
Deep Learning Assisted Diagnosis of Onychomycosis on Whole-Slide Images

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Image Data Collection
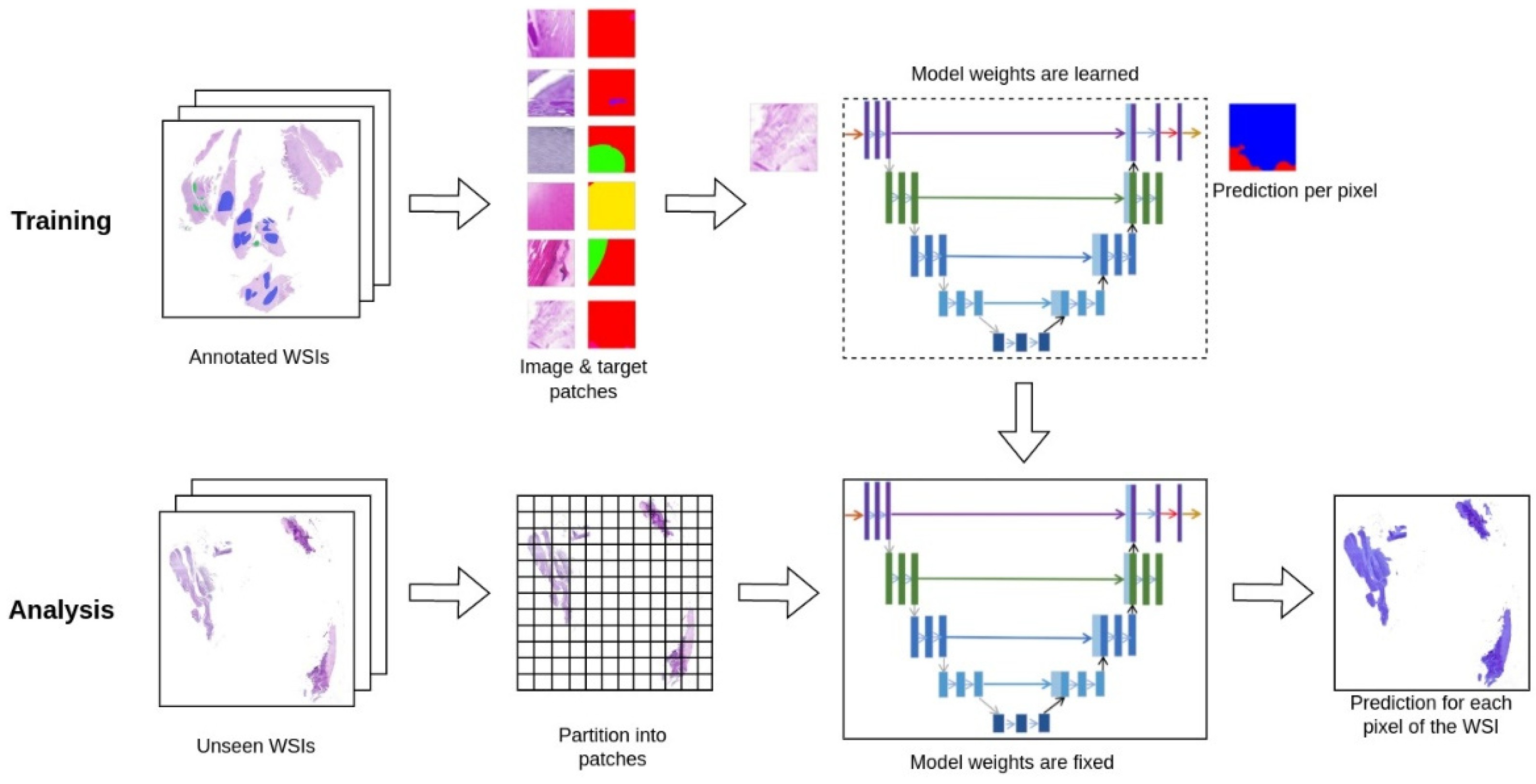
2.3. Machine-Learning Model and Training
2.4. Annotation Data Collection
2.5. Case-Level Prediction
2.6. Study Evaluation
3. Results
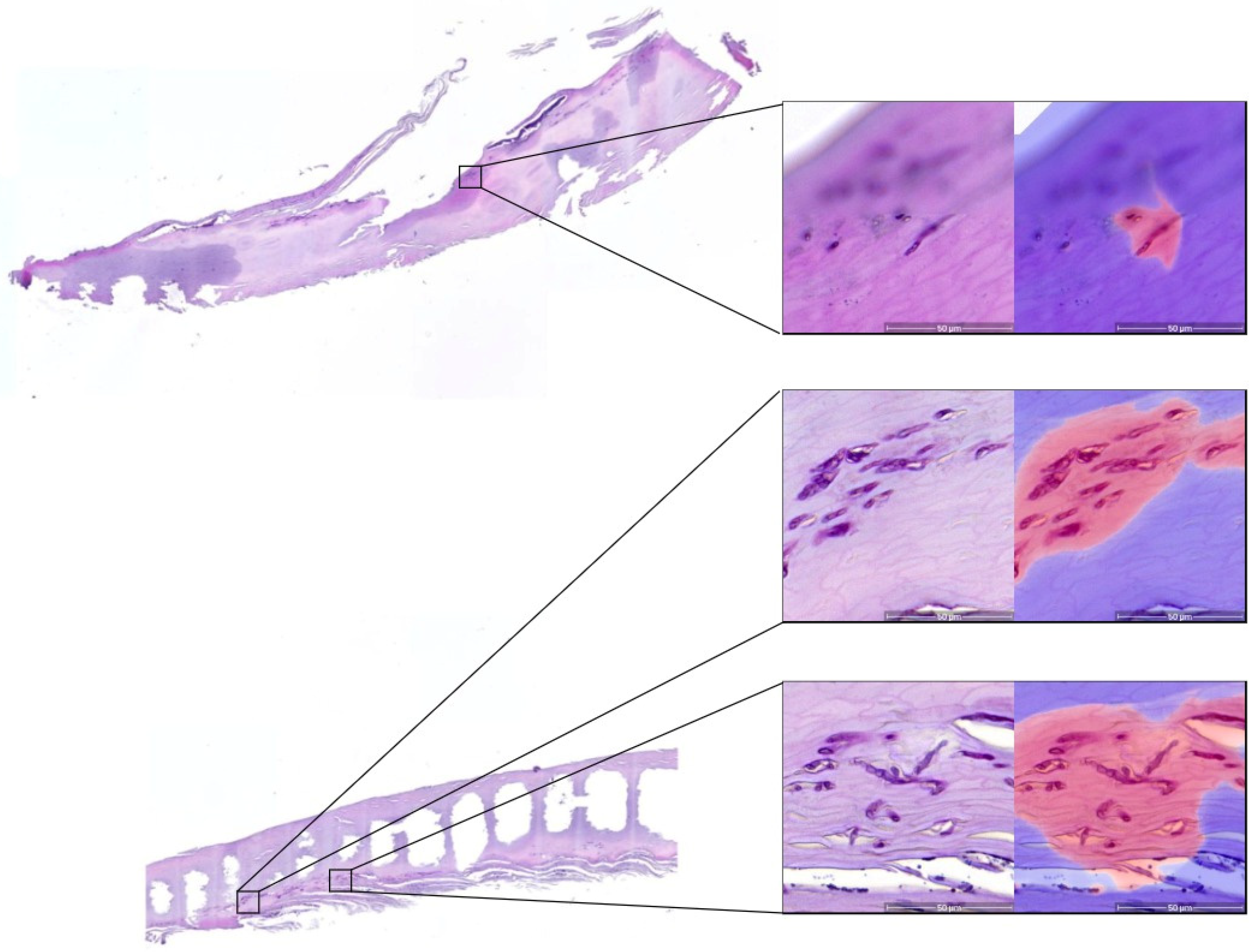
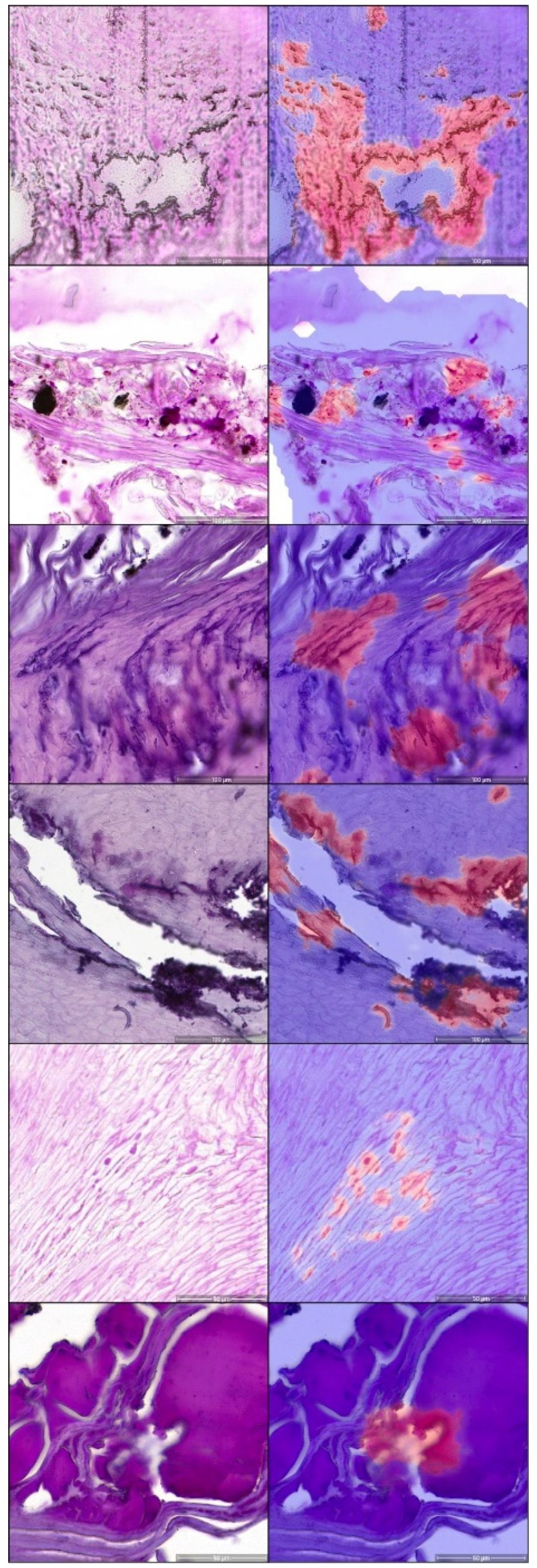
3.1. Segmentation Performance
3.2. Case-Level Performance
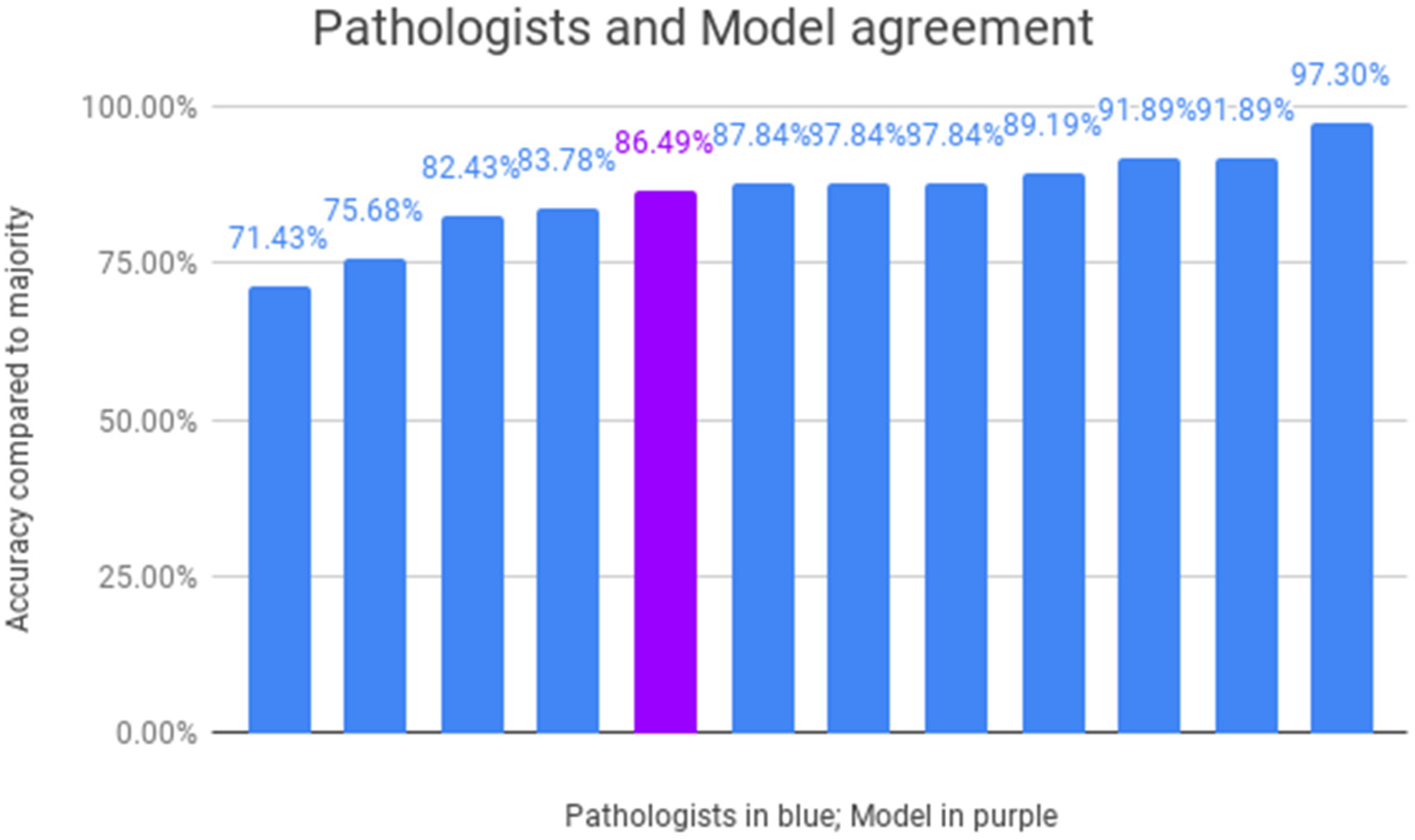
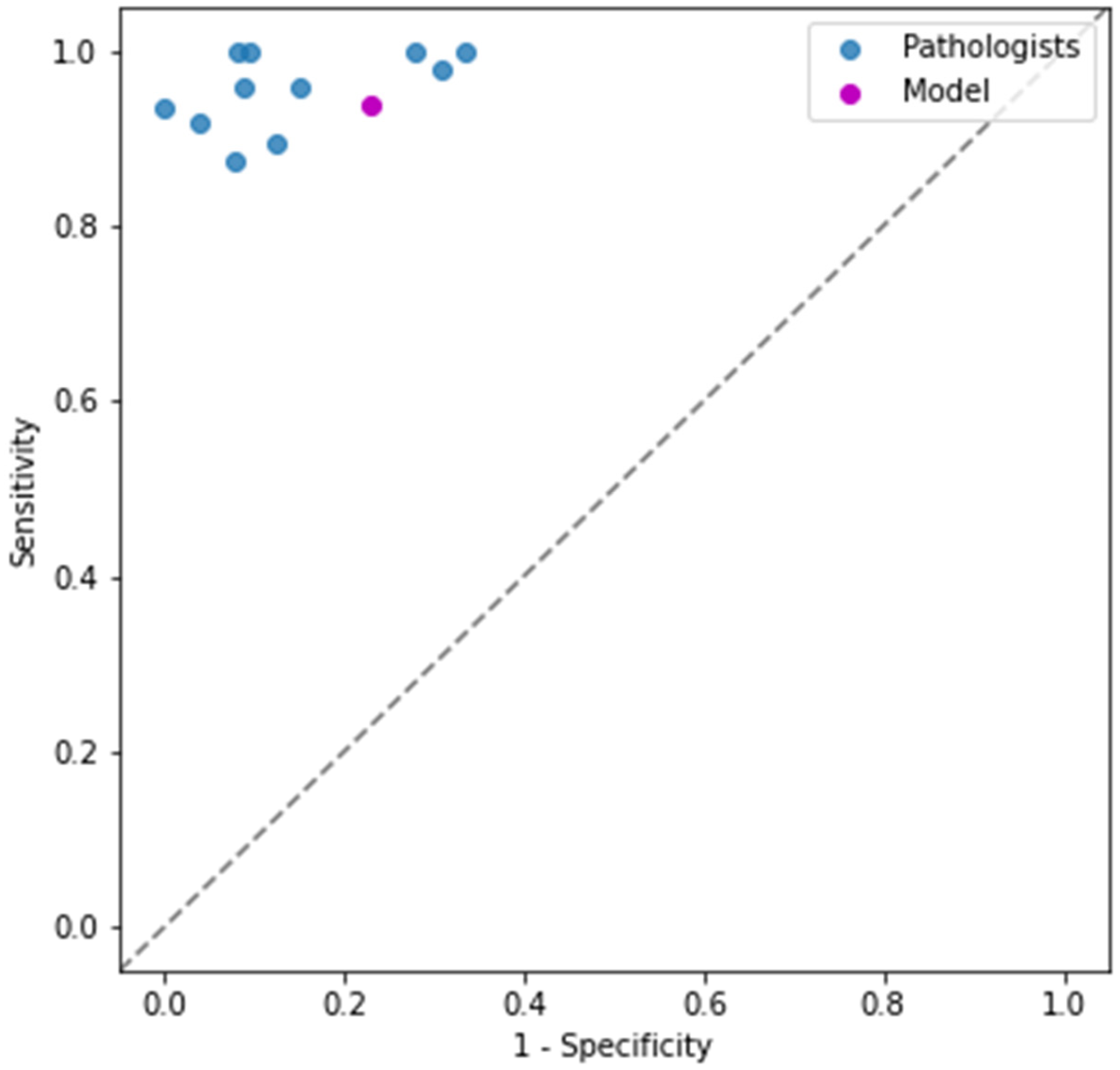
3.3. Inter-Dermatopathologist Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, A.K.; Taborda, V.B.A.; Taborda, P.R.O.; Shemer, A.; Summerbell, R.C.; Nakrieko, K.A. High prevalence of mixed infections in global onychomycosis. PLoS ONE 2020, 15, e0239648. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Versteeg, S.G.; Shear, N.H. Onychomycosis in the 21st Century: An Update on Diagnosis, Epidemiology, and Treatment. J. Cutan. Med. Surg. 2017, 21, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Guibal, F.; Baran, R.; Duhard, E.; de Chauvin, M.F. Epidemiology and management of onychomycosis in private dermatological practice in France. Ann. Dermatol. Venereol. 2008, 135, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Koshnick, R.L.; Lilly, K.K.; St Clair, K.; Finnegan, M.T.; Warshaw, E.M. Use of diagnostic tests by dermatologists, podiatrists and family practitioners in the United States: Pilot data from a cross-sectional survey. Mycoses 2007, 50, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U.; Nenoff, P.; Haroske, G.; Haenssle, H.A. The Diagnosis and Treatment of Nail Disorders. Dtsch. Arztebl. Int. 2016, 113, 509–518. [Google Scholar] [CrossRef]
- Chokoeva, A.A.; Tchernev, G.; Patterson, J.W.; Lotti, T.; Wollina, U. Life-threatening onychomycosis imitator. J. Biol. Regul. Homeost. Agents 2015, 29, 31–32. [Google Scholar]
- Wilsmann-Theis, D.; Sareika, F.; Bieber, T.; Schmid-Wendtner, M.H.; Wenzel, J. New reasons for histopathological nail-clipping examination in the diagnosis of onychomycosis. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Bombace, F.; Iovene, M.R.; Galdiero, M.; Martora, F.; Nicoletti, G.F.; D’Andrea, M.; Della Pepa, M.E.; Vitiello, M. Non-dermatophytic onychomycosis diagnostic criteria: An unresolved question. Mycoses 2016, 59, 558–565. [Google Scholar] [CrossRef]
- Hamer, E.; Moore, C.; Denning, D. Comparison of two fluorescent whiteners, Calcofluor and Blankophor, for the detection of fungal elements in clinical specimens in the diagnostic laboratory. Clin. Microbiol. Infect. 2006, 12, 181–184. [Google Scholar] [CrossRef]
- Bosshard, P.P. Incubation of fungal cultures: How long is long enough? Mycoses 2011, 54, e539–e545. [Google Scholar] [CrossRef]
- Gupta, A.K.; Zaman, M.; Singh, J. Fast and sensitive detection of Trichophyton rubrum DNA from the nail samples of patients with onychomycosis by a double-round polymerase chain reaction-based assay. Br. J. Dermatol. 2007, 157, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Reisberger, E.M.; Abels, C.; Landthaler, M.; Szeimies, R.M. Histopathological diagnosis of onychomycosis by periodic acid-Schiff-stained nail clippings. Br. J. Dermatol. 2003, 148, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Lawry, M.A.; Haneke, E.; Strobeck, K.; Martin, S.; Zimmer, B.; Romano, P.S. Methods for diagnosing onychomycosis: A comparative study and review of the literature. Arch. Dermatol. 2000, 136, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Helfen, M.; Wagenpfeil, S.; Vogt, T.; Muller, C.S.L. Neglect of the histological diagnostics of onychomycosis—The best would be so easy. J. Dtsch. Dermatol. Ges. 2021, 19, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Velasquez-Agudelo, V.; Cardona-Arias, J.A. Meta-analysis of the utility of culture, biopsy, and direct KOH examination for the diagnosis of onychomycosis. BMC Infect. Dis. 2017, 17, 166. [Google Scholar] [CrossRef] [PubMed]
- Lilly, K.K.; Koshnick, R.L.; Grill, J.P.; Khalil, Z.M.; Nelson, D.B.; Warshaw, E.M. Cost-effectiveness of diagnostic tests for toenail onychomycosis: A repeated-measure, single-blinded, cross-sectional evaluation of 7 diagnostic tests. J. Am. Acad. Dermatol. 2006, 55, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.; Schrittwieser, J.; Simonyan, K.; Antonoglou, I.; Huang, A.; Guez, A.; Hubert, T.; Baker, L.; Lai, M.; Bolton, A.; et al. Mastering the game of Go without human knowledge. Nature 2017, 550, 354–359. [Google Scholar] [CrossRef]
- Jumper, J.; Evans, R.; Pritzel, A.; Green, T.; Figurnov, M.; Ronneberger, O.; Tunyasuvunakool, K.; Bates, R.; Zidek, A.; Potapenko, A.; et al. Highly accurate protein structure prediction with AlphaFold. Nature 2021, 596, 583–589. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Anwar, S.M.; Majid, M.; Qayyum, A.; Awais, M.; Alnowami, M.; Khan, M.K. Medical Image Analysis using Convolutional Neural Networks: A Review. J. Med. Syst. 2018, 42, 226. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Haenssle, H.A.; Fink, C.; Schneiderbauer, R.; Toberer, F.; Buhl, T.; Blum, A.; Kalloo, A.; Hassen, A.B.H.; Thomas, L.; Enk, A.; et al. Man against machine: Diagnostic performance of a deep learning convolutional neural network for dermoscopic melanoma recognition in comparison to 58 dermatologists. Ann. Oncol. 2018, 29, 1836–1842. [Google Scholar] [CrossRef]
- Winkler, J.K.; Sies, K.; Fink, C.; Toberer, F.; Enk, A.; Deinlein, T.; Hofmann-Wellenhof, R.; Thomas, L.; Lallas, A.; Blum, A.; et al. Melanoma recognition by a deep learning convolutional neural network-Performance in different melanoma subtypes and localisations. Eur. J. Cancer 2020, 127, 21–29. [Google Scholar] [CrossRef] [PubMed]
- De Logu, F.; Ugolini, F.; Maio, V.; Simi, S.; Cossu, A.; Massi, D.; Italian Association for Cancer Research Study Group; Nassini, R.; Laurino, M. Recognition of Cutaneous Melanoma on Digitized Histopathological Slides via Artificial Intelligence Algorithm. Front. Oncol. 2020, 10, 1559. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Jiang, Q.; Zhou, B.; Chen, D. Convolutional neural networks for computer-aided detection or diagnosis in medical image analysis: An overview. Math. Biosci. Eng. 2019, 16, 6536–6561. [Google Scholar] [CrossRef]
- Schmitz, R.; Madesta, F.; Nielsen, M.; Krause, J.; Steurer, S.; Werner, R.; Rosch, T. Multi-scale fully convolutional neural networks for histopathology image segmentation: From nuclear aberrations to the global tissue architecture. Med. Image Anal. 2021, 70, 101996. [Google Scholar] [CrossRef]
- Le’Clerc Arrastia, J.; Heilenkotter, N.; Otero Baguer, D.; Hauberg-Lotte, L.; Boskamp, T.; Hetzer, S.; Duschner, N.; Schaller, J.; Maass, P. Deeply Supervised UNet for Semantic Segmentation to Assist Dermatopathological Assessment of Basal Cell Carcinoma. J. Imaging 2021, 7, 71. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.W.; Liou, Y.A.; Lin, Y.J.; Chang, C.C.; Chu, P.H.; Lee, Y.C.; Wang, C.H.; Chao, T.K. Artificial intelligence-assisted fast screening cervical high grade squamous intraepithelial lesion and squamous cell carcinoma diagnosis and treatment planning. Sci. Rep. 2021, 11, 16244. [Google Scholar] [CrossRef]
- Bussola, N.; Papa, B.; Melaiu, O.; Castellano, A.; Fruci, D.; Jurman, G. Quantification of the Immune Content in Neuroblastoma: Deep Learning and Topological Data Analysis in Digital Pathology. Int. J. Mol. Sci. 2021, 22, 8804. [Google Scholar] [CrossRef]
- Decroos, F.; Springenberg, S.; Lang, T.; Papper, M.; Zapf, A.; Metze, D.; Steinkraus, V.; Boer-Auer, A. A Deep Learning Approach for Histopathological Diagnosis of Onychomycosis: Not Inferior to Analogue Diagnosis by Histopathologists. Acta. Derm. Venereol. 2021, 101, adv00532. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; pp. 234–241. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 14–19 June 2020; pp. 770–778. [Google Scholar]
- Bokhorst, J.-M.; Pinckaers, H.; van Zwam, P.; Nagtegaal, I.; van der Laak, J.; Ciompi, F. Learning from sparsely annotated data for semantic segmentation in histopathology images. In Proceedings of the International Conference on Medical Imaging with Deep Learning—Full Paper Track, Zurich, Switzerland, 6–9 July 2020. [Google Scholar]
- Daniel, C.R., 3rd; Elewski, B.E. The diagnosis of nail fungus infection revisited. Arch. Dermatol. 2000, 136, 1162–1164. [Google Scholar] [CrossRef] [PubMed]
- Harvey, C.K.; Richardson, A. Techniques for obtaining specimens for culture to confirm onychomycosis. J. Am. Podiatr. Med. Assoc. 2000, 90, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Braun, M.; Hummel, P.; Beck, S.; Dabrock, P. Primer on an ethics of AI-based decision support systems in the clinic. J. Med. Ethics. 2020, 47, e3. [Google Scholar] [CrossRef] [PubMed]
- Safdar, N.M.; Banja, J.D.; Meltzer, C.C. Ethical considerations in artificial intelligence. Eur. J. Radiol. 2020, 122, 108768. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Pixel Count (Millions) | Share of Dataset |
|---|---|---|
| Cornified nail | 166.15 | 44.27% |
| Artifact | 80.51 | 21.46% |
| Air bubble | 48.46 | 12.91% |
| Out of focus | 39.33 | 10.48% |
| Serum | 15.67 | 4.18% |
| Tinea (fungal elements) | 9.38 | 2.50% |
| Parakeratosis | 7.82 | 2.08% |
| Tissue border | 3.63 | 0.97% |
| Squamous epithelium | 2.13 | 0.57% |
| Erythrocytes | 1.02 | 0.27% |
| Bacteria | 0.99 | 0.26% |
| Neutrophiles | 0.15 | 0.04% |
| Not pathological | 0.02 | 0.01% |
| Tinea | Other | Total | Recall | |
|---|---|---|---|---|
| Air bubble | 0 | 31,381 | 31,381 | 100% |
| Erythrocytes | 0 | 101,001 | 101,001 | 100% |
| Not pathological | 0 | 1509 | 1509 | 100% |
| Out of focus | 0 | 10,454,027 | 10,454,027 | 100% |
| Squamous epithelium | 0 | 38,153 | 38,153 | 100% |
| Serum | 3279 | 3,694,931 | 3,698,210 | 99.9% |
| Cornified nail | 224,223 | 220,575,318 | 220,799,541 | 99.9% |
| Artifact | 75,452 | 23,382,523 | 23,457,975 | 99.7% |
| Parakeratosis | 19,056 | 1,315,798 | 1,334,854 | 98.6% |
| Tissue border | 71,738 | 4,458,402 | 4,530,140 | 98.4% |
| Bacteria | 38,060 | 726,020 | 764,080 | 95.0% |
| Tinea (fungal elements) | 2,456,456 | 669,049 | 3,125,505 | 78.6% |
| Total | 2,888,264 | 265,448,112 | 268,336,376 | |
| Precision | 85.0% | 99.7% |
| Positive | Negative | Recall | ||
|---|---|---|---|---|
| True label | Positive | 45 | 3 | 0.94 |
| Negative | 6 | 20 | 0.77 | |
| Precision | 0.88 | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jansen, P.; Creosteanu, A.; Matyas, V.; Dilling, A.; Pina, A.; Saggini, A.; Schimming, T.; Landsberg, J.; Burgdorf, B.; Giaquinta, S.; et al. Deep Learning Assisted Diagnosis of Onychomycosis on Whole-Slide Images. J. Fungi 2022, 8, 912. https://doi.org/10.3390/jof8090912
Jansen P, Creosteanu A, Matyas V, Dilling A, Pina A, Saggini A, Schimming T, Landsberg J, Burgdorf B, Giaquinta S, et al. Deep Learning Assisted Diagnosis of Onychomycosis on Whole-Slide Images. Journal of Fungi. 2022; 8(9):912. https://doi.org/10.3390/jof8090912
Chicago/Turabian StyleJansen, Philipp, Adelaida Creosteanu, Viktor Matyas, Amrei Dilling, Ana Pina, Andrea Saggini, Tobias Schimming, Jennifer Landsberg, Birte Burgdorf, Sylvia Giaquinta, and et al. 2022. "Deep Learning Assisted Diagnosis of Onychomycosis on Whole-Slide Images" Journal of Fungi 8, no. 9: 912. https://doi.org/10.3390/jof8090912