Early Predictors of Employment Status One Year Post Injury in Individuals with Traumatic Brain Injury in Europe

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Instruments and Variables
2.3. Ethical Approval
2.4. Statistical Analyses
3. Results
3.1. Participants
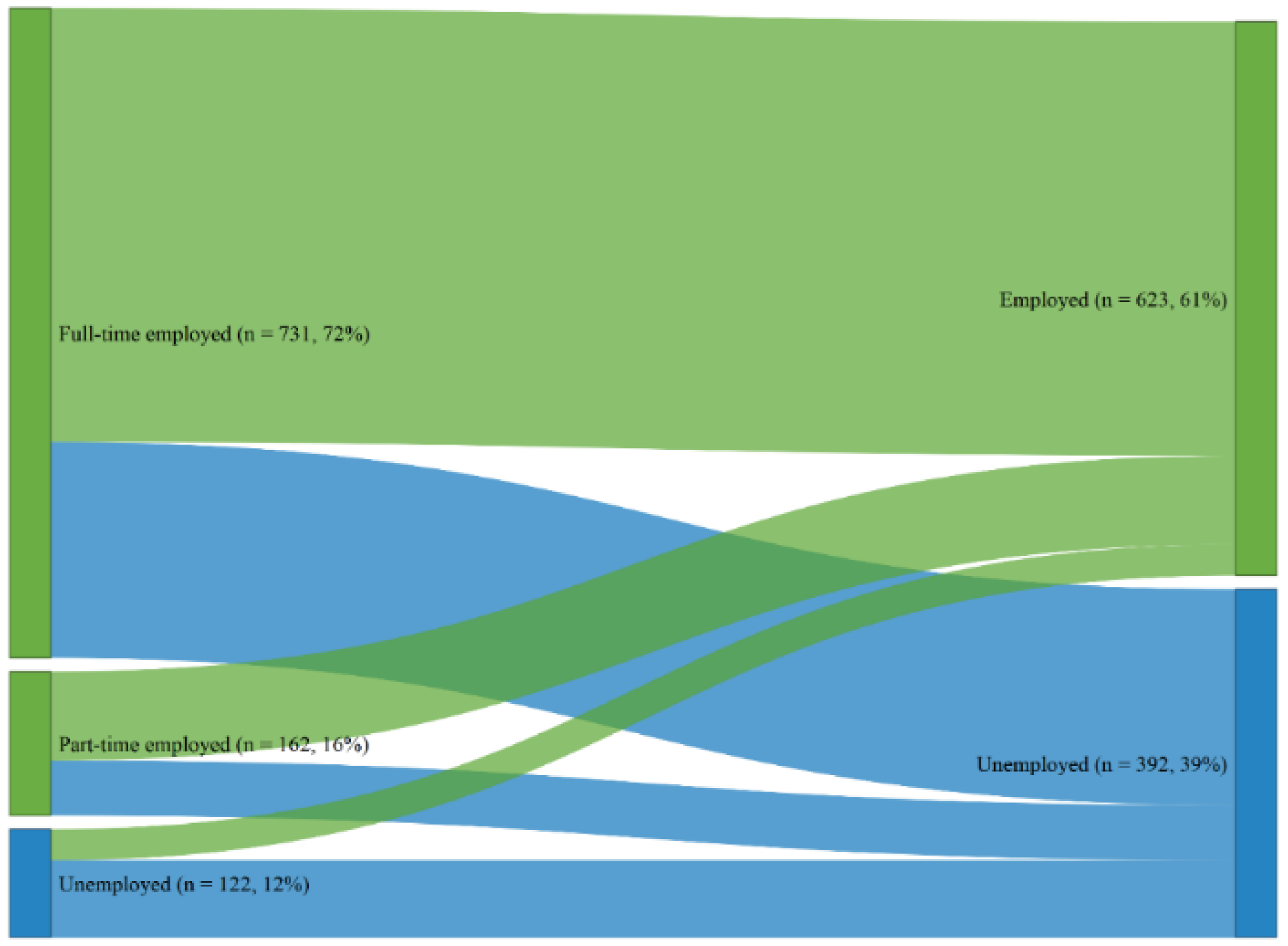
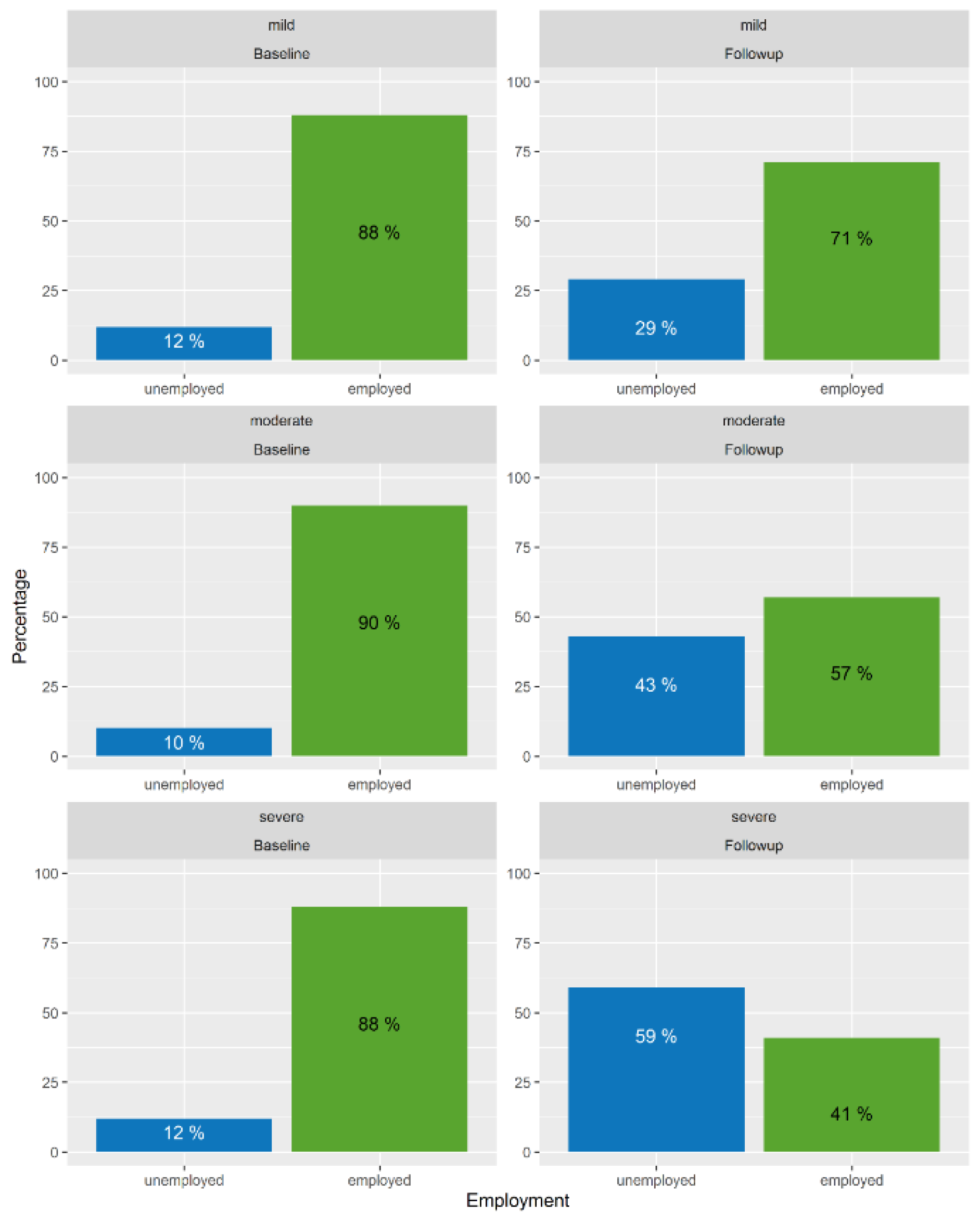
3.2. Employment Status
3.3. Model Estimation and Stepwise AIC Procedure
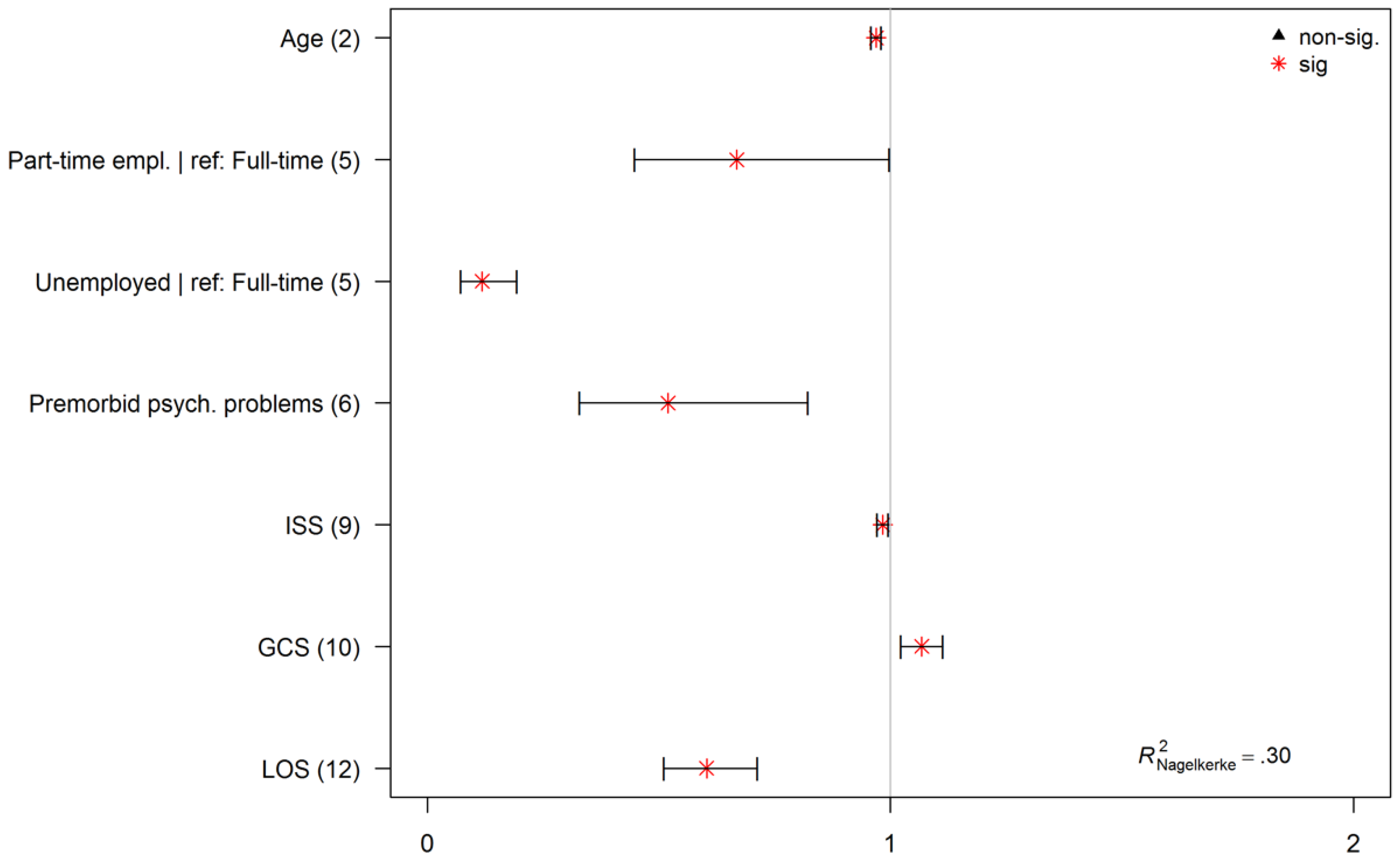
3.4. Final Model
4. Discussion
4.1. Limitations and Strengths
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [Green Version]
- Rubiano, A.M.; Carney, N.; Chesnut, R.; Puyana, J.C. Global neurotrauma research challenges and opportunities. Nature 2015, 527, S193–S197. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andelic, N.; Arango-Lasprilla, J.C.; Perrin, P.B.; Sigurdardottir, S.; Lu, J.; Olabarrieta-Landa, L.; Forslund, M.V.; Roe, C. Modeling of Community Integration Trajectories in the First Five Years after Traumatic Brain Injury. J. Neurotrauma 2016, 33, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Soberg, H.; Roe, C.; Anke, A.; Arango-Lasprilla, J.; Skandsen, T.; Sveen, U.; Steinbüchel, N.; Andelic, N. Health-related Quality of Life 12 months after severe traumatic brain injury: A prospective nationwide cohort study. J. Rehabil. Med. 2013, 45, 785–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gormley, M.; Devanaboyina, M.; Andelic, N.; Røe, C.; Seel, R.T.; Lu, J. Long-term employment outcomes following moderate to severe traumatic brain injury: A systematic review and meta-analysis. Brain Inj. 2019, 33. [Google Scholar] [CrossRef] [PubMed]
- Jourdan, C.; Bosserelle, V.; Azerad, S.; Ghout, I.; Bayen, E.; Aegerter, P.; Weiss, J.J.; Mateo, J.; Lescot, T.; Vigué, B.; et al. Predictive factors for 1-year outcome of a cohort of patients with severe traumatic brain injury (TBI): Results from the PariS-TBI study. Brain Inj. 2013, 27, 1000–1007. [Google Scholar] [CrossRef]
- Scaratti, C.; Leonardi, M.; Sattin, D.; Schiavolin, S.; Willems, M.; Raggi, A. Work-related difficulties in patients with traumatic brain injury: A systematic review on predictors and associated factors. Disabil. Rehabil. 2016, 39, 847–855. [Google Scholar] [CrossRef]
- Arango-Lasprilla, J.C.; Ketchum, J.M.; Lewis, A.N.; Krch, D.; Gary, K.W.; Dodd, B.A. Racial and Ethnic Disparities in Employment Outcomes for Persons With Traumatic Brain Injury: A Longitudinal Investigation 1-5 Years After Injury. Arch. Phys. Med. Rehabil. 2011, 3, 1083–1091. [Google Scholar] [CrossRef]
- Donker-Cools, B.H.P.M.; Wind, H.; Frings-Dresen, M.H.W. Prognostic factors of return to work after traumatic or non-traumatic acquired brain injury. Disabil. Rehabil. 2015, 38, 733–741. [Google Scholar] [CrossRef]
- Hofgren, C.; Esbjörnsson, E.; Sunnerhagen, K.S. Return to work after acquired brain injury: Facilitators and hindrances observed in a sub-acute rehabilitation setting. Work 2010, 36, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Saltychev, M.; Eskola, M.; Tenovuo, O.; Laimi, K. Return to work after traumatic brain injury: Systematic review. Brain Inj. 2013, 27, 1516–1527. [Google Scholar] [CrossRef] [PubMed]
- Schönberger, M.; Ponsford, J.; Olver, J.; Ponsford, M.; Wirtz, M. Prediction of functional and employment outcome 1 year after traumatic brain injury: A structural equation modelling approach. J. Neurol. Neurosurg. Psychiatry 2011, 82, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Sigurdardottir, S.; Andelic, N.; Wehling, E.; Anke, A.; Skandsen, T.; Holthe, O.O.; Manskow, U.S.; Roe, C. Return to work after severe traumatic brain injury: A national study with a one-year follow-up of neurocognitive and behavioural outcomes. Neuropsychol. Rehabil. 2018, 1–17. [Google Scholar] [CrossRef]
- Howe, E.I.; Andelic, N.; Perrin, P.B.; Røe, C.; Sigurdardottir, S.; Arango-Lasprilla, J.C.; Lu, J.; Løvstad, M.; Forslund, M.V. Employment Probability Trajectories Up To 10 Years After Moderate-To-Severe Traumatic Brain Injury. Front. Neurol. 2018, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hart, T.; Ketchum, J.M.; O’Neil-Pirozzi, T.M.; Novack, T.A.; Johnson-Greene, D.; Dams-O’Connor, K. Neurocognitive status and return to work after moderate to severe traumatic brain injury. Rehabil. Psychol. 2019, 64, 435–444. [Google Scholar] [CrossRef] [PubMed]
- DiSanto, D.; Kumar, R.G.; Juengst, S.B.; Hart, T.; O’Neil-Pirozzi, T.M.; Zasler, N.D.; Novack, T.A.; Dillahunt-Aspillaga, C.; Graham, K.M.; Cotner, B.A.; et al. Employment Stability in the First 5 Years After Moderate-to-Severe Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2018, 100, 412–421. [Google Scholar] [CrossRef]
- Forslund, M.V.; Arango-Lasprilla, J.C.; Roe, C.; Perrin, P.B.; Sigurdardottir, S.; Andelic, N. Multi-level modelling of employment probability trajectories and employment stability at 1, 2 and 5 years after traumatic brain injury. Brain Inj. 2014, 28, 980–986. [Google Scholar] [CrossRef]
- Kreutzer, J.S.; Marwitz, J.H.; Walker, W.; Sander, A.; Sherer, M.; Bogner, J.; Fraser, R.; Bushnik, T. Moderating Factors in Return to Work and Job Stability After Traumatic Brain Injury. J. Head Trauma Rehabil. 2003, 18, 128–138. [Google Scholar] [CrossRef]
- Cuthbert, J.P.; Harrison-Felix, C.; Corrigan, J.D.; Bell, J.M.; Haarbauer-Krupa, J.K.; Miller, A.C. Unemployment in the United States After Traumatic Brain Injury for Working-Age Individuals: Prevalence and Associated Factors 2 Years Postinjury. J. Head Trauma Rehabil. 2015, 30, 160–174. [Google Scholar] [CrossRef]
- Ketchum, J.M.; Almaz Getachew, M.; Krch, D.; Baños, J.H.; Kolakowsky-Hayner, S.A.; Lequerica, A.; Jamison, L.; Arango-Lasprilla, J.C. Early predictors of employment outcomes 1 year post traumatic brain injury in a population of Hispanic individuals. NeuroRehabilitation 2012, 30, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.K.; Hammond, F.M.; Sasser, H.C.; Wiercisiewski, D. Return to productive activity after traumatic brain injury: Relationship with measures of disability, handicap, and community integration. Arch. Phys. Med. Rehabil. 2002, 83, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Grauwmeijer, E.; Heijenbrok-Kal, M.H.; Haitsma, I.K.; Ribbers, G.M. Employment Outcome Ten Years after Moderate to Severe Traumatic Brain Injury: A Prospective Cohort Study. J. Neurotrauma 2017, 34, 2575–2581. [Google Scholar] [CrossRef] [PubMed]
- Andelic, N.; Stevens, L.F.; Sigurdardottir, S.; Arango-Lasprilla, J.C.; Roe, C. Associations between disability and employment 1 year after traumatic brain injury in a working age population. Brain Inj. 2012, 26, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, J.P.; Pretz, C.R.; Bushnik, T.; Fraser, R.T.; Hart, T.; Kolakowsky-Hayner, S.A.; Malec, J.F.; O’Neil-Pirozzi, T.M.; Sherer, M. Ten-Year Employment Patterns of Working Age Individuals After Moderate to Severe Traumatic Brain Injury: A National Institute on Disability and Rehabilitation Research Traumatic Brain Injury Model Systems Study. Arch. Phys. Med. Rehabil. 2015, 96, 2128–2136. [Google Scholar] [CrossRef] [PubMed]
- Walker, W.C.; Marwitz, J.H.; Kreutzer, J.S.; Hart, T.; Novack, T.A. Occupational Categories and Return to Work After Traumatic Brain Injury: A Multicenter Study. Arch. Phys. Med. Rehabil. 2006, 87, 1576–1582. [Google Scholar] [CrossRef]
- Chien, D.-K.; Hwang, H.-F.; Lin, M.-R. Injury severity measures for predicting return-to-work after a traumatic brain injury. Accid. Anal. Prev. 2017, 98, 101–107. [Google Scholar] [CrossRef]
- Van Velzen, J.M.; van Bennekom, C.A.M.; Edelaar, M.J.A.; Sluiter, J.K.; Frings-Dresen, M.H.W. Prognostic factors of return to work after acquired brain injury: A systematic review. Brain Inj. 2009, 23, 385–395. [Google Scholar] [CrossRef]
- Willmott, C.; Ponsford, J.; Downing, M.; Carty, M. Frequency and Quality of Return to Study Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2014, 29, 248–256. [Google Scholar] [CrossRef]
- Van Velzen, J.M.; van Bennekom, C.A.M.; Edelaar, M.J.A.; Sluiter, J.K.; Frings-Dresen, M.H.W. How many people return to work after acquired brain injury?: A systematic review. Brain Inj. 2009, 23, 473–488. [Google Scholar] [CrossRef]
- Libeson, L.; Downing, M.; Ross, P.; Ponsford, J. The experience of return to work in individuals with traumatic brain injury (TBI): A qualitative study. Neuropsychol. Rehabil. 2018, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Forslund, M.; Roe, C.; Arango-Lasprilla, J.; Sigurdardottir, S.; Andelic, N. Impact of personal and environmental factors on employment outcome two years after moderate-to-severe traumatic brain injury. J. Rehabil. Med. 2013, 45, 801–807. [Google Scholar] [CrossRef] [Green Version]
- Klonoff, P.S.; Watt, L.M.; Dawson, L.K.; Henderson, S.W.; Gehrels, J.-A.; Wethe, J.V. Psychosocial outcomes 1–7 years after comprehensive milieu-oriented neurorehabilitation: The role of pre-injury status. Brain Inj. 2006, 20, 601–612. [Google Scholar] [CrossRef]
- Arango-Lasprilla, J.C.; Ketchum, J.M.; Williams, K.; Kreutzer, J.S.; Marquez de la Plata, C.D.; O’Neil-Pirozzi, T.M.; Wehman, P. Racial Differences in Employment Outcomes After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2008, 89, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Calvete Oliva, A. Estrategia de salud de la Unión Europea: Salud pública para las personas europeas. Rev. Esp. Salud Pública 2008, 82, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Romero, C.; Ortega-Díaz, M.I.; Ocaña-Riola, R.; Martín-Martín, J.J. Análisis de la eficiencia técnica en los hospitales del Sistema Nacional de Salud español. Gac. Sanit. 2017, 31, 108–115. [Google Scholar] [CrossRef]
- Majdan, M.; Plancikova, D.; Brazinova, A.; Rusnak, M.; Nieboer, D.; Feigin, V.; Maas, A. Epidemiology of traumatic brain injuries in Europe: A cross-sectional analysis. Lancet Public Health 2016, 1, e76–e83. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Steyerberg, E.W.; Citerio, G.; Lecky, F.; Manley, G.T.; Hill, S.; Legrand, V.; Sorgner, A. Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI): A Prospective Longitudinal Observational Study. Neurosurgery 2015, 76, 67–80. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; De Keyser, V.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: A European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 304, 81–84. [Google Scholar] [CrossRef]
- Gennarelli, T.A.; Wodzin, E. Abbreviated Injury Scale 2005: Update 2008; Association for the Advancement of Automative Medicine: Barrington, IL, USA, 2008. [Google Scholar]
- Rubin, D.B. (Ed.) Multiple Imputation for Nonresponse in Surveys; Wiley Series in Probability and Statistics; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1987. [Google Scholar]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Nagelkerke, N.J.D. A note on a general definition of the coefficient of determination. Biometrika 1991, 78, 691–692. [Google Scholar] [CrossRef]
- Melo, F. Area under the ROC Curve. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.-H., Yokota, H., Eds.; Springer New York: New York, NY, USA, 2013; pp. 38–39. [Google Scholar]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019.
- Heymas, M. Psfmi: Prediction Model Selection and Performance Evaluation in Multiple Imputed Datasets. R Package Version 0.2.0. Available online: https://cran.r-project.org/web/packages/psfmi/index.html (accessed on 31 March 2020).
- Benedictus, M.R.; Spikman, J.M.; van der Naalt, J. Cognitive and Behavioral Impairment in Traumatic Brain Injury Related to Outcome and Return to Work. Arch. Phys. Med. Rehabil. 2010, 91, 1436–1441. [Google Scholar] [CrossRef] [PubMed]
- Watkin, C.; Phillips, J.; Radford, K. What is a ‘return to work’ following traumatic brain injury? Analysis of work outcomes 12 months post TBI. Brain Inj. 2019, 34, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Radford, K.; Phillips, J.; Drummond, A.; Sach, T.; Walker, M.; Tyerman, A.; Haboubi, N.; Jones, T. Return to work after traumatic brain injury: Cohort comparison and economic evaluation. Brain Inj. 2013, 27, 507–520. [Google Scholar] [CrossRef]
- Nakase-Richardson, R.; Yablon, S.A.; Sherer, M. Prospective comparison of acute confusion severity with duration of post-traumatic amnesia in predicting employment outcome after traumatic brain injury. J. Neurol. Neurosurg. Amp Psychiatry 2007, 78, 872–876. [Google Scholar] [CrossRef] [Green Version]
- Johnstone, B.; Mount, D.; Schopp, L.H. Financial and vocational outcomes 1 year after traumatic brain injury. Arch. Phys. Med. Rehabil. 2003, 84, 238–241. [Google Scholar] [CrossRef]
- Ownsworth, T.; Desbois, J.; Grant, E.; Fleming, J.; Strong, J. The associations among self-awareness, emotional well-being, and employment outcome following acquired brain injury: A 12-month longitudinal study. Rehabil. Psychol. 2006, 51, 50–59. [Google Scholar] [CrossRef]
- Van Gyes, G.; Szekér, L. Impact of the Crisis on Working Conditions in Europe; Eurofound: Dublin, Ireland, 2013. [Google Scholar]
- European Disability Strategy 2010-2020: A Renewed Commitment to a Barrier-Free Europe; European Commission: Brussels, Belgium, 2010.
- Willemse-van Son, A.H.P.; Ribbers, G.M.; Verhagen, A.P.; Stam, H.J. Prognostic factors of long-term functioning and productivity after traumatic brain injury: A systematic review of prospective cohort studies. Clin. Rehabil. 2007, 21, 1024–1037. [Google Scholar] [CrossRef]
- Sherer, M.; Sander, A.M.; Nick, T.G.; High, W.M.; Malec, J.F.; Rosenthal, M. Early cognitive status and productivity outcome after traumatic brain injury: Findings from the TBI Model Systems. Arch. Phys. Med. Rehabil. 2002, 83, 183–192. [Google Scholar] [CrossRef]
- Konle-Seidl, R. Retention and Re-Integration of Older Workers into the Labour Market: What Works? Institut für Arbeitsmarkt- und Berufsforschung (IAB): Nürnberg, Germany, 2017. [Google Scholar]
- Machamer, J.; Temkin, N.; Fraser, R.; Doctor, J.N.; Dikmen, S. Stability of employment after traumatic brain injury. J. Int. Neuropsychol. Soc. 2005, 11, 807–816. [Google Scholar] [CrossRef]
- Fraser, R.; Machamer, J.; Temkin, N.; Dikmen, S.; Doctor, J. Return to work in traumatic brain injury (TBI): A perspective on capacity for job complexity. J. Vocat. Rehabil. 2006, 25, 141–148. [Google Scholar]
- Dahm, J.; Ponsford, J. Long-term employment outcomes following traumatic brain injury and orthopaedic trauma: A ten-year prospective study. J. Rehabil. Med. 2015, 47, 932–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrelfs, S.F.; Donker-Cools, B.H.P.M.; Wind, H.; Frings-Dresen, M.H.W. Return-to-work in patients with acquired brain injury and psychiatric disorders as a comorbidity: A systematic review. Brain Inj. 2015, 29, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.T.L.; Pettigrew, L.E.L.; Teasdale, G.M. Structured Interviews for the Glasgow Outcome Scale and the Extended Glasgow Outcome Scale: Guidelines for Their Use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Faul, M.; Wald, M.M.; Xu, L.; Coronado, V.G. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths, 2002–2006; US Department of Health and Human Services, CDC: Atlanta, GA, USA, 2010.
- Peeters, W.; van den Brande, R.; Polinder, S.; Brazinova, A.; Steyerberg, E.W.; Lingsma, H.F.; Maas, A.I.R. Epidemiology of traumatic brain injury in Europe. Acta Neurochir. (Wien) 2015, 157, 1683–1696. [Google Scholar] [CrossRef] [Green Version]
- Alves, D.E.; Nilsen, W.; Fure, S.C.R.; Enehaug, H.; Howe, E.I.; Løvstad, M.; Fink, L.; Andelic, N.; Spjelkavik, Ø. What characterises work and workplaces that retain their employees following acquired brain injury? Systematic review. Occup. Environ. Med. 2020, 77, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Reme, S.E.; Monstad, K.; Fyhn, T.; Sveinsdottir, V.; Løvvik, C.; Lie, S.A.; Øverland, S. A randomized controlled multicenter trial of individual placement and support for patients with moderate-to-severe mental illness. Scand. J. Work. Environ. Health 2019, 45, 33–41. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Original Data | Imputed Data d | |||||||
|---|---|---|---|---|---|---|---|---|
| No | Variable | Groups (Reference Group in Italic) or No. of Cases | N | % | M (SD) | N | % | M (SD) |
| (1) | Sex | female | 256 | 25.22% | - | - | - | - |
| male | 759 | 74.78% | - | - | - | - | ||
| NA | 0 | 0.00% | - | - | - | - | ||
| (2) | Age a | valid cases | 1015 | 100.00% | 44.20 (13.70) | - | - | - |
| NA | 0 | 0.00% | - | - | - | - | ||
| (3) | Marital state | partnered | 560 | 55.17% | - | - | - | - |
| single | 455 | 44.83% | - | - | - | - | ||
| NA | 0 | 0.00% | - | - | - | - | ||
| (4) | Education | post-high school | 496 | 48.87% | - | 535 | 52.71% | - |
| secondary/high school | 348 | 34.29% | - | 382 | 37.64% | - | ||
| none/primary school | 90 | 8.87% | - | 98 | 9.66% | - | ||
| NA | 81 | 7.98% | - | 0 | 0.00% | - | ||
| (5) | Employment baseline | full-time employed | 731 | 72.02% | - | - | - | - |
| part-time employed | 162 | 15.96% | - | - | - | - | ||
| not working | 122 | 12.02% | - | - | - | - | ||
| NA | 0 | 0.00% | - | - | - | - | ||
| (-) | Employment follow up | employed | 623 | 61.38% | - | - | - | - |
| not working | 392 | 38.62% | - | - | - | - | ||
| NA | 0 | 0.00% | - | - | - | - | ||
| (6) | Premorbid psychological/psychiatric problems | no | 881 | 86.80% | - | 891 | 87.78% | - |
| yes | 122 | 12.02% | - | 124 | 12.22% | - | ||
| NA | 12 | 1.18% | - | 0 | 0.00% | - | ||
| (7) | Injury cause | road traffic accident | 458 | 45.12% | - | 459 | 45.22% | - |
| fall | 365 | 35.96% | - | 366 | 36.06% | - | ||
| violent/other c | 190 | 18.72% | - | 190 | 18.72% | - | ||
| NA | 2 | 0.20% | - | 0 | 0.00% | - | ||
| (8) | Stratum | ward | 404 | 39.80% | - | - | - | - |
| ICU | 611 | 60.20% | - | - | - | - | ||
| NA | 0 | 0.00% | - | - | - | - | ||
| (9) | ISS score a | valid cases | 999 | 98.42% | 24.56 (15.79) | 1015 | 100.00% | 24.63 (15.81) |
| NA | 16 | 1.58% | - | 0 | 0.00% | - | ||
| (10) | GCS score a | valid cases | 977 | 96.26% | 11.63 (4.33) | 1015 | 100.00% | 11.61 (4.34) |
| NA | 38 | 3.74% | - | 0 | 0.00% | - | ||
| (-) | Injury severity b | mild | 611 | 60.20% | - | - | - | - |
| moderate | 115 | 11.33% | - | - | - | - | ||
| severe | 251 | 24.73% | - | - | - | - | ||
| NA | 38 | 3.74% | - | - | - | - | ||
| (11) | LOC | no | 237 | 23.35% | - | 272 | 26.80% | - |
| yes | 657 | 64.73% | - | 743 | 73.20% | - | ||
| NA | 121 | 11.92% | - | 0 | 0.00% | - | ||
| (12) | LOS a | valid cases | 994 | 97.93% | 16.94 (24.97) | 1015 | 100.00% | 16.92 (24.88) |
| NA | 21 | 2.07% | - | 0 | 0.00% | - | ||
| Total | 1015 | 100.00% | - | 1015 | 100.00% | - | ||
| No. | Variable/Category | Reference Group | Estimate | S.E. | p | Odds Ratios | CI2.5% | CI97.5% |
|---|---|---|---|---|---|---|---|---|
| (–) | Intercept | - | 3.09 | 0.46 | <0.001 | 22.004 | 8.9239 | 54.256 |
| (2) | Age | - | −0.03 | 0.01 | <0.001 | 0.97 | 0.96 | 0.98 |
| (5) | Part-time employed | Full-time employed | −0.40 | 0.20 | 0.048 | 0.67 | 0.45 | 1.00 |
| Not working | Full-time employed | −2.14 | 0.25 | <0.001 | 0.12 | 0.07 | 0.19 | |
| (6) | Premorbid psychiatric problems | No | −0.65 | 0.23 | 0.005 | 0.52 | 0.33 | 0.82 |
| (9) | ISS | - | −0.02 | 0.01 | 0.007 | 0.98 | 0.97 | 1.00 |
| (10) | GCS score | - | 0.06 | 0.02 | 0.003 | 1.07 | 1.02 | 1.11 |
| (12) | Length of stay (ln) | - | −0.51 | 0.09 | <.001 | 0.60 | 0.51 | 0.71 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arango-Lasprilla, J.C.; Zeldovich, M.; Olabarrieta-Landa, L.; Forslund, M.V.; Núñez-Fernández, S.; von Steinbuechel, N.; Howe, E.I.; Røe, C.; Andelic, N.; CENTER-TBI Participants and Investigators. Early Predictors of Employment Status One Year Post Injury in Individuals with Traumatic Brain Injury in Europe. J. Clin. Med. 2020, 9, 2007. https://doi.org/10.3390/jcm9062007
Arango-Lasprilla JC, Zeldovich M, Olabarrieta-Landa L, Forslund MV, Núñez-Fernández S, von Steinbuechel N, Howe EI, Røe C, Andelic N, CENTER-TBI Participants and Investigators. Early Predictors of Employment Status One Year Post Injury in Individuals with Traumatic Brain Injury in Europe. Journal of Clinical Medicine. 2020; 9(6):2007. https://doi.org/10.3390/jcm9062007
Chicago/Turabian StyleArango-Lasprilla, Juan Carlos, Marina Zeldovich, Laiene Olabarrieta-Landa, Marit Vindal Forslund, Silvia Núñez-Fernández, Nicole von Steinbuechel, Emilie Isager Howe, Cecilie Røe, Nada Andelic, and CENTER-TBI Participants and Investigators. 2020. "Early Predictors of Employment Status One Year Post Injury in Individuals with Traumatic Brain Injury in Europe" Journal of Clinical Medicine 9, no. 6: 2007. https://doi.org/10.3390/jcm9062007