Comparing the Diagnostic Value of Serum D-Dimer to CRP and IL-6 in the Diagnosis of Chronic Prosthetic Joint Infection

 ,
,
Abstract
:1. Introduction:
2. Materials and Methods
2.1. Study Design
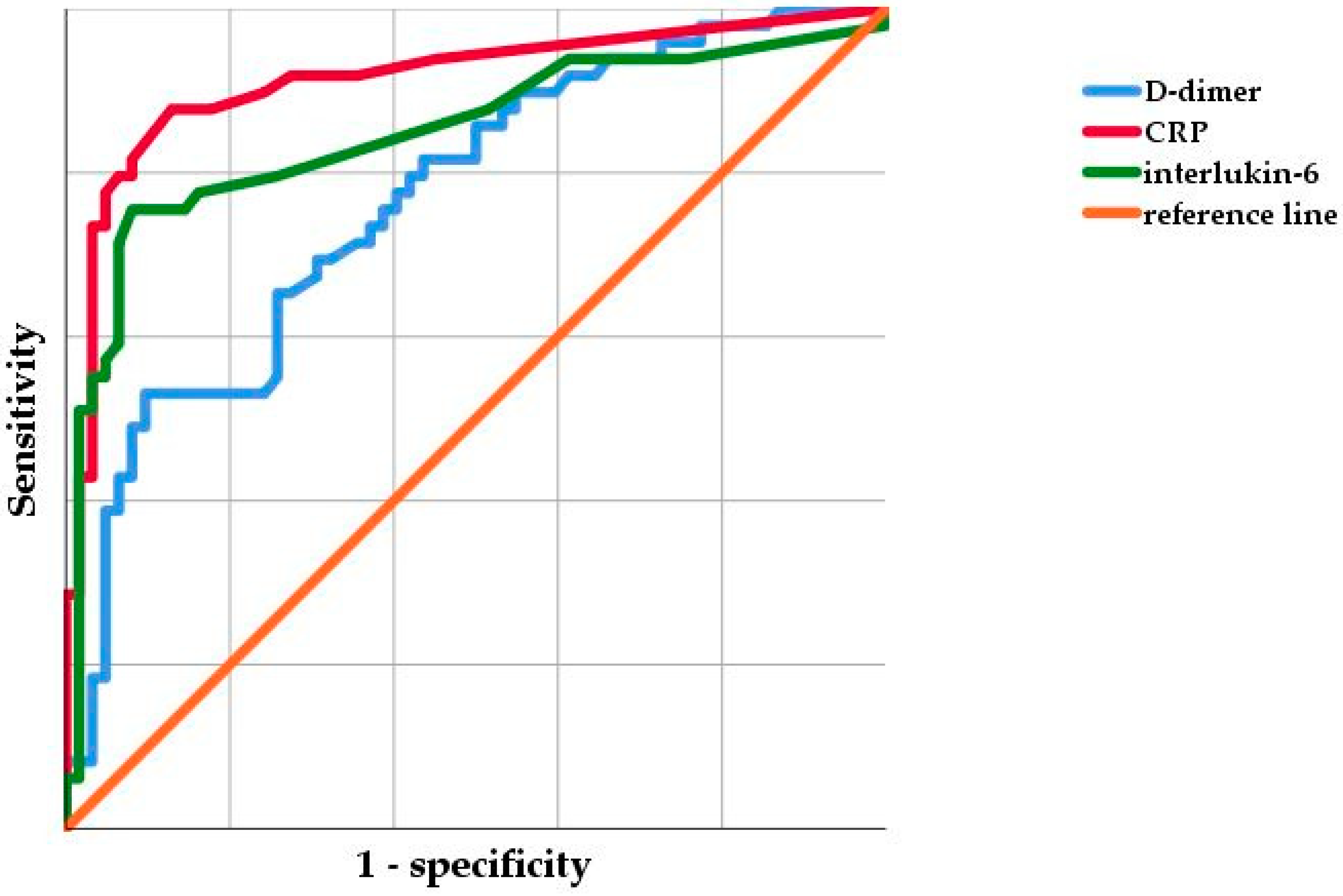
2.2. Statistical Analysis
3. Results
3.1. Demographic Details
3.2. Preoperative Serum Parameters
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Huotari, K.; Peltola, M.; Jämsen, E. The incidence of late prosthetic joints infections: A registry-based study of 112,708 primary hip and knee replacements. Acta Orthop. 2015, 86, 321–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jämsen, E.; Varonen, M.; Huhtala, H.; Lehto, M.U.; Lumio, J.; Konttinen, Y.T.; Moilanen, T. Incidence of prosthetic joint infections after primary knee arthroplasty. J. Arthroplast. 2010, 25, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Cavanaugh, P.K.; Diaz-Ledezma, C. Periprothetic knee infection: Ten strategies that work. Knee Surg. Relat. Res. 2013, 25, 155–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, B.; Schuster, P.; Braun, R.; Tagtalianidou, E.; Schlumberger, M. The diagnostic value of routine preliminary biopsy in diagnosing late prosthetic joint infection after hip and knee arthroplasty. Bone Jt. J. 2020, 102-B, 329–335. [Google Scholar] [CrossRef]
- Tarabichi, M.; Shohat, N.; Goswami, K.; Alvand, A.; Silibovsky, R.; Belden, K.; Parvizi, J. Diagnosis of Periprosthetic Joint Infection: The Potential of Next-Generation Sequencing. J. Bone Jt. Surg. Am. 2018, 100, 147–154. [Google Scholar] [CrossRef]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Parvizi, J. Diagnosing periprosthetic joint infection: Has the era of the biomarker arrived? Clin. Orthop. Relat. Res. 2014, 472, 3254–3262. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314. [Google Scholar] [CrossRef]
- Shohat, N.; Bauer, T.; Buttaro, M.; Budhiparama, N.; Cashman, J.; Della Valle, C.J.; Drago, L.; Gehrke, T.; Marcelino, G.L.; Goswami, K.; et al. Hip and knee section, what is the definition of a periprosthetic joint infection (PJI) of the knee and the hip? Can the same criteria be used for both joints? Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S325–S327. [Google Scholar] [CrossRef]
- Schwameis, M.; Steiner, M.M.; Schoergenhofer, C.; Lagler, H.; Buchtele, N.; Jilma-Stohlawetz, P.; Boehm, T.; Jilma, B. D-dimer and histamine in early stage beacteremia: A prospective controlled cohort study. Eur. J. Intern. Med. 2015, 26, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Shahi, A.; Kheir, M.M.; Tarabichi, M.; Hosseinzadeh, H.R.S.; Tan, T.L.; Parvizi, J. Serum D-dimer test is promising for the diagnosis of periprosthetic joint infection and timing of reimplantation. J. Bone Jt. Surg. Am. 2017, 99, 1419–1427. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Shao, H.Y.; Hao, L.B.; Yu, B.Z.; Qu, P.F.; Zhou, Y.X.; Chen, J.Y. Plasma Fibrinogen Exhibits Better Performance Than Plasma D-Dimer in the Diagnosis of Periprosthetic Joint Infection: A Multicenter Retrospective Study. J. Bone Jt. Surg. Am. 2019, 101, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Xie, J.; Huang, Q.; Lei, Y.; Zhang, S.; Pei, F. Plasma Fibrin Degradation Product and D-Dimer Are of Limited Value for Diagnosing Periprosthetic Joint Infection. J. Arthroplast. 2019, 34, 2454–2460. [Google Scholar] [CrossRef] [PubMed]
- Goswami, K.; Parvizi, J.; Maxwell Courtney, P. Current Recommendations for the Diagnosis of Acute and Chronic PJI for Hip and Knee-Cell Counts, Alpha-Defensin, Leukocyte Esterase, Next-generation Sequencing. Curr. Rev. Musculoskelet. Med. 2018, 11, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Svoboda, M.; Zapletalova, J.; Proskova, J.; Juranova, J. Serum IL-6 in combination with synovial IL-6/CRP shows excellent diagnostic power to detect hip and knee prosthetic joint infection. PLoS ONE 2018, 13, e0199226. [Google Scholar] [CrossRef]
- Yoon, J.R.; Yang, S.H.; Shin, Y.S. Diagnostic accuracy of interleukin-6 and procalcitonin in patients with periprosthetic joint infection: A systematic review and meta-analysis. Int. Orthop. 2018, 42, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Fu, Y.; Tang, L. Serum D-dimer as a diagnostic index of PJI and retrospective analysis of etiology in patients with PJI. Clin. Chim. Acta 2020, 506, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Li, F.; Gong, X.; Wang, J.; Huang, W.; Hu, N. Combined measurement of D-dimer and c-reactive protein levels: Highly accurate for diagnosing chronic periprothetic joint infection. J. Arthroplast. 2020, 35, 229–234. [Google Scholar] [CrossRef] [Green Version]
- Pannu, T.S.; Villa, J.M.; Patel, P.D.; Riesgo, A.M.; Barsoum, W.K.; Higuera, C.A. The utility of d-dimer for the diagnosis of periprosthetic joint infection in revision total hip and knee arthroplasty. J. Arthroplast. 2020, 35, 1692–1695. [Google Scholar] [CrossRef]
- Pieper, C.T.; Rao, K.M.; Currie, M.S.; Harris, T.B.; Cohen, H.J. Age, functional status and racial differences in plasma D-dimer levels in community dwelling eldery persons. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M649. [Google Scholar] [CrossRef]
- Zakai, N.A.; McClure, L.A.; Judd, S.E.; Kissela, B.; Howard, G.; Safford, M.; Cushman, M. D-dimer and the risk of stroke and coronary heart disease. The Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Thromb. Haemost. 2017, 117, 618–624. [Google Scholar]
- Nybo, M.; Hvas, A.M. Age-adjusted D-dimer cut-off in the diagnostic strategy for deep vein thrombosis: A systematic review. Scand. J. Clin. Lab. Investig. 2017, 77, 568–573. [Google Scholar] [CrossRef]
- Silva, D.R.; Coelho, A.C.; Gazzana, M.B.; Menna Barreto, S.S.; Knorst, M.M. D-Dimer levels in stable COPD patients: A case-control study. COPD 2012, 9, 426–431. [Google Scholar] [CrossRef]
- Kawai, T.; Kuroda, Y.; Goto, K.; Matsuda, S. Does prophylactic administration of edoxaban increase d-dimer levels after total hip arthroplasty? J. Clin. Med. 2019, 8, 678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alamanda, V.K.; Springer, B.D. The prevention of infection: 12 modifiable risk factors. Bone Jt. J. 2019, 101-B, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Lübbeke, A.; Zingg, M.; Vu, D.; Miozzari, H.H.; Christifilopoulos, P.; Uckay, I.; Harbarth, S.; Hoffmyer, P. Body mass and weight thresholds for increased prosthetic joint infection rates after primary total joint arthroplasty. Acta Orthop. 2016, 87, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Franklin, P.D.; Miozzari, H.; Christifilopopoulos, P.; Hoffmeyer, P.; Ayes, D.C.; Lübbeke, A. Important patient characteristics differ prior to total knee arthroplasty and total hip arthroplasty between Switzerland and the United States. BMC Musculoskelet. Disord. 2017, 18, 14. [Google Scholar] [CrossRef] [Green Version]
- Shohat, N.; Fleischman, A.; Tarabichi, M.; Tan, T.L.; Parvizi, J. Weighting in on Body Mass Index and Infection after Total Joint Arthroplasty: Is There Evidence for a Body Mass Index Threshold? Clin. Orthop. Relat. Res. 2018, 476, 1964–1969. [Google Scholar] [CrossRef]
- Zusmanovich, M.; Kester, B.S.; Schwarzkopf, R. Postoperative Complications of Total Joint Arthroplasty in Obese Patients Stratified by BMI. J. Arthroplas. 2018, 33, 856–864. [Google Scholar] [CrossRef]
- Theil, C.; Schmidt-Braekling, T.; Gosheger, G.; Thuener, B.; Moellenbeck, B.; Roeder, J.; Andreou, D.; Schwarze, J.; Dieckmann, R. Acceptable mid- to long-term survival rates and functional outcomes following a single design rotating hinge total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 28, 1868–1875. [Google Scholar] [CrossRef]
- Theil, C.; Schmidt-Braekling, T.; Gosheger, G.; Idelevich, E.A.; Moellenbeck, B.; Dieckmann, R. Fungal prosthetic joint infection in total hip or knee arthroplasty: A retrospective single-centre study of 26 cases. Bone Jt. J. 2019, 101-B, 589–595. [Google Scholar] [CrossRef]
- Weitz, J.L.; Eikelboom, J.W.; Samama, M.M. New antithrombotic drugs: Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2012, 141, e120S–e151S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akgün, D.; Müller, M.; Perka, C.; Winkler, T. The serum level of C-reactive protein alone cannot be used for the diagnosis of prosthetic joint infections, especially in those caused by organisms of low virulence. Bone Jt. J. 2018, 100-B, 1482–1486. [Google Scholar]
- Majors, I.; Jagadale, V.S. Serum interleukin 6 could be a valuable initial diagnostic tool in prosthetic knee joint infections. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1781–1788. [Google Scholar] [CrossRef]
- Mühlhofer, H.; Renz, N.; Zahar, A.; Lüdemann, M.; Rudert, M.; Hube, R.; Frommelt, L.; Ascherl, R.; Perka, C.; von Eisenhart-Rothe, E. Diagnosis of periprosthetic joint infection: Development of an evidence-based algorithm by the work of implant-associated infection of the AE-(German Society for Arthroplasty). Orthopade 2020. [Google Scholar] [CrossRef]
- Marson, B.A.; Deskmukh, S.R.; Grindlay, D.J.C.; Scammell, B.E. Alpha-defensin and the Synovasure lateral flow device for the diagnosis of prosthetic joint infection: A systematic review and meta-analysis. Bone Jt. J. 2018, 100-B, 703–711. [Google Scholar] [CrossRef]
- Hassebrock, J.D.; Fox, M.G.; Spangehl, M.J.; Neville, M.R.; Schwartz, A.J. What Is the Role of Repeat Aspiration in the Diagnosis of Periprosthetic Hip Infection? J. Arthroplast. 2019, 34, 126–131. [Google Scholar] [CrossRef]
- Signore, A.; Sconfienza, L.M.; Borens, O.; Glaudemans, A.W.J.M.; Cassar-Pullicino, V.; Trampuz, A.; Winkler, H.; Gheysens, O.; Vanhoenacker, F.M.H.M.; Petrosillo, N.; et al. Consensus document for the diagnosis of prosthetic joint infections: A joint paper by the EANM, EBJIS, and ESR (with ESCMID endorsement). Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 971–988. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| PJI (n = 52) | Non-PJI (n = 67) | p Value | |
|---|---|---|---|
| Mean age * (year) | 70.5 (60.05–83.7) | 68.0 (61.0–76.0) | 0.499 |
| Patients with Primary TJA | 27 (51.9%) | 29 (43.3%) | 0.226 |
| Patients with Revision TJA | 25 (48.1%) | 38 (56.7%) | 0.362 |
| Patients sex * | |||
| Male | 30 (57.7%) | 39 (58.2%) | 0.699 |
| Female | 22 (42.3%) | 28 (41.8%) | |
| Mean BMI * (kg/m2) | 30.9 (27.0 to 38.4) | 28.4 (25.5 to 31.9) | 0.008 |
| Affected joint * | |||
| Knee | 30 (57.7%) | 41 (61.2%) | 0.711 |
| Hip | 22 (42.3) | 26 (38.8%) |
| Marker | Cut-off Used | Sensitivity (%) | Specificity (%) | PPV | NPV |
|---|---|---|---|---|---|
| D-dimer | 2750 ng/mL | 38 | 94 | 0.8333 | 0.6631 |
| D-dimer | 860 ng/mL | 92 | 39 | 0.5393 | 0.8667 |
| CRP | 1.2 mg/dL | 88 | 87 | 0.8364 | 0.9063 |
| Il-6 | 10.0 pg/mL | 76 | 92 | 0.8810 | 0.8261 |
| CRP/Il-6 | 1.2 mg/dL/10.0 pg/dL | 74 | 97 | 0.9474 | 0.8219 |
| CRP/D-dimer | 1.2 mg/dL/2750 ng/mL | 35 | 96 | 0.8571 | 0.6531 |
| Il-6/D-dimer | 10.0 pg/dL/2750 ng/mL | 33 | 97 | 0.8889 | 0.6451 |
| Author | Year | Sensitivity (%) | Specificity (%) | Used Cut-off Value [ng/mL] |
|---|---|---|---|---|
| Hu et al. [16] | 2020 | 87.50 | 89.19 | 955 |
| Qin et al. [17] | 2020 | 92.72 | 74.63 | 1170 |
| Li et al. [11] | 2019 | 64.5 | 65.0 | 1250 |
| Xu et al. [12] | 2019 | 68.29 | 50.70 | 1020 |
| Pannu et al. [18] | 2020 | 95.9 | 32.3 | 850 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ackmann, T.; Möllenbeck, B.; Gosheger, G.; Schwarze, J.; Schmidt-Braekling, T.; Schneider, K.N.; Frommer, A.; Dieckmann, R.; Theil, C. Comparing the Diagnostic Value of Serum D-Dimer to CRP and IL-6 in the Diagnosis of Chronic Prosthetic Joint Infection. J. Clin. Med. 2020, 9, 2917. https://doi.org/10.3390/jcm9092917
Ackmann T, Möllenbeck B, Gosheger G, Schwarze J, Schmidt-Braekling T, Schneider KN, Frommer A, Dieckmann R, Theil C. Comparing the Diagnostic Value of Serum D-Dimer to CRP and IL-6 in the Diagnosis of Chronic Prosthetic Joint Infection. Journal of Clinical Medicine. 2020; 9(9):2917. https://doi.org/10.3390/jcm9092917
Chicago/Turabian StyleAckmann, Thomas, Burkhard Möllenbeck, Georg Gosheger, Jan Schwarze, Tom Schmidt-Braekling, Kristian Nikolaus Schneider, Adrien Frommer, Ralf Dieckmann, and Christoph Theil. 2020. "Comparing the Diagnostic Value of Serum D-Dimer to CRP and IL-6 in the Diagnosis of Chronic Prosthetic Joint Infection" Journal of Clinical Medicine 9, no. 9: 2917. https://doi.org/10.3390/jcm9092917