A Comparison of Cervical and Thoracolumbar Fractures Associated with Diffuse Idiopathic Skeletal Hyperostosis—A Nationwide Multicenter Study

 ,
,  , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Subject Criteria
2.2. Data Collection
2.2.1. Demographics and Cause of Injury
2.2.2. Radiological Characteristics
2.2.3. Delay in Diagnosis and Neurological Status
2.3. Statistical Analyses
3. Results
3.1. Demographics and Cause of Injury
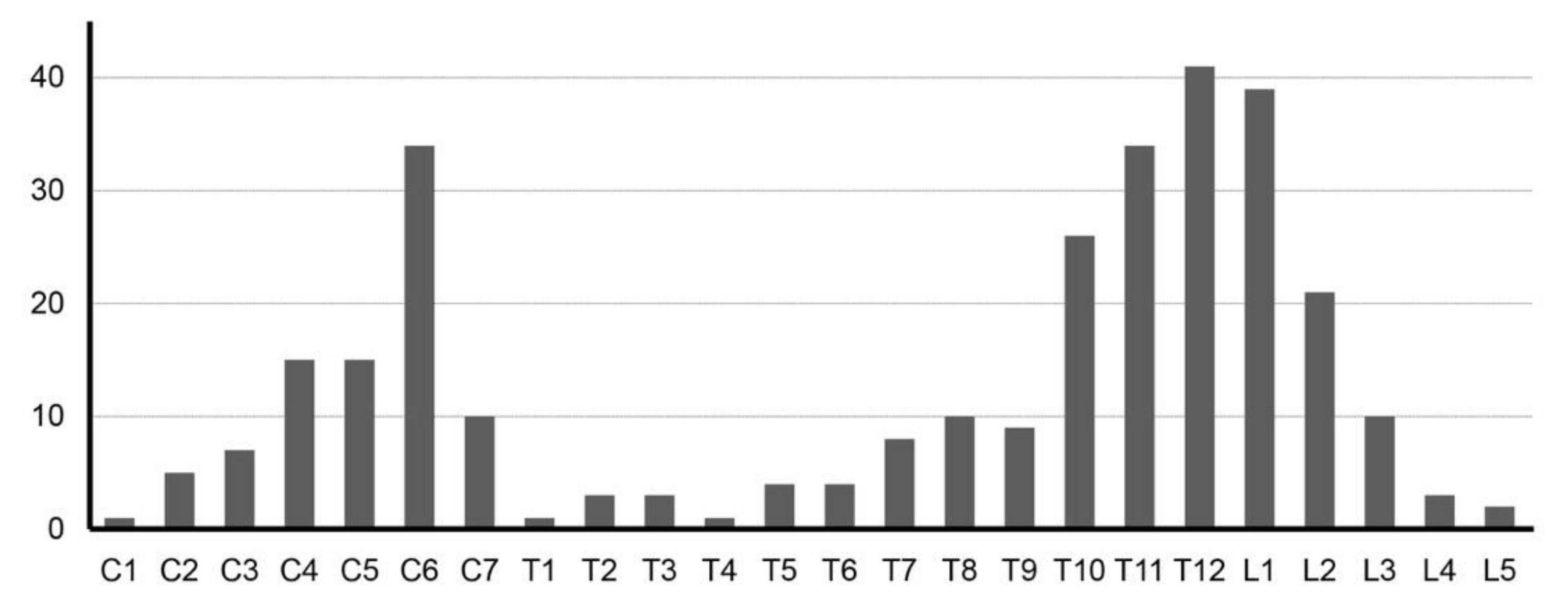
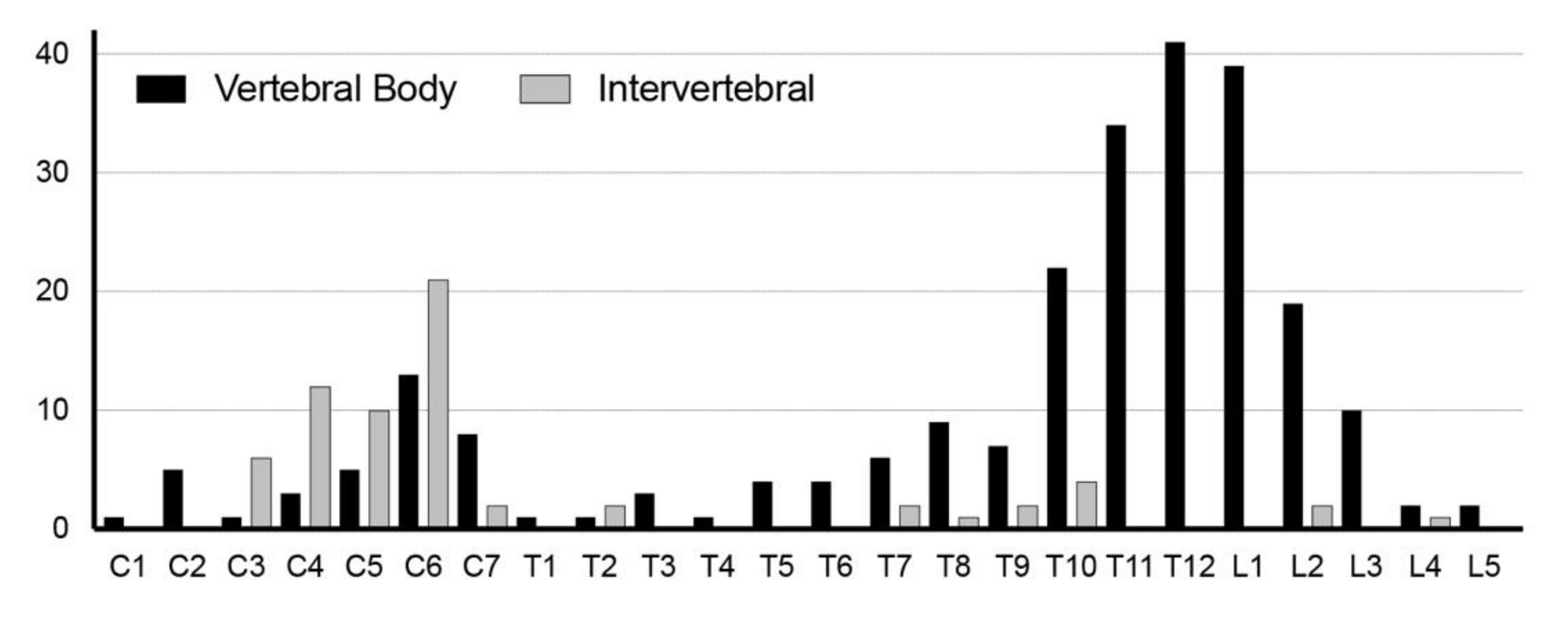
3.2. Radiological Characteristics
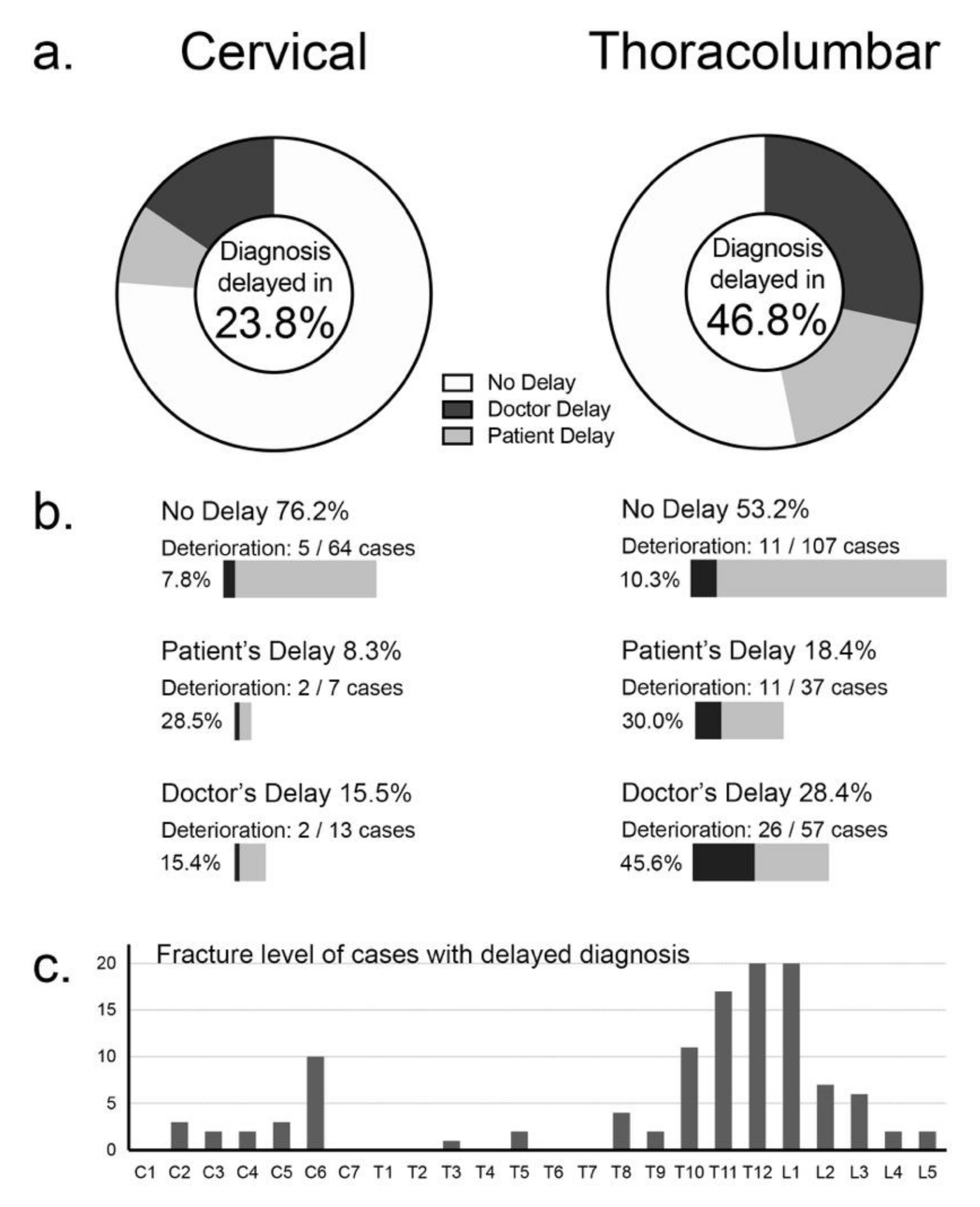
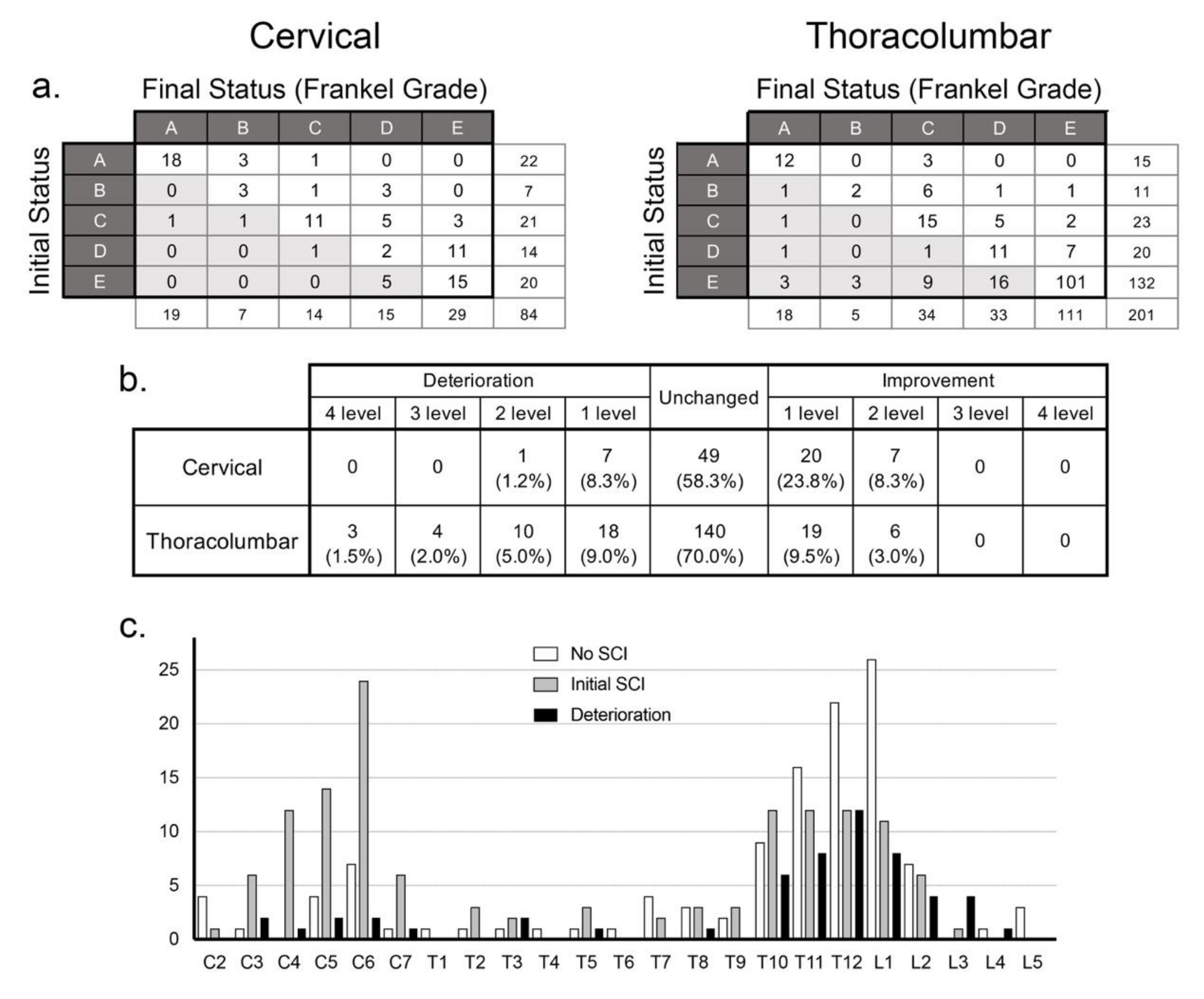
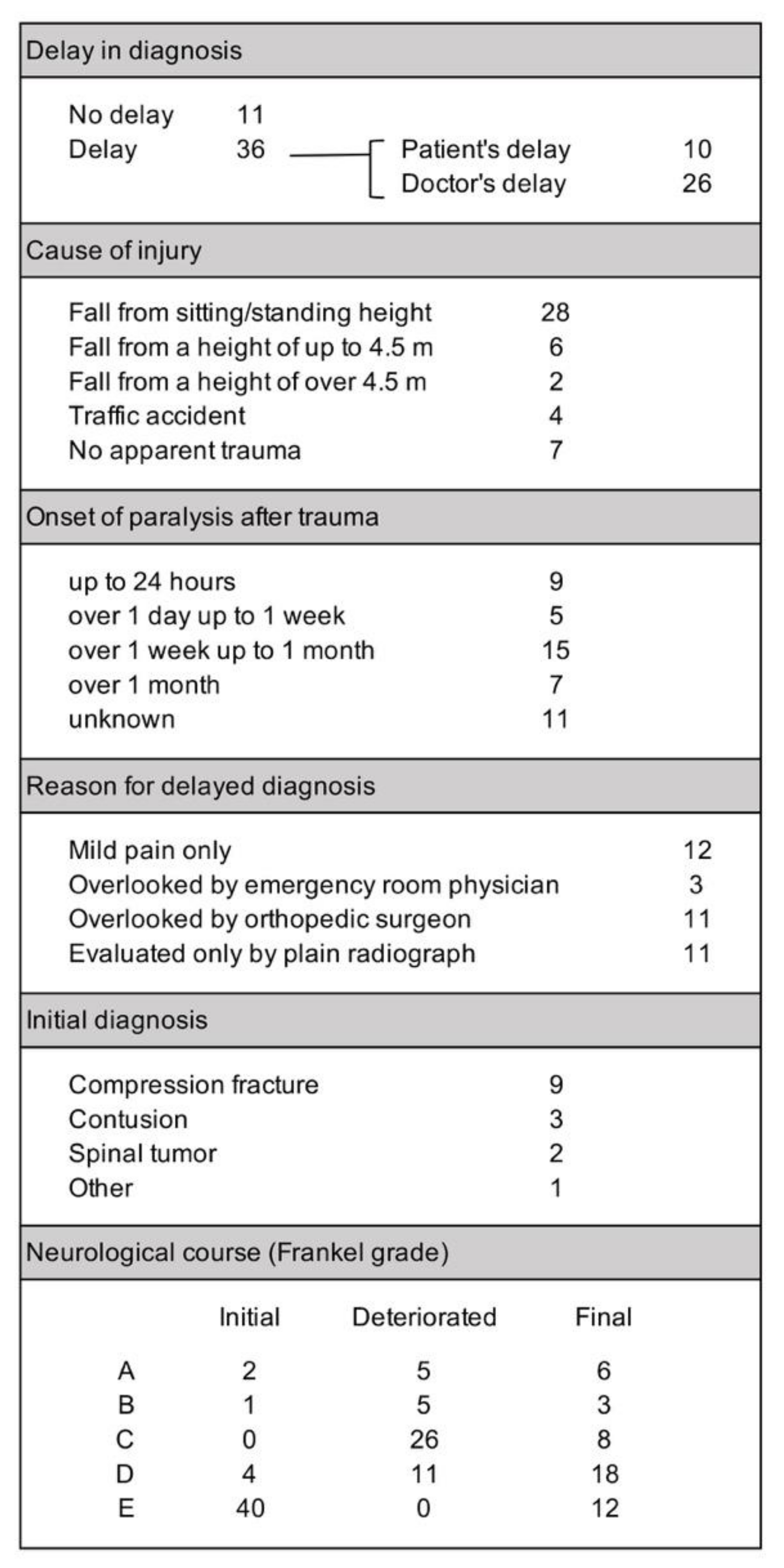
3.3. Delay in Diagnosis and Neurological Status
3.4. Thoracolumbar Cases with Neurological Deterioration
3.5. Treatment and Complications
4. Discussion
4.1. Prevalence of DISH-Associated Spine Fractures
4.2. Fracture Characteristics
4.3. Neurological Status and Course
4.4. Mortality
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forestier, J.; Rotes-Querol, J. Senile ankylosing hyperostosis of the spine. Ann. Rheum. Dis. 1950, 9, 321–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resnick, D.; Niwayama, G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976, 119, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Bjorkengren, A.G.; Sartoris, D.J.; Shermis, S.; Resnick, D. Patterns of paravertebral ossification in the prehistoric saber-toothed cat. AJR Am. J. Roentgenol. 1987, 148, 779–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothschild, B.M.; Woods, R. Old World spondylarthropathy: The gorilla connection. Arthritis Rheum. 1988, 31, 934–935. [Google Scholar] [CrossRef]
- Rothschild, B.M. Diffuse idiopathic skeletal hyperostosis as reflected in the paleontologic record: dinosaurs and early mammals. Semin. Arthritis Rheum. 1987, 17, 119–125. [Google Scholar] [CrossRef]
- Lee, B.B.; Cripps, R.A.; Fitzharris, M.; Wing, P.C. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord 2014, 52, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Toda, M.; Nakatani, E.; Omae, K.; Fukushima, M.; Chin, T. Age-specific characterization of spinal cord injuries over a 19-year period at a Japanese rehabilitation center. PLoS ONE 2018, 13, e0195120. [Google Scholar] [CrossRef]
- Okada, E.; Yoshii, T.; Yamada, T.; Watanabe, K.; Katsumi, K.; Hiyama, A.; Watanabe, M.; Nakagawa, Y.; Okada, M.; Endo, T.; et al. Spinal fractures in patients with Diffuse idiopathic skeletal hyperostosis: A nationwide multi-institution survey. J. Orthop. Sci. 2019, 24, 601–606. [Google Scholar] [CrossRef]
- Caron, T.; Bransford, R.; Nguyen, Q.; Agel, J.; Chapman, J.; Bellabarba, C. Spine fractures in patients with ankylosing spinal disorders. Spine 2010, 35, E458–E464. [Google Scholar] [CrossRef]
- Westerveld, L.A.; Verlaan, J.J.; Oner, F.C. Spinal fractures in patients with ankylosing spinal disorders: A systematic review of the literature on treatment, neurological status and complications. Eur. Spine J. 2009, 18, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Frankel, H.L.; Hancock, D.O.; Hyslop, G.; Melzak, J.; Michaelis, L.S.; Ungar, G.H.; Vernon, J.D.; Walsh, J.J. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia 1969, 7, 179–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerveld, L.A.; van Bemmel, J.C.; Dhert, W.J.; Oner, F.C.; Verlaan, J.J. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014, 14, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, F.R.; Verbeek, B.M.; Cha, T.D.; Schwab, J.H. Spinal cord injury after traumatic spine fracture in patients with ankylosing spinal disorders. J. Neurosurg. Spine 2017, 27, 709–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiyama, A.; Katoh, H.; Sakai, D.; Sato, M.; Tanaka, M.; Watanabe, M. Prevalence of diffuse idiopathic skeletal hyperostosis (DISH) assessed with whole-spine computed tomography in 1479 subjects. BMC Musculoskelet. Disord. 2018, 19, 178. [Google Scholar] [CrossRef] [Green Version]
- Toyoda, H.; Terai, H.; Yamada, K.; Suzuki, A.; Dohzono, S.; Matsumoto, T.; Nakamura, H. Prevalence of Diffuse Idiopathic Skeletal Hyperostosis in Patients with Spinal Disorders. Asian Spine J. 2017, 11, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, A.J.; Harris, M.B.; McGuire, K.J.; Warholic, N.; Wood, K.B.; Bono, C.M. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011, 11, 257–264. [Google Scholar] [CrossRef]
- Dean, L.E.; Jones, G.T.; MacDonald, A.G.; Downham, C.; Sturrock, R.D.; Macfarlane, G.J. Global prevalence of ankylosing spondylitis. Rheumatology 2014, 53, 650–657. [Google Scholar] [CrossRef] [Green Version]
- Hukuda, S.; Minami, M.; Saito, T.; Mitsui, H.; Matsui, N.; Komatsubara, Y.; Makino, H.; Shibata, T.; Shingu, M.; Sakou, T.; et al. Spondyloarthropathies in Japan: Nationwide questionnaire survey performed by the Japan Ankylosing Spondylitis Society. J. Rheumatol. 2001, 28, 554–559. [Google Scholar]
- Kagotani, R.; Yoshida, M.; Muraki, S.; Oka, H.; Hashizume, H.; Yamada, H.; Enyo, Y.; Nagata, K.; Ishimoto, Y.; Teraguchi, M.; et al. Prevalence of diffuse idiopathic skeletal hyperostosis (DISH) of the whole spine and its association with lumbar spondylosis and knee osteoarthritis: The ROAD study. J. Bone Miner. Metab. 2015, 33, 221–229. [Google Scholar] [CrossRef]
- Mori, K.; Kasahara, T.; Mimura, T.; Nishizawa, K.; Nakamura, A.; Imai, S. Prevalence of thoracic diffuse idiopathic skeletal hyperostosis (DISH) in Japanese: Results of chest CT-based cross-sectional study. J. Orthop. Sci. 2017, 22, 38–42. [Google Scholar] [CrossRef]
- Fujimori, T.; Watabe, T.; Iwamoto, Y.; Hamada, S.; Iwasaki, M.; Oda, T. Prevalence, Concomitance, and Distribution of Ossification of the Spinal Ligaments: Results of Whole Spine CT Scans in 1500 Japanese Patients. Spine 2016, 41, 1668–1676. [Google Scholar] [CrossRef] [PubMed]
- Kuperus, J.S.; Samsour, L.; Buckens, C.F.; Oner, F.C.; de Jong, P.A.; Verlaan, J.J. Bone mineral density changes over time in diffuse idiopathic skeletal hyperostosis of the thoracic spine. Bone 2018, 112, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Bransford, R.J.; Koller, H.; Caron, T.; Zenner, J.; Hitzl, W.; Tomasino, A.; Mayer, M. Cervical spine trauma in diffuse idiopathic skeletal hyperostosis: Injury characteristics and outcome with surgical treatment. Spine 2012, 37, 1923–1932. [Google Scholar] [CrossRef] [PubMed]
- Carile, L.; Verdone, F.; Aiello, A.; Buongusto, G. Diffuse idiopathic skeletal hyperostosis and situs viscerum inversus. J. Rheumatol. 1989, 16, 1120–1122. [Google Scholar]
- Bakker, J.T.; Kuperus, J.S.; Kuijf, H.J.; Oner, F.C.; de Jong, P.A.; Verlaan, J.J. Morphological characteristics of diffuse idiopathic skeletal hyperostosis in the cervical spine. PLoS ONE 2017, 12, e0188414. [Google Scholar] [CrossRef] [Green Version]
- Taljanovic, M.S.; Hunter, T.B.; Wisneski, R.J.; Seeger, J.F.; Friend, C.J.; Schwartz, S.A.; Rogers, L.F. Imaging characteristics of diffuse idiopathic skeletal hyperostosis with an emphasis on acute spinal fractures: Review. AJR Am. J. Roentgenol. 2009, 193, S10–S19. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, S.; Nagoshi, N.; Iwanami, A.; Takeuchi, A.; Hirai, T.; Yoshii, T.; Takeuchi, K.; Mori, K.; Yamada, T.; Seki, S.; et al. Prevalence and Distribution of Diffuse Idiopathic Skeletal Hyperostosis on Whole-spine Computed Tomography in Patients With Cervical Ossification of the Posterior Longitudinal Ligament: A Multicenter Study. Clin. Spine Surg. 2018, 31, E460–E465. [Google Scholar] [CrossRef]
- Whang, P.G.; Goldberg, G.; Lawrence, J.P.; Hong, J.; Harrop, J.S.; Anderson, D.G.; Albert, T.J.; Vaccaro, A.R. The management of spinal injuries in patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis: A comparison of treatment methods and clinical outcomes. J. Spinal Disord. Tech. 2009, 22, 77–85. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cervical | Thoracolumbar | p value | |
|---|---|---|---|
| Cases | 84 | 201 | |
| Gender | |||
| Male | 77 (91.7%) | 144 (71.6%) | <0.01 * |
| Female | 7 (8.3%) | 57 (28.4) | |
| Age (years, mean ± std) | 74.5 ± 9.0 | 75.4 ± 9.8 | 0.434 |
| Body Mass Index (kg/m2, mean ± std) | 22.9 ± 3.9 | 23.7 ± 3.7 | 0.181 |
| Past Medical History | |||
| Diabetes | 26 (31.0%) | 41 (20.4%) | 0.055 |
| Kidney disease | 2 (2.4%) | 11 (5.5%) | 0.254 |
| Liver disease | 0 | 5 (2.5%) | — |
| Osteoporosis | 1 (1.2%) | 4 (2.0%) | 0.64 |
| History of past fractures | 0 | 2 (1.0%) | — |
| Malignancies | 4 (4.8%) | 21 (10.4%) | 0.122 |
| Cause of Injury | <0.05 * | ||
| Fall from standing/sitting position | 48 (57.1%) | 100 (49.8%) | |
| Fall from a height | 22 (26.2%) | 59 (29.4%) | |
| Traffic accident | 13 (15.5%) | 21 (10.4%) | |
| No apparent trauma | 1 (1.2%) | 21 (10.4%) | <0.0125 * |
| Cervical | Thoracolumbar | p value | |
|---|---|---|---|
| Ossification at fracture site | |||
| Ossification of posterior longitudinal ligament (OPLL) | 39 (47.0%) | 5 (2.5%) | <0.01 * |
| Ossification of ligamentum flavum (OLF) | 1 (1.2%) | 1 (0.5%) | 0.524 |
| Posterior elements | 19 (22.6%) | 123 (62.1%) | <0.01 * |
| Fracture site | |||
| Anterior | 84 (100%) | 201 (100%) | |
| Intervertebral | 55 (65.5%) | 49 (24.4%) | <0.01 * |
| Vertebral body | 29 (34.5%) | 152 (75.6%) | <0.01 * |
| Posterior | 39 (46.4%) | 134 (67.7%) | <0.05 * |
| Fracture pattern (Caron classification) | |||
| Type 1 (disc injury) | 31 | 17 | <0.125 * |
| Type 2 (body injury) | 25 | 134 | <0.125 * |
| Type 3 (anterior body or posterior disc injury) | 14 | 21 | |
| Type 4 (anterior disc or posterior body injury) | 9 | 16 |
| Cervical | Thoracolumbar | p value | |
|---|---|---|---|
| Conservative treatment | 9 (10.7%) | 36 (17.9%) | 0.129 |
| Surgical treatment | 75 (89.3%) | 165 (82.1%) | |
| Anterior fusion | 1 (1.2%) | 0 | 0.177 |
| Posterior fusion | 67 (79.8%) | 153 (76.1%) | |
| Anteroposterior fusion | 7 (8.3%) | 12 (6.0%) | |
| Complications | 31 (36.9%) | 55 (27.4%) | 0.11 |
| representative conditions: | respiratory: 13 | instrument-related: 8 | |
| UTI: 4 | UTI: 8 | ||
| dysphagia: 3 | respiratory: 6 | ||
| wound infection: 2 | wound infection: 6 | ||
| DVT: 2 | DVT: 3 | ||
| Death (within 6 months) | 13 (15.5%) | 10 (5.0%) | <0.05 * |
| causes: | pneumonia: 4 | pneumonia: 2 | |
| heart failure: 1 | heart failure: 1 | ||
| renal failure: 1 | septic cholecystitis: 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katoh, H.; Okada, E.; Yoshii, T.; Yamada, T.; Watanabe, K.; Katsumi, K.; Hiyama, A.; Nakagawa, Y.; Okada, M.; Endo, T.; et al. A Comparison of Cervical and Thoracolumbar Fractures Associated with Diffuse Idiopathic Skeletal Hyperostosis—A Nationwide Multicenter Study. J. Clin. Med. 2020, 9, 208. https://doi.org/10.3390/jcm9010208
Katoh H, Okada E, Yoshii T, Yamada T, Watanabe K, Katsumi K, Hiyama A, Nakagawa Y, Okada M, Endo T, et al. A Comparison of Cervical and Thoracolumbar Fractures Associated with Diffuse Idiopathic Skeletal Hyperostosis—A Nationwide Multicenter Study. Journal of Clinical Medicine. 2020; 9(1):208. https://doi.org/10.3390/jcm9010208
Chicago/Turabian StyleKatoh, Hiroyuki, Eijiro Okada, Toshitaka Yoshii, Tsuyoshi Yamada, Kei Watanabe, Keiichi Katsumi, Akihiko Hiyama, Yukihiro Nakagawa, Motohiro Okada, Teruaki Endo, and et al. 2020. "A Comparison of Cervical and Thoracolumbar Fractures Associated with Diffuse Idiopathic Skeletal Hyperostosis—A Nationwide Multicenter Study" Journal of Clinical Medicine 9, no. 1: 208. https://doi.org/10.3390/jcm9010208