Clinical Impact of Atypical Chest Pain and Diabetes Mellitus in Patients with Acute Myocardial Infarction from Prospective KAMIR-NIH Registry

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
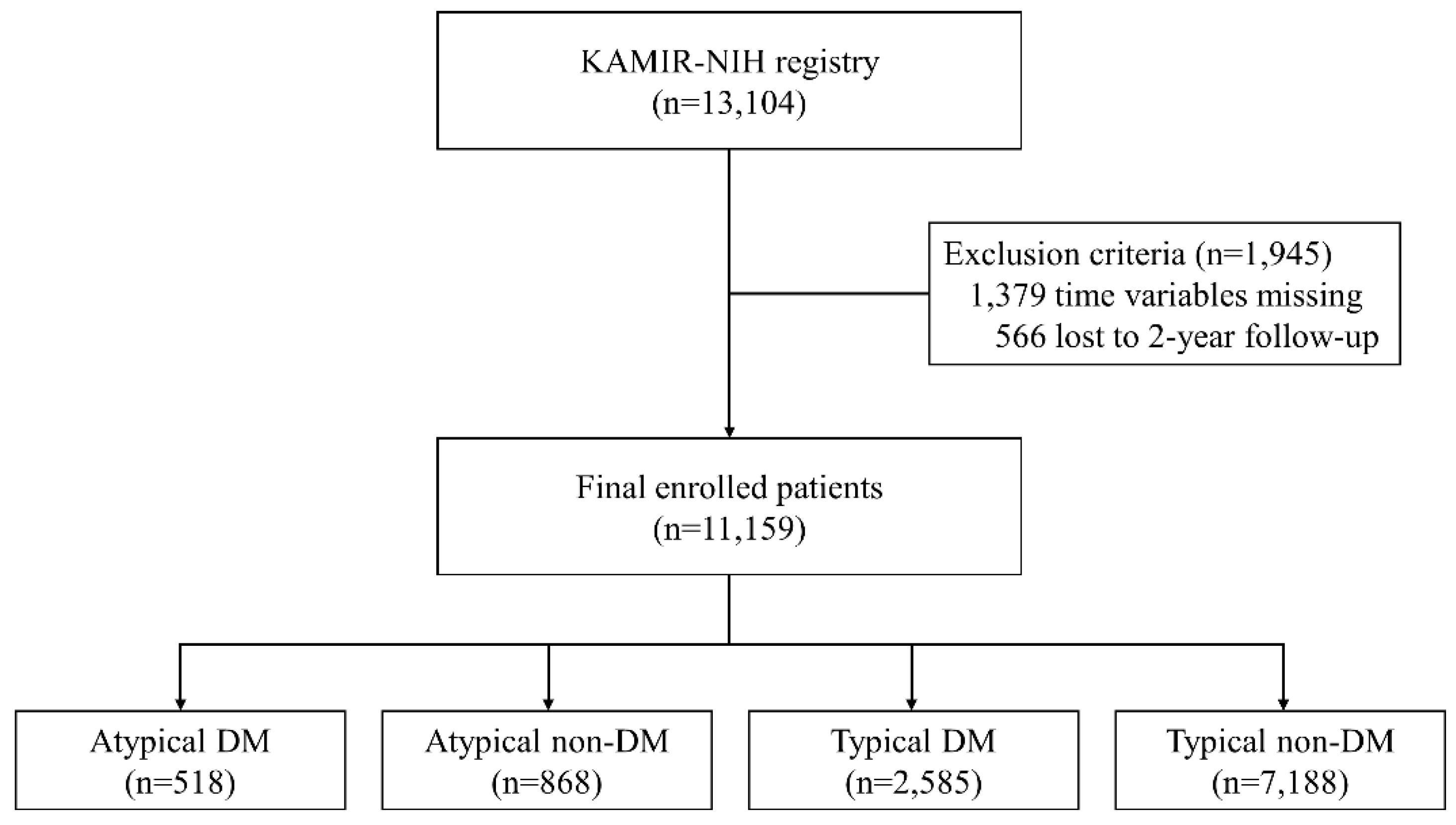
2.1. Study Population
2.2. Definition and Data Collection
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Angiographic and Procedural Characteristics
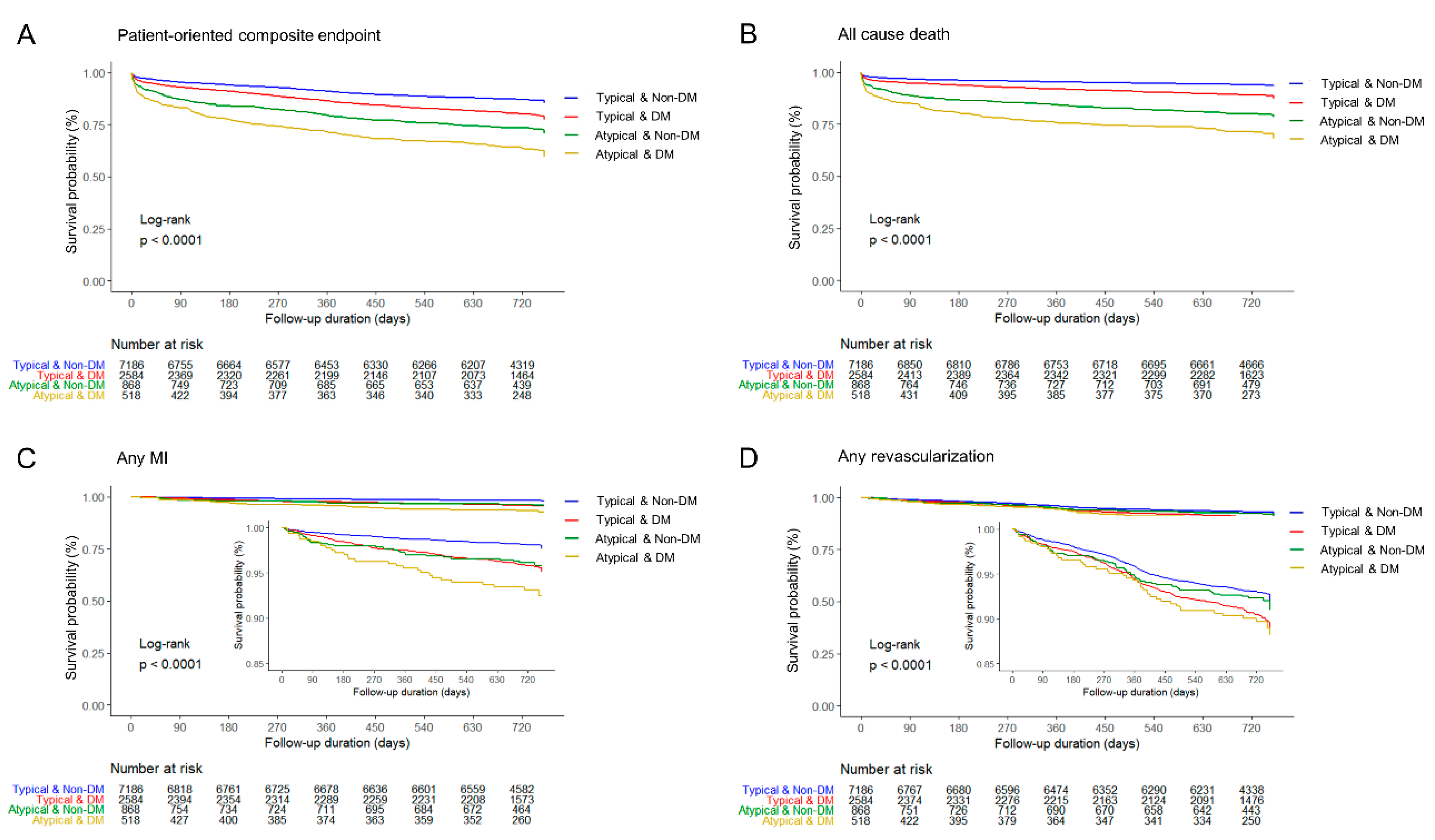
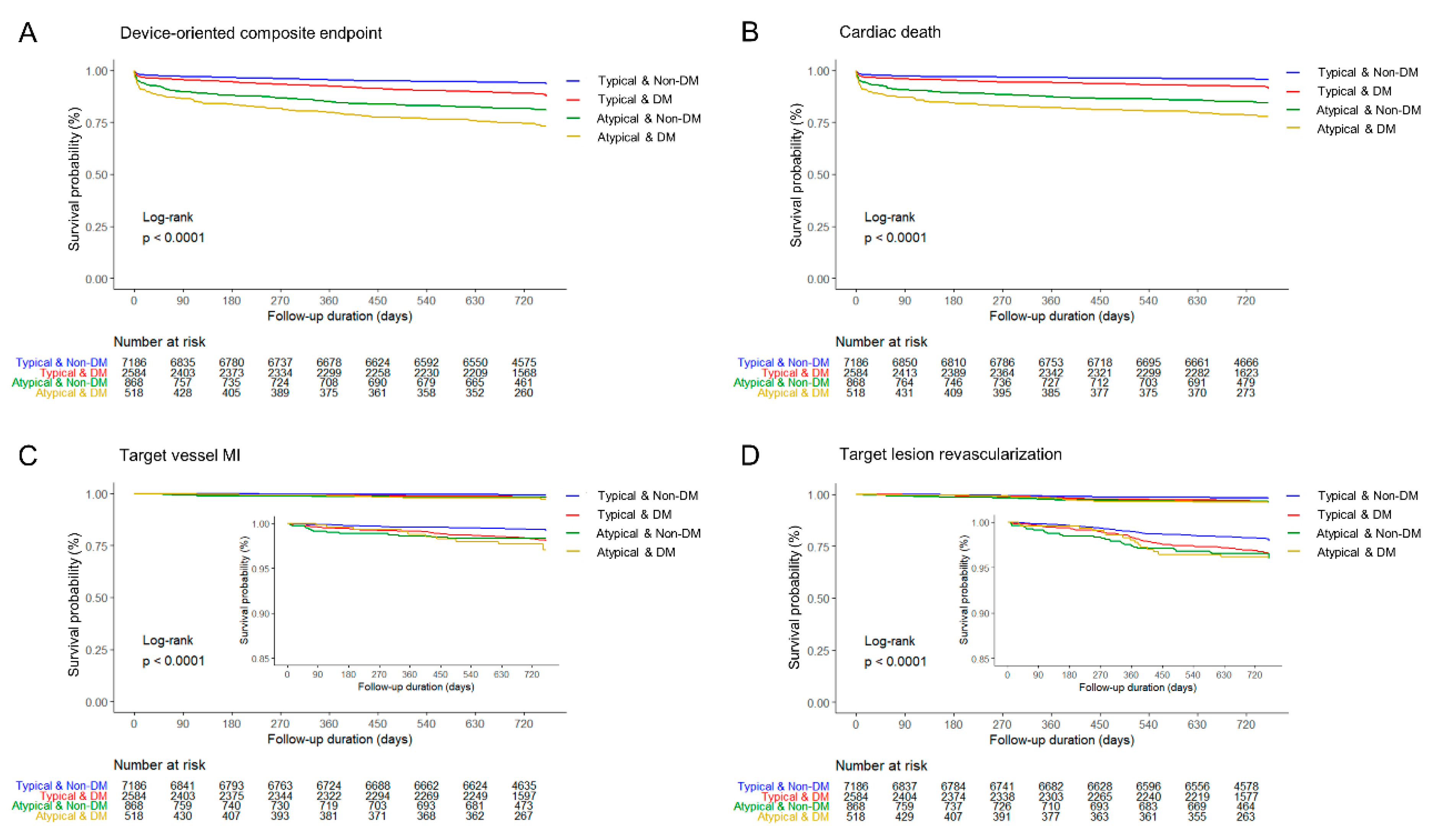
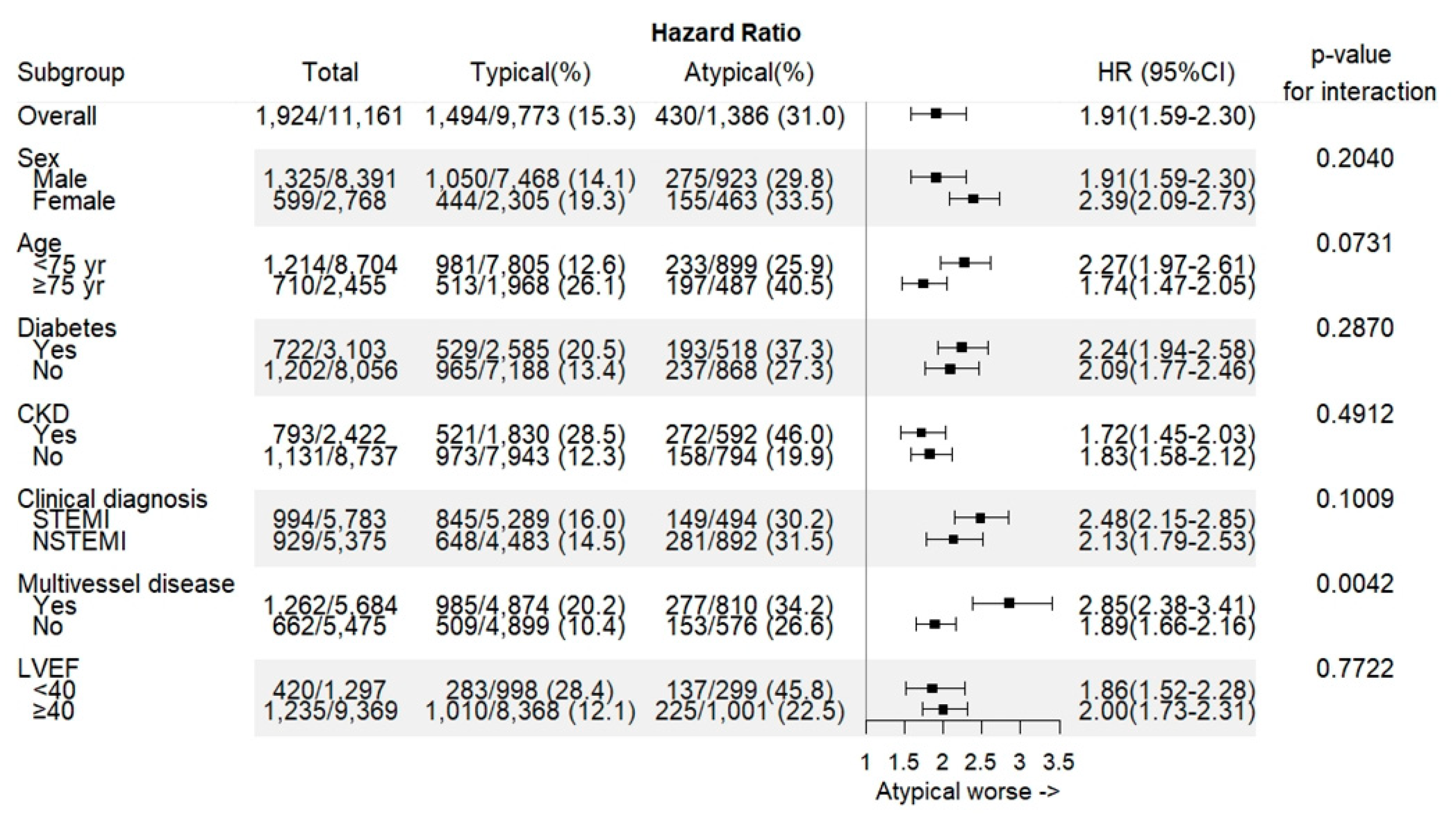
3.3. Clinical Outcomes
4. Discussion
- Patients with atypical chest pain were older, affected more females, had more comorbidities, delayed admission, and delayed treatment.
- Patients with atypical chest pain showed higher in-hospital death and long-term mortality irrespective of diabetes history.
- The coexistence of atypical chest pain and DM was at the highest risk of cardiovascular events.
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, T.H.; Goldman, L. Evaluation of the Patient with Acute Chest Pain. N. Engl. J. Med. 2000, 342, 1187–1195. [Google Scholar] [CrossRef]
- Hermann, L.K.; Weingart, S.D.; Yoon, Y.M.; Genes, N.G.; Nelson, B.P.; Shearer, P.L.; Duvall, W.L.; Henzlova, M.J. Comparison of Frequency of Inducible Myocardial Ischemia in Patients Presenting to Emergency Department with Typical Versus Atypical or Nonanginal Chest Pain. Am. J. Cardiol. 2010, 105, 1561–1564. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J. Chronic Stable Angina. N. Engl. J. Med. 2005, 352, 2524–2533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Body, R.; Carley, S.; Wibberley, C.; McDowell, G.; Ferguson, J.; Mackway-Jones, K. The value of symptoms and signs in the emergent diagnosis of acute coronary syndromes. Resuscitation 2010, 81, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Canto, J.G.; Shlipak, M.G.; Rogers, W.J.; Malmgren, J.A.; Frederick, P.D.; Lambrew, C.T.; Ornato, J.P.; Barron, H.V.; Kiefe, C.I. Prevalence, Clinical Characteristics, and Mortality Among Patients With Myocardial Infarction Presenting Without Chest Pain. JAMA 2000, 283, 3223–3229. [Google Scholar] [CrossRef]
- Brieger, D.; Eagle, K.A.; Goodman, S.G.; Steg, P.G.; Budaj, A.; White, K.; Montalescot, G.; GRACE Investigators. Acute Coronary Syndromes Without Chest Pain, An Underdiagnosed and Undertreated High-Risk Group: Insights From The Global Registry of Acute Coronary Events. Chest 2004, 126, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Bjorck, L.; Nielsen, S.; Jernberg, T.; Zverkova-Sandstrom, T.; Giang, K.W.; Rosengren, A. Absence of chest pain and long-term mortality in patients with acute myocardial infarction. Open Heart 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Expert Panel on Detection; Evaluation and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Newman, J.D.; Rockman, C.B.; Kosiborod, M.; Guo, Y.; Zhong, H.; Weintraub, H.S.; Schwartzbard, A.Z.; Adelman, M.A.; Berger, J.S. Diabetes mellitus is a coronary heart disease risk equivalent for peripheral vascular disease. Am. Heart J. 2017, 184, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Acharya, D.U.; Shekhar, Y.C.; Aggarwal, A.; Anand, I.S. Lack of pain during myocardial infarction in diabetics—Is autonomic dysfunction responsible? Am. J. Cardiol. 1991, 68, 793–796. [Google Scholar] [CrossRef]
- Junghans, C.; Sekhri, N.; Zaman, M.J.; Hemingway, H.; Feder, G.S.; Timmis, A. Atypical chest pain in diabetic patients with suspected stable angina: impact on diagnosis and coronary outcomes. Eur. Heart J. Qual. Care Clin. Outcomes 2015, 1, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Chae, S.C.; Oh, D.J.; Kim, H.S.; Kim, Y.J.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Yoon, J.H.; Park, H.Y.; et al. Korea Acute Myocardial Infarction-National Institutes of Health Registry Investigators. Multicenter Cohort Study of Acute Myocardial Infarction in Korea—Interim Analysis of the Korea Acute Myocardial Infarction Registry-National Institutes of Health Registry. Circ. J. 2016, 80, 1427–1436. [Google Scholar] [PubMed] [Green Version]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: Executive Summary. J. Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swap, C.J.; Nagurney, J.T. Value and Limitations of Chest Pain History in the Evaluation of Patients With Suspected Acute Coronary Syndromes. JAMA 2005, 294, 2623–2629. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Mickley, H.; Crea, F.; Van De Werf, F. Fourth universal definition of myocardial infarction (2018). Eur. Heart. J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- El-Menyar, A.; Zubaid, M.; Sulaiman, K.; AlMahmeed, W.; Singh, R.; Alsheikh-Ali, A.A.; Al Suwaidi, J.; Gulf Registry of Acute Coronary Events (Gulf RACE) Investigators. Atypical presentation of acute coronary syndrome: a significant independent predictor of in-hospital mortality. J. Cardiol. 2011, 57, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Kim, Y.J.; Jeong, M.H. Current status of acute myocardial infarction in Korea. Korean J. Intern. Med. 2019, 34, 1–10. [Google Scholar] [CrossRef]
- Kirchberger, I.; Heier, M.; Kuch, B.; von Scheidt, W.; Meisinger, C. Presenting symptoms of myocardial infarction predict short- and long-term mortality: The MONICA/KORA Myocardial Infarction Registry. Am. Heart. J. 2012, 164, 856–861. [Google Scholar] [CrossRef]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [Green Version]
- Beckman, J.A.; Paneni, F.; Cosentino, F.; Creager, M.A. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Eur. Heart J. 2013, 34, 2444–2452. [Google Scholar] [CrossRef] [Green Version]
- Emerging Risk Factors Collaboration. Association of Cardiometabolic Multimorbidity with Mortality. JAMA 2015, 314, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Vinik, A.I.; Maser, R.E.; Mitchell, B.D.; Freeman, R. Diabetic Autonomic Neuropathy. Diabetes Care 2003, 26, 1553–1579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maser, R.E.; Mitchell, B.D.; Vinik, A.I.; Freeman, R. The Association Between Cardiovascular Autonomic Neuropathy and Mortality in Individuals With Diabetes. Diabetes Care 2003, 26, 1895–1901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.K.; Bullard, K.M.; Saaddine, J.B.; Cowie, C.C.; Imperatore, G.; Gregg, E.W. Achievement of Goals in U.S. Diabetes Care, 1999–2010. N. Engl. J. Med. 2013, 368, 1613–1624. [Google Scholar] [CrossRef] [Green Version]
- Pop-Busui, R.; Evans, G.W.; Gerstein, H.C.; Fonseca, V.; Fleg, J.L.; Hoogwerf, B.J.; Genuth, S.; Grimm, R.H.; Corson, M.A.; Prineas, R.; et al. Effects of Cardiac Autonomic Dysfunction on Mortality Risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Trial. Diabetes Care. 2010, 33, 1578–1584. [Google Scholar] [CrossRef] [Green Version]
- Rawshani, A.; Rawshani, A.; Franzén, S.; Sattar, N.; Eliasson, B.; Svensson, A.M.; Zethelius, B.; Miftaraj, M.; McGuire, D.K.; Rosengren, A.; et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2018, 379, 633–644. [Google Scholar] [CrossRef]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, I.; Yardim, M. Biomarkers in acute myocardial infarction: current perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 11,161 | Diabetic Patients | Non-Diabetic Patients | |||||
|---|---|---|---|---|---|---|---|
| Atypical n = 518 | Typical n = 2585 | p-Value | Atypical n = 868 | Typical n = 7188 | p-Value | ||
| Age (year) | 63.6 ± 12.5 | 68.5 ± 10.7 | 65.2 ± 11.2 | <0.0001 | 68.4 ± 12.8 | 62.0 ± 12.7 | <0.0001 |
| Male | 8812 (75.2) | 328 (63.3) | 1822 (70.5) | 0.0013 | 595 (68.6) | 5646 (78.6) | <0.0001 |
| Height (cm) | 164.4 ± 11.3 | 161.9 ± 11.4 | 163.5 ± 12.1 | 0.0062 | 162.8 ± 9.0 | 165.1 ± 11.2 | <0.0001 |
| Weight (kg) | 65.7 ± 12.1 | 62.2 ± 12.0 | 65.8 ± 11.6 | <0.0001 | 61.6 ± 12.2 | 66.4 ± 12.1 | <0.0001 |
| BMI (kg/m2) | 24.1 ± 3.3 | 23.5 ± 3.6 | 24.3 ± 3.3 | <0.0001 | 23.1 ± 3.5 | 24.2 ± 3.3 | <0.0001 |
| Medical history | |||||||
| Hypertension | 5894 (50.3) | 371 (71.6) | 1719 (66.5) | 0.0232 | 429 (49.4) | 3095 (43.1) | 0.0004 |
| CKD | 2566 (21.9) | 294 (56.8) | 812 (31.4) | <0.0001 | 298 (34.3) | 1018 (14.2) | <0.0001 |
| Dyslipidemia | 1330 (11.3) | 49 (9.5) | 417 (16.1) | 0.0001 | 52 (6.0) | 753 (10.5) | <0.0001 |
| Previous MI | 824 (7.0) | 72 (13.9) | 252 (9.8) | 0.0048 | 52 (6.0) | 401 (5.6) | 0.6187 |
| Old CVA | 777 (6.6) | 72 (13.9) | 234 (9.1) | 0.0007 | 83 (9.6) | 355 (4.9) | <0.0001 |
| Current smoker | 4713 (40.2) | 135 (26.1) | 852 (33.0) | 0.0021 | 279 (32.1) | 3211 (44.7) | <0.0001 |
| Associated dyspnea | 2630 (22.4) | 266 (51.4) | 545 (21.1) | <0.0001 | 373 (43.0) | 1298 (18.1) | <0.0001 |
| Clinical Diagnosis | |||||||
| STEMI | 6078 (51.8) | 165 (31.9) | 1273 (49.3) | <0.0001 | 329 (37.9) | 4016 (55.8) | <0.0001 |
| NSTEMI | 5646 (48.2) | 353 (68.2) | 1312 (50.8) | 539 (62.1) | 3171 (44.1) | ||
| Systolic BP (mmHg) | 129.9 ± 30.1 | 124.9 ± 33.4 | 130.4 ± 29.6 | 0.0006 | 124.1±33.9 | 130.8 ± 29.4 | <0.0001 |
| Diastolic BP (mmHg) | 78.7 ± 18.5 | 74.5 ± 20.5 | 77.7 ± 17.4 | 0.0008 | 75.4 ± 21.2 | 79.7 ± 18.3 | <0.0001 |
| HR, bpm | 78.1 ± 19.3 | 85.7 ± 24.6 | 80.0 ± 19.2 | <0.0001 | 80.8 ± 25.1 | 76.5 ± 17.9 | <0.0001 |
| Hemoglobin (g/dL) | 13.9 ± 2.1 | 12.0 ± 2.4 | 13.4 ± 2.1 | <0001 | 13.1 ± 2.3 | 14.3 ± 1.9 | <0001 |
| Glucose (mg/dL) | 169.7 ± 81.0 | 245.0 ± 123.8 | 223.1 ± 99.1 | 0.0002 | 157.7 ± 70.4 | 146.3 ± 53.9 | <0001 |
| Creatinine (mg/dL) | 1.1 ± 1.1 | 2.0 ± 2.1 | 1.3 ± 1.4 | <0001 | 1.3 ± 1.4 | 1.0 ± 0.8 | <0001 |
| Peak CK-MB (ng/mL) | 118.80 ± 170.90 | 62.11 ± 108.80 | 97.32 ± 134.30 | <0001 | 100.30 ± 164.30 | 132.80 ± 184.60 | <0001 |
| Peak Troponin I (ng/mL) | 50.58 ± 109.70 | 32.31 ± 59.37 | 49.86 ± 89.21 | <0001 | 45.77 ± 127.60 | 52.90 ± 116.80 | 0.1337 |
| Total cholesterol (mg/dL) | 179.4 ± 45.7 | 158.3 ± 46.3 | 167.2 ± 46.2 | 0.0001 | 175.1 ± 45.9 | 185.8 ± 44.0 | <0001 |
| Triglyceride (mg/dL) | 136.1 ± 119.4 | 118.2 ± 70.5 | 142.1 ± 115.0 | <0001 | 109.7 ± 68.1 | 138.3 ± 127.4 | <0001 |
| HDL-cholesterol (mg/dL) | 42.6 ± 11.7 | 39.0 ± 12.7 | 41.1 ± 11.6 | 0.0010 | 42.6 ± 12.6 | 43.4 ± 11.4 | 0.1126 |
| LDL-cholesterol (mg/dL) | 113.1 ± 39.2 | 94.6 ± 39.0 | 101.9 ± 38.3 | 0.0004 | 111.0 ± 40.6 | 118.5 ± 38.2 | <0001 |
| Killip class | <0.0001 | <0.0001 | |||||
| 1 | 9280 (79.2) | 248 (48.0) | 1993 (77.1) | 521 (60.0) | 6054 (84.2) | ||
| 2 | 959 (8.2) | 67 (13.0) | 241 (9.3) | 105 (12.1) | 509 (7.1) | ||
| 3 | 789 (6.7) | 124 (24.0) | 192 (7.4) | 142 (16.4) | 291 (4.1) | ||
| 4 | 696 (5.9) | 78 (15.1) | 159 (6.2) | 100 (11.5) | 334 (4.7) | ||
| Killip class ≥2 | 2445 (20.9) | 270 (52.1) | 592 (22.9) | <0.0001 | 347 (40.0) | 1134 (15.8) | <0.0001 |
| LVEF, % | 52.0 ± 10.9 | 46.3±13.0 | 51.1 ± 11.4 | <0.0001 | 49.6 ± 11.5 | 53.0 ± 10.2 | <0.0001 |
| STD time (minute) | 216.0 (87.0, 749.5) | 408.5 (92.0, 2880.0) | 238.0 (100.5, 822.0) | <0.0001 | 361.0 (112.0, 1448.0) | 194.0 (80.0, 597.0) | <0.0001 |
| DTB time (minute) | 104.0 (58.0, 861.0) | 401.5 (96.0, 1388.0) | 122.0 (59.00, 922.0) | <0.0001 | 233.5 (75.0, 1125.0) | 85.0 (55.0, 728.0) | <0.0001 |
| Discharge medication | |||||||
| Aspirin | 11,698 (99.8) | 511 (98.7) | 2579 (99.8) | 0.0024 | 866 (99.8) | 7176 (99.8) | 0.6572 |
| P2Y12 inhibitor | 11,108 (99.5) | 511 (98.7) | 2575 (99.6) | 0.0146 | 863 (99.4) | 7159 (99.6) | 0.4068 |
| CCB | 651 (5.8) | 53 (10.2) | 174 (6.7) | 0.0052 | 53 (6.1) | 371 (5.2) | 0.2391 |
| Beta blocker | 9355 (83.8) | 388 (74.9) | 2190 (84.7) | <0.0001 | 655 (75.5) | 6122 (85.2) | <0.0001 |
| RAS inhibitor | 8882 (79.6) | 380 (73.4) | 2050 (79.3) | 0.0027 | 640 (73.7) | 5812 (80.9) | <0.0001 |
| Statin | 10,277 (92.1) | 405 (78.2) | 2342 (90.6) | <0.0001 | 748 (86.2) | 6782 (94.4) | <0.0001 |
| Total n = 11,161 | Diabetic Patients | Non-Diabetic Patients | |||||
|---|---|---|---|---|---|---|---|
| Atypical n = 518 | Typical n = 2585 | p-Value | Atypical n = 868 | Typical n = 7188 | p-Value | ||
| Disease extent | 0.0020 | <0.0001 | |||||
| 1-vessel disease | 5475 (49.1) | 175 (33.8) | 1054 (40.8) | 401 (46.2) | 3845 (53.5) | ||
| 2-vessel disease | 3812 (34.2) | 201 (38.8) | 978 (37.8) | 305 (35.1) | 2328 (32.4) | ||
| 3-vessel disease | 1872 (16.8) | 142 (27.4) | 553 (21.4) | 162 (18.7) | 1015 (14.1) | ||
| Multivessel disease | 5684 (50.9) | 343 (66.2) | 1531 (59.2) | 0.0030 | 467 (53.8) | 3343 (46.5) | <0.0001 |
| Culprit lesion | 0.0367 | 0.0003 | |||||
| Left main | 264 (2.4) | 24 (4.6) | 70 (2.7) | 27 (3.1) | 143 (2.0) | ||
| LAD | 5208 (46.7) | 235 (45.4) | 1174 (45.4) | 357 (41.1) | 3442 (47.9) | ||
| LCX | 1950 (17.5) | 73 (14.1) | 452 (17.5) | 157 (18.1) | 1268 (17.6) | ||
| RCA | 3737 (33.5) | 186 (35.9) | 889 (34.4) | 327 (37.7) | 2335 (32.5) | ||
| Lesion type | 0.0521 | 0.1673 | |||||
| A | 148 (1.3) | 12 (2.3) | 25 (1.0) | 10 (1.2) | 101 (1.4) | ||
| B1 | 1337 (12.0) | 66 (12.7) | 308 (11.9) | 103 (11.2) | 860 (12.0) | ||
| B2 | 4180 (37.5) | 197 (38.0) | 961 (37.2) | 299 (34.5) | 2723 (37.9) | ||
| C | 5494 (49.2) | 243 (46.9) | 1291 (49.9) | 456 (52.5) | 3504 (48.8) | ||
| Lesion treatment | 0.9000 | 0.4315 | |||||
| Stent | 10,343 (93.1) | 473 (91.8) | 2372 (92.0) | 800 (92.9) | 6698 (93.6) | ||
| Balloon angioplasty | 766 (6.9) | 42 (8.2) | 206 (8.0) | 61 (7.1) | 457 (6.4) | ||
| Total number of stents | 1.5 ± 0.8 | 1.6 ± 0.9 | 1.6 ± 0.8 | 0.0745 | 1.5 ± 0.8 | 1.4 ± 0.7 | 0.0030 |
| GP IIb/IIIa inhibitor | 1720 (15.4) | 51 (9.9) | 355 (13.7) | 0.0166 | 109 (12.6) | 1205 (16.8) | 0.0015 |
| Thrombolysis | 2790 (25.0) | 62 (12.0) | 582 (22.5) | <0.0001 | 143 (16.5) | 2003 (27.9) | <0.0001 |
| Pre TIMI | 0.0062 | 0.0117 | |||||
| 0 | 5258 (47.1) | 172 (33.2) | 1066 (41.2) | 387 (44.6) | 3633 (50.5) | ||
| 1 | 1232 (11.0) | 77 (14.9) | 322 (12.5) | 100 (11.5) | 733 (10.2) | ||
| 2 | 1739 (15.6) | 109 (21.0) | 457 (17.7) | 140 (16.1) | 1033 (14.4) | ||
| 3 | 2930 (26.3) | 160 (30.9) | 740 (28.6) | 241 (27.8) | 1789 (24.9) | ||
| Pre TIMI 0, 1 | 6490 (58.2) | 249 (48.1) | 1388 (53.7) | 0.0193 | 487 (56.1) | 4366 (60.7) | 0.0084 |
| Pre TIMI 3 | 2930 (26.3) | 160 (30.9) | 740 (28.6) | 0.3006 | 241 (27.8) | 1789 (24.9) | 0.0652 |
| Post TIMI | 0.0028 | 0.0256 | |||||
| 0 | 43 (0.4) | 4 (0.8) | 8 (0.3) | 8 (0.9) | 23 (0.3) | ||
| 1 | 48 (0.4) | 8 (1.5) | 8 (0.3) | 5 (0.6) | 27 (0.4) | ||
| 2 | 301 (2.7) | 17(3.28) | 72 (2.79) | 28 (3.2) | 184 (2.6) | ||
| 3 | 10,767 (96.5) | 489 (94.4) | 2497 (96.6) | 827 (95.3) | 6954 (96.7) | ||
| Post TIMI 0, 1 | 91 (0.8) | 12 (2.3) | 16 (0.6) | 0.0009 | 13 (1.5) | 50 (0.7) | 0.0113 |
| Post TIMI 3 | 10,767 (96.5) | 489 (94.4) | 2497 (96.6) | 0.0167 | 827 (95.3) | 6954 (96.7) | 0.0244 |
| Total n = 11,161 | Diabetic Patients | Non-Diabetic Patients | |||||
|---|---|---|---|---|---|---|---|
| Atypical n = 518 | Typical n = 2585 | p-Value | Atypical n = 868 | Typical n = 7188 | p-Value | ||
| In-hospital death | 388 (3.5) | 60 (11.6) | 98 (3.8) | <0.0001 | 67 (7.8) | 163 (2.3) | <0.0001 |
| Cardiac death | 329 (3.0) | 50 (9.7) | 79 (3.1) | <0.0001 | 56 (6.5) | 144 (2.0) | <0.0001 |
| Non-cardiac death | 59 (0.5) | 10 (1.9) | 19 (0.7) | 0.0200 | 11 (1.3) | 19 (0.3) | 0.0002 |
| Two-year clinical outcomes | |||||||
| POCE | 1924 (17.2) | 193 (37.3) | 529 (20.5) | <0.0001 | 237 (27.3) | 965 (13.4) | <0.0001 |
| All-cause of death | 1077 (9.7) | 153 (29.5) | 294 (11.4) | <0.0001 | 177 (20.4) | 453 (6.3) | <0.0001 |
| Any MI | 300 (2.7) | 29 (5.6) | 104 (4.0) | 0.1062 | 30 (3.5) | 137 (1.9) | 0.0025 |
| Any revascularization | 836 (7.5) | 43 (8.3) | 238 (9.2) | 0.5120 | 60 (6.9) | 495 (6.9) | 0.9772 |
| DOCE | 1020 (9.1) | 129 (24.9) | 292 (11.3) | <0.0001 | 159 (18.3) | 440 (6.1) | <0.0001 |
| Cardiac death | 755 (6.8) | 109 (21.0) | 206 (8.0) | <0.0001 | 130 (15.0) | 310 (4.3) | <0.0001 |
| Target vessel MI | 117 (1.1) | 10 (1.9) | 43 (1.7) | 0.6685 | 13 (1.5) | 51 (0.7) | 0.0135 |
| TLR | 246 (2.2) | 15 (2.9) | 78 (3.0) | 0.8822 | 27 (3.1) | 126 (1.8) | 0.0056 |
| Unadjusted Models | Adjusted Models | |||
|---|---|---|---|---|
| HR(95% CI) | p for Trend | HR (95% CI) | p for Trend | |
| POCE | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 1.58 (1.43–1.76) | 1.27 (1.13–1.42) | ||
| Atypical & Non-DM | 2.24 (1.94–2.58) | 1.43 (1.22–1.68) | ||
| Atypical & DM | 3.30 (2.83–3.85) | 1.76 (1.47–2.10) | ||
| All-cause of death | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 1.85 (1.60–2.14) | 1.44 (1.23–1.69) | ||
| Atypical & Non-DM | 3.50 (2.94–4.16) | 1.62 (1.33–1.97) | ||
| Atypical & DM | 5.36(4.46-6.44) | 2.23 (1.80–2.77) | ||
| Any MI | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 2.20 (1.70–2.84) | 1.79 (1.37–2.34) | ||
| Atypical & Non-DM | 2.03 (1.37–3.02) | 1.67 (1.11–2.53) | ||
| Atypical & DM | 3.60 (2.41–5.37) | 2.34 (1.51–3.63) | ||
| Any revascularization | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 1.40 (1.20–1.63) | 1.25 (1.06–1.48) | ||
| Atypical & Non-DM | 1.13 (0.86–1.47) | 1.11 (0.84–1.46) | ||
| Atypical & DM | 1.50 (1.10–2.05) | 1.34 (0.96–1.86) | ||
| DOCE | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 1.90 (1.64–2.20) | 1.48 (1.26–1.74) | ||
| Atypical & Non-DM | 3.26 (2.72–3.91) | 1.76 (1.44–2.17) | ||
| Atypical & DM | 4.70 (3.87–5.72) | 2.16 (1.72–2.72) | ||
| Cardiac death | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 1.88 (1.58–2.25) | 1.49 (1.22–1.81) | ||
| Atypical & Non-DM | 3.71 (3.02–4.55) | 1.70 (1.34–2.15) | ||
| Atypical & DM | 5.46 (4.39–6.80) | 2.27 (1.75–2.94) | ||
| Target vessel MI | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 2.43 (1.62–3.65) | 1.97 (1.28–3.01) | ||
| Atypical & Non-DM | 2.37 (1.29–4.35) | 1.92 (1.02–3.63) | ||
| Atypical & DM | 3.30 (1.68–6.51) | 2.17 (1.05–4.48) | ||
| TLR | <0.0001 | <0.0001 | ||
| Typical & Non-DM | 1 | 1 | ||
| Typical & DM | 1.79 (1.35–2.38) | 1.51 (1.12–2.03) | ||
| Atypical & Non-DM | 2.01 (1.32–3.04) | 1.79 (1.15–2.77) | ||
| Atypical & DM | 2.05 (1.20–3.50) | 1.55 (0.88–2.73) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-W.; Moon, J.S.; Kang, D.R.; Lee, S.J.; Son, J.-W.; Youn, Y.J.; Ahn, S.G.; Ahn, M.-S.; Kim, J.-Y.; Yoo, B.-S.; et al. Clinical Impact of Atypical Chest Pain and Diabetes Mellitus in Patients with Acute Myocardial Infarction from Prospective KAMIR-NIH Registry. J. Clin. Med. 2020, 9, 505. https://doi.org/10.3390/jcm9020505
Lee J-W, Moon JS, Kang DR, Lee SJ, Son J-W, Youn YJ, Ahn SG, Ahn M-S, Kim J-Y, Yoo B-S, et al. Clinical Impact of Atypical Chest Pain and Diabetes Mellitus in Patients with Acute Myocardial Infarction from Prospective KAMIR-NIH Registry. Journal of Clinical Medicine. 2020; 9(2):505. https://doi.org/10.3390/jcm9020505
Chicago/Turabian StyleLee, Jun-Won, Jin Sil Moon, Dae Ryong Kang, Sang Jun Lee, Jung-Woo Son, Young Jin Youn, Sung Gyun Ahn, Min-Soo Ahn, Jang-Young Kim, Byung-Su Yoo, and et al. 2020. "Clinical Impact of Atypical Chest Pain and Diabetes Mellitus in Patients with Acute Myocardial Infarction from Prospective KAMIR-NIH Registry" Journal of Clinical Medicine 9, no. 2: 505. https://doi.org/10.3390/jcm9020505