
Effects of Stochastic Resonance on Sensorimotor Performance during Exercise-Induced Muscle Damage

School of Health Sciences, Queen Margaret University, Edinburgh, Scotland EH21 6UU, UK
J. Funct. Morphol. Kinesiol. 2017, 2(2), 16; https://doi.org/10.3390/jfmk2020016
Submission received: 15 March 2017
/
Revised: 26 April 2017
/
Accepted: 6 May 2017
/
Published: 16 May 2017
(This article belongs to the Special Issue Muscle Damage and Regeneration)
Abstract
:The aim of this study was to assess the effects of stochastic resonance (SR) stimulation on sensorimotor performance during an episode of exercise-induced muscle damage (EIMD). Thirty four men (age: 21.3 (±2.6) years; height 1.78 (±0.06) m; body mass 72.3 (±7.4) kg (mean (±SD)) gave their informed consent to participate in this study.Sensorimotor performance (error in replicating a target force) of the knee flexors was assessed prior to, and at 0.5 and 48 h after (i) a treatment condition involving a single-leg EIMD conditioning of the non-preferred leg, with concomitant responses to (ii) randomised presentation of SR, no SR and placebo conditions. Results showed a significant ANOVA interaction for sensorimotor performance amongst factors of condition (control period; EIMD), time (pre; post 0.5 h; post 48 h) and stimuli (SR; no SR; placebo) (F[1.5,29.3] = 5.7; p < 0.01). While scores during an antecedent control period had remained relatively constant, the EIMD protocol had elicited increased error in replicating a target force for the knee flexors of the non-preferred leg over time (worsened sensorimotor performance) that had been most prominent at 48 h after exercise, but whose negative effects had been ameliorated under conditions of SR (5.6 ± 3.1% (no SR) versus 3.7 ± 2.3% (SR) (pre) and 10.3 ± 4.2% (no SR) versus 8.1 ± 5.1% (SR) (48 h), respectively; F[1,36] = 6.0; p < 0.01). In conclusion, this study has shown that SR conditioning-related increases in the sensorimotor performance of the hamstring muscle group led to some protection from performance loss following EIMD.
1. Introduction
Unaccustomed eccentric exercise results in skeletal muscle damage in humans [1,2]. Impairment to skeletal muscle function following exercise induced muscle damage (EIMD) and during prolonged exposure to eccentric contractions is associated with symptoms that include delayed onset muscle soreness (DOMS), loss of flexibility [3], altered neuromuscular and sensorimotor performance [4,5,6] and may contribute to lower limb injuries during sporting activities. An inability of m. biceps femoris to function optimally and counter excessive knee’ anterior shear stress may leave it susceptible to injury [7].
Sensorimotor performance and the ability to scale volitional force and joint position precisely [3], relies on the integration of afferent information from peripheral mechanoreceptors, central processing and efferent information to marshal effective muscular activation and joint acuity [8]. Outcomes of joint position sense (JPS) and force error (FE) [3,9] have been used in clinical research for its assessment. Mechanisms underpinning EIMD-related derangement of sensorimotor performance in which subjects consistently undershoot target forces and incorrectly estimate joint angles [5,10], include alteration to peripheral mechanoreceptor sensitivity, changes in muscle spindle signaling and reflex sensitivity [1,4], and alteration to central methods of processing and perceptual sense of effort [11,12].
Strategies and mechanisms to attenuate post-EIMD sensorimotor deficits might facilitate proper maintenance of rehabilitative progression and precision in the delivery of optimum titration of individualised stimuli for effective conditioning. No study has assessed whether the application of sub-sensory noise stimulation known as stochastic resonance (SR) [13], might provide an effective compensatory means of augmenting sensorimotor performance during episodes of EIMD. SR stimulation has improved mechanoreceptor threshold detection in asymptomatic and somatosensory deficient subjects [14,15,16], enhanced balance and postural sway parameters [17,18,19] and in conjunction with neoprene sleeving, has improved JPS of the knee joint in asymptomatic and osteoarthritic subjects [20].
This study assessed the immediate effects of SR stimulation (0.5 and 48 h) on a selected index of sensorimotor performance (FE) during an episode of EIMD.
2. Materials and Methods
2.1. Participants
Thirty four men (age: 21.3 (±2.6) years; height 1.78 (±0.06) m; body mass 72.3 (±7.4) kg (mean (±SD)) gave their informed consent to participate in this study. All participants were regularly involved in exercise (at least 3 times per week) and were asymptomatic at the time of assessment. Participants were instructed to refrain from strenuous physical activity for the 24 h prior to testing. Assessment protocols were approved by the Research Ethics Committee, Queen Margaret University Edinburgh (5265/GL-10/04/April/2010).
2.2. Experimental Procedures
Following habituation procedures, participants completed a standardised warm-up of five minutes cycle ergometry (90 watts) and a further five minutes of static stretching of the involved musculature.
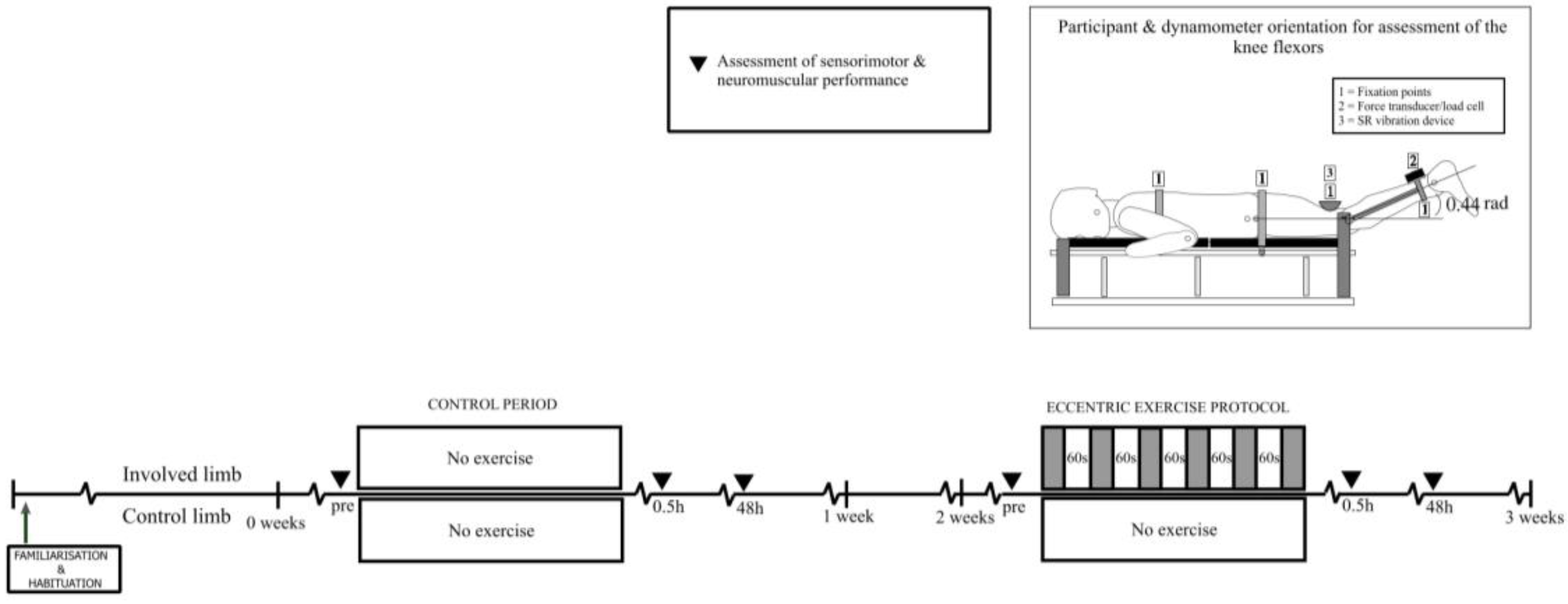
The experimental design involved comparison of the group mean responses of sensorimotor performance (force error) of the knee flexors to (i) a treatment condition involving a single-leg EIMD conditioning of the non-preferred leg (defined as the non-preferred leg for kicking [21], with contralateral limb and an antecedent time-matched period of no exercise as experimental controls, and concomitant responses to (ii) randomised presentation of SR, no SR and placebo conditions prior to, and at 0.5 and 48 h post-EIMD/control. Treatment conditions (EIMD; control) were separated by one week. The control condition was performed first in order to avoid any potential carry-over effects. Participants were verbally encouraged during periods of maximal muscle activation in a standardised manner. The protocol is illustrated schematically in Figure 1.
2.2.1. Exercise-Induced Muscle Damage (EIMD) Protocol
Participants were positioned on a gravity-resisted seated hamstring-curl machine (Life Fitness) with both knees flexed to 90°. Participants used knee flexor’ eccentric muscle actions of the non-preferred leg to actively resist knee’ movement to 0° flexion, against 120% of a concentric one repetition maximum. Participants performed a warm-up (5 sub-maximal and 5 maximal eccentric activations) and 6 sets of 10 repetitions (cadence: 0.5 Hz; 60 s inter-set recovery) with manual return of the resistance weight by the test administrator to re-establish a starting position. Verification of EIMD was undertaken using standard indirect markers including assessments of flexibility (Sit-and-Reach (Cranlea, Birmingham, UK)), delayed onset muscle soreness (visual analogue scale (VAS); 0–10 (0: no muscle soreness; 10: too sore to move the muscle); pain reported after flexing knee joint through 90°–0°) [6,22,23] and alterations in peak force (to 48 h post-EIMD/control).
2.2.2. Stochastic Resonance Protocol
SR mechanical stimulation device (Letong™ Mini Massager; model no: LT-E-007B (Ninghai Letong Electrical Appliance Company Limited, Ningbo, China), attached to a Mascot switching adapter, Type: 9885 at ~25 Hz) was attached to the participant’s non preferred leg via velcro™ strapping (3.0 ± 0.2 N) just proximal to the insertion tendon of the m. biceps femoris muscle, with the knee flexed at 25°. Participants were prone on the dynamometer and blinded to the purpose of the SR, no SR and placebo conditions and to the random order in which they were presented. Analogue control of vibration amplitude during the SR conditioning was adjusted manually by the administrator to diminish from maximal to just sub-threshold where it remained for the sequence of FE sensorimotor assessments. Similarly, no SR and placebo conditions involved the same procedure but with vibration amplitude’ end-points of zero and sub-threshold by deception, respectively. Vibration amplitude for each condition was verified by a three-dimentional accelerometer application (RS Electronics, TE 3038-0050; 0–1.2 KHz) adjacent to the tendon fitting of the stimulation device and interfaced to electronic recording components [24].
2.2.3. Assessment of Peak Force
Participants were secured in a prone position on a purpose-built dynamometer [24] with the knee flexed to a functionally relevant angle of 25° (0.44 rad) (0° = full extension) [25]. The bi-lateral lever-arms of the dynamometer were attached to the legs of the participant by padded ankle-cuffs and adjustable strapping just proximal to the lateral malleolus. Further strapping was placed across the mid-thoracic spine, pelvis and posterior thigh proximal to the knee. The dynamometer’s and knee joint’s axes of rotation were aligned as closely as possible. Following a series of sub-maximal warm-up muscle activations an auditory signal was given randomly within 1–4 s that instructed the participants to flex the knee joint as rapidly and forcefully as possible against the immovable restraint offered by the apparatus (load cell: 615, Tedea-Huntleigh, Cardiff, UK). Another auditory signal was given to the participant after 2–3 s of MVMA (maximal voluntary muscle activation) to cue neuromuscular relaxation. Each MVMA was separated from the next by at least 10 s. Static peak force (PF) was recorded as the mean score of the highest force response achieved during three intra-trial replicates. Compensation procedures for gravitational errors in forces recorded in the vertical plane were undertaken immediately prior to testing.
2.2.4. Assessment of Sensorimotor Performance
All assessments were performed prone, as described above. Familiarisation and learning (details described below) of sensorimotor performance tasks took place the day prior to the control period. A brief re-familiarisation of each task was performed on each assessment occasion. Force error (FE) was evaluated during a series of five brief muscular activations and relaxations (1 Hz) in which the aim was the precise and “blinded” attainment of a target force (50% of PF at 25° of knee flexion) using the knee flexors. The extent of FE describes the bias or constant error around a target force and lower scores reflect better sensorimotor performance. During learning, participants received only standardised verbal feedback during practice target matching (50% PF) and learned to self-perceive the performance outcomes in an arbitrary scale of measurement without units. The task was deemed to have been learned once the participant had been capable of producing consistently ten trials in which seven or more scores showed errors within ±2.0 N of the “blinded” target force (approximately to the 99% confidence limits of the technical error associated with the load cell system). FE was computed using the expression: force error = ((observed performance score − target performance score)/target performance score) × 100%) and the mean error of the five serial trials was used for subsequent data analysis.
2.3. Statistical Analysis
The effect of SR on sensorimotor performance prior to and during an episode of EIMD was assessed using two (condition: control period; EIMD) by three (time: pre; post 0.5 h; post 48 h) by three (stimuli: SR; no SR; placebo) ANOVAs with repeated measures on each of the three factors. Data for non-preferred and contralateral control limbs were analysed separately for simplicity. Similar analyses were undertaken separately for outcomes of muscle soreness, flexibility and peak force. Pre-planned difference comparisons amongst levels of factors The assumptions underpinning the use of ANOVA with repeated measures were checked and violations corrected by the Greenhouse-Geisser adjustment of the critical F-value, as indicated by GG. Statistical analyses were undertaken using SPSS version 19 (SPSS Inc., Chicago, IL, USA) and significance was accepted at p < 0.05.
3. Results
3.1. Verified EIMD
Results from ANOVA showed significant interactions for muscle soreness (F[2,36] = 8.3; p < 0.005), flexibility (F[2,36] = 6.2; p < 0.01) and peak force F[2,36] = 4.7; p < 0.01), indicating that while scores during the antecedent control period remained relatively constant, the EIMD protocol had elicited increased soreness (0.1 ± 0.2 units (pre); 0.63 ± 1.2 (0.5 h); 3.1 ± 1.8 units (48 h)), decreased flexibility (19.7 ± 5.7 cm (pre); 20.2 ± 5.7 cm (0.5 h); 17.9 ± 5.2 cm (48 h)) and decreased peak force (357.0 ± 48.8 N (pre); 321.2 ± 62.8 N (0.5 h); 261.7 ± 68.3 N (48 h) over time for the knee flexors of the non-preferred leg.
3.2. Effects of Stochastic Resonance (SR) Stimulation on Force Error (FE)
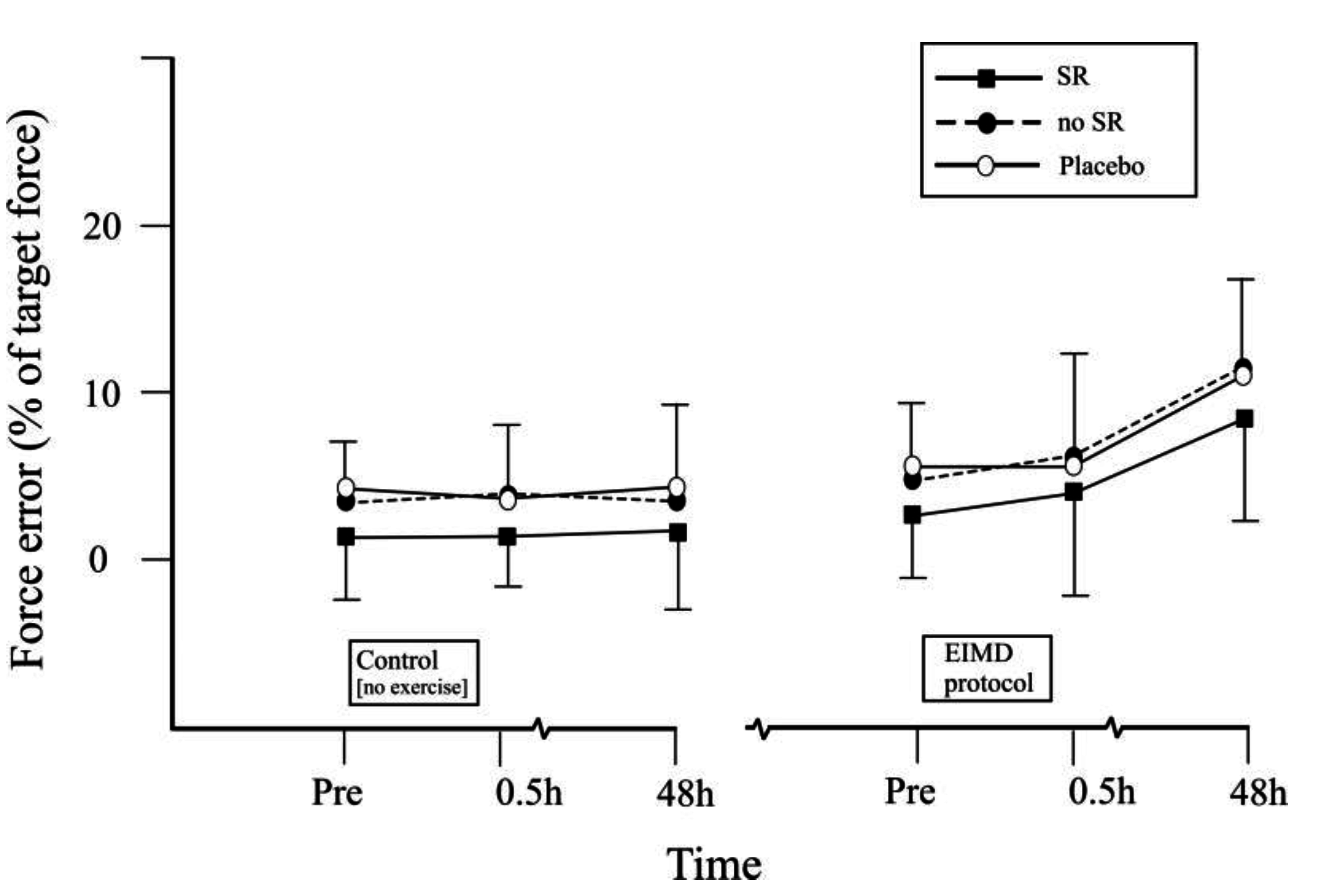
Sensorimotor performance (FE) showed a significant ANOVA interaction amongst factors of condition (control period; EIMD), time (pre; post 0.5 h; post 48 h) and stimuli (SR; no SR; placebo) (F[1.5,29.3] = 5.7; p < 0.01). Pre-planned difference comparisons amongst levels of factors suggested that while scores during the antecedent control period had remained relatively constant, the EIMD protocol had elicited increased FE for the knee flexors of the non-preferred leg over time (worse sensorimotor performance) that had been most prominent at 48 h after exercise, but whose negative effects had been ameliorated under conditions of SR (5.6 ± 3.1% (no SR) versus 3.7 ± 2.3% (SR) (pre) and 10.3 ± 4.2% (no SR) versus 8.1 ± 5.1% (SR) (48 h), respectively; F[1,36] = 6.0; p < 0.01; Please see Figure 2). The findings for the leg that had undergone EIMD and also separately for the contralateral control leg identified that patterns of sensorimotor performance under no SR and placebo conditions had been similar (7.4 ± 5.2% (no SR) versus 7.2 ± 5.7% (placebo), overall group mean scores across conditions (F[1,33] = 1.8; ns)) suggesting that expectation biases had not intruded on the findings of the study (Please see Table 1).
4. Discussion
The patterns of significantly increased muscle soreness, decreased flexibility and inferior in peak force performance capabilities after stressful eccentric-focused exercise was congruent with having elicited EIMD in this study and also with the finding of other studies in the literature [6,10,21].
There would appear to have been sufficient indirect evidence that the focal eccentric exercises in this study to have caused EIMD with concomitant localised damage to muscle fibres and deranged muscle spindle functioning [1].
The primary finding of this study was that SR delivered by means of sub-threshold mechanical vibration, has the capability to ameliorate the negative effects of EIMD on the sensorimotor performance of the knee flexors. Signal detection’ enhancement and concomitantly improved sensorimotor performance may have contributed to SR’ effects on remnant muscle spindle receptor sensitivity and monosynaptic reflex activity [26]. While the extent of SR-related improvement in sensorimotor performance during an episode of EIMD had been substantive, the study’s findings suggest that SR was not capable of completely counteracting sensorimotor losses during the period until 48 h after EIMD.
Deterioration of sensorimotor performance immediately after and at 24 h post-EIMD has been reported previously [10]. Variations in the extent of sensorimotor performance’ loss would be expected to be attributed to the specific characteristics of the eccentric-focused exercise protocols designed to produce damaging effects (for example, constant-velocity isokinetic dynamometry versus iso-inertial weight-resisted machines), and which nevertheless, may not be entirely relevant ecologically to the type and extent of muscular damage provoked by involving stretch-shortening cycles during novel everyday activities [27].
Metabolic fatigue might have contributed an interactive effect alongside EIMD-related deranged sensory apparatus to the inferior sensorimotor performance identified immediately (0.5 h) after exercise [28]. Errors in force replication may mimic losses in peak force [6] or be influenced by either increased activity of inflammatory muscle afferents [29], or decreased motor cortex activity [11]. Nevertheless, the extent of increased error in replicating a target force at 0.5 h (32%) and subsequently at 48 hours after EIMD (84%) compared to baseline is concerning in a physical performance characteristic that has been causally-related to major injuries to the knee [30]. Although the extent of improvement in SR using mechanical sub-threshold vibration was not sufficient under these specific experimental conditions to completely offset losses due to EIMD, using SR strategically as a mechanism by which to attenuate post-EIMD sensorimotor deficits might nevertheless facilitate improved maintenance of rehabilitative progressions and precision in the delivery of individualised stimuli for effective conditioning.
It is plausible also that the physically-active convenience sample of participants used in this study may not have been as susceptible to the influences of EIMD as might otherwise have been the case, given the increased possibility of intrusion from antecedent repeated-bout effects [22]. As such, the EIMD responses in this study may have been tempered and thus be unrepresentative of responses for individuals at low levels of physical conditioning status, such as patients initiating rehabilitation. In contrast, there is evidence for selective preservation of sensorimotor performance capabilities following EIMD that would otherwise make the SR-related improvements to sensorimotor performance observed in this study more noteworthy. Unilateral balance performance had been altered only at 24 h after EIMD, coinciding with peak alterations to PF and DOMS [24], with the authors speculating that efficient regulation of movement is routine in the presence of less severe damage and that proprioceptive function is only compromised under extremes of exercise-related stress. The preservation of normal muscle activation latencies [3,24,31] might highlight a protective conservation of biological resources and enhanced emergency reflex processes. Future studies should focus attention on whether other and more potent methods for delivering SR (for example, functional electrical stimulation) amongst episodes of EIMD might offer greater efficacy and effectiveness in enhancing sensorimotor performance under adverse conditions of exercise stress and strain responses. The latter mode of delivery for stochastic resonance would arguably be less dependent on a mechanically-intimate interface to the neuromuscular system and as such, offer the potential for greater utility during functional activities.
5. Conclusions
In conclusion, this study has shown that SR conditioning-related increases in the sensorimotor performance of the hamstring muscle group led to some protection from performance loss following EIMD. Nevertheless, the effects of EIMD elicited significant transient decreases in sensorimotor performance capabilities that exceeded the effects of SR conditioning alone. The EIMD-related performance deterioration was prominent at 0.5 and 48 h after exercise and was sufficiently potent even with mitigation by SR to raise concerns about commensurate losses of capability for precise and efficient scaling of dynamic muscle actions.
Conflicts of Interest
The author declares no conflict of interest.
References
- Proske, U.; Morgan, D.L. Muscle damage from eccentric exercise: Mechanism, mechanical signs adaptation and clinical applications. J. Physiol. 2001, 537, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Stupka, N.; Tarnopolsky, M.; Yardley, N.; Phillips, S. Cellular adaptation to repeated eccentric exercise-induced muscle damage. J. Appl. Physiol. 2001, 91, 1669–1678. [Google Scholar] [PubMed]
- Gleeson, N.; Eston, R.G.; Minshull, C.; Rees, D. Effects of antecedent flexibility conditioning on neuromuscular and sensorimotor performance during exercise-induced muscle damage. J. Exerc. Sci. Fit. 2013, 11, 107–117. [Google Scholar] [CrossRef]
- Saxton, J.M.; Clarkson, P.M.; James, R.; Miles, M.; Westerfer, M.; Clark, S.; Donelly, A.E. Neuromuscular dysfunction following eccentric exercise. Med. Sci. Sports Exerc. 1995, 27, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Brockett, C.; Warren, N.; Gregory, J.E.; Morgan, D.L.; Proske, U. A comparison of the effects of concentric versus eccentric exercise on force and position sense at the human elbow joint. Brain Res. 1997, 771, 251–258. [Google Scholar] [CrossRef]
- Byrne, C.; Twist, C.; Eston, R. Neuromuscular Function after exercise induced muscle damage. Sports Med. 2004, 34, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Colby, S.; Francisco, A.; Bing, Y.; Kirkendall, D.; Finch, M.; Garret, W. Electromyographic and Kinematic Analysis of Cutting Maneuvers Implications for Anterior Cruciate Ligament Injury. Am. J. Sports Med. 2000, 28, 234–240. [Google Scholar] [CrossRef]
- Lephart, S.M.; Fu, F.H. Proprioception and Neuromuscular Control in Joint Stability; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Beynnon, B.D.; Renstrom, P.A.; Konradsen, L.; Elmqvist, L.G.; Gottleib, D.; Dirks, M. Validation of Techniques to Measure Knee Proprioception. In Proprioception Neuromuscular Control Joint Stability; Lephart, S.M., Fu, F., Eds.; Human Kinetics: Champaign, IL, USA, 2000; pp. 127–138. [Google Scholar]
- Paschalis, V.; Nikolaidis, M.G.; Giakas, G.; Jamurtas, A.Z.; Pappas, A.; Koutedakis, Y.; Theodorou, A. Eccentric exercise affects the upper limbs more than the lower limbs in position sense and reaction angle. J. Sports Sci. 2010, 28, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Gregory, J.E.; Morgan, D.L.; Percival, P.; Weerakkody, N.S.; Canny, B.J. Force matching errors following eccentric exercise. Hum. Mov. Sci. 2004, 23, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.E.; Morgan, D.L.; Proske, U. Responses of muscle spindles following a series of eccentric contractions. Exp. Brain Res. 2004, 157, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Gammaitoni, L.; Hanggi, P.; Jung, P.; Marchesoni, F. Stochastic resonance. Rev. Mod. Phys. 1998, 70, 223–287. [Google Scholar] [CrossRef]
- Collins, J.J.; Imhoff, T.T.; Grigg, P. Noise-enhanced tactile sensation. Nature 1996, 383, 770. [Google Scholar]
- Liu, W.; Lipsitz, L.A.; Montero-Odasso, M.; Bean, J.; Kerrigan, D.C.; Collins, J.J. Noise-enhanced vibrotactile sensitivity in older adults, patients with stroke, and patients with diabetic neuropathy. Arch. Phys. Med. Rehabil. 2002, 83, 171–176. [Google Scholar] [CrossRef]
- Lugo, E.; Doti, R.; Faubert, J. Ubiquitous Crossmodal Stochastic Resonance in Humans: Auditory Noise Facilitates Tactile, Visual and Proprioceptive Sensations. PLoS ONE 2008, 3, e2860. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.; Arnold, B.; Blackburn, J.; Brown, C.; Guskiewicz, K. Enhanced balance associated with coordination training with Stochastic Resonance Stimulation in subjects with functional ankle stability. J. Neuroeng. Rehabil. 2007, 4, 463–470. [Google Scholar]
- Gravelle, D.; Laughton, C.; Katdare, K.; Niemi, J.; Lipsitz, L.; Collins, J. Noise Enhanced balance in older Adults. NeuroReport 2002, 13, 853–856. [Google Scholar] [CrossRef]
- Priplata, A.A.; Niemi, J.B.; Harry, J.D.; Lipsitz, L.A.; Collins, J.J. Vibrating insoles and balance control in elderly people. Lancet 2003, 362, 1123–1124. [Google Scholar] [CrossRef]
- Collins, A.; Blackburn, J.; Olcott, C.; Dirshl, D.; Weinhold, P. The Effect of Stochastic Resonance Electrical Stimulation and neoprene sleeve on knee proprioception. J. Orthop. Surg. Res. 2009, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Twist, C.; Gleeson, N.; Eston, R. The effects of plyometric exercise on unilateral balance performance. J. Sports Sci. 2008, 26, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Marginson, V.; Rowlands, A.V.; Gleeson, N.P.; Eston, R.G. Comparison of the Symptoms of Exercise Induced Muscle Damage after an Initial and Repeated bout of Plyometric Exercise in Men and Boys. J. Appl. Physiol. 2005, 99, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Highton, J.M.; Twist, C.; Eston, R. The Effects of Exercise-Induced Muscle Damage on Agility and Sprint Running Performance. J. Exerc. Sci. Fit. 2009, 7, 24–30. [Google Scholar] [CrossRef]
- Minshull, C.; Gleeson, N.P.; Eston, R.G.; Bailey, A.; Rees, D. Single measurement reliability and reproducibility of volitional and magnetically-evoked indices of neuromuscular performance in adults. J. Electromyogr. Kinesiol. 2009, 19, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Johnson, R.J. Anterior cruciate ligament injury rehabilitation in athletes: Biomechanical considerations. Sports Med. 1996, 22, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Fallon, J.; Carr, R.; Morgan, D. Stochastic Resonance in Muscle Receptors. J. Neurophysiol. 2004, 9, 2429–2436. [Google Scholar] [CrossRef] [PubMed]
- Kallerud, H.; Gleeson, N. Effects of stretching on performances involving stretch-shortening cycles. Sports Med. 2013, 43, 733–750. [Google Scholar] [CrossRef] [PubMed]
- Allen, T.J.; Proske, U. Effect of muscle fatigue on the sense of limb position and movement. Exp. Brain Res. 2006, 170, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Marqueste, T.; Decherchi, P.; Messan, F.; Kipson, N.; Gre´lot, L.; Jammes, Y. Eccentric exercise alters muscle sensory motor control through the release of inflammatory mediators. Brain Res. 2004, 1023, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R. Anterior Cruciate Ligament Injuries in Female Athletes: Part 1, Mechanisms and Risk Factors. Am. J. Sports Med. 2006, 34, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Strojnik, V.; Komi, P.V. Neuromuscular fatigue after maximal stretch-shortening cycle exercise. J. Appl. Physiol. 1998, 84, 344–350. [Google Scholar] [PubMed]
Figure 1.
A schematic of the protocol to assess the effects of stochastic resonance stimulation on sensorimotor performance during an episode of exercise-induced muscle damage (Filled inverted triangle symbols illustrate the timing of assessments of sensorimotor and neuromuscular performance).
Figure 1.
A schematic of the protocol to assess the effects of stochastic resonance stimulation on sensorimotor performance during an episode of exercise-induced muscle damage (Filled inverted triangle symbols illustrate the timing of assessments of sensorimotor and neuromuscular performance).

Figure 2.
Sensorimotor performance (force error, % of target force) of the knee flexors associated with three conditions (SR, closed square; no SR, closed circle; placebo, open circle) prior to and following (pre to post 48 h) an episode of exercise-induced muscle damage (group mean ± SD; some SD bars and contralateral control leg’s data removed for clarity.
Figure 2.
Sensorimotor performance (force error, % of target force) of the knee flexors associated with three conditions (SR, closed square; no SR, closed circle; placebo, open circle) prior to and following (pre to post 48 h) an episode of exercise-induced muscle damage (group mean ± SD; some SD bars and contralateral control leg’s data removed for clarity.


{kind=link}
{kind=link}
Table 1.
Group mean sensorimotor performance (force error, % of target force) of the knee flexors associated with three conditions (SR; no SR; placebo) prior to and following (pre to post 48 h) an episode of exercise-induced muscle damage for the non-preferred leg. Data are mean ± SD.
Table 1.
Group mean sensorimotor performance (force error, % of target force) of the knee flexors associated with three conditions (SR; no SR; placebo) prior to and following (pre to post 48 h) an episode of exercise-induced muscle damage for the non-preferred leg. Data are mean ± SD.
| Force Error (%) | Condition | Experimental Period | |||||
|---|---|---|---|---|---|---|---|
| Control | EIMD | ||||||
| Pre | 0.5 h | 48 h | Pre | 0.5 h | 48 h | ||
| Non-preferred leg ‡ | SR | 3.2 ± 3.2 | 2.9 ± 2.9 | 3.5 ± 3.4 | 3.7 ± 2.3 | 3.9 ± 3.7 | 8.1 ± 5.1 |
| no SR | 5.7 ± 3.7 | 5.8 ± 3.2 | 4.9 ± 3.8 | 5.6 ± 3.1 | 6.3 ± 3.1 | 10.7 ± 4.0 | |
| placebo | 5.2 ± 3.9 | 5.6 ± 3.7 | 5.1 ± 4.1 | 5.7 ± 3.3 | 6.0 ± 3.7 | 10.8 ± 4.4 | |
| Control leg † | SR | 3.7 ± 3.0 | 3.2 ± 2.9 | 3.3 ± 3.7 | 3.9 ± 3.4 | 3.6 ± 2.7 | 3.8 ± 3.8 |
| no SR | 5.9 ± 3.9 | 5.5 ± 3.4 | 5.0 ± 4.2 | 6.0 ± 4.1 | 6.5 ± 3.6 | 5.2 ± 3.6 | |
| placebo | 5.7 ± 3.3 | 5.8 ± 3.6 | 5.0 ± 4.7 | 5.6 ± 3.5 | 5.9 ± 3.8 | 5.5 ± 4.3 | |
Notes: † No changes in performance of the control leg over time (p > 0.05). ‡ Factorial interaction for performance of the non-preferred leg; please see explanation within the text (F[1.5,29.3] = 5.7; p < 0.01).
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gleeson, N. Effects of Stochastic Resonance on Sensorimotor Performance during Exercise-Induced Muscle Damage. J. Funct. Morphol. Kinesiol. 2017, 2, 16. https://doi.org/10.3390/jfmk2020016
AMA Style
Gleeson N. Effects of Stochastic Resonance on Sensorimotor Performance during Exercise-Induced Muscle Damage. Journal of Functional Morphology and Kinesiology. 2017; 2(2):16. https://doi.org/10.3390/jfmk2020016
Chicago/Turabian StyleGleeson, Nigel. 2017. "Effects of Stochastic Resonance on Sensorimotor Performance during Exercise-Induced Muscle Damage" Journal of Functional Morphology and Kinesiology 2, no. 2: 16. https://doi.org/10.3390/jfmk2020016