage 2007, 34, 1042–1053. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R.; Coderre, T.J.; Katz, J.; Vaccarino, A. Central Neuroplasticity and Pathological Pain. Ann. N. Y. Acad. Sci. 2006, 933, 157–174. [Google Scholar] [CrossRef]
- Russo, J.F.; Sheth, S.A. Deep brain stimulation of the dorsal anterior cingulate cortex for the treatment of chronic neuropathic pain. Neurosurg. Focus 2015, 38, E11. [Google Scholar] [CrossRef]
- Bissonette, G.B.; Powell, E.; Roesch, M.R. Neural structures underlying set-shifting: Roles of medial prefrontal cortex and anterior cingulate cortex. Behav. Brain Res. 2013, 250, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Devinsky, O.; Morrell, M.J.; Vogt, B.A. Contributions of anterior cingulate cortex to behaviour. Brain 1995, 118, 279–306. [Google Scholar] [CrossRef]
- Jahn, A.; Nee, D.E.; Alexander, W.H.; Brown, J.W. Distinct regions of anterior cingulate cortex signal prediction and outcome evaluation. NeuroImage 2014, 95, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Rolls, E.T. The cingulate cortex and limbic systems for emotion, action, and memory. Brain Struct. Funct. 2019, 224, 3001–3018. [Google Scholar] [CrossRef] [Green Version]
- Kleinhenz, J.; Streitberger, K.; Windeler, J.; Gübacher, A.; Mavridis, G.; Martin, E. Randomised clinical trial comparing the effects of acupuncture and a newly designed placebo needle in rotator cuff tendinitis. Pain 1999, 83, 235–241. [Google Scholar] [CrossRef]
- Moffet, H.H. Sham Acupuncture May Be as Efficacious as True Acupuncture: A Systematic Review of Clinical Trials. J. Altern. Complement. Med. 2009, 15, 213–216. [Google Scholar] [CrossRef]
- Assefi, N.P.; Sherman, K.J.; Jacobsen, C.; Goldberg, J.; Smith, W.R.; Buchwald, D. A Randomized Clinical Trial of Acupuncture Compared with Sham Acupuncture in Fibromyalgia. Ann. Intern. Med. 2005, 143, 10–19. [Google Scholar] [CrossRef]
- Lund, I.; Lundeberg, T. Are Minimal, Superficial Or Sham Acupuncture Procedures Acceptable as Inert Placebo Controls? Acupunct. Med. 2006, 24, 13–15. [Google Scholar] [CrossRef]
- Wise, R.A. Dopamine, learning and motivation. Nat. Rev. Neurosci. 2004, 5, 483–494. [Google Scholar] [CrossRef]
- Scott, D.J.; Stohler, C.S.; Egnatuk, C.M.; Wang, H.; Koeppe, R.A.; Zubieta, J.-K. Placebo and Nocebo Effects Are Defined by Opposite Opioid and Dopaminergic Responses. Arch. Gen. Psychiatry 2008, 65, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.-K.; Chen, Y.I.; Hamel, E.; Jenkins, B.G. Brain hemodynamic changes mediated by dopamine receptors: Role of the cerebral microvasculature in dopamine-mediated neurovascular coupling. NeuroImage 2006, 30, 700–712. [Google Scholar] [CrossRef]
- Starr, C.J.; Sawaki, L.; Wittenberg, G.; Burdette, J.H.; Oshiro, Y.; Quevedo, A.S.; Coghill, R.C. Roles of the Insular Cortex in the Modulation of Pain: Insights from Brain Lesions. J. Neurosci. 2009, 29, 2684–2694. [Google Scholar] [CrossRef]
- Colloca, L.; Klinger, R.; Flor, H.; Bingel, U. Placebo analgesia: Psychological and neurobiological mechanisms. Pain 2013, 154, 511–514. [Google Scholar] [CrossRef] [Green Version]
- Zunhammer, M.; Spisák, T.; Wager, T.D.; Bingel, U.; The Placebo Imaging Consortium. Meta-analysis of neural systems underlying placebo analgesia from individual participant fMRI data. Nat. Commun. 2021, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Roy, C.S.; Sherrington, C.S. On the Regulation of the Blood-supply of the Brain. J. Physiol. 1890, 11, 85–158. [Google Scholar] [CrossRef] [PubMed]
- Wager, T.D.; Atlas, L.Y. The neuroscience of placebo effects: Connecting context, learning and health. Nat. Rev. Neurosci. 2015, 16, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Porro, C.A.; Baraldi, P.; Pagnoni, G.; Serafini, M.; Facchin, P.; Maieron, M.; Nichelli, P. Does Anticipation of Pain Affect Cortical Nociceptive Systems? J. Neurosci. 2002, 22, 3206–3214. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.-C.; Stone-Elander, S.; Ingvar, M. Anticipatory coping of pain expressed in the human anterior cingulate cortex: A positron emission tomography study. Neurosci. Lett. 1999, 262, 61–64. [Google Scholar] [CrossRef]
- Atlas, L.Y.; Wager, T.D. A Meta-analysis of Brain Mechanisms of Placebo Analgesia: Consistent Findings and Unanswered Questions. Mediat. Drugs Gastrointest. Motil. I 2014, 225, 37–69. [Google Scholar] [CrossRef]
- Liu, P.; Liu, Y.; Wang, G.; Yang, X.; Jin, L.; Sun, J.; Qin, W. Aberrant default mode network in patients with primary dysmenorrhea: A fMRI study. Brain Imaging Behav. 2016, 11, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Tu, C.-H.; Niddam, D.M.; Chao, H.-T.; Liu, R.-S.; Hwang, R.-J.; Yeh, T.-C.; Hsieh, J.-C. Abnormal cerebral metabolism during menstrual pain in primary dysmenorrhea. NeuroImage 2009, 47, 28–35. [Google Scholar] [CrossRef]
- Huang, Y.; Tang, C.; Wang, S.; Lu, Y.; Shen, W.; Yang, J.; Chen, J.; Lin, R.; Cui, S.; Xiao, H.; et al. Acupuncture regulates the glucose metabolism in cerebral functional regions in chronic stage ischemic stroke patients—a PET-CT cerebral functional imaging study. BMC Neurosci. 2012, 13, 75. [Google Scholar] [CrossRef] [Green Version]
- Zahradnik, H.P.; Breckwoldt, M. Contribution to the pathogenesis of dysmenorrhea. Arch. Gynecol. Obstet. 1984, 236, 99–108. [Google Scholar] [CrossRef]
- Liu, C.-Z.; Xie, J.-P.; Wang, L.-P.; Zheng, Y.-Y.; Ma, Z.-B.; Yang, H.; Chen, X.; Shi, G.-X.; Li, S.-L.; Zhao, J.-P.; et al. Immediate Analgesia Effect of Single Point Acupuncture in Primary Dysmenorrhea: A Randomized Controlled Trial. Pain Med. 2011, 12, 300–307. [Google Scholar] [CrossRef] [Green Version]
- White, P.; Lewith, G.; Hopwood, V.; Prescott, P. The placebo needle, is it a valid and convincing placebo for use in acupuncture trials? A randomised, single-blind, cross-over pilot trial. Pain 2003, 106, 401–409. [Google Scholar] [CrossRef]
- Low, I.; Wei, S.-Y.; Lee, P.-S.; Li, W.-C.; Lee, L.-C.; Hsieh, J.-C.; Chen, L.-F. Neuroimaging Studies of Primary Dysmenorrhea. Adv. Exp. Med. Biol. 2018, 1099, 179–199. [Google Scholar] [CrossRef]
- Jin, L.; Yang, X.; Liu, P.; Sun, J.; Chen, F.; Xu, Z.; Qin, W.; Tian, J. Dynamic abnormalities of spontaneous brain activity in women with primary dysmenorrhea. J. Pain Res. 2017, 10, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Farmer, M.; Baliki, M.N.; Apkarian, A.V. A dynamic network perspective of chronic pain. Neurosci. Lett. 2012, 520, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Apkarian, V.A.; Hashmi, J.A.; Baliki, M.N. Pain and the brain: Specificity and plasticity of the brain in clinical chronic pain. Pain 2011, 152, S49–S64. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Verum (N = 11) | Sham (N = 12) | p-Value | |
|---|---|---|---|
| Age (year) | 22.55 ± 2.34 | 25.75 ± 4.52 | 0.09 |
| Gynecologic age (year) | 11.36 ± 2.42 | 13.25 ± 5.26 | 0.32 |
| Body mass index ((kg/m2) | 21.94 ± 4.68 | 20.46 ± 1.65 | 0.60 |
| Length of menstrual cycle (day) | 30.36 ± 2.25 | 29.67 ± 2.27 | 0.42 |
| Dysmenorrhea history (year) | 6.73 ± 3.55 | 9.92 ± 5.28 | 0.09 |
| Verum | Sham | |||||
|---|---|---|---|---|---|---|
| Pre | Post | p Value | Pre | Post | p-Value | |
| Estradiol (pg/mL) | 139.82 ± 110.08 | 141.27 ± 82.92 | 0.83 | 138.17 ± 88.89 | 132.75 ± 109.10 | 0.91 |
| Progesterone (ng/L) | 1.59 ± 3.24 | 4.09 ± 6.85 | 0.41 | 1.08 ± 1.30 | 2.38 ± 4.51 | 0.56 |
| Testosterone (ng/mL) | 0.61 ± 0.22 | 0.60 ± 0.22 | 0.95 | 0.57 ± 0.11 | 0.50 ± 0.14 | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, S.-L.; Yang, H.-C.; Lee, Y.-C.; Chen, C.-M.; Chen, Y.-Y.; Tu, C.-H. Analgesia Effect of Verum and Sham Acupuncture Treatments in Primary Dysmenorrhea: A MRI Pilot Study. J. Pers. Med. 2021, 11, 1244. https://doi.org/10.3390/jpm11121244
Peng S-L, Yang H-C, Lee Y-C, Chen C-M, Chen Y-Y, Tu C-H. Analgesia Effect of Verum and Sham Acupuncture Treatments in Primary Dysmenorrhea: A MRI Pilot Study. Journal of Personalized Medicine. 2021; 11(12):1244. https://doi.org/10.3390/jpm11121244
Chicago/Turabian StylePeng, Shin-Lei, Hui-Chieh Yang, Yu-Chen Lee, Chun-Ming Chen, Ying-Yu Chen, and Cheng-Hao Tu. 2021. "Analgesia Effect of Verum and Sham Acupuncture Treatments in Primary Dysmenorrhea: A MRI Pilot Study" Journal of Personalized Medicine 11, no. 12: 1244. https://doi.org/10.3390/jpm11121244