Incidence of Cardiovascular Disease in Patients with Familial Hypercholesterolemia Phenotype: Analysis of 5 Years Follow-Up of Real-World Data from More than 1.5 Million Patients

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Source
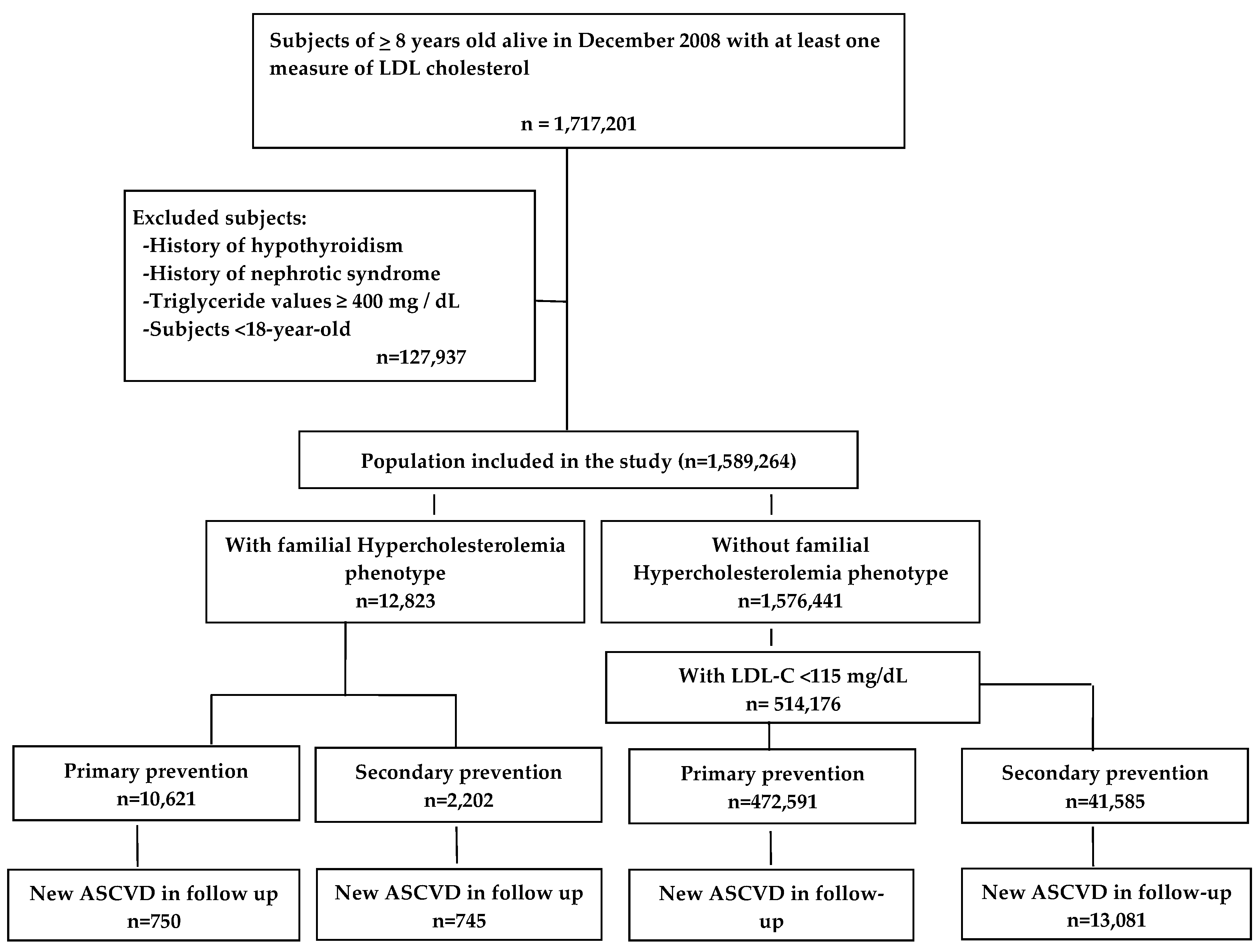
2.3. Study Population
2.4. Follow up and Outcomes
2.5. Variables and Definitions
2.6. Statistical Analyses
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Akioyamen, L.E.; Genest, J.; Shan, S.D.; Reel, R.L.; Albaum, J.M.; Chu, A.; Tu, J.V. Estimating the prevalence of heterozygous familial hypercholesterolaemia: A systematic review and meta-analysis. BMJ Open 2017, 7, e016461. [Google Scholar] [CrossRef] [PubMed]
- Zamora, A.; Masana, L.; Comas-Cufi, M.; Vila, A.; Plana, N.; García-Gil, M.; Alves-Cabratosa, L.; Marrugat, J.; Roman, I.; Ramos, R. Rrepresenting the XULA and ISV-Girona groups. Familial hypercholesterolemia in a European Mediterranean population-Prevalence and clinical data from 2.5 million primary care patients Journal of Clinical. Lipidology 2017, 11, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Vallejo-Vaz, A.J.; Robertson, L.; Catapano, L.A.; Watts, G.F.; Kastelein, J.J.; Packard, C.J.; Ford, I.; Kausik, K.R. LDL-Cholesterol Lowering for the Primary Prevention of Cardiovascular Disease Among Men with primary elevations of LDL-cholesterol levels of 190 mg/dL or above. Analyses from the WOSCOPS 5-year Randomised Trial and 20-year Observational Follow-Up. Circulation 2017, 136, 1878–1891. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R. Authors/Task Force Members, Additional Contributor. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed]
- Perez de Isla, L.; Alonso, R.; Watts, G.F.; Mata, N.; Saltijeral-Cerezo, A.; Muñiz, O.; Fuentes, F.; Diaz-Diaz, J.L.; de Andrés, R.; Zambón, D.; et al. Attainment of LDL-Cholesterol Treatment Goals in Patients with Familial Hypercholesterolemia: 5-Year SAFEHEART Registry Follow-Up. J. Am. Coll. Cardiol. 2016, 67, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Bacquer, D.D.; Smedt, D.D.; Kotseva, K.; Jennings, C.; Wood, D.; Rydén, L.; Gyberg, V.; Shahim, B.; Amouyel, P.; Bruthans, J.; et al. EUROASPIRE Investigators. Incidence of cardiovascular events in patients with stabilized coronary heart disease: The EUROASPIRE IV follow-up study. Eur. J. Epidemiol. 2019, 34, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Benn, M.; Watts, G.F.; Tybjaerg-Hansen, A.; Nordestgaard, B.G. Familial hypercholesterolemia in the danish general population: Prevalence, coronary artery disease, and cholesterol-lowering medication. J. Clin. Endocrinol. Metab. 2012, 97, 3956–3964. [Google Scholar] [CrossRef]
- Pérez de Isla, L.; Alonso, R.; Mata, N.; Saltijeral, A.; Muñiz, O.; Rubio-Marin, P.; Diaz-Diaz, J.L.; Fuentes, F.; de Andrés, R.; Zambón, D.; et al. SAFEHEART Coronary Heart Disease, Peripheral Arterial Disease, and Stroke in Familial Hypercholesterolaemia: Insights From the SAFEHEART Registry (Spanish Familial Hypercholesterolaemia Cohort Study). Arterioscler. Thromb. Vasc. Biol. 2016, 36, 2004–2010. [Google Scholar] [CrossRef]
- Pérez de Isla, L.; Alonso, R.; Mata, N.; Fernández-Pérez, C.; Muñiz, O.; Díaz-Díaz, J.L.; Saltijeral, A.; Fuentes-Jiménez, F.; de Andrés, R.; Zambón, D.; et al. Predicting Cardiovascular Events in Familial Hypercholesterolemia: The SAFEHEART Registry (Spanish Familial Hypercholesterolemia Cohort Study). Circulation 2017, 135, 2133–2144. [Google Scholar] [CrossRef]
- García-Gil, M.M.; Hermosilla, E.; Prieto-Alhambra, D.; Prieto-Alhambra, D.; Fina, F.; Rosell, M.; Ramos, R.; Rodriguez, J.; Williams, T.; Van Staa, T.; et al. Construction and validation of a scoring system for the selection of high-quality data in a Spanish population primary care database (SIDIAP). Inform. Prim. Care 2011, 19, 135–145. [Google Scholar] [CrossRef]
- Ramos, R.; Ballo, E.; Marrugat, J.; Elosua, R.; Sala, J.; Grau, M.; Vila, J.; Bolíbar, B.; García-Gil, M.; Martí, R.; et al. Validity for use in research on vascular diseases of the SIDIAP (Information System for the Development of Research in Primary Care): The EMMA study. Rev. Esp. Cardiol. 2012, 65, 29–37. [Google Scholar] [CrossRef] [PubMed]
- García-Gil, M.; Blanch, J.; Comas-Cufí, M.; Daunis-i-Estadella, J.; Bolíbar, B.; Martí, R.; Ponjoan, A.; Alves-Cabratosa, L.; Ramos, R. Patterns of statin use and cholesterol goal attainment in a high-risk cardiovascular population: A retrospective study of primary care electronic medical records. J. Clin. Lipidol. 2015, 10, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.; Comas-Cufí, M.; Martí-Lluch, R.; Balló, E.; Ponjoan, A.; Alves-Cabratosa, L.; Blanch, J.; Marrugat, J.; Elosua, R.; Grau, M.; et al. Statins for primary prevention of cardiovascular events and mortality in old and very old adults with and without type 2 diabetes: Retrospective cohort study. BMJ 2018, 362, k3359. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, N.W.; Sibley, C.T.; McClelland, R.L. Using imputed pretreatment cholesterol in a propensity score model to reduce confounding by indication: Results from the multi-ethnic study of atherosclerosis. BMC Med. Res. Methodol. 2013, 13, 81. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef] [PubMed]
- Civeira, F.; Ros, E.; Jarauta, E.; Plana, N.; Zambon, D.; Puzo, J.; Martinez de Esteban, J.P.; Ferrando, J.; Zabala, S.; Almagro, F.; et al. Comparison of genetic versus clinical diagnosis in familial hypercholesterolemia. Am. J. Cardiol. 2008, 102, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: https://www.R-project.org (accessed on 5 July 2019).
- Mundal, L.J.; Igland, J.; Veierød, M.B.; Holven, K.B.; Ose, L.; Selmer, R.M.; Wisloff, T.; Kristiansen, I.S.; Tell, G.S.; Leren, T.P.; et al. Impact of age on excess risk of coronary heart disease in patients with familial hypercholesterolaemia. Heart 2018, 104, 1600–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphries, S.E.; Cooper, J.A.; Capps, N.; Durrington, P.N.; Jones, B.; McDowell, I.F.; Soran, H.; Neil, A.H.W. Simon Broome Familial Hyperlipidaemia Register Group. Coronary heart disease mortality in severe vs. non-severe familial hypercholesterolaemia in the Simon Broome Register. Atherosclerosis 2019, 281, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Iyen, B.; Qureshi, N.; Kai, J.; Akyea, R.K.; Leonardi-Bee, J.; Roderick, P.; Humphries, S.E.; Weng, S. Risk of cardiovascular disease outcomes in primary care subjects with familial hypercholesterolaemia: A cohort study. Atherosclerosis 2019, 287, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Amrock, S.M.; Duell, P.B.; Knickelbine, T.; Martin, S.S.; O’Brien, E.C.; Watson, K.E.; Mitri, J.; Kindt, I.; Shrader, P.; Baum, S.J.; et al. Health disparities among adult patients with a phenotypic diagnosis of familial hypercholesterolemia in the CASCADE-FH patient registry. Atherosclerosis 2017, 267, 19–26. [Google Scholar] [CrossRef]
- Akioyamen, L.E.; Genest, J.; Chu, A.; Inibhunu, H.; Ko, D.T.; Tu, J.V. Risk factors for cardiovascular disease in heterozygous familial hypercholesterolemia: A systematic review and meta-analysis. J. Clin. Lipidol. 2019, 13, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.; Bernard, S.; Ruel, I.; Blank, D.W.; Genest, J.; Baass, A. Diabetes is associated with an increased risk of cardiovascular disease in patients with familial hypercholesterolemia. J. Clin. Lipidol. 2019, 13, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Zafrir, B.; Jubran, A.; Lavie, G.; Halon, D.A.; Flugelman, M.Y.; Shapira, C. Clinical Features and Gaps in the Management of Probable Familial Hypercholesterolemia and Cardiovascular Disease. Circ. J. 2017, 82, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Perez-Calahorra, S.; Laclaustra, M.; Marco-Benedí, V.; Lamiquiz-Moneo, I.; Pedro-Botet, J.; Plana, N.; Sanchez-Hernandez, R.M.; Amor, A.J.; Almagro, F.; Fuentes, F.; et al. Dyslipemia Registry of Spanish Arteriosclerosis Society. Effect of lipid-lowering treatment in cardiovascular disease prevalence in familial hypercholesterolemia. Atherosclerosis 2019, 284, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Nanchen, D.; Gencer, B.; Muller, O.; Auer, R.; Aghlmandi, S.; Heg, D.; Klingenberg, R.; Räber, L.; Carballo, D.; Carballo, S.; et al. Prognosis of Patients with Familial Hypercholesterolemia After Acute Coronary Syndromes. Circulation 2016, 134, 698–709. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. ODYSSEY OUTCOMES Committees and Investigators. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef]
- Gencer, B.; Koskinas, K.C.; Räber, L.; Karagiannis, A.; Nanchen, D.; Auer, R.; Carballo, D.; Carballo, S.; Klingenberg, R.; Heg, D.; et al. Eligibility for PCSK9 Inhibitors According to American College of Cardiology (ACC) and European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) Guidelines After Acute Coronary Syndromes. J. Am. Heart Assoc. 2017, 6, 11. [Google Scholar] [CrossRef]
- Zamora, A.; Masana, L.; Comas-Cufi, M.; Plana, N.; Vila, A.; García-Gil, M.; Alves-Cabratosa, L.; Elosua, R.; Marrugat, J.; Ramos, R. Number of Patients Eligible for PCSK9 Inhibitors Based on Real-world Data From 2.5 Million Patients. Rev. Esp. Cardiol. 2018, 71, 1010–1017. [Google Scholar] [CrossRef]
- Masana, L.; Ibarretxe, D.; Rodríguez-Borjabad, C.; Plana, N.; Valdivielso, P.; Pedro-Botet, J.; Civeira, F.; López-Miranda, J.; Guijarro, C.; Mostaza, J.; et al. Toward a new clinical classification of patients with familial hypercholesterolemia: One perspective from Spain. Atherosclerosis 2019, 287, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Khera, A.V.; Chaffin, M.; Aragam, K.G.; Haas, M.E.; Roselli, C.; Choi, S.H.; Natarajan, P.; Lander, E.S.; Lubitz, S.A.; Ellinor, P.T.; et al. Genome-wide polygenic scores for common diseases identify individuals with risk equivalent to monogenic mutations. Nat. Genet. 2018, 50, 1219–1224. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal LDL-C < 115 mg/dL | FH-P | Normal LDL-C < 115 mg/dL | FH-P | |||
|---|---|---|---|---|---|---|
| Variable | Without ASCVD | Without ASCVD | P Value | With ASCVD | With ASCVD | P Value |
| N | 472,591 | 10,621 | 41,585 | 2202 | ||
| Age, mean (SD) | 48.2 (19.3) | 60.5 (13.6) | <0.01 | 73.2 (12.1) | 67.7 (10.7) | <0.01 |
| Male, sex, % | 40.9% | 40.9% | 0.98 | 64.5% | 63.3% | 0.34 |
| Diabetes, mellitus, % | 14.2% | 21.7% | <0.01 | 44% | 36.7% | <0.01 |
| Hypertension, % | 33.6% | 60.7% | <0.01 | 91.8% | 93.3% | 0.03 |
| Current, smoker, % | 30.3% | 32.3 | <0.01 | 43.3% | 49.1 | <0.01 |
| BMI, mean (SD) | 27.5 (5.6) | 28.9 (4.7) | <0.01 | 28.8 (4.9) | 29.2 (4.5) | <0.01 |
| Receiving lipid therapy, % | 4.1% | 87.1% | <0.01 | 36.3% | 97.4% | <0.01 |
| Personal history of CAD, % | - | - | - | 36.3% | 46.9% | <0.01 |
| Personal history of PAD, % | - | - | - | 16.7% | 15.6% | 0.27 |
| Personal history of Stroke, % | - | - | - | 30.4% | 22.8% | <0.01 |
| TC, mg/dL, mean (SD) | 169.9 (26.1) | 257.9 (59.5) | <0.01 | 160.8 (29.5) | 223.9 (5) | <0.01 |
| LDL-C, mg/dL, mean (SD) | 91.8 (17.9) | 177.6 (55.5) | <0.01 | 85.4 (20.4) | 147.1 (46.0) | <0.01 |
| Untreated LDL-C, mg/dL, mean (SD) | 92.3 (16.6) | 285.2 (34.7) | <0.01 | 93.08 (16.7) | 287.5 (3) | <0.01 |
| HDL-C, mg/dL, mean (SD) | 56.1 (16.3) | 56.3 (13.8) | 0.23 | 49.3 (15.2) | 51.6 (13.0) | <0.01 |
| Non-HDL-C, mg/dL, mean (SD) | 113.7 (24.2) | 201.7 (59.3) | <0.01 | 111.4 (26.7) | 172.3 (51.3) | <0.01 |
| TG, mg/dL, mean (SD) | 111.2 (74.1) | 149.1 (88) | <0.01 | 127.3 (81.8) | 150.6 (83.1) | <0.01 |
| Creatinine, mean (SD) | 0.85 (0.3) | 0.89 (0.2) | <0.01 | 1.08 (0.6) | 1.03 (0.4) | <0.01 |
| HBA1c, mean (SD) | 5.7 (1.5) | 6.02 (1.5) | <0.01 | 6.2 (1.4) | 6.2 (1.6) | 0.55 |
| Normal LDL-C Population (<115 mg/dL) | Familial Hypercholesterolemia Phenotype | ||||||
|---|---|---|---|---|---|---|---|
| Age Groups | Number (n) | Events (n) | IR (1000 p/y) 95%CI | Number (n) | Events (n) | IR (1000 p/y) IC 95 | HR IC 95 |
| All | 472,591 | 15,980 | 7.1 (7.0–7.2) | 10,621 | 749 | 14.9 (13.7–16.2) | 1.45 (1.33–1.58) |
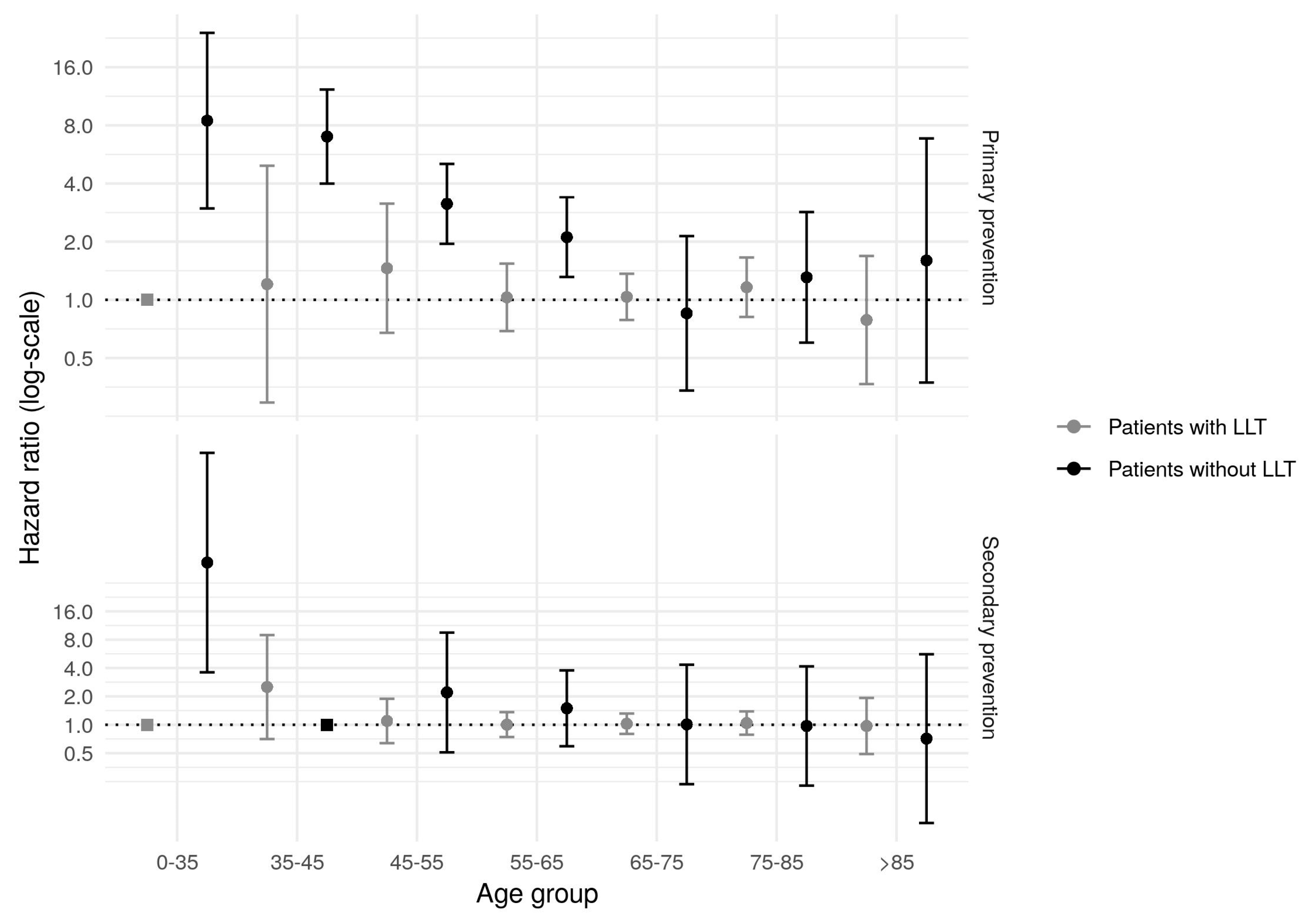
| 0–35 | 141,920 | 143 | 0.2 (0.2–0.2) | 551 | 6 | 2.1 (0.9–5.2) | 7.13 (2.85–17.84) |
| 35–45 | 91,274 | 483 | 1.1 (1.0–1.2) | 833 | 30 | 7.3 (4.7–11.2) | 3.78 (2.42–5.91) |
| 45–55 | 70,331 | 1256 | 3.6 (3.4–3.8) | 1652 | 76 | 9.4 (7.1–12.5) | 1.86 (1.41–2.46) |
| 55–65 | 56,835 | 2635 | 9.6 (9.3–10.0) | 3241 | 198 | 12.7 (10.5–15.3) | 1.43 (1.19–1.72) |
| 65–75 | 50,897 | 4237 | 18.0 (17.4–18.6) | 2713 | 232 | 18.3 (15.6–21.4) | 1.16 (0.98–1.36) |
| 75–85 | 44,604 | 5232 | 27.8 (27.0–28.6) | 1441 | 181 | 28.4 (23.1–34.8) | 1.13 (0.92–1.39) |
| >85 | 16,730 | 1995 | 36.1 (34.4–37.8) | 189 | 27 | 37.8 (23.6–60.6) | 1.09 (0.68–1.75) |
| Normal LDL-C Population (<115 mg/dL) | Familial Hypercholesterolemia Phenotype | ||||||
|---|---|---|---|---|---|---|---|
| Age Groups | Number (n) | Events (n) | IR (1000 p/y) 95%CI | Number (n) | Events (n) | IR (1000 p/y) IC 95 | HR IC 95 |
| All | 41,586 | 13,081 | 91.0 (89.2–92.8) | 2202 | 745 | 89.8 (82.1–98.1) | 1.10 (1.01–1.21) |
| 0–35 | 262 | 22 | 18.2 (11.7–28.4) | 8 | 2 | 74.6 (14.4–385.9) | 2.36 (0.37–14.95) |
| 35–45 | 698 | 134 | 43.9 (36.5–52.8) | 36 | 14 | 98.6 (51.3–189.4) | 1.92 (0.98–3.76) |
| 45–55 | 2329 | 631 | 66.4 (60.8–72.4) | 214 | 68 | 79.3 (59.8–105.2) | 1.14 (0.86–1.51) |
| 55–65 | 5898 | 1772 | 75.7 (71.8–79.8) | 581 | 188 | 81.8 (67.5–99.1) | 1.12 (0.93–1.35) |
| 65–75 | 10,340 | 3480 | 90.1 (86.9–93.5) | 718 | 244 | 88.7 (75.8–103.8) | 1.07 (0.91–1.27) |
| 75–85 | 14,965 | 5128 | 103.9 (100.7–107.2) | 544 | 193 | 101.6 (84.9–121.5) | 1.06 (0.88–1.27) |
| >85 | 7094 | 1912 | 102.8 (97.9–107.9) | 100 | 35 | 111.4 (68.1–182.1) | 1.13 (0.67–1.92) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masana, L.; Zamora, A.; Plana, N.; Comas-Cufí, M.; Garcia-Gil, M.; Martí-Lluch, R.; Ponjoan, A.; Alves-Cabratosa, L.; Elosua, R.; Marrugat, J.; et al. Incidence of Cardiovascular Disease in Patients with Familial Hypercholesterolemia Phenotype: Analysis of 5 Years Follow-Up of Real-World Data from More than 1.5 Million Patients. J. Clin. Med. 2019, 8, 1080. https://doi.org/10.3390/jcm8071080
Masana L, Zamora A, Plana N, Comas-Cufí M, Garcia-Gil M, Martí-Lluch R, Ponjoan A, Alves-Cabratosa L, Elosua R, Marrugat J, et al. Incidence of Cardiovascular Disease in Patients with Familial Hypercholesterolemia Phenotype: Analysis of 5 Years Follow-Up of Real-World Data from More than 1.5 Million Patients. Journal of Clinical Medicine. 2019; 8(7):1080. https://doi.org/10.3390/jcm8071080
Chicago/Turabian StyleMasana, Luís, Alberto Zamora, Núria Plana, Marc Comas-Cufí, Maria Garcia-Gil, Ruth Martí-Lluch, Anna Ponjoan, Lia Alves-Cabratosa, Roberto Elosua, Jaume Marrugat, and et al. 2019. "Incidence of Cardiovascular Disease in Patients with Familial Hypercholesterolemia Phenotype: Analysis of 5 Years Follow-Up of Real-World Data from More than 1.5 Million Patients" Journal of Clinical Medicine 8, no. 7: 1080. https://doi.org/10.3390/jcm8071080