Additional Value of 2-[18F]FDG PET/CT Comparing to MRI in Treatment Approach of Anal Cancer Patients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Patients
2.2. 2-[18F]FDG PET/CT
2.3. MRI
2.4. Therapeutic Approach
2.5. Standard of the Truth
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Imaging Results
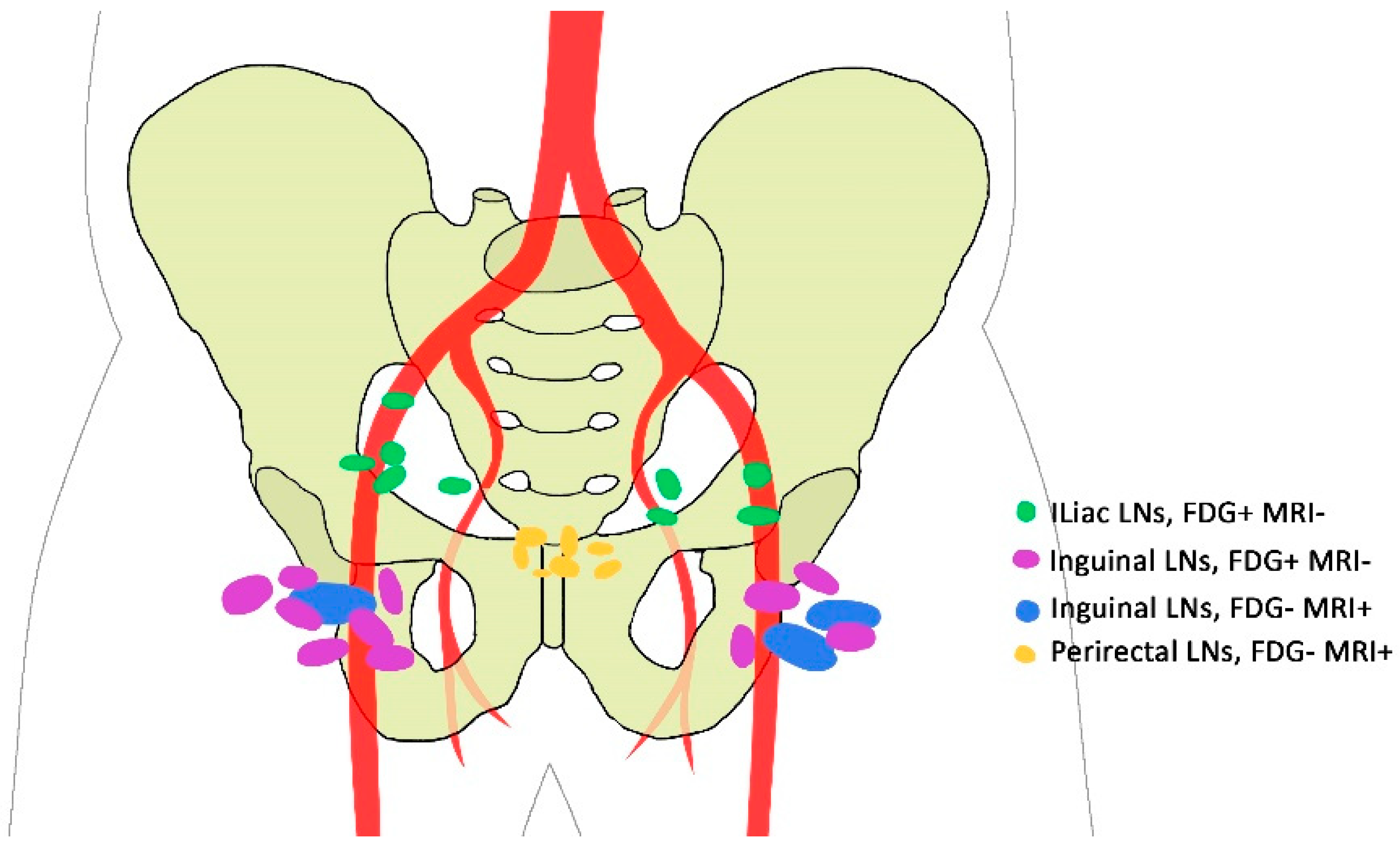
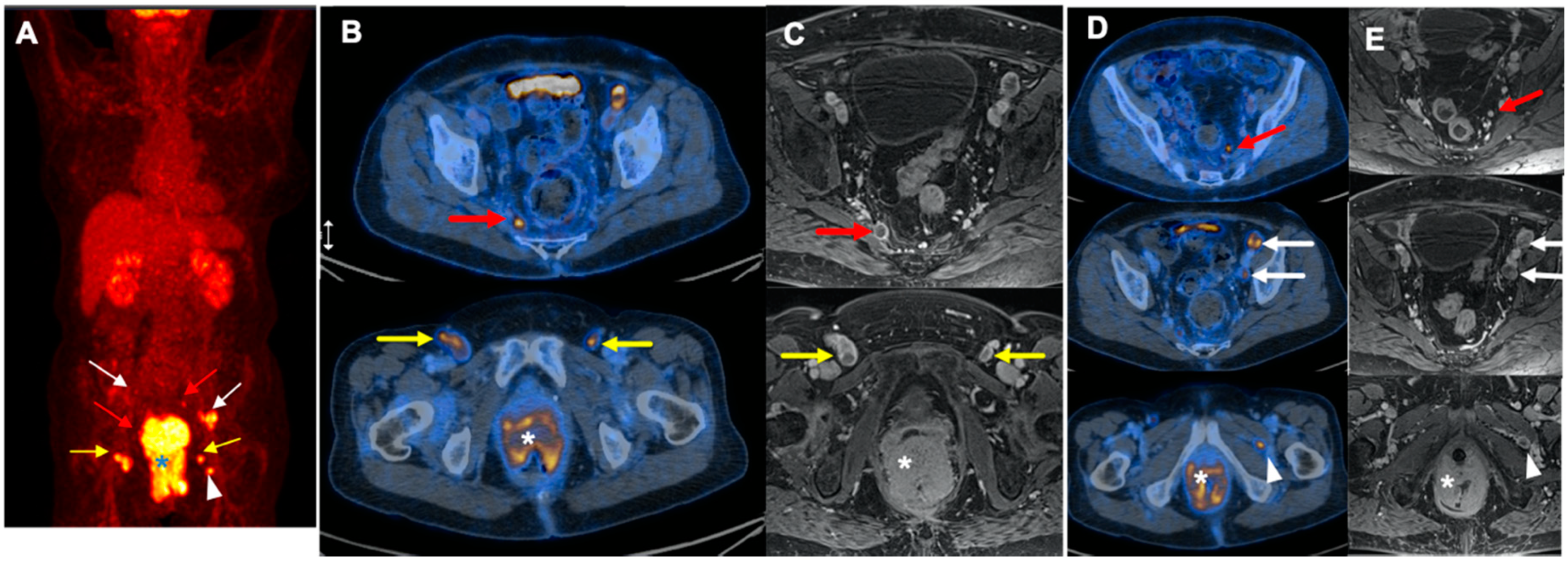
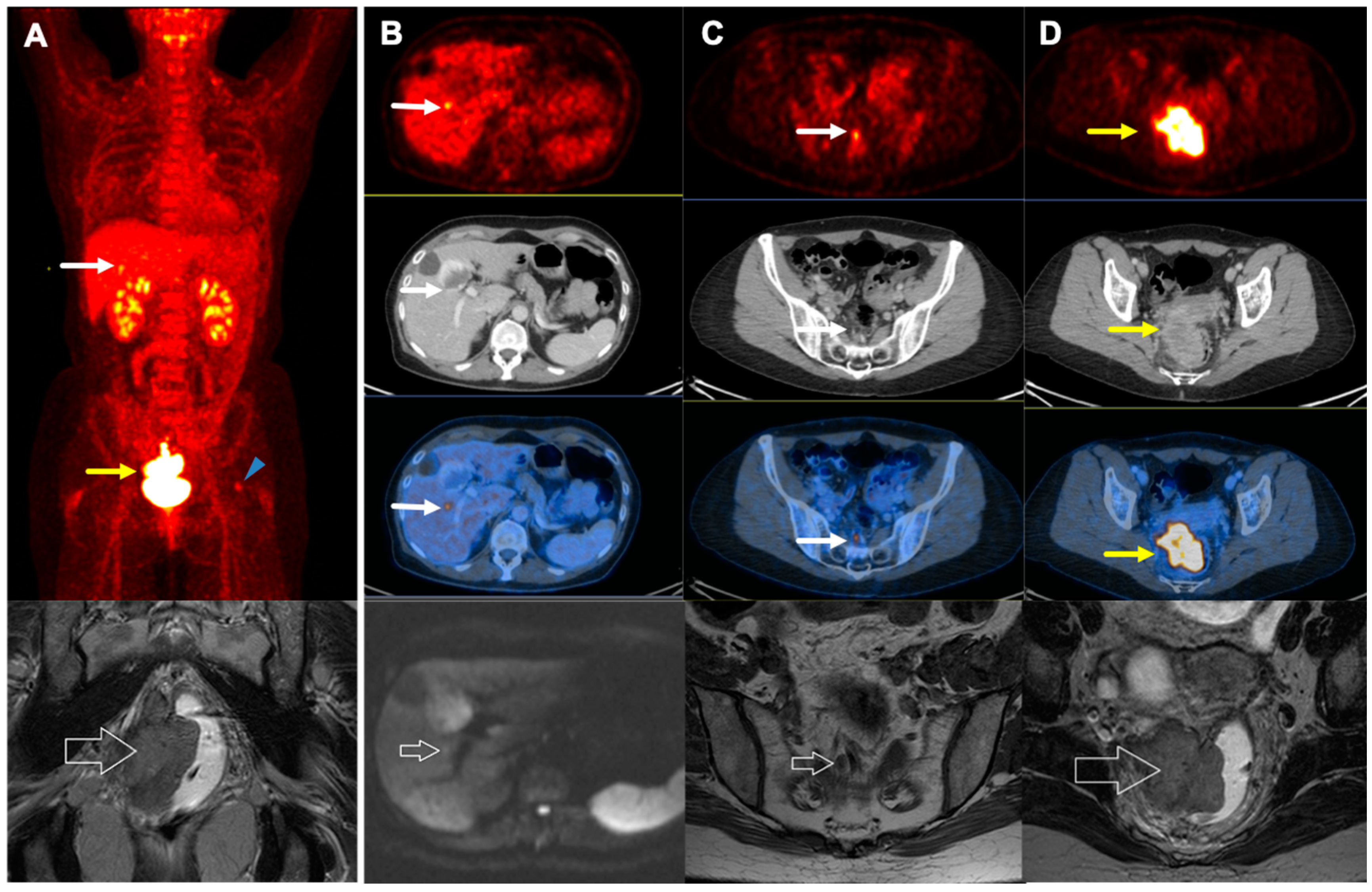
3.2. Discordant Findings
3.3. TNM Stage
3.4. Treatment Approach
3.5. Survival
4. Discussion
4.1. Additive Value of 2-[18F]FDG PET/CT in Staging
4.2. Additive Value of 2-[18F]FDG PET/CT in Treatment Approach
4.3. Value of 2-[18F]FDG PET/CT in Prognosis
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SEER Cancer Stat Facts: Anal Cancer. 2019. Available online: https://seer.cancer.gov/statfacts/html/anus.html (accessed on 25 September 2019).
- Johnson, L.G.; Madeleine, M.M.; Newcomer, L.M.; Schwartz, S.M.; Daling, J.R. Anal cancer incidence and survival: The surveillance, epidemiology, and end results experience, 1973–2000. Cancer 2004, 101, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Durot, C.; Dohan, A.; Boudiaf, M.; Servois, V.; Soyer, P.; Hoeffel, C. Cancer of the anal canal: Diagnosis, staging and follow-up with MRI. Korean J. Radiol. 2017, 18, 946–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldarella, C.; Annunziata, S.; Treglia, G.; Sadeghi, R.; Ayati, N.; Giovanella, L. Diagnostic performance of positron emission tomography/computed tomography using fluorine-18 fluorodeoxyglucose in detecting locoregional nodal involvement in patients with anal canal cancer: A systematic review and meta-analysis. Sci. World J. 2014, 2014, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.B.; Gaertner, W.B.; Glasgow, S.C.; Herzig, D.O.; Feingold, D.; Steele, S.R. The American Society of Colon and Rectal Surgeons clinical practice guidelines for anal squamous cell cancers (revised 2018). Dis. Colon Rectum 2018, 61, 755–774. [Google Scholar] [CrossRef] [PubMed]
- Mistrangelo, M.; Pelosi, E.; Bellò, M.; Ricardi, U.; Milanesi, E.; Cassoni, P.; Baccega, M.; Filippini, C.; Racca, P.; Lesca, A.; et al. Role of positron emission tomography-computed tomography in the management of anal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 66–72. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Reginelli, A.; Roberto, L.; Granata, F.; Rega, D.; Rotondo, A.; Grassi, R.; Izzo, F.; Petrillo, A. Radiological assessment of anal cancer: An overview and update. Infect. Agents Cancer 2016, 11, 52. [Google Scholar] [CrossRef] [Green Version]
- Glynne-Jones, R.; Nilsson, P.J.; Aschele, C.; Goh, V.; Peiffert, D.; Cervantes, A.; Arnold, D. Anal cancer: ESMO-ESSO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25 (Suppl. 3), iii10–iii20. [Google Scholar] [CrossRef]
- Corrigan, A.J.G.; Schleyer, P.J.; Cook, G.J. Pitfalls and artifacts in the use of PET/CT in oncology imaging. Semin. Nucl. Med. 2015, 45, 481–499. [Google Scholar] [CrossRef]
- Trautmann, T.G.; Zuger, J.H. Positron emission tomography for pretreatment staging and posttreatment evaluation in cancer of the anal canal. Mol. Imaging Biol. 2005, 7, 309–313. [Google Scholar] [CrossRef]
- Wells, I.; Fox, B. PET/CT in anal cancer—Is it worth doing? Clin. Radiol. 2012, 67, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Sveistrup, J.; Loft, A.; Berthelsen, A.K.; Henriksen, B.M.; Nielsen, M.B.; Engelholm, S.A. Positron emission tomography/computed tomography in the staging and treatment of anal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Bhuva, N.; Glynne-Jones, R.; Sonoda, L.; Wong, W.-L.; Harrison, M. To PET or not to PET? That is the question. Staging in anal cancer. Ann. Oncol. 2012, 23, 2078–2082. [Google Scholar] [CrossRef] [PubMed]
- Engledow, A.; Skipworth, J.; Blackman, G.; Groves, A.; Bomanji, J.; Warren, S.; Ell, P.; Boulos, P. The role of 18fluoro-deoxy glucose combined position emission and computed tomography in the clinical management of anal squamous cell carcinoma. Colorectal Dis. 2011, 13, 532–537. [Google Scholar] [CrossRef]
- De Winton, E.; Heriot, A.; Ng, M.; Hicks, R.; Hogg, A.; Milner, A.; Leong, T.; Fay, M.; MacKay, J.; Drummond, E. The impact of 18-fluorodeoxyglucose positron emission tomography on the staging, management and outcome of anal cancer. Br. J. Cancer 2009, 100, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Anal Carcinoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 852–871. [Google Scholar] [CrossRef] [Green Version]
- The Royal College Of Radiologists; College Of Physicians Of London Royal; College Of Physicians Royal. Royal College of Physicians of Edinburgh and Administration Of Radioactive Substances Advisory Committee. Evidence-based indications for the use of PET-CT in the United Kingdom 2016. Clin. Radiol. 2016, 71, 171–188. [Google Scholar]
- Klausner, G.; Blais, E.; Jumeau, R.; Biau, J.; de Meric de Bellefon, M.; Ozsahin, M.; Zilli, T.; Miralbell, R.; Thariat, J.; Troussier, I. Management of locally advanced anal canal carcinoma with intensity-modulated radiotherapy and concurrent chemotherapy. Med. Oncol. 2018, 35, 134. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Marcus, C.; Xiao, J.; Nene, P.; Kachnic, L.A.; Subramaniam, R.M. FDG PET/CT in the management of colorectal and anal cancers. Am. J. Roentgenol. 2014, 203, 1109–1119. [Google Scholar] [CrossRef]
- Zimmermann, M.; Beer, J.; Bodis, S.; von Moos, R.; Vlachopoulou, V.; Zwahlen, D.R.; Oehler, C. PET-CT guided SIB-IMRT combined with concurrent 5-FU/MMC for the treatment of anal cancer. Acta Oncol. 2017, 56, 1734–1740. [Google Scholar] [CrossRef] [Green Version]
- Yates, A.; Carroll, S.; Kneebone, A.; Tse, R.; Horvath, L.; Byrne, C.; Solomon, M.; Hruby, G. Implementing intensity-modulated radiotherapy with simultaneous integrated boost for anal cancer: 3 year outcomes at two Sydney institutions. Clin. Oncol. 2015, 27, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Albertsson, P.; Alverbratt, C.; Liljegren, A.; Björkander, E.; Strandell, A.; Samuelsson, O.; Palm, S.; Hallqvist, A. Positron emission tomography and computed tomographic (PET/CT) imaging for radiation therapy planning in anal cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 126, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, A.; Poon, R.; Jonker, D. PET imaging in anal canal cancer: A systematic review and meta-analysis. Br. J. Radiol. 2017, 90, 20170370. [Google Scholar] [CrossRef] [PubMed]
- Myerson, R.J.; Outlaw, E.D.; Chang, A.; Birnbaum, E.H.; Fleshman, J.W.; Grigsby, P.W.; Kodner, I.J.; Malayapa, R.S.; Mutch, M.G.; Parikh, P. Radiotherapy for epidermoid carcinoma of the anus: Thirty years’ experience. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 428–435. [Google Scholar] [CrossRef]
- Duimering, A.; Riauka, T.; Nijjar, Y.; Ghosh, S.; MacEwan, R.; Warkentin, H.; Schiller, D.; Tankel, K.; Usmani, N.; Severin, D.; et al. Prognostic utility of pre-and post-treatment FDG-PET parameters in anal squamous cell carcinoma. Radiother. Oncol. 2019, 136, 21–28. [Google Scholar] [CrossRef]
- Leccisotti, L.; Manfrida, S.; Barone, R.; Ripani, D.; Tagliaferri, L.; Masiello, V.; Privitera, V.; Gambacorta, M.A.; Rufini, V.; Valentini, V.; et al. The prognostic role of FDG PET/CT before combined radio-chemotherapy in anal cancer patients. Ann. Nucl. Med. 2020, 34, 65–73. [Google Scholar] [CrossRef]
- Rusten, E.; Rekstad, B.L.; Undseth, C.; Klotz, D.; Hernes, E.; Guren, M.G.; Malinen, E. Anal cancer chemoradiotherapy outcome prediction using (18)F-fluorodeoxyglucose positron emission tomography and clinicopathological factors. Br. J. Radiol. 2019, 92, 20181006. [Google Scholar] [CrossRef] [Green Version]
- Kidd, E.A.; Dehdashti, F.; Siegel, B.A.; Grigsby, P.W. Anal cancer maximum F-18 fluorodeoxyglucose uptake on positron emission tomography is correlated with prognosis. Radiother. Oncol. 2010, 95, 288–291. [Google Scholar] [CrossRef]
- Deantonio, L.; Milia, M.E.; Cena, T.; Sacchetti, G.; Perotti, C.; Brambilla, M.; Turri, L.; Krengli, M. Anal cancer FDG-PET standard uptake value: Correlation with tumor characteristics, treatment response and survival. La Radiol. Med. 2016, 121, 54–59. [Google Scholar] [CrossRef]
- Sadeghi, R.; Harsini, S.; Qodsi Rad, M.A.; Dabbagh, V.R.; Treglia, G. Prognostic Significance of Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography in Anal Squamous Cell Carcinoma: A Systematic Review and a Meta-Analysis. Contrast Media. Mol. Imaging 2018, 2018, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Jones, M.; Hruby, G.; Solomon, M.; Rutherford, N.; Martin, J. The role of FDG-PET in the initial staging and response assessment of anal cancer: A systematic review and meta-analysis. Ann. Surg. Oncol. 2015, 22, 3574–3581. [Google Scholar] [CrossRef] [PubMed]
- Rusten, E.; Rekstad, B.L.; Undseth, C.; Al-Haidari, G.; Hanekamp, B.; Hernes, E.; Hellebust, T.P.; Malinen, E.; Guren, M.G. Target volume delineation of anal cancer based on magnetic resonance imaging or positron emission tomography. Radiat. Oncol. 2017, 12, 147. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Cederquist, L.; Chan, E.; Chen, Y.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; Enzinger, P.C.; Fichera, A.; et al. NCCN Clinical Practice Guidelines in Oncology: Anal Carcinoma, Version 2. 2017. Available online: NCCN.org (accessed on 10 August 2018).
- Mistrangelo, M.; Pelosi, E.; Bellò, M.; Castellano, I.; Cassoni, P.; Ricardi, U.; Munoz, F.; Racca, P.; Contu, V.; Beltramo, G. Comparison of positron emission tomography scanning and sentinel node biopsy in the detection of inguinal node metastases in patients with anal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Dapper, H.; Schiller, K.; Münch, S.; Peeken, J.C.; Borm, K.; Weber, W.; Combs, S.E. Have we achieved adequate recommendations for target volume definitions in anal cancer? A PET imaging based patterns of failure analysis in the context of established contouring guidelines. BMC Cancer 2019, 19, 742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pernicka, J.S.G.; Sheedy, S.P.; Ernst, R.D.; Minsky, B.D.; Ganeshan, D.; Rauch, G.M. MR staging of anal cancer: What the radiologist needs to know. Abdom. Radiol. 2019, 44, 3726–3739. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.; Wang, Y.; Wang, L.; Chen, J.; Byanju, S.; Zhang, H.; Liao, M. Prognostic value of the maximum standardized uptake value of pre-treatment primary lesions in small-cell lung cancer on 18F-FDG PET/CT: A meta-analysis. Acta Radiol. 2018, 59, 1082–1090. [Google Scholar] [CrossRef]
- Diao, W.; Tian, F.; Jia, Z. The prognostic value of SUVmax measuring on primary lesion and ALN by 18F-FDG PET or PET/CT in patients with breast cancer. Eur. J. Radiol. 2018, 105, 1–7. [Google Scholar] [CrossRef]
- Jones, M.P.; Hruby, G.; Metser, U.; Sridharan, S.; Capp, A.; Kumar, M.; Gallagher, S.; Rutherford, N.; Holder, C.; Oldmeadow, C.; et al. FDG-PET parameters predict for recurrence in anal cancer—Results from a prospective, multicentre clinical trial. Radiat. Oncol. 2019, 14, 140. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, J.K.; Siegel, B.A.; Dehdashti, F.; Myerson, R.J.; Fleshman, J.W.; Grigsby, P.W. Tumor response and survival predicted by post-therapy FDG-PET/CT in anal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 180–186. [Google Scholar] [CrossRef]
- Cardenas, M.L.; Spencer, C.R.; Markovina, S.; DeWees, T.A.; Mazur, T.R.; Weiner, A.A.; Parikh, P.J.; Olsen, J.R. Quantitative FDG-PET/CT predicts local recurrence and survival for squamous cell carcinoma of the anus. Adv. Radiat. Oncol. 2017, 2, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Gauthé, M.; Richard-Molard, M.; Fayard, J.; Alberini, J.-L.; Cacheux, W.; Lièvre, A. Prognostic impact of tumour burden assessed by metabolic tumour volume on FDG PET/CT in anal canal cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Gerard, J.P.; Chapet, O.; Samiei, F.; Morignat, E.; Isaac, S.; Paulin, C.; Romestaing, P.; Favrel, V.; Mornex, F.; Bobin, J.Y. Management of inguinal lymph node metastases in patients with carcinoma of the anal canal: Experience in a series of 270 patients treated in Lyon and review of the literature. Cancer 2001, 92, 77–84. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Response to Treatment | 7/54 (12.9%) |
| Recurrence/Metastasis | 5/54 (9.3%) |
| Complete remission in the first 6 months after therapy | 35/54 (64.9%) |
| Complete remission in the 6–12 months after therapy | 7/54 (12.9%) |
| 2-[18F]FDG PET/CT | MRI | |||
|---|---|---|---|---|
| T | 0 | Recent surgical removal | 5 (9.3) | 5 (9.3) |
| 1 | ≤2 cm | 8 (14.8%) | 8 (14.8%) | |
| 2 | 2 cm < and ≤5 cm | 22 (40.7%) | 20 (37.0%) | |
| 3 | >5 cm | 6 (11.1%) | 6 (11.1%) | |
| 4 | Any size with invasion to adjacent organs | 13 (24.1%) | 15 (27.8%) | |
| N | 0 | No lymph node involvement | 28 (51.9%) | 28 (51.9%) |
| 1a | Involvement of inguinal, mesorectal and/or internal iliac lymph nodes | 18 (33.3%) | 23 (42.6%) | |
| 1b | Involvement of, external iliac lymph nodes | 1 (1.9%) | - | |
| 1c | Involvement of, external iliac and/or inguinal, mesorectal and/or internal iliac lymph nodes | 7 (12.9%) | 3 (5.5%) | |
| M | 0 | No distant metastasis | 52 (96.3%) | 53 (98.1%) |
| 1 | Distant metastasis | 2 (3.7%) | 1 (1.9%) | |
| Stage | I | T1N0M0 | 10 (18.5%) | 10 (18.5%) |
| IIA | T2N0M0 | 16 (29.6%) | 13 (24.1%) | |
| IIB | T3N0M0 | 1 (1.9%) | 3 (5.5%) | |
| IIIA | T1N1M0, T2N1M0 | 9 (16.6%) | 10 (18.5%) | |
| IIIB | T4N0M0 | 1 (1.9%) | 2 (3.7%) | |
| IIIC | T4N1M0, T3N1M0, T2N1M0 | 15 (27.8%) | 15 (27.8%) | |
| IV | Any T, Any N, M1 | 2 (3.7%) | 1 (1.9%) | |
| 2-[18F]FDG PET/CT | MRI | |||
|---|---|---|---|---|
| T | Size (mm) | mean | 45.9 ± 29.6 | 43.0 ± 26.2 |
| median | 40.0 | 35.0 | ||
| Interquartile range | 22–61 | 25–62 | ||
| range | 0.0 *–120.0 | 0.0 *–109.0 | ||
| SUVmax | mean | 12.1 ± 6.4 | - | |
| median | 10.7 | - | ||
| range | 0.0 *–35.9 | - | ||
| Invasion | 13 | 15 | ||
| N | Positive for Involvement | 26 (22 in both, 4 only on FDG) | 26 (22 in both, 4 only on MRI) | |
| Size (mm), the most prominent one | mean | 18.7 ± 7.4 | 15.5 ± 8.6 | |
| median | 18.0 | 15.0 | ||
| Interquartile range | 14.0–22.0 | 8.0–18.0 | ||
| range | 6.0–36.0 | 6.0–37.0 | ||
| SUVmax, the most prominent one | mean | 7.0 ± 5.3 | - | |
| median | 5.9 | - | ||
| range | 1.3–25.0 | - | ||
| M | Positive for Involvement | 2 | 1 | |
| Number (Percent) | Details | |||
|---|---|---|---|---|
| Additional data provided by 2-[18F]FDG PET/CT | N | Increase | 10/54 (18.5%) | 1 → One region: unilateral external iliac lymph nodes 2 → One region: unilateral inguinal lymph nodes 2 → Two regions: bilateral inguinal lymph nodes 1 → Two regions: bilateral external iliac lymph nodes 2 → Two regions: unilateral inguinal and unilateral external iliac lymph nodes 1 → Three regions: unilateral inguinal and iliac lymph nodes (bilateral external and unilateral internal) 1 → Four regions: bilateral inguinal and bilateral external iliac lymph nodes |
| Decrease | 2/54 (3.7%) | 1 → One region: unilateral Inguinal lymph nodes 1 → Two regions: bilateral Inguinal lymph nodes | ||
| M | Increase | 1/54 (1.9%) | 1 → Metastasis to liver | |
| Missing data on 2-[18F]FDG PET/CT | T | Increase | 2/54 (3.7%) | 2 → Larger on 2-[18F]FDG PET/CT |
| Decrease | 4/54 (7.5%) | 2 → Smaller on 2-[18F]FDG PET/CT 2 → Unable to detect invasion | ||
| N | Decrease | 7/54 (12.9%) | 7 → Perirectal lymph nodes |
| Number (Percent) | Details | ||
|---|---|---|---|
| True | Increase | 5/54 (9.3%) | 1 → Metastasis to liver 1 → Inguinal and iliac lymph nodes involvement 3 → Inguinal lymph nodes involvement |
| Decrease | 2/54 (3.7%) | 2 → Inguinal lymph nodes involvement | |
| False | Increase | 1/54 (1.9%) | 1 → Larger primary tumor size (T2→T1) |
| Decrease | 5/54 (9.3%) | 1 → Smaller primary tumor size (T2→T4) 2 → Unable to detect invasion to adjacent organs 2 → Perirectal lymph nodes involvement | |
| Number (Percent) | Details | ||
|---|---|---|---|
| True | Increase | 11/54 20.4 | 4 → Radiation field: inguinal regions 4 → Radiation field as well as dose: inguinal and iliac regions 2 → Radiation Dose: iliac lymph nodes 1 → Palliative therapy |
| Decrease | 2/54 (3.7%) | 2 → Radiation field: inguinal regions | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manafi-Farid, R.; Kupferthaler, A.; Wundsam, H.; Gruber, G.; Vali, R.; Venhoda, C.; Track, C.; Beheshti, A.; Langsteger, W.; Geinitz, H.; et al. Additional Value of 2-[18F]FDG PET/CT Comparing to MRI in Treatment Approach of Anal Cancer Patients. J. Clin. Med. 2020, 9, 2715. https://doi.org/10.3390/jcm9092715
Manafi-Farid R, Kupferthaler A, Wundsam H, Gruber G, Vali R, Venhoda C, Track C, Beheshti A, Langsteger W, Geinitz H, et al. Additional Value of 2-[18F]FDG PET/CT Comparing to MRI in Treatment Approach of Anal Cancer Patients. Journal of Clinical Medicine. 2020; 9(9):2715. https://doi.org/10.3390/jcm9092715
Chicago/Turabian StyleManafi-Farid, Reyhaneh, Alexander Kupferthaler, Helwig Wundsam, Georg Gruber, Reza Vali, Clemens Venhoda, Christine Track, Ali Beheshti, Werner Langsteger, Hans Geinitz, and et al. 2020. "Additional Value of 2-[18F]FDG PET/CT Comparing to MRI in Treatment Approach of Anal Cancer Patients" Journal of Clinical Medicine 9, no. 9: 2715. https://doi.org/10.3390/jcm9092715