
Changes in the Prevalence of Metabolic Syndrome, Its Components, and Relevant Preventive Medication between 2011 and 2018 in the Northeast Hungarian Roma Population

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations of Roma for Comparison from 2011 and 2018
2.2. Determination of the Prevalence of Metabolic Syndrome and Its Components
- 1.
- raised blood pressure (BP; systolic BP of ≥130 mmHg and/or diastolic BP of ≥85 mmHg) or treatment of previously diagnosed hypertension;
- 2.
- raised FG levels (≥5.6 mmol/L) or previously diagnosed type 2 diabetes mellitus;
- 3.
- raised triglyceride levels (≥1.7 mmol/L) or specific treatment for this lipid abnormality;
- 4.
- reduced HDL-C levels (<1.03 mmol/L in males and <1.29 mmol/L in females) or specific treatment for this lipid abnormality.
2.3. Statistical Analyses
2.4. Ethical Statement
3. Results
3.1. Anthropometric and Demographic Characteristics of the Study Populations
3.2. Parameters Used to Estimate the Prevalence of Metabolic Syndrome and Its Components in the Study Populations
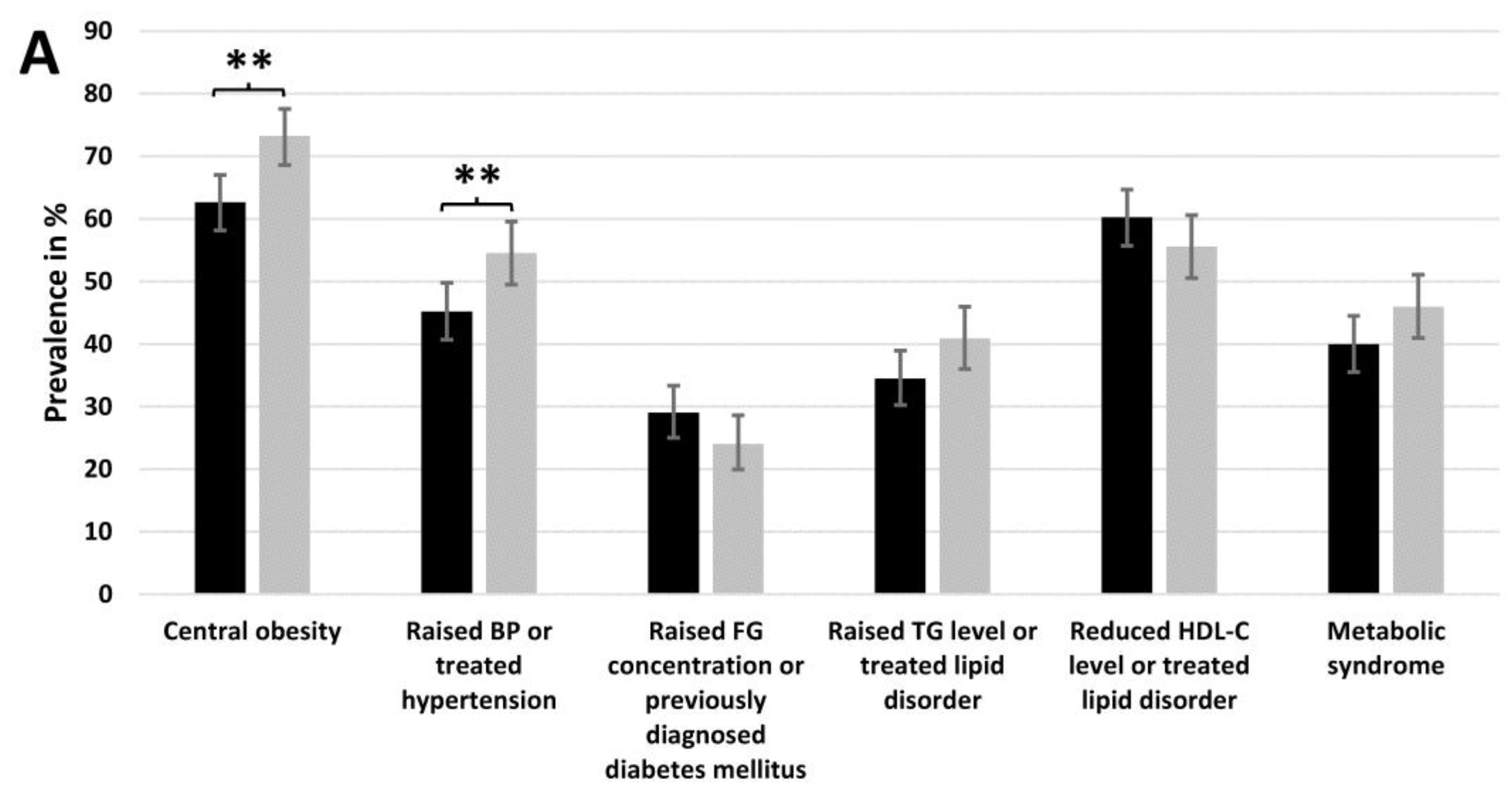
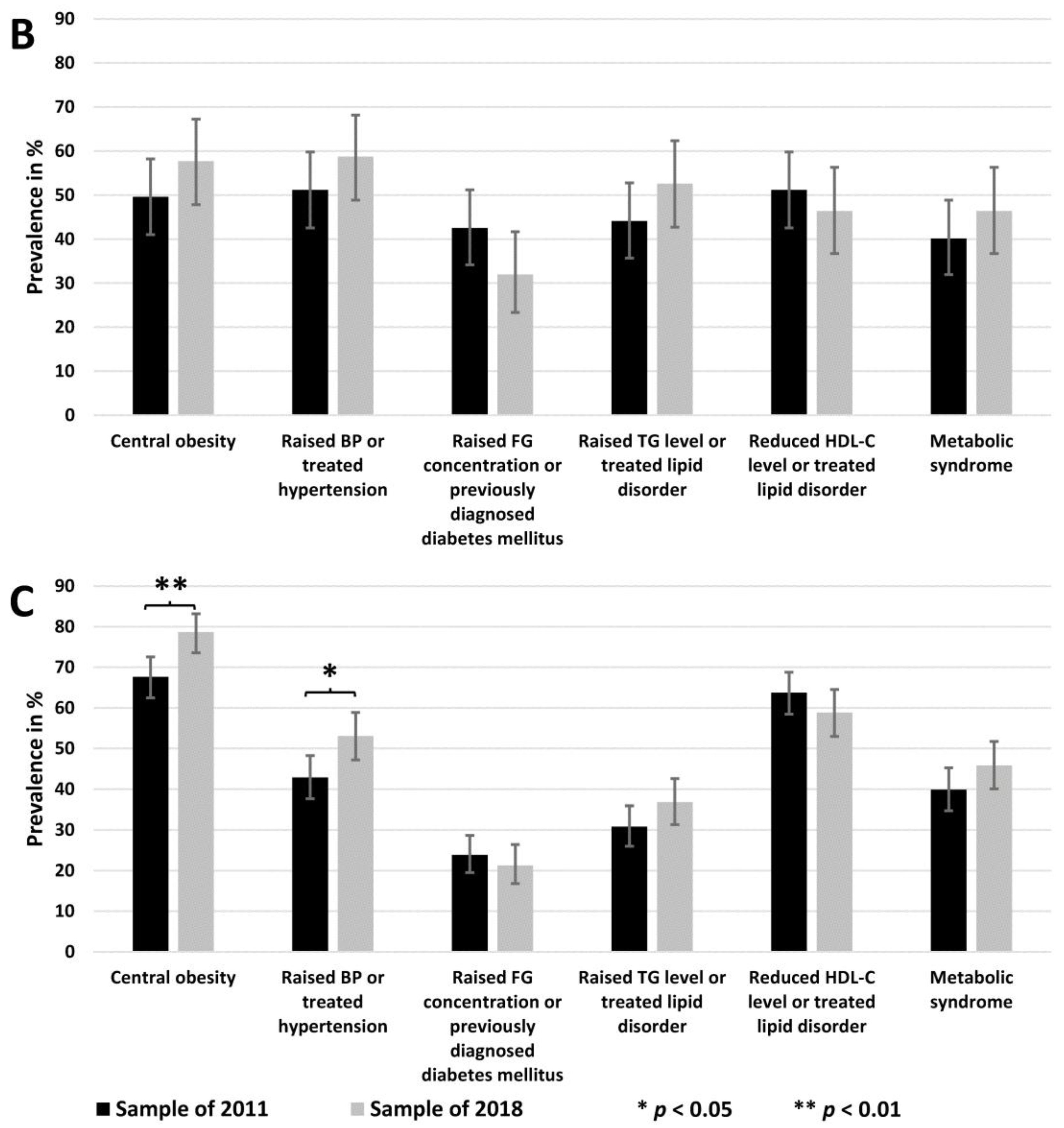
3.3. The Prevalence of MetS and Its Components in the Study Populations
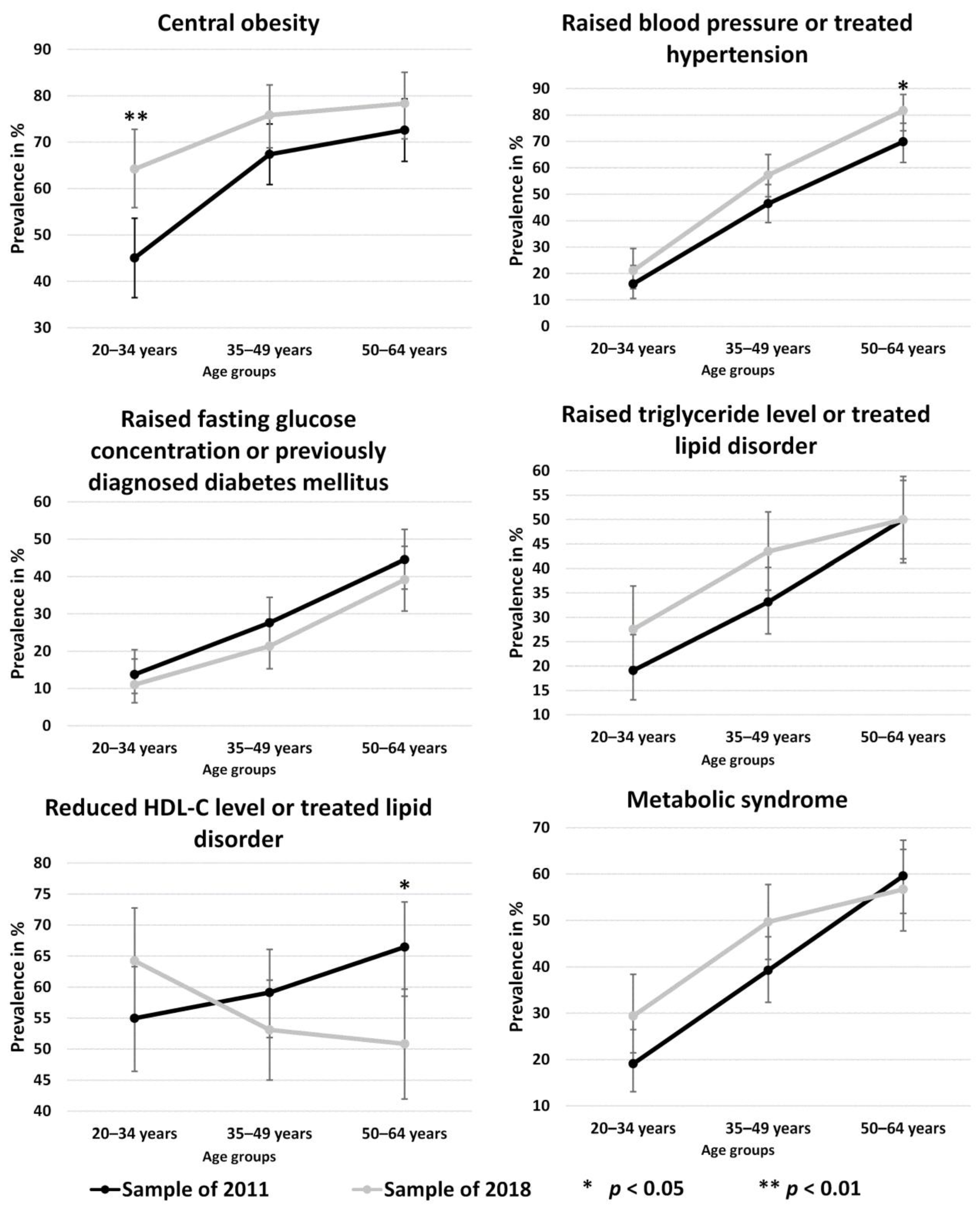
3.4. Age-Specific Prevalence of Metabolic Syndrome and Its Components in the Study Populations
3.5. The Change in Risk for the Development of MetS and Its Components between 2011 and 2018
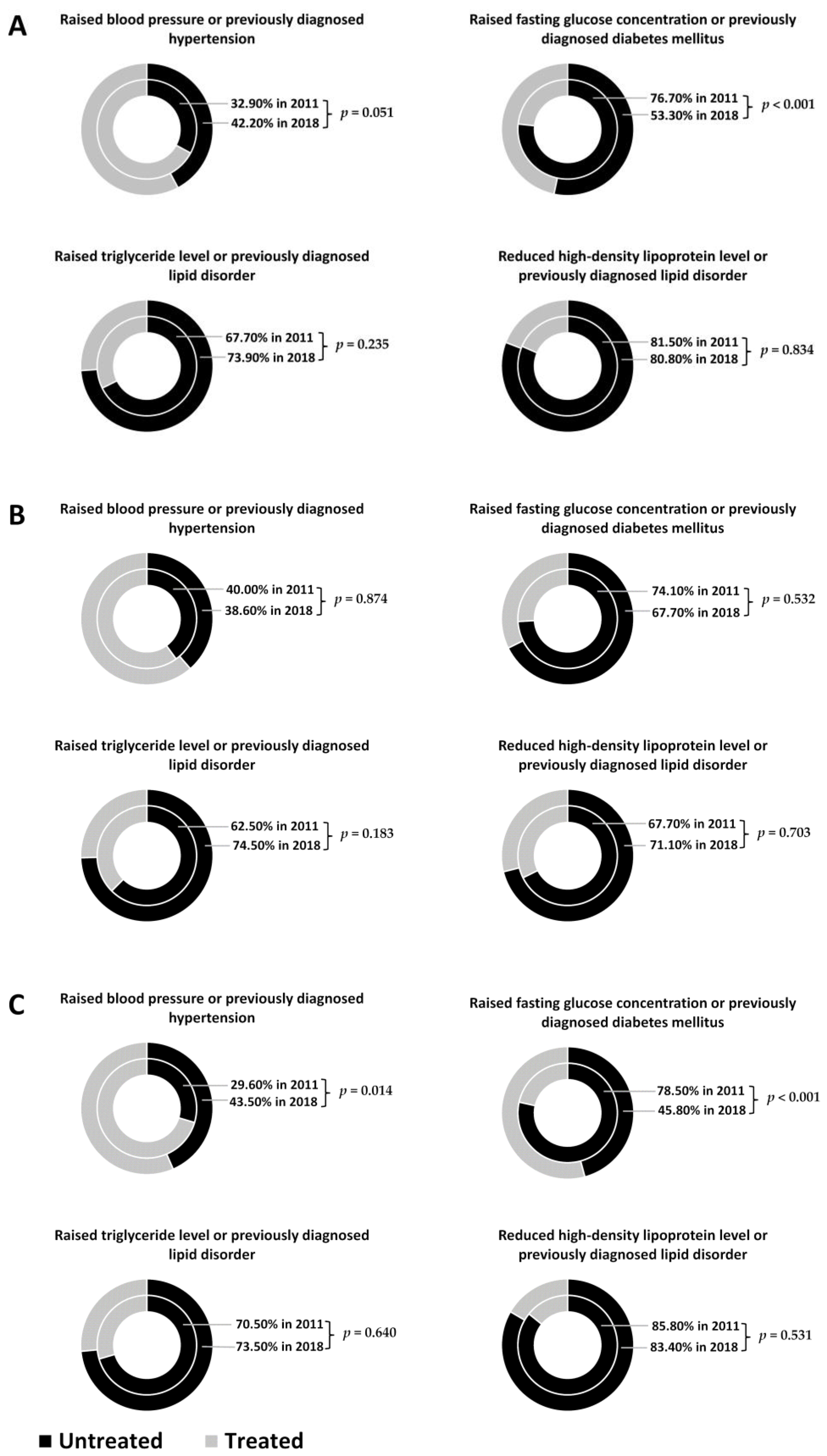
3.6. The Change in the Proportion of Those with Untreated Metabolic Syndrome Components in Sample Populations from 2011 and 2018
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Commission. Roma: Commission Calls on Member States to Step Up Efforts on Integration; European Commission: Brussels, Belgium, 2013. [Google Scholar]
- Hungarian Central Statistical Office. Population Census of Hungary in 2011; Hungarian Central Statistical Office: Budapest, Hungary, 2011.
- Pénzes, J.; Tátrai, P.; Pásztor, I.Z. A roma népesség területi megoszlásának változása Magyarországon az elmúlt évtizedekben (Changes in the Spatial Distribution of the Roma Population in Hungary During the Last Decades). Területi Stat. 2018, 58, 3–26. [Google Scholar] [CrossRef]
- European Union Agency for Fundamental Rights. Poverty and Employment: The Situation of Roma in 11 EU Member States; Publications Office of the European Union: Luxembourg, 2016. [Google Scholar]
- Sedlakova, D. Low socioeconomic status and unhealthy lifestyle lead to high morbidity in young Roma of East Slovakia. Cent. Eur. J. Public Health 2014, 22, S3–S5. [Google Scholar] [CrossRef] [Green Version]
- Dioszegi, J.; Piko, P.; Kosa, Z.; Sandor, J.; Llanaj, E.; Adany, R. Taste and Food Preferences of the Hungarian Roma Population. Front. Public Health 2020, 8, 359. [Google Scholar] [CrossRef]
- Llanaj, E.; Vincze, F.; Kosa, Z.; Sandor, J.; Dioszegi, J.; Adany, R. Dietary Profile and Nutritional Status of the Roma Population Living in Segregated Colonies in Northeast Hungary. Nutrients 2020, 12, 2836. [Google Scholar] [CrossRef] [PubMed]
- Cook, B.; Wayne, G.F.; Valentine, A.; Lessios, A.; Yeh, E. Revisiting the evidence on health and health care disparities among the Roma: A systematic review 2003–2012. Int. J. Public Health 2013, 58, 885–911. [Google Scholar] [CrossRef] [PubMed]
- Foldes, M.E.; Covaci, A. Research on Roma health and access to healthcare: State of the art and future challenges. Int. J. Public Health 2012, 57, 37–39. [Google Scholar] [CrossRef] [Green Version]
- Dixon, K.C.; Ferris, R.; Kuhn, I.; Spathis, A.; Barclay, S. Gypsy, Traveller and Roma experiences, views and needs in palliative and end of life care: A systematic literature review and narrative synthesis. BMJ Support. Palliat. Care 2021. [Google Scholar] [CrossRef] [PubMed]
- Voko, Z.; Csepe, P.; Nemeth, R.; Kosa, K.; Kosa, Z.; Szeles, G.; Adany, R. Does socioeconomic status fully mediate the effect of ethnicity on the health of Roma people in Hungary? J. Epidemiol. Community Health 2009, 63, 455–460. [Google Scholar] [CrossRef] [Green Version]
- Weiss, E.; Japie, C.; Balahura, A.M.; Bartos, D.; Badila, E. Cardiovascular risk factors in a Roma sample population from Romania. Rom. J. Intern. Med. 2018, 56, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Dobranici, M.; Buzea, A.; Popescu, R. The cardiovascular risk factors of the Roma (gypsies) people in Central-Eastern Europe: A review of the published literature. J. Med. Life 2012, 5, 382–389. [Google Scholar]
- Piko, P.; Kosa, Z.; Sandor, J.; Adany, R. Comparative risk assessment for the development of cardiovascular diseases in the Hungarian general and Roma population. Sci. Rep. 2021, 11, 3085. [Google Scholar] [CrossRef] [PubMed]
- Powell Doherty, R.; Telionis, P.A.; Muller-Demary, D.; Hosszu, A.; Duminica, A.; Bertke, A.; Lewis, B.; Eubank, S. A survey of quality of life indicators in the Romanian Roma population following the ‘Decade of Roma Inclusion’. F1000Research 2017, 6, 1692. [Google Scholar] [CrossRef]
- Sandor, J.; Kosa, Z.; Boruzs, K.; Boros, J.; Tokaji, I.; McKee, M.; Adany, R. The decade of Roma Inclusion: Did it make a difference to health and use of health care services? Int. J. Public Health 2017, 62, 803–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosa, K.; Adany, R. Studying vulnerable populations: Lessons from the Roma minority. Epidemiology 2007, 18, 290–299. [Google Scholar] [CrossRef]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.; Zimmet, P.; Shaw, J.; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Kosa, Z.; Moravcsik-Kornyicki, A.; Dioszegi, J.; Roberts, B.; Szabo, Z.; Sandor, J.; Adany, R. Prevalence of metabolic syndrome among Roma: A comparative health examination survey in Hungary. Eur. J. Public Health 2015, 25, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Kosa, K.; Darago, L.; Adany, R. Environmental survey of segregated habitats of Roma in Hungary: A way to be empowering and reliable in minority research. Eur. J. Public Health 2011, 21, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Adany, R.; Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Biro, E.; Kosa, K.; Paragh, G.; Bacsne Baba, E.; Veres-Balajti, I.; et al. Prevalence of Insulin Resistance in the Hungarian General and Roma Populations as Defined by Using Data Generated in a Complex Health (Interview and Examination) Survey. Int. J. Environ. Res. Public Health 2020, 17, 4833. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Zarkesh, M.; Daneshpour, M.S.; Faam, B.; Fallah, M.S.; Hosseinzadeh, N.; Guity, K.; Hosseinpanah, F.; Momenan, A.A.; Azizi, F. Heritability of the metabolic syndrome and its components in the Tehran Lipid and Glucose Study (TLGS). Genet. Res. 2012, 94, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Genetic factors exist behind the high prevalence of reduced high-density lipoprotein cholesterol levels in the Roma population. Atherosclerosis 2017, 263, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Generalizability and applicability of results obtained from populations of European descent regarding the effect direction and size of HDL-C level-associated genetic variants to the Hungarian general and Roma populations. Gene 2019, 686, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Piko, P.; Fiatal, S.; Werissa, N.A.; Bekele, B.B.; Racz, G.; Kosa, Z.; Sandor, J.; Adany, R. The Effect of Haplotypes in the CETP and LIPC Genes on the Triglycerides to HDL-C Ratio and Its Components in the Roma and Hungarian General Populations. Genes 2020, 11, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Data to genetic risk assessment on high-density cholesterol level associated polymorphisms in Hungarian general and Roma populations. Data Brief 2017, 14, 354–359. [Google Scholar] [CrossRef]
- Arai, Y.; Hirose, N. Aging and HDL metabolism in elderly people more than 100 years old. J. Atheroscler. Thromb. 2004, 11, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Shi, L.; Zou, Y.; Tang, J.; Cai, J.; Wei, Y.; Qin, J.; Zhang, Z. Positive association of familial longevity with the moderate-high HDL-C concentration in Bama Aging Study. Aging 2018, 10, 3528–3540. [Google Scholar] [CrossRef] [PubMed]
- Laks, R.; Araujo, L.M.; Almada Filho, C.M.; Cendoroglo, M.S. The importance of HDL-C and CRP in cardiovascular risk evaluation in longevous elderly individuals. Einstein 2011, 9, 397–403. [Google Scholar] [CrossRef]
- van Leeuwen, E.M.; Huffman, J.E.; Bis, J.C.; Isaacs, A.; Mulder, M.; Sabo, A.; Smith, A.V.; Demissie, S.; Manichaikul, A.; Brody, J.A.; et al. Fine mapping the CETP region reveals a common intronic insertion associated to HDL-C. NPJ Aging Mech. Dis. 2015, 1, 15011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, G.A.; Huffman, M.D.; Moran, A.E.; Feigin, V.; Mensah, G.A.; Naghavi, M.; Murray, C.J. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation 2015, 132, 1667–1678. [Google Scholar] [CrossRef] [Green Version]
- Bansal, R.; Gubbi, S.; Muniyappa, R. Metabolic Syndrome and COVID 19: Endocrine-Immune-Vascular Interactions Shapes Clinical Course. Endocrinology 2020, 161. [Google Scholar] [CrossRef]
- Katz, M.H. Regardless of Age, Obesity and Hypertension Increase Risks With COVID-19. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef]
- Aghili, S.M.M.; Ebrahimpur, M.; Arjmand, B.; Shadman, Z.; Sani, M.P.; Qorbani, M.; Larijani, B.; Payab, M. Obesity in COVID-19 era, implications for mechanisms, comorbidities, and prognosis: A review and meta-analysis. Int. J. Obes. 2021, 45, 998–1016. [Google Scholar] [CrossRef]
- Clark, C.E.; McDonagh, S.T.J.; McManus, R.J.; Martin, U. COVID-19 and hypertension: Risks and management. A scientific statement on behalf of the British and Irish Hypertension Society. J. Hum. Hypertens. 2021, 35, 304–307. [Google Scholar] [CrossRef]
- Armitage, C.J.; Keyworth, C.; Leather, J.Z.; Byrne-Davis, L.; Epton, T. Identifying targets for interventions to support public adherence to government instructions to reduce transmission of SARS-CoV-2. BMC Public Health 2021, 21, 522. [Google Scholar] [CrossRef] [PubMed]
- Ekezie, W.; Czyznikowska, B.M.; Rohit, S.; Harrison, J.; Miah, N.; Campbell-Morris, P.; Khunti, K. The views of ethnic minority and vulnerable communities towards participation in COVID-19 vaccine trials. J. Public Health 2020. [Google Scholar] [CrossRef]
- Adany, R.; Kosa, K.; Sandor, J.; Papp, M.; Furjes, G. General practitioners’ cluster: A model to reorient primary health care to public health services. Eur. J. Public Health 2013, 23, 529–530. [Google Scholar] [CrossRef] [Green Version]
- Llanaj, E.; Vincze, F.; Kosa, Z.; Bardos, H.; Dioszegi, J.; Sandor, J.; Adany, R. Deteriorated Dietary Patterns with Regards to Health and Environmental Sustainability among Hungarian Roma Are Not Differentiated from Those of the General Population. Nutrients 2021, 13, 721. [Google Scholar] [CrossRef]
- Sandor, J.; Nagy, A.; Foldvari, A.; Szabo, E.; Csenteri, O.; Vincze, F.; Sipos, V.; Kovacs, N.; Palinkas, A.; Papp, M.; et al. Delivery of cardio-metabolic preventive services to Hungarian Roma of different socio-economic strata. Fam. Pract. 2017, 34, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandor, J.; Nagy, A.; Jenei, T.; Foldvari, A.; Szabo, E.; Csenteri, O.; Vincze, F.; Sipos, V.; Kovacs, N.; Palinkas, A.; et al. Influence of patient characteristics on preventive service delivery and general practitioners’ preventive performance indicators: A study in patients with hypertension or diabetes mellitus from Hungary. Eur. J. Gen. Pract. 2018, 24, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Sandor, J.; Kosa, K.; Papp, M.; Furjes, G.; Korosi, L.; Jakovljevic, M.; Adany, R. Capitation-Based Financing Hampers the Provision of Preventive Services in Primary Health Care. Front. Public Health 2016, 4, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosa, K.; Katona, C.; Papp, M.; Furjes, G.; Sandor, J.; Biro, K.; Adany, R. Health mediators as members of multidisciplinary group practice: Lessons learned from a primary health care model programme in Hungary. BMC Fam. Pract. 2020, 21, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | Sample from 2011 | Sample from 2018 | p-Value |
| Mean (95% CI) | Mean (95% CI) | ||
| Fasting plasma glucose (mmol/L) | 5.5 (5.3–5.7) | 5.1 (5.0–5.3) | <0.001 |
| Fasting TG (mmol/L) | 1.6 (1.5–1.7) | 1.6 (1.5–1.7) | 0.274 |
| HDL-C (mmol/L) | 1.2 (1.2–1.2) | 1.3 (1.2–1.3) | 0.049 |
| Waist circumference (cm) | 90.7 (89.1–92.3) | 94.8 (93.1–96.5) | 0.001 |
| Systolic blood pressure (mmHg) | 126.4 (124.6–128.3) | 123.1 (121.4–124.9) | 0.036 |
| Diastolic blood pressure (mmHg) | 78.8 (77.9–79.7) | 80.0 (78.9–81.0) | 0.032 |
| B | Prevalence in % (95% CI) | Prevalence in % (95% CI) | p-Value |
| Prevalence of antihypertensive treatment | 30.3 (26.3–34.7) | 31.6 (27.0–36.4) | 0.709 |
| Prevalence of antidiabetic treatment | 6.8 (4.7–9.3) | 11.2 (8.3–14.7) | 0.024 |
| Prevalence of lipid-lowering therapy | 11.1 (8.5–14.3) | 10.7 (7.9–14.1) | 0.840 |
| 20–34 Years | 35–49 Years | 50–64 Years | ||||
|---|---|---|---|---|---|---|
| MetS and Its Components | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Central obesity | 1.13 (1.04–1.22) | 0.002 | 1.07 (0.99–1.14) | 0.085 | 1.04 (0.96–1.13) | 0.373 |
| Raised BP or treated hypertension | 1.06 (0.96–1.16) | 0.270 | 1.07 (1.00–1.14) | 0.037 | 1.10 (1.01–1.19) | 0.028 |
| Raised FPG concentration or previously diagnosed diabetes mellitus | 0.97 (0.87–1.08) | 0.576 | 0.96 (0.89–1.03) | 0.221 | 0.97 (0.90–1.04) | 0.421 |
| Raised TG levels or treated lipid disorder | 1.09 (0.99–1.20) | 0.059 | 1.07 (1.00–1.14) | 0.041 | 1.00 (0.933–1.07) | 0.992 |
| Reduced HDL-C levels or treated lipid disorder | 1.06 (0.98–1.14) | 0.136 | 0.97 (0.91–1.03) | 0.274 | 0.91 (0.84–0.98) | 0.008 |
| Metabolic syndrome | 1.10 (1.01–1.20) | 0.038 | 1.07 (1.00–1.14) | 0.048 | 0.98 (0.91–1.05) | 0.523 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piko, P.; Dioszegi, J.; Kosa, Z.; Sandor, J.; Moizs, M.; Adany, R. Changes in the Prevalence of Metabolic Syndrome, Its Components, and Relevant Preventive Medication between 2011 and 2018 in the Northeast Hungarian Roma Population. J. Pers. Med. 2021, 11, 595. https://doi.org/10.3390/jpm11070595
Piko P, Dioszegi J, Kosa Z, Sandor J, Moizs M, Adany R. Changes in the Prevalence of Metabolic Syndrome, Its Components, and Relevant Preventive Medication between 2011 and 2018 in the Northeast Hungarian Roma Population. Journal of Personalized Medicine. 2021; 11(7):595. https://doi.org/10.3390/jpm11070595
Chicago/Turabian StylePiko, Peter, Judit Dioszegi, Zsigmond Kosa, Janos Sandor, Mariann Moizs, and Roza Adany. 2021. "Changes in the Prevalence of Metabolic Syndrome, Its Components, and Relevant Preventive Medication between 2011 and 2018 in the Northeast Hungarian Roma Population" Journal of Personalized Medicine 11, no. 7: 595. https://doi.org/10.3390/jpm11070595