Intra-Abdominal Nocardiosis—Case Report and Review of the Literature

 ,
,
Abstract
:1. Introduction
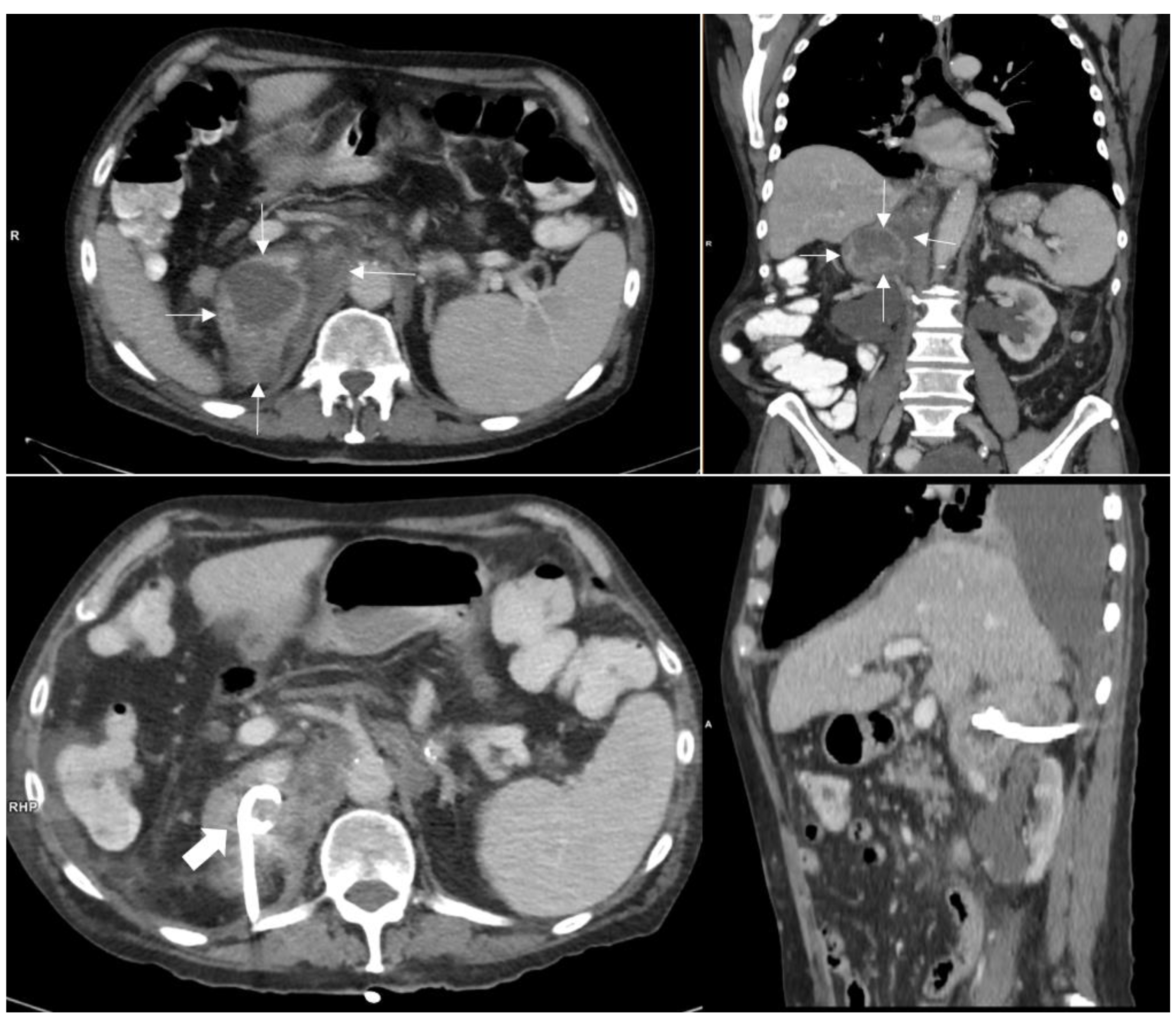
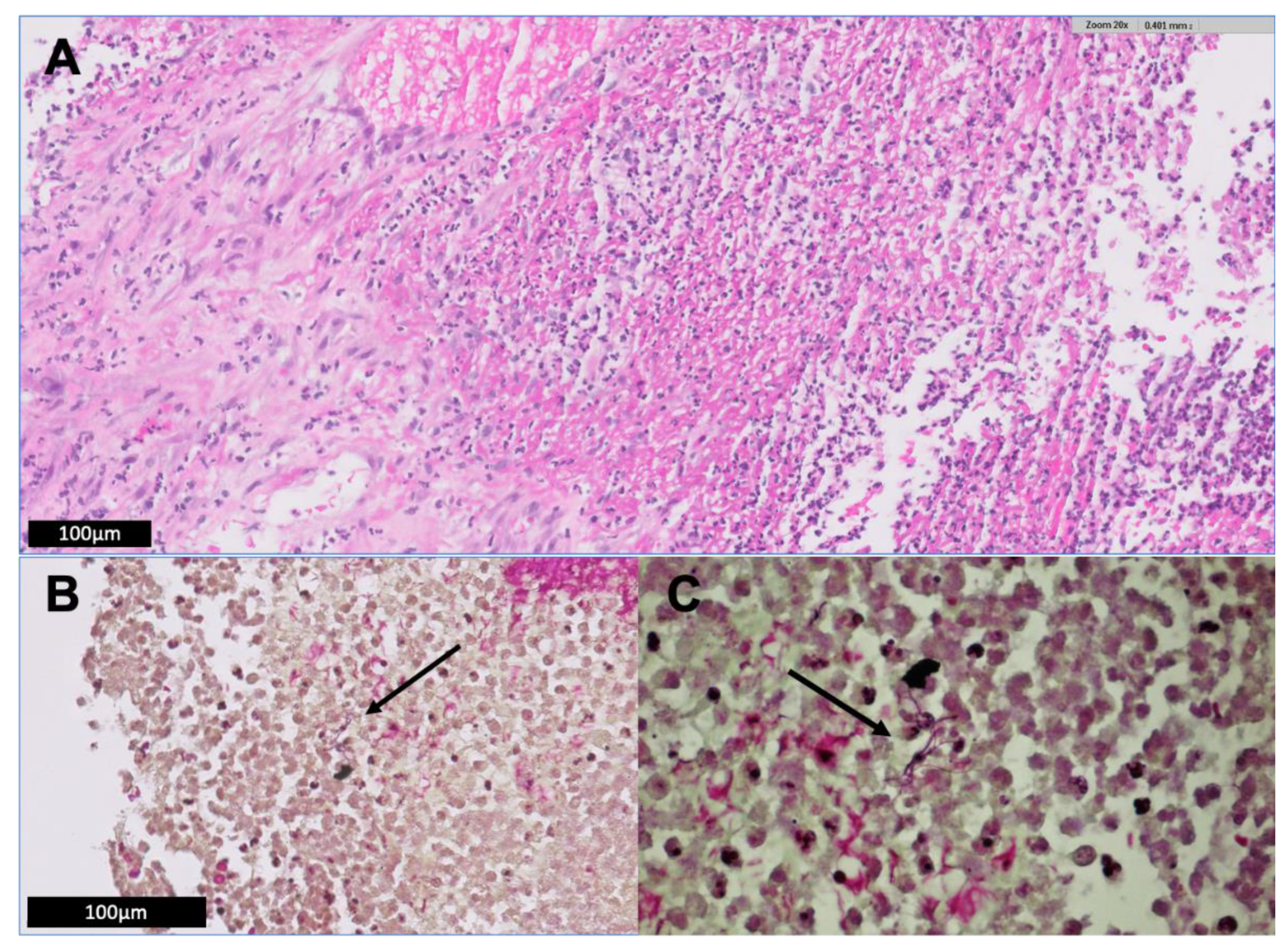
2. Illustrative Case Report
3. Methods
4. Literature Review and Discussion
4.1. Route of Nocardia acquisition
4.2. Infection Due to Nocardia Paucivorans
4.3. Abdominal/Retroperitoneal Infection Due to Nocardia Species
4.4. Peritoneal Dialysis-Related Nocardia Peritonitis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brown-Elliott, B.A.; Brown, J.M.; Conville, P.S.; Wallace, R.J., Jr. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin. Microbiol. Rev. 2006, 19, 259–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biswas Roy, S.; Ross, M.D.; Patil, P.D.; Trepeta, R.; Bremner, R.M.; Panchabhai, T.S. Primary Nocardia Infection Causing a Fluorodeoxyglucose-Avid Right Renal Mass in a Redo Lung Transplant Recipient. Case Rep. Transplant. 2018, 2018, 9752860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliaga, L.; Fatoul, G.; Guirao, E.; Pena, A.; Rodriguez-Granger, J.; Cobo, F. Nocardia paucivorans brain abscess. Clinical and microbiological characteristics. IDCases 2018, 13, e00422. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Tsuchiya, K.; Fujisawa, H. Nocardia paucivorans cerebellar abscess: Surgical and pharmacotherapy. Surg. Neurol. Int. 2019, 10, 22. [Google Scholar] [CrossRef]
- Chong, Y.L.; Green, J.A.; Toh, K.L.; Tan, J.K. Laparoscopic drainage of nocardial adrenal abscess in an HIV positive patient. Int. J. Urol. 2004, 11, 547–549. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Al-Khatti, A.A. Disseminated systemic Nocardia farcinica infection complicating alefacept and infliximab therapy in a patient with severe psoriasis. Int. J. Infect. Dis. 2010, 14, e153–e157. [Google Scholar] [CrossRef] [Green Version]
- Lerner, P.I. Nocardiosis. Clin. Infect. Dis. 1996, 22, 891–903; quiz 904–905. [Google Scholar] [CrossRef] [Green Version]
- Kendrick-Jones, J.; Ratanjee, S.K.; Taylor, S.L.; Marshall, M.R. Nocardia asteroides peritoneal dialysis-related peritonitis: A case of successful treatment and return to peritoneal dialysis. Nephrol. Dial. Transplant. 2008, 23, 2693–2694. [Google Scholar] [CrossRef]
- Lovett, I.S.; Houang, E.T.; Burge, S.; Turner-Warwick, M.; Thompson, F.D.; Harrison, A.R.; Joekes, A.M.; Parkinson, M.C. An outbreak of Nocardia asteroides infection in a renal transplant unit. Q. J. Med. 1981, 50, 123–135. [Google Scholar]
- Salfield, S.A.; Duerden, B.I.; Dickson, J.A.; Milner, R.D. Abdominal nocardiosis in a Sudanese girl. Eur. J. Pediatr. 1983, 140, 135–137. [Google Scholar] [CrossRef]
- Meier, B.; Metzger, U.; Muller, F.; Siegenthaler, W.; Luthy, R. Successful treatment of a pancreatic Nocardia asteroides abscess with amikacin and surgical drainage. Antimicrob. Agents Chemother. 1986, 29, 150–151. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Minamoto, G.Y.; Grieco, M.H. Nocardial infection as a complication of AIDS: Report of six cases and review. Rev. Infect. Dis. 1991, 13, 624–629. [Google Scholar] [CrossRef]
- Bocchetti, M.; Muzj, A.; Gargiulo, F.; Cipullo, P.; Amato, G. A case of abdominal aortic aneurysm infected by Nocardia asteroides. Biomed. Pharmacother. 1996, 50, 36. [Google Scholar] [CrossRef]
- Smit, L.H.; Leemans, R.; Overbeek, B.P. Nocardia farcinica as the causative agent in a primary psoas abscess in a previously healthy cattle inspector. Clin. Microbiol. Infect. 2003, 9, 445–448. [Google Scholar] [CrossRef] [Green Version]
- Saeed, S.; Varela, J.E.; Nelson, R.L.; Blend, M.J. An unusual case of intraabdominal nocardia abscess detected by Tc-99m HMPAO-labeled WBC study. Clin. Nucl. Med. 2004, 29, 270–271. [Google Scholar] [CrossRef]
- Cassar, C.L. Nocardia sepsis in a multigravida with systemic lupus erythematosus and autoimmune hepatitis. Anaesth. Intensive Care 2007, 35, 601–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chedid, M.B.; Chedid, M.F.; Porto, N.S.; Severo, C.B.; Severo, L.C. Nocardial infections: Report of 22 cases. Rev. Inst. Med. Trop. Sao Paulo 2007, 49, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pai, K.; Rao, L. Isolated renal nocardiosis in a patient with AIDS: Unusual presentation. Indian J. Urol. 2009, 25, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Patil, R.N.; Bafna, U.D.; Pallavi, V.R.; Rathod, P.S. Successful Intra-peritoneal Antibiotic Therapy for Primary Abdominal Nocardiosis in an Immunocompetent Young Female Masquerading as Carcinoma Ovary. Online J. Health Allied Sci. 2011, 10, 11. [Google Scholar]
- De Montmollin, E.; Corcos, O.; Noussair, L.; Leflon-Guibout, V.; Belmatoug, N.; Joly, F.; Lefort, A. Retroperitoneal abscesses due to Nocardia farcinica: Report of two cases in patients with malnutrition. Infection 2012, 40, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Kamyab, A.; Fakhoury, J.D.; Sutkowski, R.; Drelichman, E.; Jacobs, M.J. Fulminant colitis secondary to nocardiosis. Int. J. Colorectal. Dis. 2012, 27, 841–842. [Google Scholar] [CrossRef] [PubMed]
- Naha, K.; Dasari, S.; Vivek, G.; Prabhu, M. Primary abdominal nocardiosis masquerading as tubercular pelvic inflammatory disease in an immunocompetent individual. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Hanchanale, P.; Jain, M.; Varghese, J.; V, J.; Rela, M. Nocardia liver abscess post liver transplantation-A rare presentation. Transpl. Infect. Dis. 2017, 19, e12670. [Google Scholar] [CrossRef]
- David Turer, B.G.; Raghavendran, K. Fulminant Nocardia Colitis: A Case Report. Surgical Infect. Case Rep. 2016, 1, 69–71. [Google Scholar] [CrossRef]
- Singh, S.; Verma, Y.; Pandey, P.; Singh, U.B. Granulomatous hepatitis by Nocardia species: An unusual case. Int. J. Infect. Dis. 2019, 81, 97–99. [Google Scholar] [CrossRef] [Green Version]
- Acharya, R.; Amin, K.; Rajderkar, D.; Washam, M.; Pekkucuksen, N.; Mannemuddhu, S.; Upadhyay, K. Isolated abdominal nocardiosis in a pediatric renal transplant recipient. Pediatr. Transplant. 2019, 23, e13392. [Google Scholar] [CrossRef] [PubMed]
- Idriss, Z.H.; Cunningham, R.J.; Wilfert, C.M. Nocardiosis in children: Report of three cases and review of the literature. Pediatrics 1975, 55, 479–484. [Google Scholar] [PubMed]
- Chulay, J.D.; Lankerani, M.R. Splenic abscess. Report of 10 cases and review of the literature. Am. J. Med. 1976, 61, 513–522. [Google Scholar] [CrossRef]
- Sandre, R.M.; Summerbell, R.C. Disseminated Nocardia otitidiscaviarum in a patient with AIDS. Can. J. Infect. Dis. 1997, 8, 347–350. [Google Scholar] [CrossRef] [Green Version]
- Midiri, M.; Finazzo, M.; Bartolotta, T.V.; Maria, M.D. Nocardial adrenal abscess: CT and MR findings. Eur. Radiol. 1998, 8, 466–468. [Google Scholar] [CrossRef]
- Indumathi, V.A.; Shivakumar, A.N.S. Disseminated nocardiosis in an elderly patient presenting with prolonged pyrexia: Diagnosis by thyroid abscess culture. Indian J. Med. Microbiol. 2007, 25, 294–296. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Galanes Marchan, S.; Meneu Díaz, J.C.; Caso Maestro, O.; Perez Saborido, B.; Moreno Elola-Olaso, A.; Abradelo Usera, M.; Fundora Suarez, Y.; Gimeno Calvo, A.; Moreno Molinero, V.; Garcia Reyne, A. Disseminated nocardiosis: A rare infectious complication following Non-heart-beating donor liver transplantation. Transplant. Proc. 2009, 41, 2495–2497. [Google Scholar] [CrossRef]
- Arora, G.; Friedman, M.; Macdermott, R.P. Disseminated Nocardia nova infection. South Med. J. 2010, 103, 1269–1271. [Google Scholar] [CrossRef] [PubMed]
- John, M.A.; Madiba, T.E.; Mahabeer, P.; Naidoo, K.; Sturm, A.W. Disseminated nocardiosis masquerading as abdominal tuberculosis. S. Afr. J. Surg. 2004, 42, 17–19. [Google Scholar]
- Hu, Y.; Zheng, D.; Takizawa, K.; Mikami, Y.; Dai, L.; Yazawa, K.; Fukushima, K.; Lu, C.; Xi, L. Systemic nocardiosis caused by Nocardia concava in China. Med. Mycol. 2011, 49, 662–666. [Google Scholar] [PubMed] [Green Version]
- Xu, J.; Yachnis, A.T.; Malaty, I. An independent elderly woman with rapid onset of coma. JAMA Neurol. 2014, 71, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Piau, C.; Kerjouan, M.; Le Mouel, M.; Patrat-Delon, S.; Henaux, P.L.; Brun, V.; Morin, M.P.; Gautier, P.; Rodriguez-Nava, V.; Kayal, S. First case of disseminated infection with Nocardia cerradoensis in a human. J. Clin. Microbiol. 2015, 53, 1034–1037. [Google Scholar] [CrossRef] [Green Version]
- Lim, M.Y.; Alker, A.P.; Califano, S.; Trembath, D.G.; Alby, K.; Gilligan, P.H.; Jamieson, K.; Serody, J.S.; Shea, T.C. Concurrent Disseminated Nocardiosis and GI Mucormycosis in a Stem-Cell Transplantation Recipient. J. Clin. Oncol. 2016, 34, e84–e86. [Google Scholar] [CrossRef]
- Senard, O.; Blanot, S.; Jouvion, G.; Rodriguez-Nava, V.; Lortholary, O.; Join-Lambert, O.; Toubiana, J. Fulminant Nocardiosis Due to a Multidrug-Resistant Isolate in a 12-Year-Old Immunocompetent Child. Pediatrics 2018, 141, e20163131. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Huang, A.; Fang, Q. Disseminated nocardiosis caused by. Exp. Ther. Med. 2016, 12, 3339–3346. [Google Scholar] [CrossRef] [Green Version]
- Bonacini, M.; Walden, J.M. Nocardia brasiliensis peritonitis in a patient with AIDS. Am. J. Gastroenterol. 1990, 85, 1432–1433. [Google Scholar]
- Schlebusch, S.; Nimmo, G.; Carter, R. Bowel abscess with Nocardia veterana associated with colon carcinoma. Pathology 2010, 42, 306–307. [Google Scholar] [CrossRef] [PubMed]
- Arfania, D.; Everett, E.D.; Nolph, K.D.; Rubin, J. Uncommon causes of peritonitis in patients undergoing peritoneal dialysis. Arch. Intern. Med. 1981, 141, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.T.; Cheng, I.K.; Chan, P.C.; Mok, K.Y. Nocardia peritonitis complicating continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 1990, 10, 99. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarski, E.B.; Wilkie, M.; Thornhill, C.; Oppenheim, B.A.; Ackrill, P. Problems encountered in diagnosis of Nocardia asteroides peritonitis complicating CAPD. Perit. Dial. Int. 1990, 10, 106. [Google Scholar] [CrossRef]
- Lopes, J.O.; Alves, S.H.; Benevenga, J.P.; Salla, A.; Tatsch, I. Nocardia asteroides peritonitis during continuous ambulatory peritoneal dialysis. Rev. Inst. Med. Trop. Sao Paulo 1993, 35, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Recule, C.; Milongo, R.; Boiron, P.; Croize, J. Nocardia peritonitis complicating CAPD. Perit. Dial. Int. 1994, 14, 297–298. [Google Scholar]
- Dwyer, K.M. Nocardia peritonitis and abdominal abscess complicating continuous ambulatory peritoneal dialysis. Nephrology 2001, 263–265. [Google Scholar] [CrossRef]
- Chu, K.H.; Fung, K.S.; Tsang, W.K.; Chan, H.W.; Tong, K.L. Nocardia peritonitis: Satisfactory response to intraperitoneal trimethoprim-sulfamethoxazole. Perit. Dial. Int. 2003, 23, 197–198. [Google Scholar] [CrossRef]
- Ortiz, A.M.; Rabagliati, R.; Machuca, E. Successful treatment of Nocardia asteroides peritonitis in a patient undergoing automated peritoneal dialysis and receiving immunosuppressive therapy. Adv. Perit. Dial. 2005, 21, 66–68. [Google Scholar]
- Li, S.Y.; Yu, K.W.; Yang, W.C.; Chen, T.W.; Lin, C.C. Nocardia peritonitis—A case report and literature review. Perit. Dial. Int. 2008, 28, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Prasad, N.; Suresh, J.K.; Gupta, A.; Prasad, K.N.; Sharma, R.K. Nocardia asteroides peritonitis in peritoneal dialysis patients: Case report and review of the literature. Indian J. Nephrol. 2011, 21, 276–279. [Google Scholar] [CrossRef] [PubMed]
- El-Naggari, M.; El Nour, I.; Al-Nabhani, D.; Al Muharrmi, Z.; Gaafar, H.; Abdelmogheth, A.A. Nocardia asteroides peritoneal dialysis-related peritonitis: First case in pediatrics, treated with protracted linezolid. J. Infect. Public Health 2016, 9, 192–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosshard, P.P.; Abels, S.; Zbinden, R.; Böttger, E.C.; Altwegg, M. Ribosomal DNA sequencing for identification of aerobic gram-positive rods in the clinical laboratory (an 18-month evaluation). J. Clin. Microbiol. 2003, 41, 4134–4140. [Google Scholar] [CrossRef] [Green Version]
- Wayne, P. Performance Standards for Susceptibility Testing of Mycobacteria, Nocardia spp., and other Aerobic Actinomycetes, 1st ed.; CLSI supplement M62, ed.; Clinical and Laboratory Standards Institute: Wayne, NY, USA, 2018. [Google Scholar]
- Hammoud, M.; Kraft, C.; Pulst-Korenberg, J.; Chenoweth, C.; Gregg, K.S. Disseminated Nocardia paucivorans infection in an immunocompetent host. Infection 2014, 42, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Minero, M.V.; Marin, M.; Cercenado, E.; Rabadan, P.M.; Bouza, E.; Munoz, P. Nocardiosis at the turn of the century. Medicine (Baltimore) 2009, 88, 250–261. [Google Scholar] [CrossRef]
- Yassin, A.F.; Rainey, F.A.; Burghardt, J.; Brzezinka, H.; Mauch, M.; Schaal, K.P. Nocardia paucivorans sp. nov. Int. J. Syst. Evol. Microbiol. 2000, 50 Pt 2, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Wellinghausen, N.; Pietzcker, T.; Kern, W.V.; Essig, A.; Marre, R. Expanded spectrum of Nocardia species causing clinical nocardiosis detected by molecular methods. Int. J. Med. Microbiol. 2002, 292, 277–282. [Google Scholar] [CrossRef]
- Eisenblatter, M.; Disko, U.; Stoltenburg-Didinger, G.; Scherubl, H.; Schaal, K.P.; Roth, A.; Ignatius, R.; Zeitz, M.; Hahn, H.; Wagner, J. Isolation of Nocardia paucivorans from the cerebrospinal fluid of a patient with relapse of cerebral nocardiosis. J. Clin. Microbiol. 2002, 40, 3532–3534. [Google Scholar] [CrossRef] [Green Version]
- Wegerle, S.; Markus, A.; Weber, N.; Steffen, H.; King, B.; Eder, W.; Philipp, E.; Morresi-Hauff, A.; Haussinger, K.; Hoffmann, H. Pulmonary nocardiosis with trimethoprime/sulphamethoxazole-resistant Nocardia paucivorans in a patient with no signs of immunosuppression. Pneumologie 2007, 61, 46–51. [Google Scholar] [CrossRef]
- Khan, S.H.; Sanche, S.E.; Robinson, C.A.; Pirouzmand, F. N. paucivorans infection presenting as a brain abscess. Can. J. Neurol. Sci. 2006, 33, 426–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, T.J.; Serisier, D.J.; Gilpin, C.M.; Coulter, C.; Bowler, S.J.; McCormack, J.G. Nocardia paucivorans—A cause of disseminated nocardiosis. J. Infect. 2007, 54, e95–e98. [Google Scholar] [CrossRef] [PubMed]
- Monticelli, J.; Luzzati, R.; Maurel, C.; Rosin, C.; Valentinotti, R.; Farina, C. Brain Abscesses Caused by Nocardia paucivorans in a Multiple Myeloma Patient Treated with Lenalidomide and Dexamethasone: A Case Report and Review of Literature. Mediterr. J. Hematol. Infect. Dis. 2015, 7, e2015011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delavari, N.; Than, K.D.; Chen, K.S.; McKeever, P.E.; Wang, A.C.; Pandey, A.S. Resolution of innumerable cerebral Nocardia paucivorans abscesses after medical management. J. Clin. Neurosci. 2016, 27, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Rafiei, N.; Peri, A.M.; Righi, E.; Harris, P.; Paterson, D.L. Central nervous system nocardiosis in Queensland: A report of 20 cases and review of the literature. Medicine (Baltimore) 2016, 95, e5255. [Google Scholar] [CrossRef]
- Schiaroli, E.; Pasticci, M.B.; De Carolis, E.; Mello, E.; Pallotto, C.; Leli, C.; De Socio, G.V.; Baldelli, F.; Sanguinetti, M.; Mencacci, A. Diagnosis of Nocardia paucivorans central nervous system infection by DNA sequencing from paraffin-embedded tissue. Infez. Med. 2016, 24, 147–152. [Google Scholar]
- Samuel, D.M.G.; Matta, M.; Podgore, J.K. Nocardia Paucivorans Empyema in a Patient with Suspected Silicosis. Am. J. Respir. Crit. Care Med. 2018, 2018, 197. [Google Scholar]
- Wilson, J.W. Nocardiosis: Updates and clinical overview. Mayo Clin. Proc. 2012, 87, 403–407. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Case n°/Reference | Year ** | Age | Sex | Site | Immune Status | Therapy Regimen | Therapy Duration | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 [58] | 2000 | 51 | M | Sputum | Chronic lung disease | NR | NR | NR |
| 2 [59] | 2002 | 40 | F | Brain abscess | NR | NR | NR | NR |
| 3 [60] | 2002 | 63 | M | Brain abscess | Low CD4+ count of unknown origin | Cef, Amp, Amk, Mer, Levo, Mino | >6 months | survived |
| 4 [61] | 2006 | 54 | M | Sputum, BAL, lung biopsy | Immunocompetent | TMP/SMX, A/clav, Cip | 6 months | NR |
| 5 [62] | 2006 | 63 | M | Brain abscess | Immunocompetent | Surgical resection, TMP/SMX | 3 months | survived |
| 6 [63] | 2007 | 52 | M | Lung abscess | NR | NR | NR | died |
| 7 [63] | 2007 | 55 | M | Brain abscess | NR | NR | NR | NR |
| 8 [63] | 2007 | NR | M | Pleural fluid | NR | NR | NR | NR |
| 9 [63] | 2007 | 44 | M | Mediastinal lymph node | NR | NR | NR | NR |
| 10 [63] | 2007 | 78 | F | Lung abscess | Chronic lung disease | NR | NR | NR |
| 11 [63] | 2007 | 50 | F | Sputum | NR | NR | NR | NR |
| 12 [63] | 2007 | 41 | M | Brain abscess | Hodgkin’s lymphoma | NR | NR | NR |
| 13 [63] | 2007 | 53 | M | Lung abscess | NR | NR | NR | NR |
| 14 [63] | 2007 | 58 | F | Brain abscess | Corticosteroid therapy | NR | NR | NR |
| 15 [63] | 2007 | 66 | F | Sputum | NR | NR | NR | NR |
| 16 [63] | 2007 | 54 | M | Endocarditis, brain abscess, | NR | NR | NR | NR |
| skin abscess | ||||||||
| 17 [63] | 2007 | 65 | F | Sputum | NR | NR | NR | NR |
| 18 [63] | 2007 | 72 | F | Lung abscess | Corticosteroid therapy | NR | NR | NR |
| 19 [63] | 2007 | 66 | M | Brain abscess | Immunosuppression * | NR | NR | NR |
| 20 [63] | 2007 | 74 | M | BAL fluid | NR | NR | NR | NR |
| 21 [63] | 2007 | NR | M | Sputum | NR | NR | NR | NR |
| 22 [63] | 2007 | 74 | M | Skin abscess | NR | NR | NR | NR |
| 23 [63] | 2007 | 57 | M | Brain abscess, pneumonia | NR | NR | NR | NR |
| 24 [63] | 2007 | 80 | M | Lung, skin | NR | NR | NR | NR |
| 25 [63] | 2007 | 62 | M | Skin | Immunocompetent | NR | NR | NR |
| 26 [63] | 2007 | 87 | M | Sputum | NR | NR | NR | NR |
| 27 [63] | 2007 | 77 | F | BAL fluid | Immunocompetent | NR | NR | NR |
| 28 [63] | 2007 | 50 | M | Sputum | Lung cancer | NR | NR | NR |
| 29 [63] | 2007 | 67 | M | Brain abscess | Diabetes mellitus | NR | NR | NR |
| 30 [63] | 2007 | 67 | M | Sputum | Immunocompetent | NR | NR | NR |
| 31 [63] | 2007 | 47 | F | Sputum | NR | NR | NR | NR |
| 32 [63] | 2007 | 66 | F | Sputum | Previous lung infection | NR | NR | NR |
| 33 [63] | 2007 | 46 | M | Sputum | Immunocompetent | NR | NR | NR |
| 34 [63] | 2007 | 79 | M | Pleural fluid | Corticosteroid therapy | NR | NR | NR |
| 35 [63] | 2007 | 76 | M | Pleural fluid | Immunocompetent | NR | NR | NR |
| 36 [63] | 2007 | 61 | M | Skin abscess | NR | NR | NR | NR |
| 37 [63] | 2007 | 60 | M | Blood | Chemotherapy | NR | NR | NR |
| 38 [63] | 2007 | 53 | M | BAL fluid and skin lesion | Smoking and other drug abuse, Hepatitis C | Tica/clav, Rox, TMP/SMX | 12 months | survived |
| 39 [56] | 2014 | 50 | M | M. iliopsoas, brain, lung, | Smoking and other drug abuse | TMP/SMX, Imi, Mox | 12 months | survived |
| mediastinal lymph nodes | ||||||||
| 40 [64] | 2015 | 70 | M | Brain abscesses | Multiple Myeloma under chemotherapy | TMP/SMX, Mer, Cip | 12 months | survived |
| 41 [65] | 2016 | 50 | M | Brain abscesses | Smoking and other drug abuse | TMP/SMX, Imi, Line, Mox | 12 months | survived |
| 42 [66] | 2016 | 80 | F | Brain and lung abscess | Immunocompetent | Surgical resection, TMP/SMX, Cef | 9 months | survived |
| 43 [66] | 2016 | 50 | M | Spinal cord, lung | Alcohol abuse | Surgical resection, TMP/SMX, Mer, Cef | 9 months | survived |
| 44 [66] | 2016 | 59 | M | Brain and lung abscess | Immunocompetent | TMP/SMX, Mer | 12 months | survived |
| 45 [67] | 2016 | 54 | M | Brain abscess | Immunocompetent | Cef, Met, Mer, Line, Imi, Van, Rif, TMP/SMX | 21 weeks | survived |
| 46 [3] | 2018 | 61 | M | Brain abscess | Myasthenia gravis, corticosteroid therapy | TMP/SMX, Cef, Met, Line, Levo | 11 months | survived |
| 47 [2] | 2018 | 66 | F | Renal abscess | Post Lung Transplantation | TMP/SMX, Imi | 9–12 months | survived |
| 48 [68] | 2018 | 42 | M | Lung empyema | Suspected silicosis | TMP/SMX | NR | survived |
| 49 [4] | 2019 | 52 | F | Brain abscess | Immunocompetent | Surgical resection, Cef, TMP/SMX, Levo | 13 months | survived |
| 50 [present report] | 81 | M | Abscess in right adrenal loge | B-Cell Lymphoma, Hypogammaglobulinemia | Surgical resection, A/clav, TMP/SMX, Amk, Cef, Mino, Cip | 6 months | survived |
| Case n°/Reference | Year ** | Age | Sex | Species | Site | Immune Status | Therapy Regimen | Therapy Duration | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 [28] | 1976 | 49 | F | NR | Spleen abscess | Immunocompetent | Sulfisoxazole | NR | survived |
| 2 [9] | 1981 | 26 | F | N. asteroides | Perirenal area * | Post renal transplant | Sulphatriad, fusidic acid | NR | survived |
| 3 [10] | 1983 | 11 | F | N. asteroides | Liver and kidney abscesses | Immunocompetent | Surgical resection, Amk, TMP/SMX, Sulphadimidine | 12 weeks | survived |
| 4 [11] | 1986 | 76 | M | N. asteroides | Pancreas abscess | Immunocompetent | Surgical resection, A/clav, Amk, Orn, TMP/SMX | NR | survived |
| 5 [41] | 1990 | 19 | M | N. brasiliensis | Cholecystitis and Peritonitis | AIDS | NR | 7 days | died |
| 6 [12] | 1991 | 38 | M | N. asteroides | Left suprarenal abscess | AIDS | Surgical resection | NR | died |
| 7 [13] | 1996 | 67 | M | N. asteroides | Abdominal aortic aneurysm | Immunocompetent | TMP/SMX, Amk | NR | survived |
| 8 [14] | 2003 | 42 | M | N. farcinica | Psoas abscess | Immunocompetent | TMP/SMX | 11 months | survived |
| 9 [15] | 2004 | 37 | F | NR | Abdominal abscess | M. Crohn | NR | NR | NR |
| 10 [5] | 2004 | 34 | M | N. asteroides | Left Adrenal abscess | AIDS | Surgical resection, TMP/SMX, Cef | NR | survived |
| 11 [16] | 2007 | 25 | F | NR | Bilateral kidney abscesses | Corticosteroids and Azathioprin for SLE | Methylprednisolone | NR | died |
| 12 [17] | 2007 | 44 | F | NR | Jejunum | Post liver transplant | Surgical resection, Imi, Van | NR | died |
| 13 [18] | 2009 | 55 | M | NR | Kidney abscess | AIDS | Surgical resection | NR | NR |
| 14 [42] | 2010 | 83 | F | N. veterana | Bowel abscess | Colon cancer | Surgical resection, Cef, Gen, Met, TMP/SMX | NR | survived |
| 15 [19] | 2011 | 32 | F | NR | Bilateral abscesses of ovaries and fallopian tubes, omentum | Immunocompetent | Surgical resection, Mino, TMP/SMX, Amk, Line, Cip | 6 Months | survived |
| 16 [20] | 2012 | 59 | F | N. farcinica | Right adrenal compartment | Chronic hepatitis C, post treatment for lymphoma | Amk, Cefu, TMP/SMX | 4 months | died |
| 17 [21] | 2012 | 54 | F | NR | Colon | Immunocompetent | Surgical resection, antibiotics not specified | NR | survived |
| 18 [22] | 2013 | 30 | F | NR | Left adnexal collection * | Immunocompetent | TMP/SMX, Amk | 6 months | survived |
| 19 [24] | 2016 | 58 | F | N. farcinica | Colon, blood | TNFa-antagonist for M. Crohn | Van, Met, Imi, Amk, TMP/SMX | 12 months | survived |
| 20 [23] | 2017 | 59 | M | N. farcinica | Liver abscess | Post liver transplant | TMP/SMX, Amk, Imi | NR | survived |
| 21 [2] | 2018 | 63 | F | N. paucivorans | Renal abscess | Post lung transplant | Surgical resection, Imi, TMP/SMX | 9–12 months | NR |
| 22 [25] | 2019 | 63 | M | N. farcinica | Liver (hepatitis) | Immunocompetent | TMP/SMX, Amk | 4 weeks | died |
| 23 [26] | 2019 | 11 | F | N. farcinica | Abdominal abscesses | Post renal transplant | TMP/SMX, Mer, Imi, Cila, Line | NR | NR |
| 24 [present report] | 81 | M | N. paucivorans | Right adrenal space | B-Cell Lymphoma, Hypogammaglobulinemia | Surgical resection, A/clav, TMP/SMX, Amk, Cef, Mino, Cip | 6 months | survived |
| Case n°/Reference | Year ** | Age | Sex | Species | Site | Immune Status | Therapy Regimen | Therapy Duration | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 [27] | 1975 | 13 | M | N. asteroides | Lungs, liver, pancreas, lymph nodes | Immunocompetent | Surgical resection, sulphadiazine, sulfisoxazole | 6 months | NR |
| 2 [29] | 1997 | 59 | M | N. otitidiscaviarum | Thoracoabdominal abscess, lung | HIV positive | Surgical drainage, TMP/SMX, Amk, Cefotaxime | NR | survived |
| 3 [30] | 1998 | 49 | F | N. asteroides | Left adrenal abscess, spleen, lung | chronic steroids for RA | Surgical resection | NR | survived |
| 4 [34] | 2004 | 32 | M | N. brasiliensis | Lung, intestines | AIDS | Surgical resection | NR | died |
| 5 [17] | 2007 | 30 | M | N. asteroides | Lung, pleura, abdomen * | Post kidney transplant, chemotherapy, corticosteroids | NR | NR | survived |
| 6 [31] | 2007 | 67 | M | N. asteroides | Pancreas, omentum, brain, lungs, thyroid | Chronic steroids for Still’s disease | Mer, Amk, TMP/SMX | NR | died |
| 7 [32] | 2009 | 69 | M | N. farcinica | Adrenal glands, brain, lung, skin, muscle | Post liver transplant | TMP/SMX | 7 months | survived |
| 8 [6] | 2010 | 66 | F | N. farcinica | Brain, bilateral adrenal abscesses, abdominal lymph nodes | aTNF-therapy for Psoriasis | Van, Amp, Mer, Voriconazole, TMP/SMX, Line | 2.5 months | died |
| 9 [33] | 2010 | 61 | F | N. nova | Lung, skin, kidney, pancreas, brain | Chronic steroids and Azathioprine for ulcerative colitis | TMP/SMX | 1 year | survived |
| 10 [35] | 2011 | 42 | M | N. concava | Lung, liver | Chronic steroids for polychondritis | Sulphadiazine, Van, Imi, Cip, Amk | 25 days | died |
| 11 [20] | 2012 | 68 | F | N. farcinica | Right kidney abscess, brain abscess, lung | Anorexia nervosa | Cef, Erythromycin, TMP/SMX, Amk, Imi, Cip | 65 days | died |
| 12 [36] | 2014 | 75 | M | N. farcinica | Kidney, liver, spleen, lung, brain | Immunocompetent | Mer, Van, Cefepime, Doxycycline, Acilovir | 3 days | died |
| 13 [37] | 2015 | 59 | F | N. cerradoensis | Brain, skin, retroperitoneum, lung | Post renal transplant | Mer, Amk | 3 months | survived |
| 14 [40] | 2016 | 37 | M | N. otitidiscaviarum | Subcutaneous soft tissue, liver, lung | Immunocompetent | Cef, TMP/SMX, Mino | NR | survived |
| 15 [38] | 2016 | 58 | M | N. nova | Lung, ileum | B-cell Non-Hodgkin lymphoma | TMP/SMX, Imi | 11 months | died |
| 16 [39] | 2018 | 12 | M | N. elegans/aobensis/ africana complex | Kidney, lung, brain | Immunocompetent | Pip/Taz, Amk, Imi, Cip | 6 days | died |
| Case n°/Reference | Year ** | Age | Sex | Species | Cause of ESRD | Therapy Regimen | Therapy Duration | Outcome | Catheter Removal |
|---|---|---|---|---|---|---|---|---|---|
| 1 [43] | 1981 | 70 | M | N. asteroides | CIN | Ceph, Sulf | 6 weeks | survived | No |
| 2 [44] | 1990 | 60 | M | NR | PCKD | Ofl, Tob, Ceph, Van, Azt, TMP/SMX | 8 weeks | survived | No |
| 3 [45] | 1990 | 58 | F | N. asteroides | NR | Ceft, Net, Van, TMP/SMX | NR | survived | Yes |
| 4 [46] | 1993 | 38 | M | N. asteroides | SLE | Ceph, TMP/SMX | 4 weeks | died | No |
| 5 [47] | 1994 | 80 | M | N. nova | NR | TMP/SMX | 3 weeks | survived | Yes |
| 6 [48] | 2001 | 32 | M | N. nova | Type 1 DM | TMP/SMX, Imi | 4 months | survived | Yes |
| 7 [49] | 2003 | 68 | F | N. nova | Unknown | Cefa, Net, Ceft, Amk, Imi, TMP/SMX, Cef | 2 weeks | died | No |
| 8 [50] | 2005 | 35 | M | N. asteroides | CBUS | Van, Ceft, TMP/SMX, Amk, Cefu | 19 weeks | survived | No |
| 9 [51] | 2008 | 75 | M | NR | Type 2 DM | Van, TMP/SMX | 11 weeks | survived | Yes |
| 10 [8] | 2008 | 66 | M | N. asteroides | Type 2 DM | Cefa, Gen TMP/SMX | 12 months | survived | Yes |
| 11 [52] | 2011 | 57 | M | N. asteroides | Type 2 DM | Van, Ceft, TMP/SMX, Cef, Cip | 2 weeks | died | Yes |
| 12 [53] | 2016 | 13 | F | N. asteroides | DGS | Van, Cip, Ceft, Line | 8 months | survived | Yes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tramèr, L.; Mertz, K.D.; Huegli, R.; Hinic, V.; Jost, L.; Burkhalter, F.; Wirz, S.; Tarr, P.E. Intra-Abdominal Nocardiosis—Case Report and Review of the Literature. J. Clin. Med. 2020, 9, 2141. https://doi.org/10.3390/jcm9072141
Tramèr L, Mertz KD, Huegli R, Hinic V, Jost L, Burkhalter F, Wirz S, Tarr PE. Intra-Abdominal Nocardiosis—Case Report and Review of the Literature. Journal of Clinical Medicine. 2020; 9(7):2141. https://doi.org/10.3390/jcm9072141
Chicago/Turabian StyleTramèr, Lucas, Kirsten D. Mertz, Rolf Huegli, Vladimira Hinic, Lorenz Jost, Felix Burkhalter, Sebastian Wirz, and Philip E. Tarr. 2020. "Intra-Abdominal Nocardiosis—Case Report and Review of the Literature" Journal of Clinical Medicine 9, no. 7: 2141. https://doi.org/10.3390/jcm9072141