Metastatic Tumors of the Oro-Facial Tissues: Clear Cell Renal Cell Carcinoma. A Clinico-Pathological and Immunohistochemical Study of Seven Cases

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
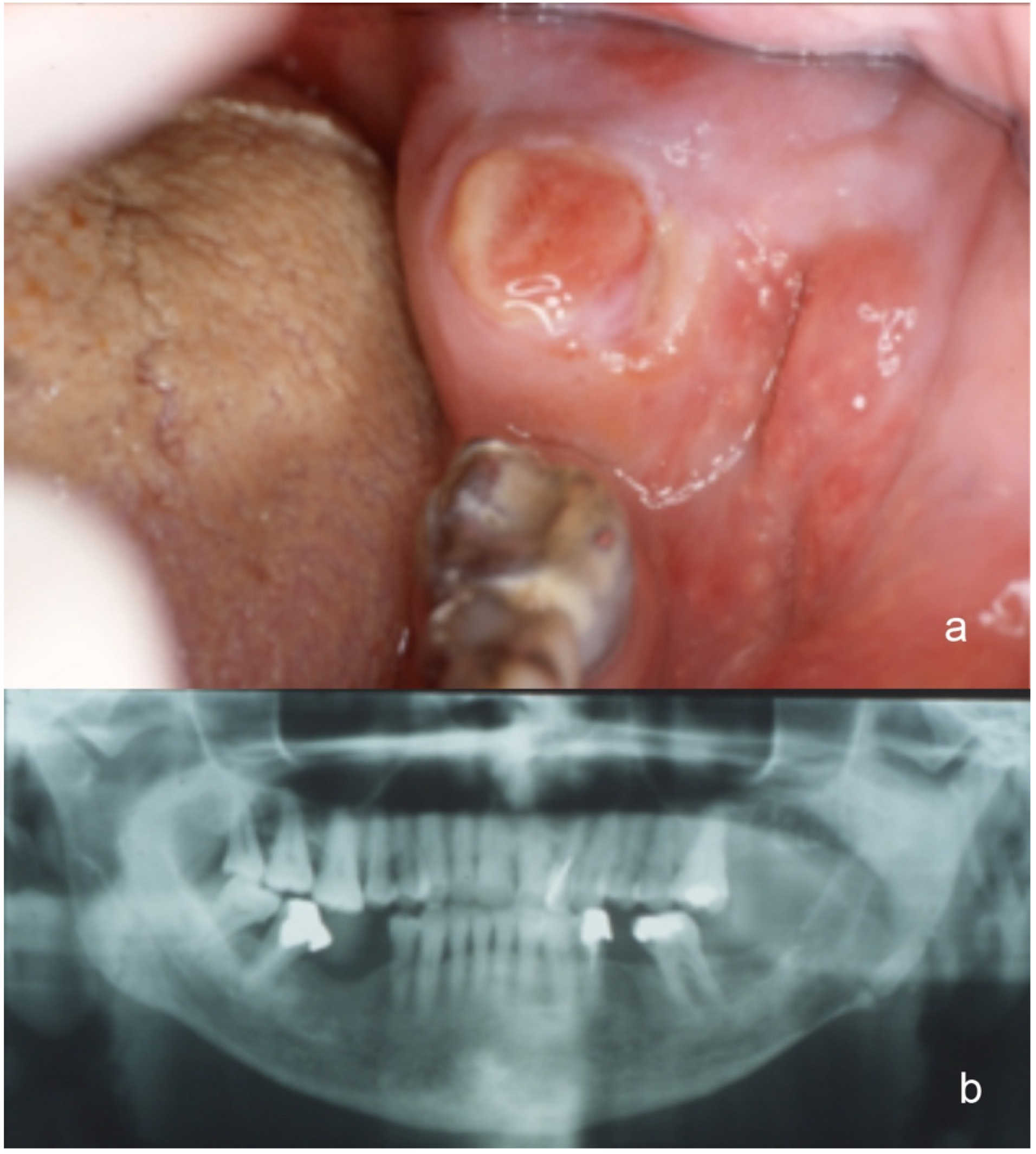
3.1. Clinical Features
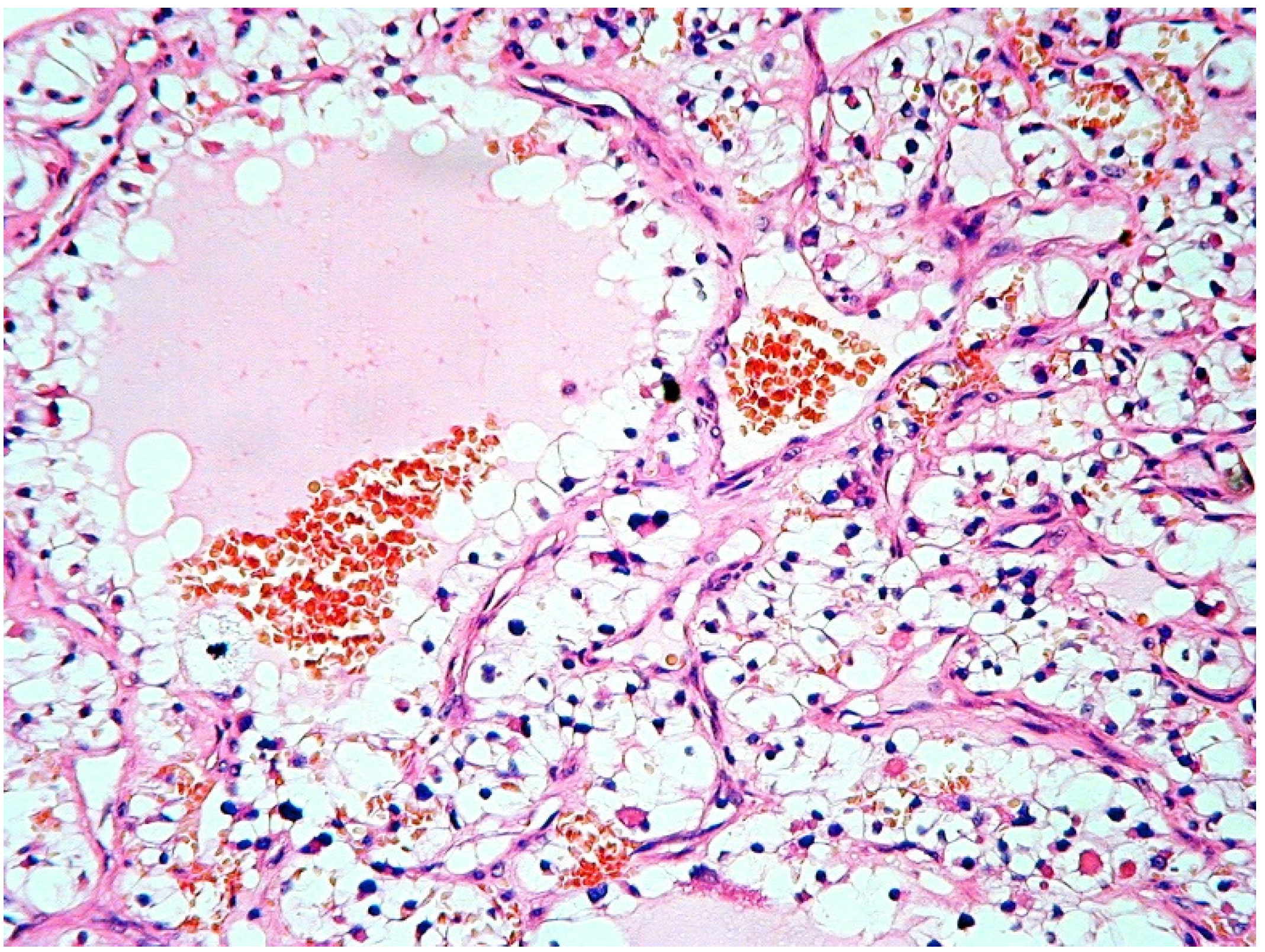
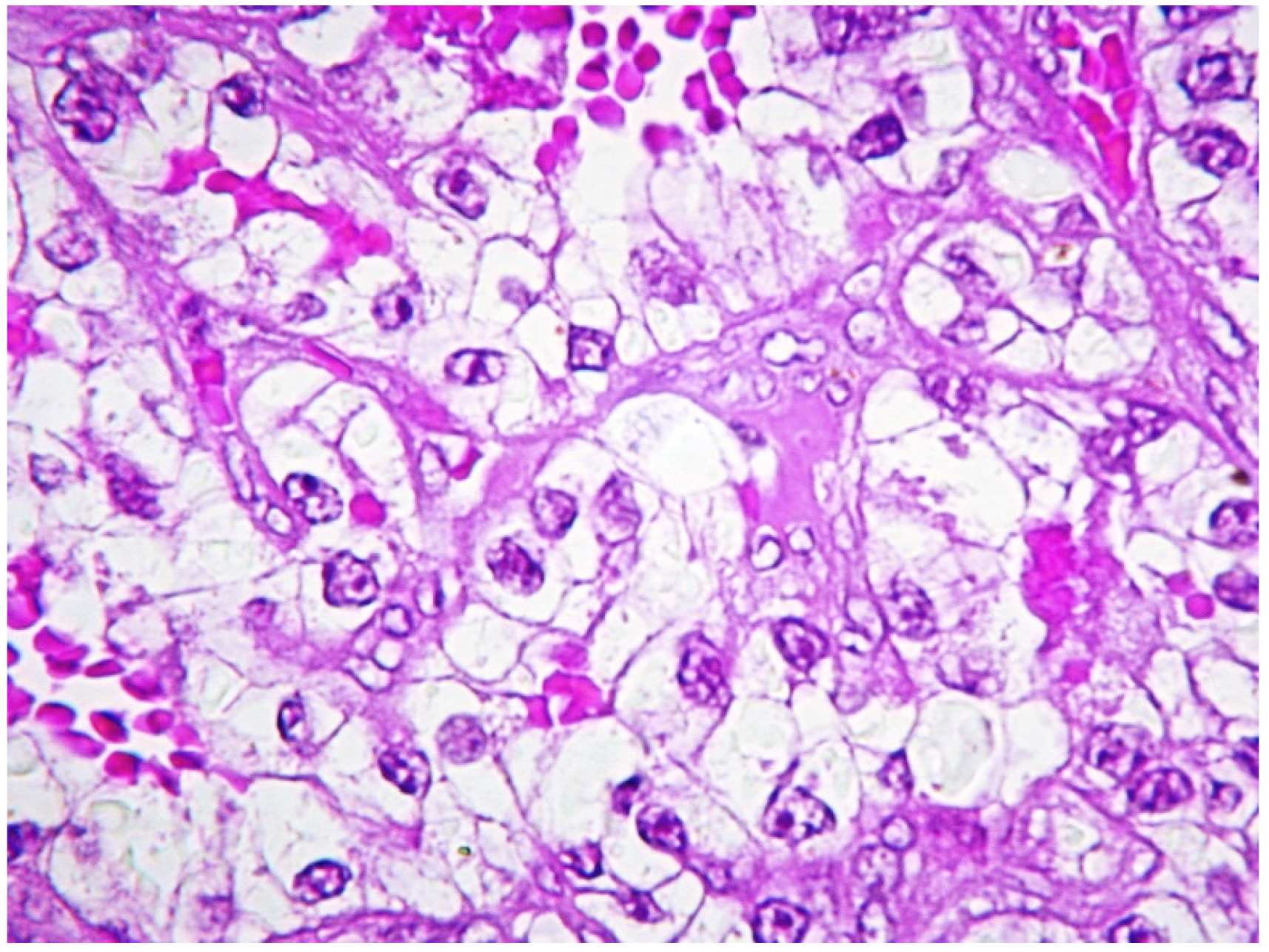
3.2. Histopathology
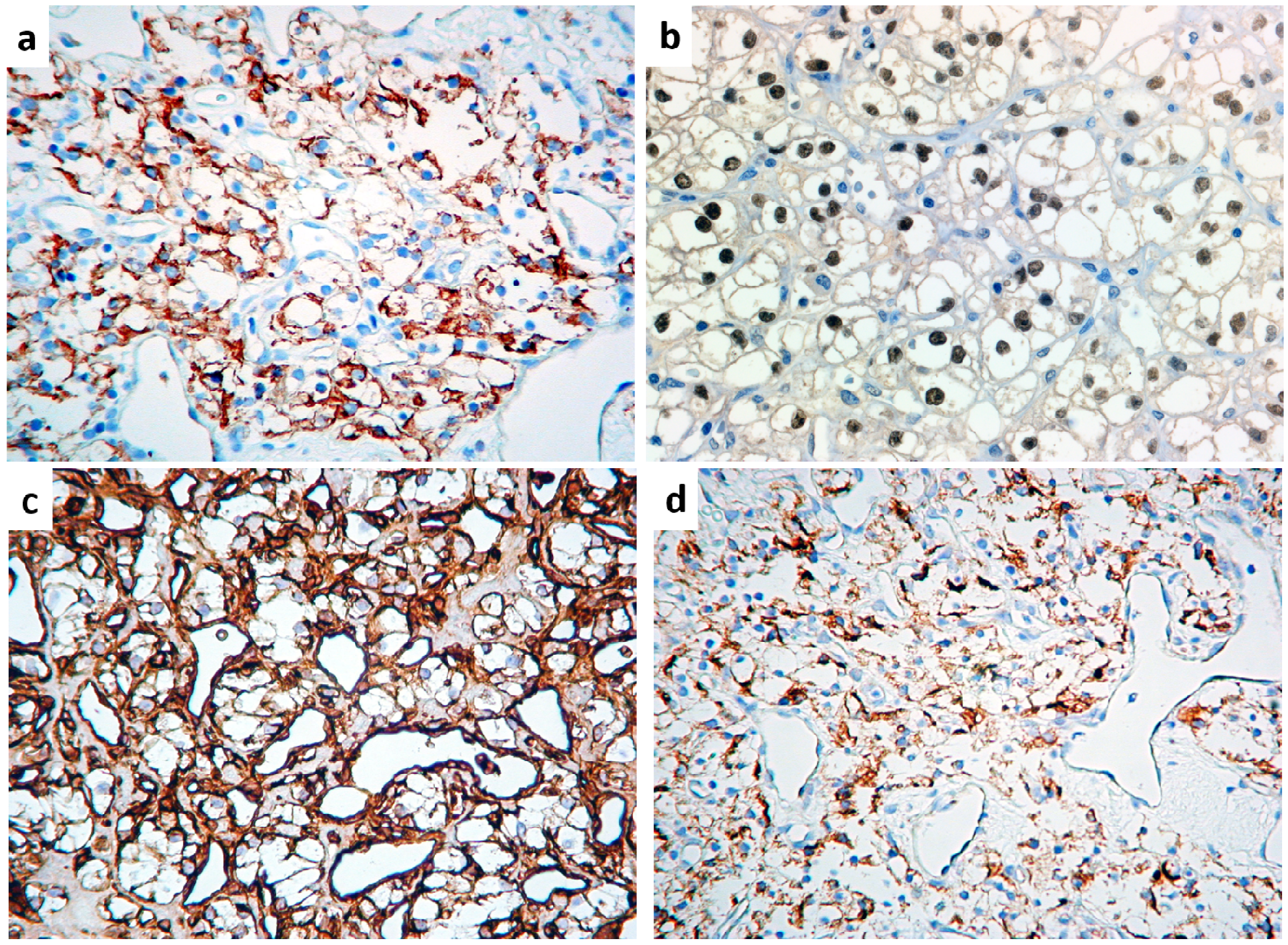
3.3. Immunohistochemistry
- cytokeratins AE1/AE3, cytokeratin 7 and EMA were detected in all tumors, with less extensive positivity for cytokeratins AE1/AE3 in myoepithelioma, for cytokeratin 7 in epithelial-myoepithelial carcinoma (EMEC), hyalinizing clear cell carcinoma (HCCC) and myoepithelioma, and for EMA in HCCC and myoepithelioma;
- muscle markers (smooth muscle actin, calponin, myosin) were highlighted in adenoid cystic carcinoma, EMEC, myoepithelioma and pleomorphic adenoma;
- CD117 was extensively positive in adenoid cystic carcinoma and EMEC and, to a lesser extent, in mucoepidermoid carcinoma and pleomorphic adenoma;
- GFAP was diffusely expressed by pleomorphic adenoma and only focally detectable in EMEC and myoepithelioma;
- Mitochondria Ag was consistently expressed by oncocytoma and occasionally by acinic cell carcinoma and adenoid cystic carcinoma;
- S-100 protein and vimentin were present in adenoid cystic carcinoma, EMEC, myoepithelioma and pleomorphic adenoma;
- Calretinin positivity was highlighted in a minority of tumor cells of acinic cell carcinoma;
- CD10, PAX8 and RCCAg were consistently negative in all tumors of this subgroup;as to odontogenic tumors:
- cytokeratins AE1/AE3, cytokeratin 7 and EMA were detected in odontogenic carcinoma but cytokeratins AE1/AE3 only was present in ameloblastoma;
- calretinin was unequivocally present in ameloblastoma but absent in odontogenic carcinoma, as was vimentin, which decorated a small number of tumor cells;
- all other antigens were invariably lacking in all odontogenic tumors.
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Hirshberg, A.; Buchner, A. Metastatic tumor to the oral region. An overview. Eur. J. Cancer B Oral Oncol. 1995, 31, 355–360. [Google Scholar] [CrossRef]
- Allon, I.; Berger, R.; Allon, I.; Kaplan, I. Metastatic Tumors to the Jaws and Mouth. Head Neck Pathol. 2014, 8, 463–474. [Google Scholar] [CrossRef] [Green Version]
- McClure, S.A.; Movahed, R.; Salama, A.; Ord, R.A. Maxillofacial Metastases: A Retrospective Review of One Institution’s 15-Year Experience. J. Oral Maxillofac. Surg. 2013, 71, 178–188. [Google Scholar] [CrossRef]
- Shen, M.L.; Kang, J.; Wen, Y.L.; Ying, W.M.; Yi, J.; Hua, C.G.; Tang, X.F.; Wen, Y.M. Metastatic tumors of the oral and maxillofacial region: A retrospective study of 19 cases in Western China and review of Chinese and English literature. J. Oral Maxillofac. Surg. 2009, 67, 718–737. [Google Scholar] [CrossRef]
- Pastremoli, A. Gingival metastasis, the first clinical sign of a silent kidney carcinoma. A case report. Minerva Stomatol. 1991, 40, 825–828. [Google Scholar]
- Raiss, H.; Duplomb, S.; Tartas, S.; Layachi, M.; Errihani, H. Lingual metastasis as an initial presentation of renal cell carcinoma: A case report. J. Med. Case Rep. 2017, 11, 314. [Google Scholar] [CrossRef] [Green Version]
- Vallata Morales, M.; Todoli Parra, J.; Cervera Miguel, J.I.; Calabuig Alborch, J.R. Right hemiparesis as presentation of renal cell carcinoma. Med. Int. 2004, 21, 359–360. [Google Scholar]
- Hirshberg, A.; Leibovich, P.; Buchner, A. Metastatic tumors at the Jawbones: Analysis of 390 cases. J. Oral Pathol. Med. 1994, 23, 337–341. [Google Scholar] [CrossRef]
- Hirshberg, A.; Leibovich, P.; Buchner, A. Metastasis to the oral mucosa: Analysis of 157 cases. J. Oral Pathol. Med. 1993, 22, 358–390. [Google Scholar] [CrossRef]
- Hirshberg, A.; Leibovich†, P.; Horowitz, I.; Buchner, A. Metastatic tumors to postextraction sites. J. Oral Maxillofac. Surg. 1993, 51, 1334–1337. [Google Scholar] [CrossRef]
- Pires, F.R.; Azevedo, R.S.; Ficarra, G.; Cardoso, A.S.; Carlos, R.; Kowalski, L.; De Almeida, O.P. Metastatic renal cell carcinoma to the oral cavity and clear cell mucoepidermoid carcinoma: Comparative clinicopathologic and immunohistochemical study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, e22–e27. [Google Scholar] [CrossRef]
- Maiorano, E.; Altini, M.; Maiorano, E. Clear cell tumors of the salivary glands, jaws, and oral mucosa. Semin. Diagn. Pathol. 1997, 14, 203–212. [Google Scholar]
- Sangoi, A.R.; Fujiwara, M.; West, R.B.; Montgomery, K.D.; Bonventre, J.V.; Higgins, J.P.; Rouse, R.V.; Gokden, N.; McKenney, J.K. Immunohistochemical Distinction of Primary Adrenal Cortical Lesions From Metastatic Clear Cell Renal Cell Carcinoma. Am. J. Surg. Pathol. 2011, 35, 678–686. [Google Scholar] [CrossRef]
- Gobbo, S.; Eble, J.N.; Grignon, D.J.; Martignoni, G.; MacLennan, G.T.; Shah, R.B.; Zhang, S.; Brunelli, M.; Cheng, L. Clear Cell Papillary Renal Cell Carcinoma. Am. J. Surg. Pathol. 2008, 32, 1239–1245. [Google Scholar] [CrossRef]
- Griffin, N.; Gore, M.E.; Sohaib, S.A. Imaging in Metastatic Renal Cell Carcinoma. Am. J. Roentgenol. 2007, 189, 360–370. [Google Scholar] [CrossRef]
- Corsi, A.; Guerra, F.; Grippaudo, G.; Bosman, C. Oral metastasis of renal cell carcinoma. Report of case and critical evaluation of morphologic features for differential diagnosis. Pathology 1994, 86, 665–669. [Google Scholar]
- Kumamoto, H.; Yamazaki, S.; Sato, A.; Yamaguchi, T.; Tezuka, F.; Ooya, K. Clear cell odontogenic tumor in the mandible: Report of a case with duct-like appearances and dentinoid induction. J. Oral Pathol. Med. 2000, 29, 43–47. [Google Scholar] [CrossRef]
- Nair, M.K.; Burkes, E.; Chai-U-Dom, O. Radiographic manifestation of clear cell odontogenic tumor. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 89, 250–254. [Google Scholar] [CrossRef]
- Pastore, A.; Ciorba, A.; Soliani, M.; Di Laora, A.; Valpiani, G.; Bianchini, C.; Stomeo, F.; Merlo, R.; Pelucchi, S. Secondary malignant tumors of the parotid gland: Not a secondary problem! J. Buon. 2017, 22, 513–518. [Google Scholar]
- Franzen, A.; Buchali, A.; Lieder, A. The rising incidence of parotid metastases: Our experience from four decades of parotid gland surgery. Acta Otorhinolaryngol. Ital. 2017, 37, 264–269. [Google Scholar]
- Majewska, H.; Skálová, A.; Radecka, K.; Stodulski, D.; Hyrcza, M.; Stankiewicz, C.; Biernat, W. Renal clear cell carcinoma metastasis to salivary glands—A series of 9 cases: Clinico-pathological study. Pol. J. Pathol. 2016, 1, 39–45. [Google Scholar] [CrossRef]
- Serouya, S.M.; Dultz, L.A.; Concors, S.J.; Wang, B.; Patel, K.N. Late Solitary Metastasis of Renal Cell Carcinoma to the Submandibular Gland. J. Oral Maxillofac. Surg. 2012, 70, 2356–2359. [Google Scholar] [CrossRef]
- Aguirre, A.; Rinaggio, J.; Diaz-Ordaz, E. Lingual metastasis of renal cell carcinoma. J. Oral Maxillofac. Surg. 1996, 54, 344–347. [Google Scholar] [CrossRef]
- Selden, H.S.; Manhoff, D.T.; Hatges, N.A.; Michel, R.C. Metastatic carcinoma to the mandible that mimicked pulpal/periodontal disease. J. Endod. 1998, 24, 267–270. [Google Scholar] [CrossRef]
- Sauerborn, D.; Vidakovic, B.; Baranovic, M.; Mahovne, I.; Danic, P.; Danic, D. Gastric adenocarcinoma metastasis to the alveolar mucosa of the mandible. A case report and reviev of the literature. J. Craniomaxillofac. Surg. 2011, 39, 645–648. [Google Scholar] [CrossRef]
- Jain, A.; Shetty, D.C.; Juneja, S.; Narwal, N. Molecular Characterization of Clear Cell Lesions of Head and Neck. J. Clin. Diagn. Res. 2016, 10, ZE18–ZE23. [Google Scholar] [CrossRef]
- Truong, L.D.; Shen, S.S. Immunohistochemical diagnosis of renal neoplasms. Arch. Pathol. Lab. Med. 2011, 135, 92–109. [Google Scholar]
- Reuter, V.E.; Argani, P.; Zhou, M.; Delahunt, B. Best Practices Recommendations in the Application of Immunohistochemistry in the Kidney Tumors. Am. J. Surg. Pathol. 2014, 38, e35–e49. [Google Scholar] [CrossRef]
- Amin, M.B.; Epstein, J.I.; Ulbright, T.M.; Humphrey, P.A.; Egevad, L.; Montironi, R.; Grignon, D.; Trpkov, K.; Lopez-Beltran, A.; Zhou, M.; et al. Best Practices Recommendations in the Application of Immunohistochemistry in Urologic Pathology. Am. J. Surg. Pathol. 2014, 38, 1017–1022. [Google Scholar] [CrossRef]
- Mirkovic, J.; Calicchio, M.; Pérez-Atayde, A.R.; Fletcher, C.D. Diffuse and strong cyclin D1 immunoreactivity in clear cell sarcoma of the kidney. Histopathology 2015, 67, 306–312. [Google Scholar] [CrossRef]
- Ozcan, A.; De La Roza, G.; Ro, J.; Shen, S.S.; Truong, L.D. PAX2 and PAX8 Expression in Primary and Metastatic Renal Tumors: A Comprehensive Comparison. Arch. Pathol. Lab. Med. 2012, 136, 1541–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, S.S.; Truong, L.D.; Scarpelli, M.; Lopez-Beltran, A. Role of Immunohistochemistry in Diagnosing Renal Neoplasms: When Is It Really Useful? Arch. Pathol. Lab. Med. 2012, 136, 410–417. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antigen | Clone | Dilution | Source | Positive control |
|---|---|---|---|---|
| Actin (smooth muscle) | 1A4 | 1/200 | Agilent Technologies (Santa Clara, CA, USA) | Leiomyoma |
| Calponin | CALP | 1/400 | Agilent Technologies | Leiomyoma |
| Calretinin | Cal6 | 1/50 | Novocastra (Newcastle upon Tyne, UK) | Mesothelioma |
| CD 10 | 56C6 | 1/100 | Novocastra | Lymph node |
| CD 117 | polyclonal | 1/100 | Agilent Technologies | GIST |
| Cytokeratins (pan) | AE1/AE3 | 1/300 | Agilent Technologies | Breast carcinoma |
| Cytokeratin 7 | OV-TL 12/30 | 1/250 | Agilent Technologies | Breast carcinoma |
| Epithelial membrane antigen (EMA) | E29 | 1/20 | Agilent Technologies | Colon |
| Glial fibrillary acidic protein (GFAP) | 6F2 | 1/100 | Agilent Technologies | Brain |
| Mitochondria Ag | 113-1 | 1/300 | Menarini Diagnostics (Firenze, IT, USA) | Salivary oncocytoma |
| Myosin (SMMHC) | SMMS-1 | 1/50 | Agilent Technologies | Leiomyoma |
| PAX-8 | polyclonal | 1/200 | Bio Care Medical (The Hague, NL, USA) | Kidney |
| Renal cell carcinoma antigen (RCC Ag) | SPM314 | 1/100 | Agilent Technologies | Kidney |
| S-100 Protein | polyclonal | 1/50 | Agilent Technologies | Brain |
| Vimentin | V9 | 1/50 | Agilent Technologies | Leiomyoma |
| Case | Sex | Age | Site | Size | First Sign of Disease | Additional Metastases |
|---|---|---|---|---|---|---|
| 1 | F | 69 | Gingiva | 5 cm | No | Lungs |
| 2 | M | 56 | Tongue | 4 cm | No | Thyroid, opposite kidney, finger |
| 3 | M | 45 | Mandible | 5.5 cm | No | - |
| 4 | M | 63 | Mandible | 5 cm | Yes | Vertebra |
| 5 | M | 55 | Parotid Gland | 2.2 | Yes | - |
| 6 | F | 55 | Parotid Gland | 1.8 | No | - |
| 7 | M | 60 | Mandible | 3.5 cm | No | - |
| Actin (Smooth Muscle) | Calponin | Calretinin | CD 10 | CD 117 | CK AE1/AE3 | CK 7 | EMA | GFAP | Myosin (SMMHC) | Mitochondria | PAX8 | RCCAg | S-100Protein | Vimentin | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CCRCC | - | - | - | + | - | + | - | + | - | - | ± | + | + | ± | + |
| Acinic cell carcinoma | - | - | ± | - | - | + | + | + | - | - | ± | - | - | - | - |
| Adenoid cystic carcinoma | + | + | - | - | + | + | + | + | + | - | - | - | + | + | |
| EMEC | + | + | - | - | + | + | ± | + | ± | + | - | - | - | + | + |
| HCCC | - | - | - | - | - | + | ± | ± | - | - | - | - | - | - | - |
| Mucoepidermoid carcinoma | - | - | - | - | ± | + | + | + | - | - | - | - | - | - | - |
| Myoepithelioma | + | + | - | - | - | ± | ± | ± | ± | + | - | - | - | + | + |
| Oncocytoma | - | - | - | - | - | + | - | + | - | - | + | - | - | - | - |
| Pleomorphic adenoma | + | + | - | - | ± | + | + | + | + | + | - | - | - | + | + |
| Ameloblastoma | - | - | + | - | - | + | - | - | - | - | - | - | - | - | + |
| Odontogenic carcinoma | - | - | - | - | - | + | + | + | - | - | - | - | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capodiferro, S.; Limongelli, L.; Mastropasqua, M.G.; Favia, G.; Lajolo, C.; Colella, G.; Tempesta, A.; Maiorano, E. Metastatic Tumors of the Oro-Facial Tissues: Clear Cell Renal Cell Carcinoma. A Clinico-Pathological and Immunohistochemical Study of Seven Cases. J. Clin. Med. 2020, 9, 1151. https://doi.org/10.3390/jcm9041151
Capodiferro S, Limongelli L, Mastropasqua MG, Favia G, Lajolo C, Colella G, Tempesta A, Maiorano E. Metastatic Tumors of the Oro-Facial Tissues: Clear Cell Renal Cell Carcinoma. A Clinico-Pathological and Immunohistochemical Study of Seven Cases. Journal of Clinical Medicine. 2020; 9(4):1151. https://doi.org/10.3390/jcm9041151
Chicago/Turabian StyleCapodiferro, Saverio, Luisa Limongelli, Mauro Giuseppe Mastropasqua, Gianfranco Favia, Carlo Lajolo, Giuseppe Colella, Angela Tempesta, and Eugenio Maiorano. 2020. "Metastatic Tumors of the Oro-Facial Tissues: Clear Cell Renal Cell Carcinoma. A Clinico-Pathological and Immunohistochemical Study of Seven Cases" Journal of Clinical Medicine 9, no. 4: 1151. https://doi.org/10.3390/jcm9041151