
Culture of Oral Mucosal Epithelial Cells for the Purpose of Treating Limbal Stem Cell Deficiency

Abstract
:1. Introduction
1.1. Limbal Stem Cell Deficiency
1.2. Treatment Strategies for Limbal Stem Cell Deficiency
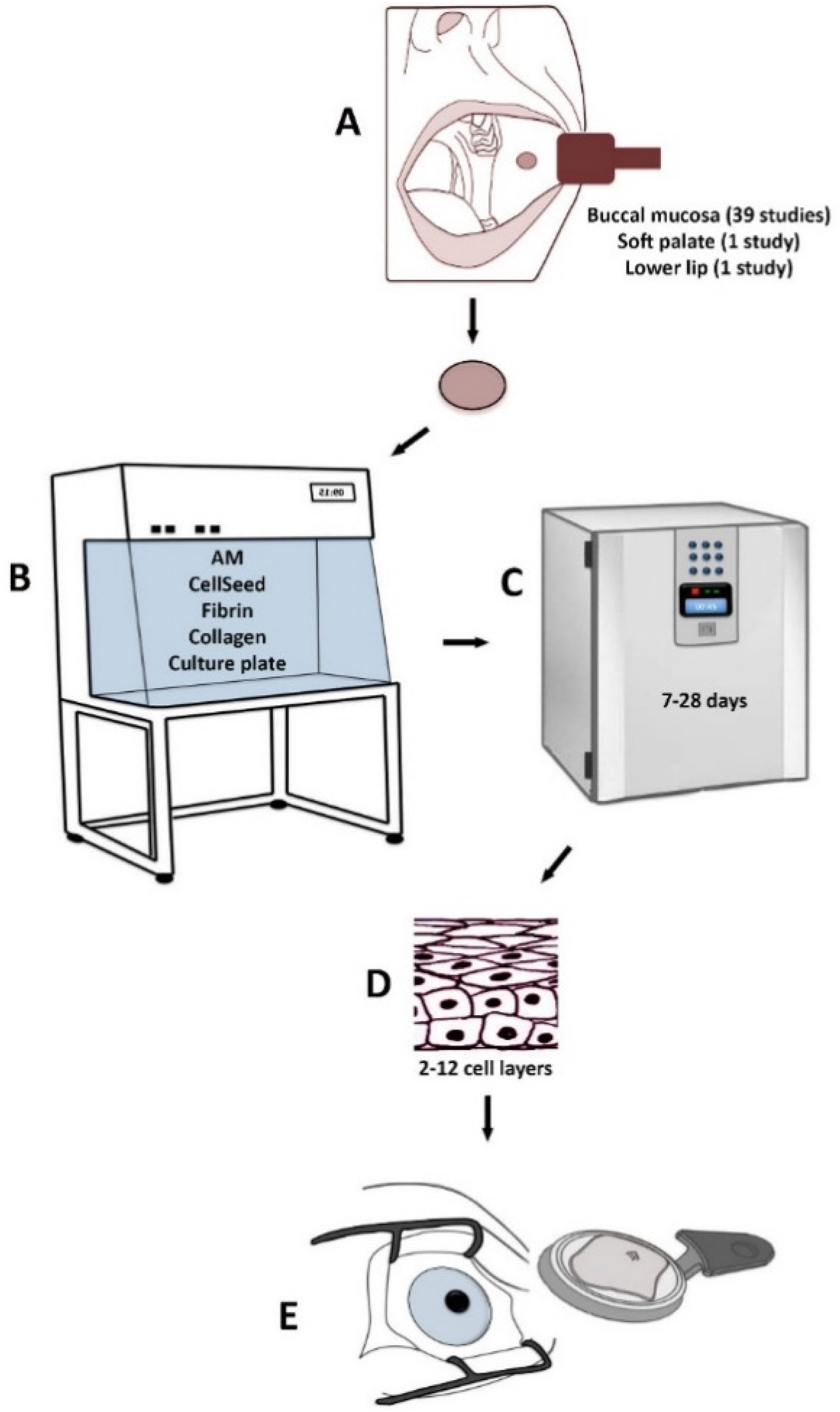
2. Cultured Autologous Oral Mucosal Epithelial Cell Sheet
3. Characteristics of the Culture Protocol for Cultured Autologous Oral Mucosal Epithelial Cell Sheet
4. Culture of Oral Mucosal Epithelial Cells on Amniotic Membrane
5. Culture of Oral Mucosal Epithelial Cells on Temperature- Responsive Surfaces
6. Culture of Oral Mucosal Epithelial Cells on Fibrin Substrates
7. Culture of Oral Mucosal Epithelial Cells on Collagen Substrates
8. Culture of Oral Mucosal Epithelial Cells on Non-Coated Culture Plates
9. Challenges and Future Perspectives
10. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Land, M.F.; Fernald, R.D. The evolution of eyes. Ann. Rev. Neurosci. 1992, 15, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Utheim, T.P. Limbal epithelial cell therapy: Past, present, and future. Methods Mol. Biol. 2013, 1014, 3–43. [Google Scholar] [PubMed]
- Cotsarelis, G.; Cheng, S.Z.; Dong, G.; Sun, T.T.; Lavker, R.M. Existence of slow-cycling limbal epithelial basal cells that can be preferentially stimulated to proliferate: Implications on epithelial stem cells. Cell 1989, 57, 201–209. [Google Scholar] [CrossRef]
- Davanger, M.; Evensen, A. Role of the pericorneal papillary structure in renewal of corneal epithelium. Nature 1971, 229, 560–561. [Google Scholar] [CrossRef] [PubMed]
- Shortt, A.J.; Secker, G.A.; Munro, P.M.; Khaw, P.T.; Tuft, S.J.; Daniels, J.T. Characterization of the limbal epithelial stem cell niche: Novel imaging techniques permit in vivo observation and targeted biopsy of limbal epithelial stem cells. Stem cells 2007, 25, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Dua, H.S.; Shanmuganathan, V.A.; Powell-Richards, A.O.; Tighe, P.J.; Joseph, A. Limbal epithelial crypts: A novel anatomical structure and a putative limbal stem cell niche. Br. J. Ophthalmol. 2005, 89, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Modjtahedi, B.S.; Eliott, D. Vitreoretinal complications of the boston keratoprosthesis. Semin. Ophthalmol. 2014, 29, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Sehic, A.; Utheim, O.A.; Ommundsen, K.; Utheim, T.P. Pre-clinical cell-based therapy for limbal stem cell deficiency. J. Funct. Biomater. 2015, 6, 863–888. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, K.R.; Tseng, S.C. Limbal autograft transplantation for ocular surface disorders. Ophthalmol. 1989, 96, 709–722. [Google Scholar]
- Jenkins, C.; Tuft, S.; Liu, C.; Buckley, R. Limbal transplantation in the management of chronic contact-lens-associated epitheliopathy. Eye 1993, 7, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, G.; Traverso, C.E.; Franzi, A.T.; Zingirian, M.; Cancedda, R.; de Luca, M. Long-term restoration of damaged corneal surfaces with autologous cultivated corneal epithelium. Lancet 1997, 349, 990–993. [Google Scholar] [CrossRef]
- Rama, P.; Matuska, S.; Paganoni, G.; Spinelli, A.; de Luca, M.; Pellegrini, G. Limbal stem-cell therapy and long-term corneal regeneration. New Engl. J. Med. 2010, 363, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Sotozono, C.; Bentley, A.J.; Mano, S.; Inatomi, T.; Koizumi, N.; Fullwood, N.J.; Kinoshita, S. Long-term phenotypic study after allogeneic cultivated corneal limbal epithelial transplantation for severe ocular surface diseases. Ophthalmology 2010, 117, 2247–2254. [Google Scholar] [CrossRef] [PubMed]
- Kolli, S.; Ahmad, S.; Lako, M.; Figueiredo, F. Successful clinical implementation of corneal epithelial stem cell therapy for treatment of unilateral limbal stem cell deficiency. Stem cells 2010, 28, 597–610. [Google Scholar] [CrossRef] [PubMed]
- Shortt, A.J.; Secker, G.A.; Rajan, M.S.; Meligonis, G.; Dart, J.K.; Tuft, S.J.; Daniels, J.T. Ex vivo expansion and transplantation of limbal epithelial stem cells. Ophthalmology 2008, 115, 1989–1997. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Inatomi, T.; Sotozono, C.; Ang, L.P.; Koizumi, N.; Yokoi, N.; Kinoshita, S. Transplantation of autologous serum-derived cultivated corneal epithelial equivalents for the treatment of severe ocular surface disease. Ophthalmology 2006, 113, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, N.; Inatomi, T.; Suzuki, T.; Sotozono, C.; Kinoshita, S. Cultivated corneal epithelial stem cell transplantation in ocular surface disorders. Ophthalmology 2001, 108, 1569–1574. [Google Scholar] [CrossRef]
- Tsai, R.J.; Li, L.M.; Chen, J.K. Reconstruction of damaged corneas by transplantation of autologous limbal epithelial cells. New Engl. J. Med. 2000, 343, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Utheim, T.P. Concise review: Transplantation of cultured oral mucosal epithelial cells for treating limbal stem cell deficiency-current status and future perspectives. Stem Cells 2015, 33, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Homma, R.; Yoshikawa, H.; Takeno, M.; Kurokawa, M.S.; Masuda, C.; Takada, E.; Tsubota, K.; Ueno, S.; Suzuki, N. Induction of epithelial progenitors in vitro from mouse embryonic stem cells and application for reconstruction of damaged cornea in mice. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4320–4326. [Google Scholar] [CrossRef] [PubMed]
- Tanioka, H.; Kawasaki, S.; Yamasaki, K.; Ang, L.P.; Koizumi, N.; Nakamura, T.; Yokoi, N.; Komuro, A.; Inatomi, T.; Kinoshita, S. Establishment of a cultivated human conjunctival epithelium as an alternative tissue source for autologous corneal epithelial transplantation. Investig. Ophthalmol. Vis. Sci. 2006, 47, 3820–3827. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Qu, L.; Wang, X.; Zhao, M.; Li, W.; Hua, J.; Shi, M.; Moldovan, N.; Wang, H.; Dou, Z. Plasticity of epidermal adult stem cells derived from adult goat ear skin. Mol. Reprod. Dev. 2007, 74, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, B.G.; Serafim, R.C.; Melo, G.B.; Silva, M.C.; Lizier, N.F.; Maranduba, C.M.; Smith, R.L.; Kerkis, A.; Cerruti, H.; Gomes, J.A.; et al. Human immature dental pulp stem cells share key characteristic features with limbal stem cells. Cell Prolif. 2009, 42, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Xu, Y.; Xiao, Z.; Yang, W.; Zhang, C.; Song, E.; Du, Y.; Li, L. Reconstruction of chemically burned rat corneal surface by bone marrow-derived human mesenchymal stem cells. Stem Cells 2006, 24, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Blazejewska, E.A.; Call, M.K.; Yamanaka, O.; Liu, H.; Schlotzer-Schrehardt, U.; Kruse, F.E.; Kao, W.W. From hair to cornea: Towards the therapeutic use of hair follicle-derived stem cells in the treatment of limbal stem cell deficiency. Stem Cells 2010, 29, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Reza, H.M.; Ng, B.Y.; Gimeno, F.L.; Phan, T.T.; Ang, L.P. Umbilical cord lining stem cells as a novel and promising source for ocular surface regeneration. Stem Cell Rev. 2011, 7, 935–947. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.J.; Loi, M.X.; Lien, G.S.; Cheng, C.F.; Pao, H.Y.; Chang, Y.C.; Ji, A.T.; Ho, J.H. Topical administration of orbital fat-derived stem cells promotes corneal tissue regeneration. Stem Cell Res. Ther. 2013, 4. [Google Scholar] [CrossRef] [PubMed]
- Inatomi, T.; Nakamura, T.; Koizumi, N.; Sotozono, C.; Yokoi, N.; Kinoshita, S. Midterm results on ocular surface reconstruction using cultivated autologous oral mucosal epithelial transplantation. Am. J. Ophthalmol. 2006, 141, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.H.; Kuo, M.T.; Tsai, Y.J.; Chen, H.C.; Chen, X.L.; Wang, S.F.; Li, L.; Hsiao, C.H.; Lin, K.K. Transplantation of cultivated oral mucosal epithelial cells for severe corneal burn. Eye 2009, 23, 1442–1450. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Inatomi, T.; Sotozono, C.; Amemiya, T.; Kanamura, N.; Kinoshita, S. Transplantation of cultivated autologous oral mucosal epithelial cells in patients with severe ocular surface disorders. Br. J. Ophthalmol. 2004, 88, 1280–1284. [Google Scholar] [CrossRef] [PubMed]
- Nishida, K.; Yamato, M.; Hayashida, Y.; Watanabe, K.; Yamamoto, K.; Adachi, E.; Nagai, S.; Kikuchi, A.; Maeda, N.; Watanabe, H.; et al. Corneal reconstruction with tissue-engineered cell sheets composed of autologous oral mucosal epithelium. Engl. J. Med. 2004, 351, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.C.; Yeh, L.K.; Tsai, Y.J.; Lai, C.H.; Chen, C.C.; Lai, J.Y.; Sun, C.C.; Chang, G.; Hwang, T.L.; Chen, J.K.; et al. Expression of angiogenesis-related factors in human corneas after cultivated oral mucosal epithelial transplantation. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5615–5623. [Google Scholar] [CrossRef] [PubMed]
- Kanayama, S.; Nishida, K.; Yamato, M.; Hayashi, R.; Maeda, N.; Okano, T.; Tano, Y. Analysis of soluble vascular endothelial growth factor receptor-1 secreted from cultured corneal and oral mucosal epithelial cell sheets in vitro. Br. J. Ophthalmol. 2009, 93, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Kanayama, S.; Nishida, K.; Yamato, M.; Hayashi, R.; Sugiyama, H.; Soma, T.; Maeda, N.; Okano, T.; Tano, Y. Analysis of angiogenesis induced by cultured corneal and oral mucosal epithelial cell sheets in vitro. Exp. Eye Res. 2007, 85, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Sekiyama, E.; Nakamura, T.; Kawasaki, S.; Sogabe, H.; Kinoshita, S. Different expression of angiogenesis-related factors between human cultivated corneal and oral epithelial sheets. Exp. Eye Res. 2006, 83, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Lim, P.; Fuchsluger, T.A.; Jurkunas, U.V. Limbal stem cell deficiency and corneal neovascularization. Semin. Ophthalmol. 2009, 24, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Ang, L.P.; Nakamura, T.; Inatomi, T.; Sotozono, C.; Koizumi, N.; Yokoi, N.; Kinoshita, S. Autologous serum-derived cultivated oral epithelial transplants for severe ocular surface disease. Arch. Ophthalmol. 2006, 124, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Burillon, C.; Huot, L.; Justin, V.; Nataf, S.; Chapuis, F.; Decullier, E.; Damour, O. Cultured autologous oral mucosal epithelial cell sheet (CAOMECS) transplantation for the treatment of corneal limbal epithelial stem cell deficiency. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1325–1331. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.C.; Chen, H.L.; Lai, J.Y.; Chen, C.C.; Tsai, Y.J.; Kuo, M.T.; Chu, P.H.; Sun, C.C.; Chen, J.K.; Ma, D.H. Persistence of transplanted oral mucosal epithelial cells in human cornea. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4660–4668. [Google Scholar] [CrossRef] [PubMed]
- Gaddipati, S.; Muralidhar, R.; Sangwan, V.S.; Mariappan, I.; Vemuganti, G.K.; Balasubramanian, D. Oral epithelial cells transplanted on to corneal surface tend to adapt to the ocular phenotype. Indian J. Ophthalmol. 2014, 62, 644–648. [Google Scholar] [PubMed]
- Hirayama, M.; Satake, Y.; Higa, K.; Yamaguchi, T.; Shimazaki, J. Transplantation of cultivated oral mucosal epithelium prepared in fibrin-coated culture dishes. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Inatomi, T.; Nakamura, T.; Kojyo, M.; Koizumi, N.; Sotozono, C.; Kinoshita, S. Ocular surface reconstruction with combination of cultivated autologous oral mucosal epithelial transplantation and penetrating keratoplasty. Am. J. Ophthalmol. 2006, 142, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Kolli, S.; Ahmad, S.; Mudhar, H.S.; Meeny, A.; Lako, M.; Figueiredo, F.C. Successful application of ex vivo expanded human autologous oral mucosal epithelium for the treatment of total bilateral limbal stem cell deficiency. Stem Cells 2014, 32, 2135–2146. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Inatomi, T.; Cooper, L.J.; Rigby, H.; Fullwood, N.J.; Kinoshita, S. Phenotypic investigation of human eyes with transplanted autologous cultivated oral mucosal epithelial sheets for severe ocular surface diseases. Ophthalmology 2007, 114, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Takeda, K.; Inatomi, T.; Sotozono, C.; Kinoshita, S. Long-term results of autologous cultivated oral mucosal epithelial transplantation in the scar phase of severe ocular surface disorders. Br. J. Ophthalmol. 2011, 95, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Priya, C.G.; Arpitha, P.; Vaishali, S.; Prajna, N.V.; Usha, K.; Sheetal, K.; Muthukkaruppan, V. Adult human buccal epithelial stem cells: Identification, ex vivo expansion, and transplantation for corneal surface reconstruction. Eye 2011, 25, 1641–1649. [Google Scholar] [CrossRef] [PubMed]
- Satake, Y.; Dogru, M.; Yamane, G.Y.; Kinoshita, S.; Tsubota, K.; Shimazaki, J. Barrier function and cytologic features of the ocular surface epithelium after autologous cultivated oral mucosal epithelial transplantation. Arch. Ophthalmol. 2008, 126, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Satake, Y.; Higa, K.; Tsubota, K.; Shimazaki, J. Long-term outcome of cultivated oral mucosal epithelial sheet transplantation in treatment of total limbal stem cell deficiency. Ophthalmology 2011, 118, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Sotozono, C.; Inatomi, T.; Nakamura, T.; Koizumi, N.; Yokoi, N.; Ueta, M.; Matsuyama, K.; Kaneda, H.; Fukushima, M.; Kinoshita, S. Cultivated oral mucosal epithelial transplantation for persistent epithelial defect in severe ocular surface diseases with acute inflammatory activity. Acta Ophthalmol. 2014, 92, e447–e453. [Google Scholar] [CrossRef] [PubMed]
- Sotozono, C.; Inatomi, T.; Nakamura, T.; Koizumi, N.; Yokoi, N.; Ueta, M.; Matsuyama, K.; Miyakoda, K.; Kaneda, H.; Fukushima, M.; et al. Visual improvement after cultivated oral mucosal epithelial transplantation. Ophthalmology 2013, 120, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Takeda, K.; Nakamura, T.; Inatomi, T.; Sotozono, C.; Watanabe, A.; Kinoshita, S. Ocular surface reconstruction using the combination of autologous cultivated oral mucosal epithelial transplantation and eyelid surgery for severe ocular surface disease. Am. J. Ophthalmo. 2011, 152, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Rheinwald, J.G.; Green, H. Serial cultivation of strains of human epidermal keratinocytes: The formation of keratinizing colonies from single cells. Cell 1975, 6, 331–343. [Google Scholar] [CrossRef]
- Green, H.; Kehinde, O.; Thomas, J. Growth of cultured human epidermal cells into multiple epithelia suitable for grafting. Proc. Natl. Acad. Sci. USA 1979, 76, 5665–5668. [Google Scholar] [CrossRef] [PubMed]
- Mariappan, I.; Maddileti, S.; Savy, S.; Tiwari, S.; Gaddipati, S.; Fatima, A.; Sangwan, V.S.; Balasubramanian, D.; Vemuganti, G.K. In vitro culture and expansion of human limbal epithelial cells. Nat. Protoc. 2010, 5, 1470–1479. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.J.; Muotri, A.; Gage, F.; Varki, A. Human embryonic stem cells express an immunogenic nonhuman sialic acid. Nat. Med. 2005, 11, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Madhira, S.L.; Vemuganti, G.; Bhaduri, A.; Gaddipati, S.; Sangwan, V.S.; Ghanekar, Y. Culture and characterization of oral mucosal epithelial cells on human amniotic membrane for ocular surface reconstruction. Mol. Vis. 2008, 14, 189–196. [Google Scholar] [PubMed]
- Nakamura, T.; Endo, K.; Cooper, L.J.; Fullwood, N.J.; Tanifuji, N.; Tsuzuki, M.; Koizumi, N.; Inatomi, T.; Sano, Y.; Kinoshita, S. The successful culture and autologous transplantation of rabbit oral mucosal epithelial cells on amniotic membrane. Investig. Ophthalmol. Vis. Sci. 2003, 44, 106–116. [Google Scholar] [CrossRef]
- Nakamura, T.; Kinoshita, S. Ocular surface reconstruction using cultivated mucosal epithelial stem cells. Cornea 2003, 22, S75–S80. [Google Scholar] [CrossRef] [PubMed]
- Promprasit, D.; Bumroongkit, K.; Tocharus, C.; Mevatee, U.; Tananuvat, N. Cultivation and phenotypic characterization of rabbit epithelial cells expanded ex vivo from fresh and cryopreserved limbal and oral mucosal explants. Curr. Eye Res. 2014, 1–8. [Google Scholar]
- Sen, S.; Sharma, S.; Gupta, A.; Gupta, N.; Singh, H.; Roychoudhury, A.; Mohanty, S.; Sen, S.; Nag, T.C.; Tandon, R. Molecular characterization of explant cultured human oral mucosal epithelial cells. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9548–9554. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.M.; Fuchsluger, T.; Ahmad, S.; Katikireddy, K.R.; Armant, M.; Dana, R.; Jurkunas, U.V. Comparative analysis of human-derived feeder layers with 3T3 fibroblasts for the ex vivo expansion of human limbal and oral epithelium. Stem cell Rev. 2012, 8, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J.; Higa, K.; Kato, N.; Satake, Y. Barrier function of cultivated limbal and oral mucosal epithelial cell sheets. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5672–5680. [Google Scholar] [CrossRef] [PubMed]
- Yokoo, S.; Yamagami, S.; Mimura, T.; Amano, S.; Saijo, H.; Mori, Y.; Takato, T. UV absorption in human oral mucosal epithelial sheets for ocular surface reconstruction. Ophthalmic Res. 2006, 38, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Bardag-Gorce, F.; Oliva, J.; Wood, A.; Hoft, R.; Pan, D.; Thropay, J.; Makalinao, A.; French, S.W.; Niihara, Y. Carrier-free cultured autologous oral mucosa epithelial cell sheet (CAOMECS) for corneal epithelium reconstruction: A histological study. Ocul. Surf. 2015, 13, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, R.; Yamato, M.; Takayanagi, H.; Oie, Y.; Kubota, A.; Hori, Y.; Okano, T.; Nishida, K. Validation system of tissue-engineered epithelial cell sheets for corneal regenerative medicine. Tissue Eng. Part C Methods 2010, 16, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, Y.; Nishida, K.; Yamato, M.; Watanabe, K.; Maeda, N.; Watanabe, H.; Kikuchi, A.; Okano, T.; Tano, Y. Ocular surface reconstruction using autologous rabbit oral mucosal epithelial sheets fabricated ex vivo on a temperature-responsive culture surface. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Murakami, D.; Yamato, M.; Nishida, K.; Ohki, T.; Takagi, R.; Yang, J.; Namiki, H.; Okano, T. Fabrication of transplantable human oral mucosal epithelial cell sheets using temperature-responsive culture inserts without feeder layer cells. J. Artif. Organs Off. J. Jpn. Soc. Artif. Organs 2006, 9, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Oie, Y.; Hayashi, R.; Takagi, R.; Yamato, M.; Takayanagi, H.; Tano, Y.; Nishida, K. A novel method of culturing human oral mucosal epithelial cell sheet using post-mitotic human dermal fibroblast feeder cells and modified keratinocyte culture medium for ocular surface reconstruction. Br. J. Ophthalmol. 2010, 94, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Soma, T.; Hayashi, R.; Sugiyama, H.; Tsujikawa, M.; Kanayama, S.; Oie, Y.; Nishida, K. Maintenance and distribution of epithelial stem/progenitor cells after corneal reconstruction using oral mucosal epithelial cell sheets. PloS One 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, H.; Yamato, M.; Nishida, K.; Okano, T. Evidence of the survival of ectopically transplanted oral mucosal epithelial stem cells after repeated wounding of cornea. Mol. Ther. J. Am. Soc. Gene Ther. 2014, 22, 1544–1555. [Google Scholar] [CrossRef] [PubMed]
- Sheth, R.; Neale, M.H.; Shortt, A.J.; Massie, I.; Vernon, A.J.; Daniels, J.T. Culture and characterization of oral mucosal epithelial cells on a fibrin gel for ocular surface reconstruction. Curr. Eye Res. 2014, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, T.; Laine, J.; Juuti-Uusitalo, K.; Numminen, J.; Seppanen-Suuronen, R.; Uusitalo, H.; Skottman, H. Towards a defined, serum- and feeder-free culture of stratified human oral mucosal epithelium for ocular surface reconstruction. Acta Ophthalmol. 2013, 91, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.; Iyer, G.K.; Krishnakumar, S. Culture & characterisation of limbal epithelial cells & oral mucosal cells. Indian J. Med. Res. 2010, 131, 422–428. [Google Scholar] [PubMed]
- Hyun, D.W.; Kim, Y.H.; Koh, A.Y.; Lee, H.J.; Wee, W.R.; Jeon, S.; Kim, M.K. Characterization of biomaterial-free cell sheets cultured from human oral mucosal epithelial cells. J. Tissue Eng. Regener. Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Schwab, I.R.; Reyes, M.; Isseroff, R.R. Successful transplantation of bioengineered tissue replacements in patients with ocular surface disease. Cornea 2000, 19, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Schwab, I.R. Cultured corneal epithelia for ocular surface disease. Trans. Am. Ophthalmol. Soc. 1999, 97, 891–986. [Google Scholar] [PubMed]
- Pellegrini, G.; Ranno, R.; Stracuzzi, G.; Bondanza, S.; Guerra, L.; Zambruno, G.; Micali, G.; de Luca, M. The control of epidermal stem cells (holoclones) in the treatment of massive full-thickness burns with autologous keratinocytes cultured on fibrin. Transplantation 1999, 68, 868–879. [Google Scholar] [CrossRef] [PubMed]
- Rama, P.; Bonini, S.; Lambiase, A.; Golisano, O.; Paterna, P.; de Luca, M.; Pellegrini, G. Autologous fibrin-cultured limbal stem cells permanently restore the corneal surface of patients with total limbal stem cell deficiency. Transplantation 2001, 72, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Schwab, I.R.; Madsen, T.K.; Isseroff, R.R. A fibrin-based bioengineered ocular surface with human corneal epithelial stem cells. Cornea 2002, 21, 505–510. [Google Scholar] [CrossRef] [PubMed]
- De Rötth, A. Plastic repair of conjunctival defects with fetal membrane. Arch. Ophthalmol. 1940, 23, 522–525. [Google Scholar] [CrossRef]
- Sorsby, A.; Symons, H.M. Amniotic membrane grafts in caustic burns of the eye (burns of the second degree). Br. J. Ophthalmol. 1946, 30, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.F.; Ellies, P.; Pires, R.T.; Tseng, S.C. Amniotic membrane transplantation for partial limbal stem cell deficiency. Br. J. Ophthalmol. 2001, 85, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Tseng, S.C.; Prabhasawat, P.; Barton, K.; Gray, T.; Meller, D. Amniotic membrane transplantation with or without limbal allografts for corneal surface reconstruction in patients with limbal stem cell deficiency. Arch. Ophthalmol. 1998, 116, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J.; Shinozaki, N.; Tsubota, K. Transplantation of amniotic membrane and limbal autograft for patients with recurrent pterygium associated with symblepharon. Br. J. Ophthalmol. 1998, 82, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Shimazaki, J.; Shinozaki, N.; Tsubota, K. Role of growth factors for ocular surface reconstruction after amniotic membrane transplantation. Investig. Ophthalmol. Vis. Sci. 1998, 39, 428–430. [Google Scholar]
- Tosi, G.M.; Massaro-Giordano, M.; Caporossi, A.; Toti, P. Amniotic membrane transplantation in ocular surface disorders. J. Cell Physiol. 2005, 202, 849–851. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, N.J.; Inatomi, T.J.; Sotozono, C.J.; Fullwood, N.J.; Quantock, A.J.; Kinoshita, S. Growth factor mRNA and protein in preserved human amniotic membrane. Curr. Eye Res. 2000, 20, 173–177. [Google Scholar] [CrossRef]
- Nishida, K.; Yamato, M.; Hayashida, Y.; Watanabe, K.; Maeda, N.; Watanabe, H.; Yamamoto, K.; Nagai, S.; Kikuchi, A.; Tano, Y.; et al. Functional bioengineered corneal epithelial sheet grafts from corneal stem cells expanded ex vivo on a temperature-responsive cell culture surface. Transplantation 2004, 77, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Yamato, M.; Utsumi, M.; Kushida, A.; Konno, C.; Kikuchi, A.; Okano, T. Thermo-responsive culture dishes allow the intact harvest of multilayered keratinocyte sheets without dispase by reducing temperature. Tissue Eng. 2001, 7, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Kushida, A.; Yamato, M.; Konno, C.; Kikuchi, A.; Sakurai, Y.; Okano, T. Decrease in culture temperature releases monolayer endothelial cell sheets together with deposited fibronectin matrix from temperature-responsive culture surfaces. J. Biomed. Mater. Res. 1999, 45, 355–362. [Google Scholar] [CrossRef]
- Dunn, C.J.; Goa, K.L. Fibrin sealant: A review of its use in surgery and endoscopy. Drugs 1999, 58, 863–886. [Google Scholar] [CrossRef] [PubMed]
- Martinowitz, U.; Saltz, R. Fibrin sealant. Curr. Opin. Hematol. 1996, 3, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Le Guehennec, L.; Goyenvalle, E.; Aguado, E.; Pilet, P.; Spaethe, R.; Daculsi, G. Influence of calcium chloride and aprotinin in the in vivo biological performance of a composite combining biphasic calcium phosphate granules and fibrin sealant. J. Mater. Sci. Mater. Med. 2007, 18, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Radosevich, M.; Goubran, H.I.; Burnouf, T. Fibrin sealant: Scientific rationale, production methods, properties, and current clinical use. Vox Sang. 1997, 72, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Tuan, T.L.; Song, A.; Chang, S.; Younai, S.; Nimni, M.E. In vitro fibroplasia: Matrix contraction, cell growth, and collagen production of fibroblasts cultured in fibrin gels. Exp. Cell Res. 1996, 223, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Weisel, J.W. Fibrinogen and fibrin. Adv. Protein. Chem. 2005, 70, 247–299. [Google Scholar] [PubMed]
- Dvorak, H.F.; Harvey, V.S.; Estrella, P.; Brown, L.F.; McDonagh, J.; Dvorak, A.M. Fibrin containing gels induce angiogenesis. Implications for tumor stroma generation and wound healing. Lab. Invest. 1987, 57, 673–686. [Google Scholar] [PubMed]
- Pellegrini, G.; Dellambra, E.; Golisano, O.; Martinelli, E.; Fantozzi, I.; Bondanza, S.; Ponzin, D.; McKeon, F.; de Luca, M. P63 identifies keratinocyte stem cells. Proc. Natl. Acad. Sci. USA 2001, 98, 3156–3161. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, G.; Cohen, S. Epidermal growth factor. J. Biol. Chem. 1990, 265, 7709–7712. [Google Scholar] [PubMed]
- Herbst, R.S. Review of epidermal growth factor receptor biology. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Dua, H.S.; Miri, A.; Alomar, T.; Yeung, A.M.; Said, D.G. The role of limbal stem cells in corneal epithelial maintenance: Testing the dogma. Ophthalmology 2009, 116, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Kawakita, T.; Espana, E.M.; He, H.; Li, W.; Liu, C.Y.; Tseng, S.C. Intrastromal invasion by limbal epithelial cells is mediated by epithelial-mesenchymal transition activated by air exposure. Am. J. Pathol. 2005, 167, 381–393. [Google Scholar] [CrossRef]
- Ban, Y.; Cooper, L.J.; Fullwood, N.J.; Nakamura, T.; Tsuzuki, M.; Koizumi, N.; Dota, A.; Mochida, C.; Kinoshita, S. Comparison of ultrastructure, tight junction-related protein expression and barrier function of human corneal epithelial cells cultivated on amniotic membrane with and without air-lifting. Exp. Eye Res. 2003, 76, 735–743. [Google Scholar] [CrossRef]
- Henderson, H.W.; Collin, J.R. Mucous membrane grafting. Dev. Ophthalmol. 2008, 41, 230–242. [Google Scholar] [PubMed]
- Meyer-Blazejewska, E.A.; Kruse, F.E.; Bitterer, K.; Meyer, C.; Hofmann-Rummelt, C.; Wunsch, P.H.; Schlotzer-Schrehardt, U. Preservation of the limbal stem cell phenotype by appropriate culture techniques. Investig. Ophthalmol. Vis. Sci. 2010, 51, 765–774. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Type of Study | Cell Suspension/Explant | Substrate | Air-Lifting | Serum | 3T3 | Culture Medium | Culture Time (Days) | Morphology | Phenotype |
|---|---|---|---|---|---|---|---|---|---|---|
| Shimazaki et al., 2009 [62] | Animal | Cell suspension | Denuded AM | Yes | FBS | Yes | SHEM (aprotinin) | 7–10 | Multilayered stratified epithelium; Tight junctions | Expression of K3, ZO-1, and occludin |
| Sekiyama et al., 2006 [35] | in Vitro | Cell suspension | Denuded AM | Yes | – | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 7–14 | – | Expression of VEGF and Flt-1; Low expression of PEDF |
| Sotozono et al., 2013 [50] | Clinical | Cell suspension | Denuded AM | Yes | HAS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 8–9 | – | – |
| Sotozono et al., 2014 [49] | Clinical | Cell suspension | Denuded AM | Yes | HAS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 8–9 | – | – |
| Gaddipati et al., 2014 [40] | Clinical | Explant | Denuded AM | – | – | No | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 9 | 5–6 cell layers; Stratified epithelium | Expression of K3, K12, K19, Ki-67, p75, and PAX6; p63 expression in most of the basal and supra basal cells |
| Sen et al., 2011 [60] | in Vitro | Explant | Denuded AM | Yes | FCS | Yes | DMEM:F12 (penicillin, streptomycin, amphotericin, EGF, insulin) | 14 | Stratified epithelium; Desmosomes; Abundant mucin granules | Expression of K3, K4, K13, connexin 43, p63, p75, β1-integrin, CD29, ABCG2, and MUC 1, 5B, 6, 13, 15 and 16 |
| Satake et al., 2008 [47] | Clinical | Cell suspension | Denuded AM | Yes | FBS | Yes | DMEM:F12 (gentamycin, streptomycin, penicillin, amphotericin, EGF, insulin) | >14 | Non-keratinized, squamous, polygonal, cells with a low nuclear to cytoplasmatic ratio | – |
| Takeda et al., 2011 [51] | Clinical | Cell suspension | Denuded AM | Yes | – | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 14–16 | – | – |
| Chen et al., 2009 [39] | Clinical | Cell suspension | Denuded AM | No | FCS | Yes | DMEM:F12(penicillin, streptomycin, insulin, cholera toxin, EGF) | 14–21 | 2–5 cell layers; Elongated cell nuclei | Expression of K3, K4, K13, p63, p75, and ABCG2 |
| Chen et al., 2012 [32] | Clinical | Cell suspension | Denuded AM | No | FCS | Yes | SHEM (penicillin, streptomycin, insulin, cholera toxin, EGF) | 14–21 | 5–10 cell layers; Stratified epithelium | Expression of FGF2, K8, VEGF, endostatin, PEDF, and IL-1ra |
| Ma et al., 2009 [29] | Clinical | Suspension | Denuded AM | No | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 14–21 | 2–5 cell layers; Elongated cell nuclei | Expression of K3, K13, p63, p75, and ABCG2 |
| Nakamura et al., 2004 [30] | Clinical | Cell suspension | Denuded AM | Yes | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 14–21 | 5–6 cell layers; Desmosomes and hemidesmosomes | Expression of K3, K4, and K13 |
| Ang et al., 2006 [37] | Clinical | Cell suspension | Denuded AM | Yes | HAS/FBS | Yes | KGM (penicillin, streptomycin, insulin, EGF) | 15–16 | 4–6 cell layers; Cuboidal cells, More flattened cells superficially | Expression of K3, K4, K13, ZO-1, desmoplakin, integrin-α1, laminin 5, and collagen IV |
| Ang et al., 2006 [37] | Clinical | Cell suspension | Denuded AM | Yes | HAS/FBS | Yes | KGM (penicillin, streptomycin, insulin, EGF) | 15–16 | 4–6 cell layers; Cuboidal cells, More flattened cells superficially | Expression of K3, K4, K13, ZO-1, desmoplakin, integrin-α1, laminin 5, and collagen IV |
| Inatomi et al., 2006 [28] | Clinical | Cell suspension | Denuded AM | Yes | FCS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 15–16 | 5–6 cell layers; Cuboidal cells, several suprabasal cell layers, and flat apical cell layers | Expression of VEGF, FGF, and thrombospondin 1 |
| Inatomi et al., 2006 [28] | Clinical | Cell suspension | Denuded AM | Yes | FCS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 15–16 | 5–6 cell layers; Cuboidal cells, several suprabasal cell layers, and flat apical cell layers | Expression of VEGF, FGF, and thrombospondin 1 |
| Inatomi et al., 2006 [42] | Clinical | Cell suspension | Denuded AM | Yes | HAS/FCS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 15–16 | 5–6 cell layers; Cuboidal cells, several suprabasal cell layers, and flat apical cell layers | |
| Nakamura et al., 2011 [45] | Clinical | Cell suspension | Denuded AM | Yes | HAS | Yes | KGM (penicillin, streptomycin, insulin, cholera toxin, EGF) | 15–16 | – | – |
| Priya et al., 2011 [46] | Clinical | Cell suspension | Denuded AM | No | AS | Yes | DMEM:F12 (PI, mouse IgG1/IgG2a, mitomycin C, EGF, insulin, penicillin, streptomycin) | 18–21 | Flat and uniformly distributed epithelial cells | Low expression of p63 (3.0% ± 1.7% of cells); Negative expression of K12 |
| Sharma et al., 2011 [61] | In vitro | Cell suspension | Denuded AM | – | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 21 | 3–5 cell layers; Stratified epithelium | Expression of K3 and β1-integrin; High expression of p63 |
| Promprasit et al., 2014 [59] | in Vitro | Explant | Denuded AM | Yes | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, EGF) | 21 | 2–5 cell layers; Stratified epithelium; Cuboidal cells in basal layer, flat superficial cells | Expression of K3 and connexin 43; High expression of p63 |
| Nakamura et al., 2003 [57] | Animal | Cell suspension | Denuded AM | Yes | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 21 | 3–5 cell layers; Stratified epithelium; | Expression of K3, K4, and K13 |
| Nakamura et al., 2003 [58] | Animal | Cell suspension | Denuded AM | Yes | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 21 | 5–6 cell layers; Stratified epithelium; | Expression of K3, K4, and K13 |
| Nakamura et al., 2003 [58] | Animal | Cell suspension | Denuded AM | Yes | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF) | 21 | 5–6 cell layers; Stratified epithelium; | Expression of K3, K4, and K13 |
| Kolli et al., 2014 [43] | Clinical | Explant | Intact AM | Yes | HAS | No | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF, hydrocortisone, triiodothyronine, adenine) | 21 | 3–7 cell layers, firmly attached to each other; High nucleus to cytoplasm ratio | Expression of K3, ABCG2, and C/EBPδ; High expression of ΔNp63α; Negative for K12 and PAX6 |
| Madhira et al., 2008 [56] | in Vitro | Cell suspension | Denuded AM | No | FCS | No | DMEM:F12 (penicillin, streptomycin, amphotericin, gentamycin, insulin, cholera toxin, EGF) | 21–28 | 2–3 cell layers; Stratified epithelium; Gap junctions and desmosomes | Expression of K3, K4, K15, and connexin 43; Negative for K12 and PAX6 |
| Yokoo et al., 2006 [63] | in Vitro | Cell suspension | Denuded AM | Yes | FBS | Yes | DMEM/F12 (penicillin, streptomycin, amphotericin) | 28 | 3–5 cell layers; Stratified epithelium | – |
| Author, Year | Type of Study | Cell Suspension/Explant | Substrate | Air-Lifting | Serum | 3T3 | Culture Medium | CultureTime (Days) | Morphology | Phenotype |
|---|---|---|---|---|---|---|---|---|---|---|
| Burillon et al., 2012 [38] | Clinical | Cell suspension | CellSeed a | No | – | Yes | – | – | Similar characteristics to normal corneal epithelium; Basal membrane | Expression of K3/76, p63, laminin 5, and β1-integrin |
| Soma et al., 2014 [69] | Animal | Cell suspension | CellSeed a | – | FBS | Yes | DMEM:F12 (insulin, triiodthyronine, hydrocortisone) | 10–12 | 3–4 cell layers; Stratified epithelium; Cobble stone-like cell morphology | Expression of K14 and p63 |
| Sugiyama et al., 2014 [70] | Animal | Cell suspension | CellSeed a | – | FBS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, cholera toxin, EGF, hydrocortisone, triiodothyronine) | 14 | 3–5 cell layers; Stratified epithelium; Cuboidal cells in the basal layer, squamous epithelium on the apical side | Expression of K4, K13, MUC5 |
| Nishida et al., 2004 [31] | Clinical | Cell suspension | CellSeed a | No | – | Yes | – | 14 | Multilayered cell sheets; Microvilli, desmosomes, basement membrane | Expression of β1-integrin, K3, and p63 |
| Bardag-Gorce et al., 2015 [64] | Animal | Cell suspension | CellSeed a | – | FBS | Yes | – | 14 | Multilayered stratified epithelium | Expression of K4, ΔNp63, TIMP-1, TIMP-3, and connexin 43 |
| Hayashida et al., 2005 [66] | Animal | Cell suspension | CellSeed a | – | FBS | Yes | – | 14 | 3–5 cell layers; Stratified epithelium; | Expression of K3, K4, K13, p63, ΔNp63, and β1-integrin |
| Murakami et al., 2006 [67] | in Vitro | Cell suspension | CellSeed a | – | HAS | No | DMEM/F12 (penicillin, streptomycin, fungizone, transferrin, EGF, cholera toxin, hydrocortisone, triiodothyronine) | 14 | 3–5 cell layers; Cuboidal basal cells, flattened middle cells, and polygonal flattened superficial cells | Expression of p63 and Ki67 |
| Oie et al., 2010 [68] | Clinical | Cell suspension | CellSeed a | – | HAS | Yes | – | 14–17 | 4–5 cell layers; Small basal cells, flattened middle cells, and polygonal flattened superficial cells | Expression of K1, K3/76, K4, K10, K12, K13, K15, ZO-1, and MUC16; Moderate expression of p63 (30.7% ± 7.6% of cells) |
| Author, Year | Type of Study | Cell Suspension/Explant | Substrate | Air-Lifting | Serum | 3T3 | Culture Medium | Culture Time (Days) | Morphology | Phenotype |
|---|---|---|---|---|---|---|---|---|---|---|
| Satake et al., 2011 [48] | Clinical | Cell suspension | Fibrin-coated cell culture inserts | Yes | HAS | Yes | DMEM:F12 (penicillin, streptomycin, transferrin, EGF, hydrocortisone, triiodothyronine) | – | 5–6 cell layers; | – |
| Hirayama et al., 2012 [41] | Clinical | Cell suspension | Fibrin-coated cell culture inserts | Yes | HAS | Yes | DMEM:F12 (penicillin, streptomycin, insulin, EGF, hydrocortisone) | – | 5–6 cell layers; | – |
| Sheth et al., 2014 [71] | in Vitro | Explant | Fibrin gel | – | FCS | No | DMEM:F12 (penicillin, cholera toxin, insulin, EGF, hydrocortisone) | - | Multilayered epithelium; Cobblestone morphology | Expression of K3, K13, and K19; High expression of p63 |
| Ilmarinen et al., 2012 [72] | in Vitro | Cell suspension | Collagen IV-coated cell culture inserts | Yes | No | No | Serum-free oral PCT epithelium medium (EGF) | 13–17 | 4–12 cell layers; Stratified epithelium; Cuboidal basal cells and flat intermediate and superficial cells | Expression of K3/12, K4, K13, Ki67, and p63 |
| Kanayama et al., 2007 [34] | in Vitro | Cell suspension | Culture plate | – | FBS | Yes | DMEM (Supplements not reported) | – | Multilayered cells; Normal epithelial morphology | Expression of FGF2, VEGF, Ang1, and TGF-β1 |
| Kanayama et al., 2009 [33] | in Vitro | Cell suspension | Culture plate | – | FBS | Yes | DMEM (Supplements not reported) | 14 | Multilayered cells | Expression of VEGFr-1 |
| Hyun et al., 2014 [74] | Animal | Cell suspension | Culture plate | – | FBS | Yes | DMEM:F12 (penicillin, streptomycin, gentamycin, amphotericin) | 14 | 2–6 cell layers; Stratified epithelium | Expression of K3, K4, and Ki67; High expression of p63 |
| Krishnan et al., 2010 [73] | in Vitro | Explant | Culture plate | – | FBS | – | DMEM:F12 (streptomycin, amphotericin, EGF, insulin, transferrin, selenium, hydrocortisone) | 21 | Multilayered cells; Normal epithelial morphology | Expression of ABCG2, K3, MUC1/4/16, hBD1/2,3; High expression of p63 and ΔNp63 |
| Substrate | Total Number of Studies | Expression of p63 Not Reported | Non-Quantitative Expression of p63 Reported | Quantitative Expression of p63 Reported |
|---|---|---|---|---|
| Amniotic membrane | 24 | 16 studies | 4 studies: p63 expressed; 1 study: high expression of ΔNp63; 2 studies: high expression of p63 | 1 study: 3.0% ± 1.7% of cells |
| Temperature-responsivecell-culture inserts | 9 | 2 studies | 6 studies: p63 expressed | 1 study: 30.7% ± 7.6% of cells |
| Fibrin-coated culture plate | 2 | 2 studies | – | – |
| Fibrin gel | 1 | – | 1 study: high expression of p63 | – |
| Collagen IV-coated culture plate | 1 | – | 1 study: p63 expressed | – |
| Culture plate | 4 | 2 studies | 2 studies: high expression of p63 | – |
| Substrate/Method | Air-lifting | Animal-derived Nutrient | Use of 3T3 | Serum-free Medium | Viability | Morphology | Phenotype (Expression of p63) |
|---|---|---|---|---|---|---|---|
| Amniotic membrane | 17/24 | 16/24 | 21/24 | 0/24 | >98% (1) | 4.2 cell layers (15) | ++ |
| Temperature-responsive cell-culture inserts | 0/9 | 5/9 | 8/9 | 0/9 | 86%–93% (2) | 4.3 cell layers (6) | ++ |
| Fibrin-coated culture plate | 2/2 | 0/2 | 2/2 | 0/2 | 5–6 cell layers (2) | – | |
| Fibrin gel | 0/1 | 1/1 | 0/1 | 0/1 | – | – | +++ |
| Collagen IV-coated culture plate | 1/1 | 0/3 | 0/1 | 1/1 | – | 4–12 cell layers (1) | + |
| Culture plate | 0/4 | 4/4 | 3/4 | 0/4 | – | 2–6 cell layers (1) | +++ |
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paaske Utheim, T.; Aass Utheim, Ø.; Khan, Q.-E.-S.; Sehic, A. Culture of Oral Mucosal Epithelial Cells for the Purpose of Treating Limbal Stem Cell Deficiency. J. Funct. Biomater. 2016, 7, 5. https://doi.org/10.3390/jfb7010005
Paaske Utheim T, Aass Utheim Ø, Khan Q-E-S, Sehic A. Culture of Oral Mucosal Epithelial Cells for the Purpose of Treating Limbal Stem Cell Deficiency. Journal of Functional Biomaterials. 2016; 7(1):5. https://doi.org/10.3390/jfb7010005
Chicago/Turabian StylePaaske Utheim, Tor, Øygunn Aass Utheim, Qalb-E-Saleem Khan, and Amer Sehic. 2016. "Culture of Oral Mucosal Epithelial Cells for the Purpose of Treating Limbal Stem Cell Deficiency" Journal of Functional Biomaterials 7, no. 1: 5. https://doi.org/10.3390/jfb7010005